

Abstract
Background and study aims
Bubbles can impair visualization of the small bowel (SB) mucosa during capsule endoscopy (CE). We aimed to develop and validate a computed algorithm that would allow evaluation of the abundance of bubbles in SB-CE still frames.
Patients and methods
Two sets of 200 SB-CE normal still frames were created. Two experienced SB-CE readers analyzed both sets of images twice, in a random order. Each still frame was categorized as presenting with < 10 % or ≥ 10 % of bubbles. Reproducibility (κ), sensitivity (Se), specificity (Sp), receiver operating characteristic curve, and calculation time were measured for different algorithms (Grey-level of co-occurrence matrix [GLCM], fractal dimension, Hough transform, and speeded-up robust features [SURF]) using the experts’ analysis as reference. Algorithms with highest reproducibility, Se and Sp were then selected for a validation step on the second set of frames. Criteria for validation were κ = 1, Se ≥ 90 %, Sp ≥ 85 %, and a calculation time < 1 second.
Results
Both SURF and GLCM algorithms had high operating points (Se and Sp over 90 %) and a perfect reproducibility (κ = 1). The validation step showed the GLCM detector strategy had the best diagnostic performances, with a Se of 95.79 %, a Sp of 95.19 %, and a calculation time of 0.037 seconds per frame.
Conclusion
A computed algorithm based on a GLCM detector strategy had high diagnostic performance allowing assessment of the abundance of bubbles in SB-CE still frames. This algorithm could be of interest for clinical use (quality reporting) and for research purposes (objective comparison tool of different preparations).
Introduction
Capsule endoscopy (CE) has had a major influence in small bowel (SB) exploration since its inception in 2000 1 . The SB is seen entirely in over 80 % of CE procedures. The diagnostic yield of SB-CE is approximately 60 % in the setting of obscure gastrointestinal bleeding (OGIB), and 50 % in suspected Crohnʼs disease 2 .
Residues, debris, bile, chyme, and bubbles may decrease the diagnostic yield by impairing mucosal visualization. Prior SB preparation by oral purge seems to improve the visibility of the mucosa as well as the completion rate 3 4 . However, its effect on bubbles residing in the SB lumen is unknown.
In the setting of colonoscopy, the Boston Bowel Preparation Scale allows an adequate report on whether the colonic mucosa is appropriately visualized during the procedure 5 . However, there is no validated cleansing score in SB-CE, which would allow determination of whether the procedure is reliable. Consequently, a reliable evaluation of SB mucosal cleansing is difficult, and the level of evidence for efficacy of any SB-CE preparation remains low.
Attempts have been made to develop a computed SB cleansing score. Many of these scores are based on a colorimetric index, such as the red on green ratio 6 7 . For instance, Van Weyenberg et al. 6 published the first study using a computed quantitative scale to assess mucosal visibility during SB-CE, based on a colorimetric index of the tissue color bar. Although the scale was promising, presence of bubbles was not taken into account in that study. It has been suggested that anti-bubble agents, such as simethicone, given in a liquid form (80 mg to 600 mg), 20 minutes before capsule ingestion, may enhance mucosal visualization in SB-CE. However, these agents do not significantly increase the procedure’s diagnostic yield 4 8 9 10 11 12 13 . Moreover, validated methods to assess the amount of bubbles in CE recordings are lacking, which implies that data on anti-bubble agents are from low-quality evidence. Studies on SB cleaning scores suggest that grading scales should focus on quantitative rather than qualitative criteria to achieve better reproducibility. Therefore, we believe that an objective, reproducible score assessing the amount of bubbles in SB-CE is needed for both clinical practice and research purposes 14 .
The aim of this study was to develop and validate a computed method, which would allow assessment of the abundance of bubbles covering the surface of still images.
Patients and methods
Inclusion criteria
Eligible participants presented with OGIB, indicating the need for a SB-CE procedure. SB-CE videos were edited so that only the part between the first image of the duodenum and the last one of the ileum was kept for analysis. The videos were then converted into mpeg files and included in the study.
Exclusion criteria
Patients were excluded if the SB-CE was a first- or a second-generation capsule, if the procedure was incomplete, or if lesions of any kind were observed.
SB-CE procedure
Bowel preparation consisted of a clear liquid diet on the day prior to the procedure, followed by split ingestion of 1.5 L of polyethylene glycol-electrolyte (PEG) lavage solution: 1 L the evening before and 0.5 L on the morning of the procedure day. Metoclopramide (10 mg) could be administered orally if the capsule was delayed in the stomach (> 1 hour) 15 . The procedure was complete when the capsule was expelled into the cecum. The third-generation capsule system used in this study consisted of the ingestible SB3 (PillCam, Medtronic, Minnesota, United States).
Image databases
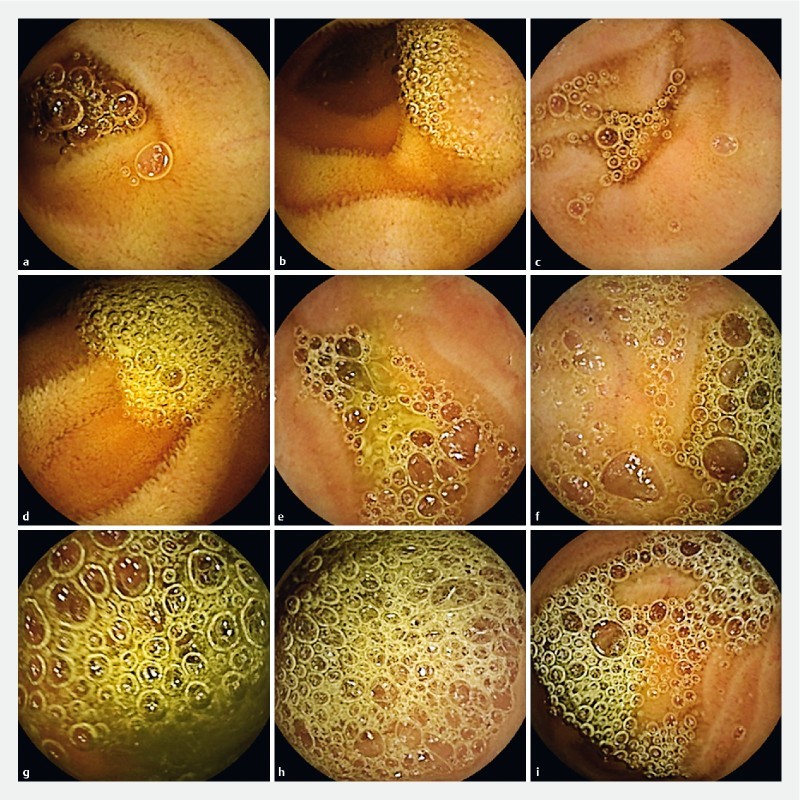
The first dataset was created using 200 SB-CE separate, non-consecutive, and non-clustered still frames exported from 45 SB-CE video sequences. The dataset was divided into five groups consisting of 40 still frames each. Each group was created based on the surface of mucosa (in percentage) that could not properly be examined because it was covered with bubbles. This first analysis was performed by OP. Group A comprised still frames with less than 2 % bubbles, group B comprised still frames with 2 % to 10 % bubbles, group C comprised still frames with 10 % to 25 % bubbles, group D comprised still frames with 25 % to 50 % bubbles, and group E comprised still frames with 50 % to 100 % bubbles. Fig. 1 and Fig. 2 show the variety of bubble abundance on different still frames. The 200 still frames were shuffled and analyzed by two experienced readers (CF, XD), blinded to the results of all the computed analysis performed on these still frames. The expert readers had previously analyzed over 500 SB-CE procedures. This review was performed twice for all 200 still frames, in random order. Each still frame was categorized based on the estimated percentage of bubbles covering the image (whether these bubbles were large or small and numerous or few), with a 10 % threshold. 16 17 . Still frames presenting with fewer than 10 % bubbles were classified as “scarce in bubbles”. Conversely, still frames presenting with 10 % or more bubbles were classified as “abundant in bubbles”. In cases of discrepancy after initial analysis (still frame classified twice as “scarce in bubbles,” and twice as “abundant in bubbles”), an agreement was reached between the two readers and the still frame categorized. A second dataset was created using 200 different separate, non-consecutive, and non-clustered SB-CE still frames, divided into five groups and subsequently analyzed using the same process.
Fig. 1.

Set of still frames categorized in the “scarce in bubbles” group, according to expert analysis. Images a , b and c represent still frames with less than 2 % of bubbles. Images d , e and f represent still frames with 2 to 10 % of bubbles.
Fig. 2.
Set of still frames categorized in the “abundant in bubbles” group, according to expert analysis. Images a , b and c represent still frames with 10 to 25 % of bubbles. Images D, E and F represent still frames with 25 to 50 % of bubbles. Images g , h and i represent still frames with 50 to 100 % of bubbles.
Computed algorithms
Four different computed algorithms, recognizing circular patterns, were tested in terms of their ability to adequately categorize each still frame based on the amount of bubbles, lower or higher than 10 % (i. e. in the “scarce in bubbles” or “abundant in bubbles” groups) using a similar binary classification. These tests were performed using the MATLAB software (MathWorks, Natick, Massachusetts, United States). The four algorithms were divided into two groups, depending on the type of results generated. The first group included two feature-based methods, since the output of each method (“scarce in bubbles” or “abundant in bubbles”) depended on a computed threshold, based on a particular characteristic of the image. The second group included two methods allowing quantification of the actual surface of the still frame presenting with bubbles. Each still-frame was categorized (“scarce in bubbles” or “abundant in bubbles”) using the same bubble abundance threshold of 10 %.
Group 1: Feature-based methods
The first algorithm (algorithm 1) was based on the contrast computed from the Grey Level Co-occurrence matrix (GLCM) of the still frame. Classic, easy-to-compute, textural features with good discrimination capacities were obtained using parameters extracted from the GLCM of a greyscale image. Element i,j of the 256 × 256 matrix of an 8-bit image (presenting with 256 grey levels for luminance) presents a high value when neighboring pixels of the same i,j value consistently appear in the considered image. Usually, this is the horizontal-right pixel with a distance of 1 pixel, which is considered to compute the matrix. From this matrix, we computed the contrast parameter of good discrimination capacity when considering repetitive texture-like bubbles. Overall, algorithm 1 was a threshold-based algorithm: first the contrast from GLCM of each still frame was computed, then a threshold of contrast value was applied to decide whether bubbles were present in a significant manner or not.
The second algorithm (algorithm 2) was based on similar principles, but the fractal dimension (FD) was used as a texture parameter instead of the GLCM contrast. The FD of an image strongly depends on replication of a unique pattern, at different scales, in an infinite way, to form a signal or an image-like small replicative bubbles texture. Algorithm 2 is also threshold-based: still frames were categorized based on presence of bubbles in a significant manner or not, depending on the FD of these still frames.
Group 2: Surface-based methods
The principle of surface-based methods is to quantify the actual surface of the still frame covered with bubbles and to compare the obtained results with the expert readers’ binary classification.
The third algorithm (algorithm 3) was based on a Hough transform (HT) 18 , which recognizes various geometrical forms, including circles, in digital images. HT increases the probability of identifying pixels within an image (contour), which would be the center C of a circle with a radius R, using gradient information, computed with a classic edge filter strategy, such as Canny filter. In our study, intervals for R values were chosen in accordance with the usual size of a bubble, constrained to a maximum value of one-third of the still frame width. Once circles are detected, they are used to compute the corresponding surface within the still frame.
The fourth algorithm (algorithm 4) was based on a speeded-up robust features (SURF) detector strategy 19 . The principle is to extract saliency points (also known as SURF points) from the grey-level image, assuming that the geometry of a bubble and the texture of the circular surrounding environment (for a given radius R) leads to a significant increase in number of SURF points when compared to a “normal” area. When the amount of surrounding SURF points is above a given, manually tuned threshold, a saliency point is considered to belong to a bubble.
Each still frame was categorized as “scarce in bubbles” or “abundant in bubbles” after analysis by all the algorithms, based on the abundance of bubbles (fewer or more than 10 % of bubbles), comparable to the threshold used during the expert analysis.
Statistical analysis
Development step
κ statistics were used to assess interobserver and intraobserver agreements regarding the expert analysis, as well as reproducibility of the algorithmic results. According to standards, κ values between 0.00 and 0.20 indicate poor agreement, κ values between 0.21 and 0.40 indicate fair agreement, κ values between 0.41 and 0.60 indicate moderate agreement, κ values between 0.61 and 0.80 indicate good agreement, κ values between 0.81 and 0.99 indicate excellent agreement, and a κ value of 1.00 indicates perfect agreement 20 .
The first dataset (200 images) was analyzed, using the binary classification (“scarce in bubbles” or “abundant in bubbles” groups) produced by expert readers as reference. Calculation time, receiver operating characteristic (ROC) curve, area under ROC curve (AUROCC), as well as sensitivity (Se), specificity (Sp), negative predictive value (NPV), and positive predictive value (PPV) of the optimal operating point were calculated for all four algorithms by tuning a specific parameter for each individual method (GLCM contrast value, FD value, HT sensitivity, number of SURF points).
Validation step
Algorithms with the best operating point (i. e., the highest sum of Se and Sp) were selected for further validation. Se, Sp, NPV and PPV values were calculated for the selected algorithms applied on the second dataset of 200 still frames (for cross-validation), using the binary classification (“scarce in bubbles” or “abundant in bubbles” groups) produced by two different expert readers (MC and INL) as reference. The primary endpoints for validation were κ = 1, Se ≥ 90 %, and Sp ≥ 85 %. The secondary endpoint was the calculation time by frame < 1 second.
Results
Forty-five eligible patients were included in the study, in order to create both datasets of still frames.
Development step
Concerning the first dataset, intraobserver correlation coefficients were κ = 0.92 for XD and κ = 0.97 for CF. The interobserver correlation coefficient was κ = 0.96 for both expert analyses. The first analysis presented a discrepancy in 13 still frames (6.5 %). Eventually, 90 still frames (45 %) were categorized as “scarce in bubbles” and 110 still frames (55 %) as “abundant in bubbles”. The diagnostic capabilities of all four algorithms are provided in Table 1 . All algorithms achieved a 1.00 intraobserver correlation κ coefficient and a sensitivity of 100 %, but specificity varied substantially. The SURF detector strategy had the highest operating point yielding the following: Se of 94.38 % (95 %CI [91.19 %;97.57 %]), Sp of 97.24 % (95 %CI [94.97 %;99.51 %]), NPV of 95.45 % (95 %CI [92.56 %;98.34 %]), PPV of 96.55 % (95 %CI [94.02 %;99.08 %]), AUROCC of 0.9897, and a calculation time by frame of 11.47 ± 7.11 seconds.
Table 1. Sensitivity, specificity, NPV, PPV, and AUROCC of the four algorithms used to evaluate bubble abundance in small bowel capsule endoscopy still frames.
| Sensitivity | Specificity | NPV | PPV | AUROCC | Calculation time | |
| [95 %CI] | [95 %CI] | [95 %CI] | [95 %CI] | by frame (s, mean ± SD) | ||
| Development step | ||||||
| Algorithm 1: GLCM | 94.38 % [91.19 %;97.57 %] |
93.58 % [90.18 %;96.98 %] |
95.32 % [92.39 %;98.25 %] |
92.31 % [88.62 %;96.00 %] |
0.9852 | 0.040 ± 0.003 |
| Algorithm 2: Fractal dimension |
84.27 % [79.22 %;89.32 %] |
82.57 % [77.31 %;87.83 %] |
86.54 % [81.81 %;91.27 %] |
79.78 % [74.21 %;85.35 %] |
0.9269 | 10.1 ± 0.7 |
| Algorithm 3: Hough transform |
85.39 % [80.49 %;90.29 %] |
81.65 % [79.29 %;87.01 %] |
87.25 % [82.63 %;91.87 %] |
79.17 % [73.54 %;84.80 %] |
0.9252 | 1.45 ± 1.2 |
| Algorithm 4: SURF | 94.38 % [91.19 %;97.57 %] |
97.24 % [94.97 %;99.51 %] |
95.45 % [92.56 %;98.54 %] |
96.55 % [94.02 %;99.08 %] |
0.9897 | 11.47 ± 7.11 |
| Validation step | ||||||
| Algorithm1: GLCM | 95.79 % [93.01 %;98.57 %] |
95.19 % [92.22 %;98.16 %] |
96.12 % [93.44 %;98.80 %] |
94.79 % [91.71 %;97.87 %] |
0.037 ± 0.005 | |
| Algorithm 4: SURF | 94.74 % [91.65 %;97.83 %] |
94.23 % [91.00 %;97.46 %] |
95.15 % [92.17 %;98.13 %] |
93.75 % [90.40 %;97.10 %] |
1.45 ± 1.78 | |
NPV, negative predictive value; PPV, positive predictive value; AUROCC, area under receiver operating characteristic curve; s, seconds; SD, standard deviation; GLCM, Grey-level of co-occurrence matrix; SURF, speeded-up robust features
Fig. 3 shows illustrations of the obtained outputs for algorithms 3 and 4 (whereas no visual illustration can be given for threshold-based algorithms 1 and 2).
Fig. 3.
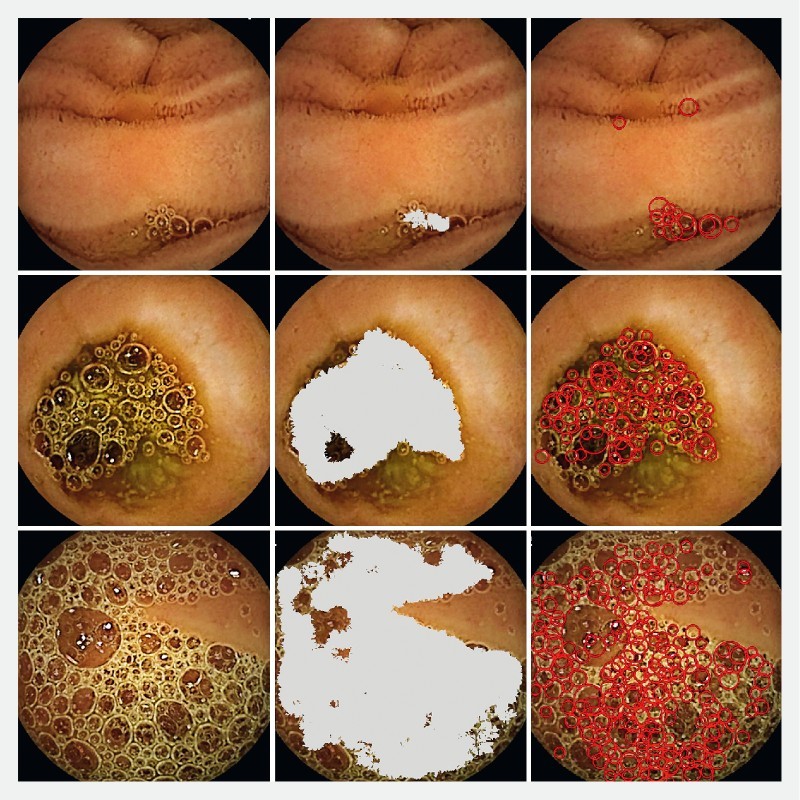
Illustrations of the outputs of surface-based methods for three different frames with various amount of bubbles: native image (left); bubbles detection based on the Grey-level of co-occurrence matrix strategy (algorithm 3, center); C bubbles detection based on the Speeded-Up Robust Features SURF point detection strategy (algorithm 4, right).
The GLCM detector strategy had similar diagnostic capabilities as compared to the SURF detection strategy: Se of 94.38 % (95 %CI [91.19 %;97.57 %]), Sp of 93.58 % (95 %CI [90.18 %; 96.98 %]), NPV of 95.32 % (95 %CI [92.39 %;98.25 %]), PPV of 92.31 % (95 %CI [88.62 %;96.00 %]), AUROCC of 0.9852, and a calculation time by frame of 0.040 ± 0.003 seconds. Both the SURF and GLCM detector strategies were selected for validation ( Fig. 4 ).
Fig. 4.
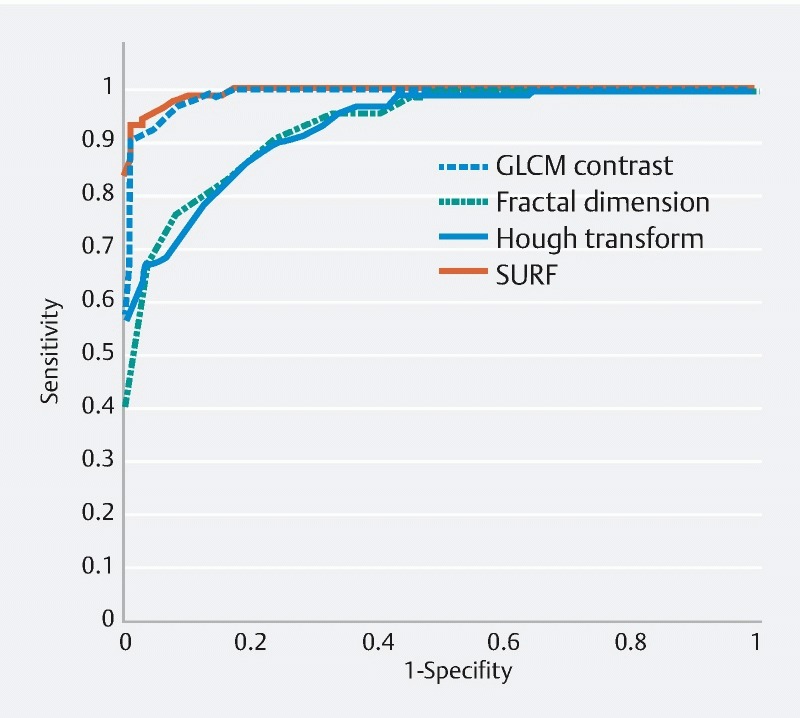
Receiver operating characteristic (ROC) curves of the four used algorithms for evaluation of bubble abundance in small bowel capsule endoscopy still frames (development step).
Validation step
In the second dataset, intraobserver correlation coefficients were κ = 0.96 for both MC and INL. The interobserver correlation coefficient was κ = 0.89 for the first analysis, and κ = 0.88 for the second analysis. The first analysis presented a discrepancy in 68 frames (34 %). Eventually, 96 frames (48 %) were categorized as “scarce in bubbles,” and 104 frames (52 %) as “abundant in bubbles”. Both the SURF and the GLCM detector strategies demonstrated perfect reproducibility (intraobserver correlation κ coefficient of 1.00). The SURF detector strategy had the following diagnostic performances: Se of 94.74 % (95 %CI [91.65 %;97.83 %]), Sp of 94.23 % (95 %CI [91.00 %;97.46 %]), NPV of 95.15 % ( 95 % CI [92.17 %;98.13 %]), PPV of 93.75 % (95 %CI [90.40 %;97.10 %]). The calculation time by frame was 1.45 ± 1.78 s. The GLCM detector strategy had slightly higher diagnostic capabilities: Se of 95.79 % (95 %CI [93.01 %;98.57 %]), Sp of 95.19 % (95 %CI [92.22 %;98.16 %]), NPV of 96.12 % (95 %CI [93.44 %;98.80 %]), PPV of 94.79 % (95 %CI [91.71 %;97.87 %]). The calculation time by frame was significantly lower than that of the SURF detector strategy (0.037 ± 0.005 seconds [ P < 10 –5 ]). The GLCM detector strategy was selected as the best algorithm in terms of diagnostic performances.
Discussion
We selected and validated a computed and comprehensive algorithm, allowing evaluation of the abundance of bubbles in SB-CE still frames, based on GLCM detector strategy. It proved to be perfectly reproducible (κ = 1.00), rapid (0.037 seconds per frame), highly sensitive (95.79 %) and specific (95.19 %).
The main strength of this study is that this algorithm allows reliable assessment of the abundance of bubbles covering the surface of SB-CE still frames. We collected 400 non-clustered images captured by the most available and most recent generation of SB-CE (SB3 PillCam system, Medtronic, Minnesota, United States). These were analyzed twice in random order by two different groups of experienced SB-CE readers blinded to the algorithmic classification. Each individual frame was categorized in a binary manner as “scarce in bubbles” or “abundant in bubbles”. Cross-validation was insured by use of two independent datasets of 200 frames/se for the development and validation phases, respectively.
Establishment of a threshold of bubble abundance for which visualization of the mucosa is significantly impaired is a challenging task. A previous grading system used in three trials was deemed clinically relevant: images with no intraluminal bubble (grade 0) or few gas bubbles (grade 1) were considered as providing no limitation of interpretation 8 9 13 . Based on the figures from these articles and on our clinical experience, we determined that a cutoff of 10 % in terms of bubble abundance on a still frame was adequate. Similarly, the only validated score used to determine the quality of visualization of the mucosa in SB-CE also considers that a visibility over 90 % is optimal 16 17 . Moreover, the chosen threshold was unchanged between the development and the validation steps of the study, for both expert analysis and algorithmic assessment. As this threshold was the same for all steps of the study, comparisons between human reading and electronic evaluation or between the four different algorithms are valid.
One may argue that a limitation of this study was that only normal SB-CE still frames were selected for analysis. However, in daily practice, most SB-CE still frames are normal, even in a video where lesions are visible on only a few still frames. Moreover, we believe that a normal examination is the most critical situation where the quality of bowel preparation should be discussed. When reporting on a normal SB-CE procedure, it is of tremendous importance to be confident in the fact that a reasonable proportion of the mucosal surface was visible throughout the whole length of the SB. In other words, SB-CE reports should clearly mention whether poor quality of preparation impaired mucosal visualization, thus hindering reliability of conclusions.
HT appeared to be a good candidate to build an algorithm, but we also assessed alternative methods. HT is computationally heavy and its processing time can be elevated when considering a large radius research interval and a large number of still frames. Moreover, circle detection sensitivity strongly correlates with the quality of the still frame and the gradient information. Thus, a low gradient level (bubble presenting a low transition intensity with the background) can lead to underestimating the surface of the bubbles. Because local textural descriptors are easy to compute and have a very low computational cost, we decided to assess a SURF one-step strategy (at a pixel level), to detect the surface occupied by bubbles. Global textural feature, such as GLCM contrast, can also provide qualitative assessment of the actual surface with bubbles within the still frame, and was expected to be a good binary estimator of bubble abundance in correlation with the physicians’ visual study. The development phase showed the sensitivity of the GLMC algorithm was exactly the same as that of SURF, but the specificity of SURF was higher and the calculation time of GLCM was lower. Both algorithms, therefore, were selected for validation. GLCM eventually demonstrated higher diagnostic capabilities with significantly lower calculation time during the validation phase.
Our algorithm, based on the GLCM detector strategy, could also be useful in allowing objective evaluation of anti-bubble agents in SB-CE preparation regimens. Up to now, evaluation of the effect of anti-foaming agents on the abundance of bubbles in prospective studies has been based on expert analysis, with good – but not always excellent – agreement between experts 4 8 9 10 11 12 13 . When reported, intercorrelation coefficients (κ or Spearman coefficients) ranged from 0.61 to 0.92 when evaluating 1-hour videos 8 9 13 , and from 0.75 to 0.90 in 1-minute videos 11 . Our study demonstrates that intercorrelation coefficients are even higher (varying between 0.88 and 0.96) when experts analyze individual still frames (and not entire videos). All in all, computed algorithms allow a comprehensive evaluation (each individual frame of the SB-CE procedure is analyzed) with perfect reproducibility (i. e., intraobserver correlation). Therefore, we believe that this computed algorithm, with perfect reproducibility and high sensitivity and specificity, could be used in future prospective trials (or on archived videos from already performed prospective trials) in an objective manner (frame-by-frame evaluation) with very high performance.
Also, the GLCM detector strategy could be combined with other criteria for evaluating SB-CE cleansing. For instance, colorimetric indexes (red/green ratio) have been used in several studies to quantify chime residues, which hinder evaluation of the mucosal surface 6 7 20 . We first aim to electronically define what an “appropriately cleansed still frame” is. In future studies, our goal is to develop a computed score to assess quality of SB preparation for complete SB-CE procedures. Such a tool would be of great interest in clinical practice as it would allow reliable reporting of the quality of preparation (much like the Boston Bowel Preparation Scale score in the setting of colonoscopy). Moreover, it would be helpful in clinical research, to help compare efficacy of different preparation regimens.
Conclusion
In conclusion, this study showed that a computed algorithm based on the GLCM detector strategy has a perfect reproducibility, a high diagnostic sensitivity (95.79 %) and specificity (95.19 %), and is a rapid method of analysis (0.037 seconds per frame), for assessment of the abundance of bubbles on SB-VCE still frames. It proved to be a powerful tool to differentiate still frames with a low amount of bubbles from those with more than 10 % bubbles. This algorithm could be implemented in SB-CE reading software and used automatically for evaluation of anti-bubble agents. In the future, we aim to develop a computed SB-CE cleaning score with the help of this algorithm. Such a score would be of great interest in the fields of clinical practice and research.
Footnotes
Competing interests Pr Dray has acted as a consultant for Boston Scientific, Fujifilm, Medtronic and Pentax.
References
- 1.Iddan G, Meron G, Glukhovsky A et al. Wireless capsule endoscopy. Nature. 2000;405:417. doi: 10.1038/35013140. [DOI] [PubMed] [Google Scholar]
- 2.Pennazio M, Spada C, Eliakim R et al. Small-bowel capsule endoscopy and device-assisted enteroscopy for diagnosis and treatment of small-bowel disorders: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2015;47:352–376. doi: 10.1055/s-0034-1391855. [DOI] [PubMed] [Google Scholar]
- 3.Yung D E, Rondonotti E, Sykes C et al. Systematic review and meta-analysis: is bowel preparation still necessary in small bowel capsule endoscopy? Expert Rev Gastroenterol Hepatol. 2017;11:979–993. doi: 10.1080/17474124.2017.1359540. [DOI] [PubMed] [Google Scholar]
- 4.Koulaouzidis A, Iakovidis D K, Karargyris A et al. Optimizing lesion detection in small-bowel capsule endoscopy: from present problems to future solutions. Expert Rev Gastroenterol Hepatol. 2015;9:217–235. doi: 10.1586/17474124.2014.952281. [DOI] [PubMed] [Google Scholar]
- 5.Lai E J, Calderwood A H, Doros G et al. The Boston bowel preparation scale: a valid and reliable instrument for colonoscopy-oriented research. Gastrointest Endosc. 2009;69:620–625. doi: 10.1016/j.gie.2008.05.057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Van Weyenberg S JB, De Leest H TJI, Mulder C JJ. Description of a novel grading system to assess the quality of bowel preparation in video capsule endoscopy. Endoscopy. 2011;43:406–411. doi: 10.1055/s-0030-1256228. [DOI] [PubMed] [Google Scholar]
- 7.Abou Ali E, Histace A, Camus A et al. Development and validation of a highly sensitive and highly specific computed assessment of cleansing score for small bowel capsule endoscopy. United European Gastroenterol J. 2016;4:A604. [Google Scholar]
- 8.Albert J, Göbel C M, Lesske J et al. Simethicone for small bowel preparation for capsule endoscopy: a systematic, single-blinded, controlled study. Gastrointest Endosc. 2004;59:487–491. doi: 10.1016/s0016-5107(04)00003-3. [DOI] [PubMed] [Google Scholar]
- 9.Wu L, Cao Y, Liao C et al. Systematic review and meta-analysis of randomized controlled trials of Simethicone for gastrointestinal endoscopic visibility. Scand J Gastroenterol. 2011;46:227–235. doi: 10.3109/00365521.2010.525714. [DOI] [PubMed] [Google Scholar]
- 10.Fang Y H, Chen C X, Zhang B L. Effect of small bowel preparation with simethicone on capsule endoscopy. J Zhejiang Univ Sci B. 2009;10:46–51. doi: 10.1631/jzus.B0820148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Spada C, Riccioni M E, Familiari P et al. Polyethylene glycol plus simethicone in small-bowel preparation for capsule endoscopy. Dig Liver Dis. 2010;42:365–370. doi: 10.1016/j.dld.2009.07.017. [DOI] [PubMed] [Google Scholar]
- 12.Rosa B J, Barbosa M, Magalhaes J et al. Oral purgative and simethicone before small bowel capsule endoscopy. World J Gastrointest Endosc. 2013;5:67–73. doi: 10.4253/wjge.v5.i2.67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Papamichael K, Karatzas P, Theodoropoulos I et al. Simethicone adjunct to polyethylene glycol improves small bowel capsule endoscopy imaging in non-Crohnʼs disease patients. Ann Gastroenterol. 2015;28:464–468. [PMC free article] [PubMed] [Google Scholar]
- 14.Keuchel M, Kurniawan N, Baltes P et al. Quantitative measurements in capsule endoscopy. Comput Biol Med. 2015;65:333–347. doi: 10.1016/j.compbiomed.2015.07.016. [DOI] [PubMed] [Google Scholar]
- 15.Koulaouzidis A, Giannakou A, Yung D E et al. Do prokinetics influence the completion rate in small-bowel capsule endoscopy? A systematic review and meta-analysis. Curr Med Res Opin 2013 Sep. 29:1171–1185. doi: 10.1185/03007995.2013.818532. [DOI] [PubMed] [Google Scholar]
- 16.Brotz C, Nandi N, Conn M et al. A validation study of 3 grading systems to evaluate small-bowel cleansing for wireless capsule endoscopy: a quantitative index, a qualitative evaluation, and an overall adequacy assessment. Gastrointest Endosc. 2009;69:262–270. doi: 10.1016/j.gie.2008.04.016. [DOI] [PubMed] [Google Scholar]
- 17.Klein A, Gizbar M, Bourke M J et al. Validated computed cleansing score for videocapsule endoscopy. Dig Endosc. 2016;28:564–569. doi: 10.1111/den.12599. [DOI] [PubMed] [Google Scholar]
- 18.Hough P VC.Method and Means for Recognizing Complex Patterns US Patent 3,069,6541962. Ser. No. 17,7156 Claims
- 19.Vilarino F, Malagelada C, Azpiroz F et al. Categorization and segmentation of intestinal content frames for wireless capsule endoscopy. IEEE Trans Inf Technol Biomed. 2012;16:1341–1352. doi: 10.1109/titb.2012.2221472. [DOI] [PubMed] [Google Scholar]
- 20.Landis J R, Koch G G. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174. [PubMed] [Google Scholar]