

Abstract
Objective
Social interaction quality is related to cardiovascular functioning. Trait emotional reactivity may amplify cardiovascular responses to social interactions, but is often examined as a tendency to react to negative events. We took a broader approach by examining the joint effects of positive and negative emotional reactivity and social interaction quality on ambulatory blood pressure (ABP) and heart rate (HR) responses to daily social interactions.
Methods
Participants were part of a larger study on BP and cardiovascular health (N = 805; MAge = 45.3; 40.1% male). Participants completed a measure of emotional reactivity (BIS/BAS) and 24-hour ABP monitoring accompanied by ecological momentary assessments (EMA) about just-experienced social interactions and their pleasantness. Multilevel models tested the associations of emotional reactivity, average pleasantness, and momentary pleasantness with BP and HR.
Results
Participants who reported more pleasant interactions on average had lower BP (systolic BP: B = −.51 mmHg; diastolic BP: B = −.46 mmHg). These effects did not depend on emotional reactivity. The effect of momentary pleasantness depended on BIS/BAS; in less reactive participants, greater pleasantness was associated with lower HR, B = −.13 bpm; in more reactive participants, greater pleasantness was associated with increased HR, B = .16).
Conclusions
Participants who had more pleasant social interactions throughout the day had lower mean ABP. The acute effect of a given social interaction on HR depended on emotional reactivity: HR increased for participants high in emotional reactivity during pleasant interactions. Thus, emotional reactivity may influence cardiovascular responses to social stimuli.
Keywords: social interactions, ambulatory blood pressure, emotional reactivity, ecological momentary assessment
Social interactions have a significant impact on cardiovascular health. Negative social interactions such as argumentative exchanges predict increased risk for cardiovascular disease and incident coronary events (De Vogli, Chandola, & Marmot, 2007; Ross, Martin, Chen, & Miller, 2011). Conversely, positive aspects of relationships such as social support and affiliation predict a lower incidence of coronary heart disease (Ruiz, Hutchinson, & Terrill, 2008; Smith, Baron, & Grove, 2014) and lower mortality among congestive heart failure patients (Coyne et al., 2001).
The effects of social interactions on cardiovascular outcomes may emerge as cumulative consequences of repeated interactions over days, weeks, and months. These physiological mechanisms can be observed most precisely at the level of a given interaction. The emotional quality of an interaction, for example, reliably alters blood pressure. Interactions with a romantic partner or close other are associated with lower ambulatory blood pressure (Gump, Polk, Kamarck, & Shiffman. 2001; Holt-Lunstad, Uchino, Smith, Olson-Cerny, & Nealey-Moore, 2003), whereas interactions with a partner toward which one has ambivalent feelings are associated with higher blood pressure throughout the day (Holt-Lunstad et al., 2003). More broadly, social interactions that are seen as unpleasant predict greater increases in blood pressure (Brondolo et al., 2003). This pattern suggests that unpleasant, uncomfortable, or stressful interactions can be detrimental for heart health, whereas pleasant or comfortable interactions can be beneficial (Zanstra & Johnston, 2011).
Yet the cardiovascular effects of social interactions are not the same for everyone. Rather, people with different dispositions react to social stimuli in different ways, and the way in which someone tends to react emotionally may shape acute physiological responses to social situations. This possibility is highlighted by research showing that individual differences in emotional responding, such as the tendency to react with hostility, affects blood pressure during social interactions (Smith & Gallo, 1999; Vella, Kamarck, & Shiffman, 2008). For instance, interactions perceived as intimate may lead to lower blood pressure, but only for individuals low in hostility (Vella et al., 2008). Threatening situations may increase blood pressure in particular for high-hostility individuals (Smith & Gallo, 1999), and social interactions that are high in instrumental support may increase blood pressure for high-hostility people (Vella et al., 2008), ostensibly because they do not want “help.” Hostility may also exacerbate increases in blood pressure during emotionally intense encounters (Brondolo et al., 2003).
A person’s emotional reactivity to pleasant and unpleasant stimuli and situations may be especially important in social contexts. Highly reactive people may over-respond to social pleasantness or unpleasantness cues, which may increase stress on the cardiovascular system through heightened blood pressure variability (Parati, Pomidossi, Albini, Malaspina, & Mancia, 1987; Stergiou et al., 2014; Stevens et al., 2016). Indeed, individuals who are more variable in negative emotion throughout the day also experience higher blood pressure in response to negative emotions (Carels, Blumenthal, & Sherwood, 2000). Emotional reactivity may be an especially potent moderator when considering how blood pressure is affected by acute changes in relative pleasantness (versus differences in average level of pleasantness). Reactivity entails reacting to a situation at hand, and therefore it should ostensibly be more relevant for shaping cardiovascular responses to momentary fluctuations in pleasantness than for influencing a person’s average blood pressure/heart rate during a generally pleasant or unpleasant day.
Emotional reactivity is a broadly defined concept pertaining to typical responses to emotion-eliciting stimuli and situations. A majority of research on this construct has focused on negative affect (e.g., “upset,” “agitated,” “anxious”) in response to unpleasant events, and this is reflected in many of the psychometric assessments designed to quantify emotional reactivity (e.g., Nock, Wedig, Holmberg, & Hooley, 2008). Yet positive affect in response to pleasant events is also an important dimension of emotional reactivity.
Because measures to assess emotional reactivity generally focus solely on reactivity to negative events, alternative approaches are warranted. Although the BIS/BAS questionnaire was originally developed to measure two aspects of personality pertaining to avoidance and approach dimensions of motivation (Carver & White, 1994), and is therefore usually treated as separate subscales, it is possible to conceptualize this scale as a single total score measuring individual differences in emotional reactivity across positive and negative domains (see also Claes et al., 2010; Claes, Vertommen, Smits, & Bijttebier, 2009). The BIS/BAS encompasses two dimensions: behavioral inhibition sensitivity (BIS) (e.g., “Criticism or scolding hurts me quite a bit”), and behavioral activation sensitivity (BAS) (e.g., “When I get something I want, I feel excited and energized”). Items on the BIS/BAS have been shown to be related to both negative and positive affect (Heubeck et al., 1998). BIS is measured by a single subscale, and is associated with greater self-reported unpleasant emotion and a higher tendency to engage in rumination (Leen-Feldner et al., 2004), whereas BAS consists of three subscales related to pleasant emotion(s) and appetitive motivation: reward responsiveness, fun-seeking, and drive. BAS has been associated with some adaptive outcomes such as lower depressive symptoms (McFarland et al., 2006), but has also been associated with adverse emotional, behavioral, and health outcomes. For example, higher reward responsiveness is associated with impulsive buying (Claes et al., 2010), and fun-seeking is associated with greater alcohol use and symptoms of mania among college students (Franken & Muris, 2006; Meyer, Johnson, & Carver, 1999). Furthermore, although there is strong evidence that negative affect is reliably associated with BIS (Heubeck et al., 1998), BAS has sometimes also been associated with negative affect (e.g., reward responsiveness is associated with heightened frustration; Carver, 2004).
This study explored the intersection of social context (both pleasantness of social interactions on average and fluctuations in pleasantness within the day) and individual differences in emotional reactivity as they relate to ambulatory blood pressure and heart rate in real time and in individuals’ naturalistic context. Given previous research showing exaggerated responses to unpleasant emotional or social stimuli amongst individuals who are higher in hostility or negative emotions (e.g., Carels et al., 2000; Smith & Gallo, 1999; Vella et al., 2008), we hypothesized that more emotionally reactive people would experience greater changes in blood pressure and heart rate in response to the pleasantness (or unpleasantness) of interactions.
We had two hypotheses. First, greater pleasantness in social interactions—both on average and relative to average (i.e., more or less pleasant than usual)—is associated with lower blood pressure and heart rate. Second, participants who are high in emotional reactivity will exhibit exaggerated changes in blood pressure and heart rate across the range of pleasantness in social interactions relative to participants low in emotional reactivity. Although we were primarily interested in emotional reactivity towards both negative and positive stimuli, it is possible that these associations may differ for participants who are reactive to unpleasant situations (i.e., high versus low BIS) and participants who are reactive to pleasant situations (i.e., high versus low on BAS subscales). As such, in addition to testing the moderating effects of the total BIS/BAS score, we explored potential moderating effects of each of the four subscales. Although we initially hypothesized that blood pressure and heart rate responses to social interactions would be similar, we were sensitive to the possibility that this might not be true. For example, Brosschot et al. (2014) found that induction of negative emotion influenced blood pressure recovery, but not heart rate recovery, after a stressor.
Method
Participants
Participants (N = 805) were part of a larger study on the correlates of and cardiovascular sequelae of masked hypertension (Masked Hypertension Study; see Schwartz et al., 2016 for further details and CONSORT information). Initial inclusion criteria included: 1) 21 years of age or older, 2) working at least 17.5 hours per week, 3) able to speak and read English, 4) pre-enrollment screening blood pressure of less than 160/105 mmHg, and 5) not taking blood pressure-lowering medication. Participants were excluded if they reported a history of cardiovascular disease (e.g., myocardial infarction), or chronic renal, liver, thyroid, or adrenal disease, cancer that was not in remission for at least six months, and active substance abuse or a serious mental health illness. Participants were also excluded if they had evidence of secondary hypertension. Finally, those taking any cardiovascular medication other than a statin and pregnant women were excluded. This study was approved by the Columbia University Medical Center and Stony Brook University Institutional Review Boards.
To be included in the analyses reported here, participants needed to have reported having had at least one social interaction “just prior” to a blood pressure reading; this question was asked first, and, if the participant indicated no interaction, it was followed by a question asking about “any” interaction since the last reading. We included only interactions “just prior” to the ABP reading, given that “any” interaction might have occurred up to 28–30 minutes prior, and therefore results would not reflect the acute/momentary effect of social interactions on ABP and HR. We acknowledge that we could examine the possibility of protracted and/or delayed effects of social interactions on BP and HR, but that would be secondary to our primary focus. Because the presence/absence of social interactions was only assessed for awake readings, all sleep readings were excluded from the analysis.
Procedure
Participants were recruited from workplace blood pressure screenings between 2005–2011. After determining eligibility, participants completed informed consent. Participation consisted of five visits to our clinic setting. Relevant to this study, at the first visit, participants received a psychosocial questionnaire including the assessment of emotional reactivity. This was returned prior to the third visit, at which participants were fitted with an ambulatory blood pressure monitor and trained in the use of an electronic diary to complete ecological momentary assessments (EMAs). Blood pressure readings were taken every 28–30 minutes, after which participants completed an EMA diary entry assessing a variety of situational factors (e.g., posture, location, recent social interaction), for the next 24 hours while going about their daily life during a normal workday.
Measures
BIS/BAS Scale
Emotional reactivity was measured using a 20-item version of the BIS/BAS Scale (Carver et al., 1994). A total emotional reactivity score (Cronbach’s α = .81) was computed as the sum of all 20 items that contribute to the four subscales such that a higher total emotional reactivity score represented greater reactivity to both positive and negative stimuli. The four subscales are: BIS (sum of seven items, e.g., “Criticism or scolding hurts me quite a bit”; Cronbach’s α = .77), BAS reward responsiveness (five items, e.g., “When I get something I want, I feel excited and energized”; Cronbach’s α = .84), BAS drive (four items, e.g., “When I want something I usually go all-out to get it”; Cronbach’s α = .82), and BAS fun-seeking (four items, e.g., “I crave excitement and new sensations”; Cronbach’s α = .78). Items were summed so that each subscale represented higher levels of emotional reactivity (e.g., higher BIS score represented greater behavioral inhibition, higher BAS reward responsiveness score represented greater reward responsiveness).
Social interaction pleasantness
At each blood pressure reading, participants were asked if they had just had a social interaction (yes or no), and to rate the pleasantness of the social interaction using a visual analog scale (VAS), translated into a numeric score between 0 and 100) with anchors of unpleasant (extreme left), neutral (center), and pleasant (extreme right). To aid in interpretability of results, these scores were divided by 10 so that the scale ranged from 0 to 10.
Pleasantness was decomposed into two separate components: average pleasantness of social interactions (between-persons, or the average pleasantness reported by each individual during that 24 hours) and momentary fluctuations in pleasantness (within-person, or the relative pleasantness of a given interaction in relation to that participant’s average pleasantness). Momentary fluctuations in pleasantness were person-centered around each participant’s average pleasantness of social interaction. For example, if a participant reported a pleasant interaction of 7.0 and had an average pleasantness of 8.2, the relative pleasantness of that interaction would be −1.2 (i.e., it is less pleasant than usual).
Blood pressure and heart rate
Ambulatory blood pressure readings were taken automatically for 24 hours using a portable blood pressure monitor (SpaceLabs, Model 90207, Snoqualmie, WA, US) placed on the non-dominant arm. Additional details are described in Schwartz et al. (2016).
Data Analysis Strategy
Multilevel models were estimated using the MIXED procedure in SAS, with an error structure that treats between-person differences in level of BP/HR as a random effect and allows for serial autocorrelation among consecutive BP/HR readings. This structure provides a flexible and effective way to account for individual variability and greater similarity between ABP readings that were taken closer in time to each other (see Schwartz & Stone, 2007 for details on specifying error structures for real-time data). Both emotional reactivity and average pleasantness were grand mean centered prior to analysis.
After testing significance of random effects (i.e., individual differences in intercept and the within-person effect of relative pleasantness) using deviance comparison tests, two models were run for each outcome (systolic blood pressure [BP], diastolic BP, and heart rate [HR]). In the first model, the main effects of average reported pleasantness of all social interactions during the awake portion of the 24-hour monitoring period, the relative pleasantness of the current/recent social interaction, and emotional reactivity were examined. In the second model, multiplicative interaction terms for emotional reactivity with average and relative pleasantness were added in order to test whether the effect of the latter differs according to the participant’s emotional reactivity. Secondary analyses examined the four BIS/BAS subscales separately to test whether the findings were specific to a given subscale.
For the models outlined above, estimates were adjusted for demographic factors (age, race, ethnicity, gender, and BMI) and momentary factors known to affect ABP (posture, location, physical exertion, temperature, and recent meal, caffeine, alcohol, or nicotine consumption) (e.g., Brondolo et al., 2003; Holt-Lunstad et al., 2003; Schwartz, Warren, & Pickering, 1994).
Results
Participants were a mean of 45.3 years old (SD = 10.3) and were predominantly female (59.9%; 40.1% male). Participants were majority non-Hispanic white (70.9%); only 6.8% were Black, and 11.4% Hispanic. Participants most often reported (38.6%) receiving some graduate training, followed by a bachelor’s degree (27.7%), some college or a vocational degree (26.0%), and high school or less (7.7%). Participants most often reported a family income of $100,000–$149,999 (44.6%), followed by ≥ $150,000 (28.3%), $50,000–$99,999 (15.8%), and < $50,000 (11.3%).
Significant correlations among BIS/BAS subscales were low to moderate in magnitude (see Table 1 for means, standard deviations, and correlations for the BIS/BAS). Participants had an average of 24.6 valid awake ABP readings accompanied by a concurrent EMA assessment (SD = 7.4) during the 24-hour monitoring period; the average number of times an interaction just prior to the ABP reading was reported was 13.9 (SD = 6.5). Daily interactions were on average rated as pleasant (M = 68.9, SD = 13.1, on original 100-point scale). Mean systolic BP was 123.9 (SD = 13.1); diastolic BP, M = 78.3, SD = 10.2; HR, M = 77.2, SD = 12.8. Preliminary nested deviance comparison tests showed that the random intercept was significant for systolic BP, diastolic BP, and HR. The random effect for relative pleasantness was statistically significant for systolic BP and HR, ps < .05, but not for diastolic BP, p = .14. Because we were primarily interested in the interaction effect of relative pleasantness with emotional reactivity on BP and HR, however, we left the random effect in the model. Interaction models for emotional reactivity predicting systolic BP, diastolic BP, and HR, including coefficients for covariates are reported in Table 2.1 Full results for systolic BP, diastolic BP, and HR across subscales are shown in Tables 3, 4, and 5, respectively.
Table 1.
Correlations among BIS/BAS subscales. Means (SDs) are on the diagonal.
| BIS | BAS – RR | BAS – FS | BAS – D | |
|---|---|---|---|---|
| Behavioral Inhibition (BIS) | 19.34 (3.25) |
|||
| Behavioral Activation – Reward Responsiveness (BAS – RR) |
.16** | 16.23 (2.23) |
||
| Behavioral Activation – Fun-Seeking (BAS – FS) |
−.03 | .31** | 10.20 (2.16) |
|
| Behavioral Activation – Drive (BAS – D) | −.01 | .37** | .35** | 9.92 (2.13) |
p < .10,
p < .05,
p < 01
Table 2.
Interaction models for systolic BP, diastolic BP, and HR, with covariate estimates reported.
| Systolic BP | Diastolic BP | HR | ||
|---|---|---|---|---|
|
| ||||
| B | B | B | ||
| Intercept | 125.29** | 78.97** | 96.90** | |
| Age | .22** | .10** | −.06+ | |
| Male | 6.33** | 4.57** | −3.01** | |
| Hispanic | −2.27* | −.44 | .29 | |
| Black | 1.50 | .61 | −.08 | |
| BMI | .42** | .02 | .33** | |
| Posture | Reclining | −3.94+ | −7.66** | −15.77** |
| Sitting | −.61 | −2.40 | −11.47** | |
| Standing | 2.19 | .91 | −5.94** | |
| Walking | 2.59 | −.60 | −5.36** | |
| Running | – | – | – | |
| Exertion | None | −3.02* | −.01 | −7.01** |
| Light | −2.05 | .24 | −5.46** | |
| Moderate | −1.22 | .14 | −1.81 | |
| Heavy | – | – | – | |
| Temperature | Comfortable | .13 | .24 | −2.73** |
| Too Cold | 1.39* | 1.35* | −3.50** | |
| Too Hot | – | – | – | |
| Location | Home | .3.35 | −2.61** | −.76* |
| Work | −1.58 | −.68** | −.98** | |
| Other | – | – | – | |
| Meal | .20** | .40* | 1.62** | |
| Caffeine | .01 | −.15 | .548 | |
| Alcohol | 1.53* | 1.81** | .69 | |
| Nicotine | 1.57* | .83 | 3.29** | |
| Day-Level Pleasantness | −.51* | −.47* | −.26 | |
| Relative Pleasantness | −.14** | −.02 | −.01 | |
| Reactivity | .03 | −.01 | .00 | |
| Day-Level × Reactivity | −.01 | −.04 | .01 | |
| Relative × Reactivity | .01 | .00 | .02** | |
p < .10,
p < .05,
p < .01
BP: blood pressure, BIS: behavioral inhibition sensitivity, BAS: behavioral activation sensitivity
Table 3.
Systolic BP predicted by day-level pleasantness, relative pleasantness, and total BIS/BAS score or individual facets of the BIS/BAS.
| Emotional Reactivity | BIS | BAS – Reward Responsiveness | BAS – Fun Seeking | BAS – Drive | ||
|---|---|---|---|---|---|---|
|
| ||||||
| B | B | B | B | B | ||
| Main Effects Model | Intercept | 125.30** | 125.35** | 125.31** | 125.31** | 125.33** |
| Day-Level Pleasantness | −.51* | −.52* | −.52* | −.53* | −.51* | |
| Relative Pleasantness | −.13* | −.13* | −.13* | −.13* | −.13* | |
| Reactivity | .03 | −.03 | .07 | .17 | .10 | |
|
| ||||||
| Interaction Model | Intercept | 125.29** | 125.33** | 125.33** | 125.29** | 125.29** |
| Day-Level Pleasantness | −.51* | −.51+ | −.53* | −.53* | −.53* | |
| Relative Pleasantness | −.14** | −.14* | −.14* | −.13* | −.13* | |
| Reactivity | .03 | −.04 | .06 | .17 | .10 | |
| Day-Level × Reactivity | −.01 | .03 | .02 | .06 | −.22+ | |
| Relative × Reactivity | .01 | .02 | .04 | .00 | .01 | |
|
| ||||||
| Variance | Intercept | 78.00* | 77.98** | 78.04** | 77.89** | 77.63** |
| Relative Pleasantness | .19* | .19* | .20* | .21* | .21* | |
| Covariance | −.61 | −.57 | −.62 | −.55 | −.60 | |
p < .10,
p < .05,
p < .01
BP: blood pressure, BIS: behavioral inhibition sensitivity, BAS: behavioral activation sensitivity
Table 4.
Diastolic BP predicted by day-level pleasantness, relative pleasantness, and total BIS/BAS score or individual facets of the BIS/BAS.
| Emotional Reactivity | BIS | BAS – Reward Responsiveness | BAS – Fun Seeking | BAS – Drive | ||
|---|---|---|---|---|---|---|
|
| ||||||
| B | B | B | B | B | ||
| Main Effects Model | Intercept | 78.99** | 78.99** | 78.99** | 78.98** | 78.98** |
| Day-Level Pleasantness | −.46* | −.46* | −.45* | −.45* | −.46* | |
| Relative Pleasantness | −.02 | −.02 | −.02 | −.02 | −.02 | |
| Reactivity | −.01 | −.02 | −.04 | −.03 | .05 | |
|
| ||||||
| Interaction Model | Intercept | 78.96** | 78.97** | 79.02 | 78.94 | 78.92** |
| Day-Level Pleasantness | −.47* | −.46* | −.44* | −.45* | −.48* | |
| Relative Pleasantness | −.02 | −.03 | −.02 | −.01 | −.02 | |
| Reactivity | −.01 | −.03 | −.05 | −.01 | .05 | |
| Day-Level × Reactivity | −.04 | .00 | −.11 | .08 | −.25** | |
| Relative × Reactivity | .00 | .02 | .01 | −.03+ | −.00 | |
|
| ||||||
| Variance | Intercept | 46.63* | 46.69** | 46.61** | 46.65** | 46.22** |
| Relative Pleasantness | .02 | .01 | .02 | .01 | .02 | |
| Covariance | −.62* | −.59* | −.62* | −.57+ | −.63* | |
p < .10,
p < .05,
p < .01
BP: blood pressure, BIS: behavioral inhibition sensitivity, BAS: behavioral activation sensitivity
Table 5.
HR predicted by day-level pleasantness, relative pleasantness, and total BIS/BAS score or individual facets of the BIS/BAS predicting HR.
| Emotional Reactivity | BIS | BAS – Reward Responsiveness | BAS – Fun Seeking | BAS – Drive | ||
|---|---|---|---|---|---|---|
|
| ||||||
| B | B | B | B | B | ||
| Main Effects Model | Intercept | 96.93** | 96.91** | 96.92** | 96.96** | 96.95** |
| Day-Level Pleasantness | −.26 | −.24 | −.29 | −.25 | −.26 | |
| Relative Pleasantness | .03 | .03 | .03 | .03 | .03 | |
| Reactivity | .02 | .06 | .12 | −.05 | −.09 | |
|
| ||||||
| Interaction Model | Intercept | 96.90** | 96.89** | 96.95** | 96.99** | 96.94** |
| Day-Level Pleasantness | −.26 | −.22 | −.28 | −.25 | −.26 | |
| Relative Pleasantness | .01 | .03 | .02 | .02 | .03 | |
| Reactivity | .00 | .04 | .10 | −.07 | −.10 | |
| Day-Level* Reactivity | .01 | .06 | −.04 | .01 | −.01 | |
| Relative* Reactivity | .02** | .03+ | .05* | .04+ | .03 | |
|
| ||||||
| Variance | Intercept | 68.15** | 68.07** | 68.12** | 68.11** | 68.10** |
| Relative Pleasantness | .11+ | .13* | .12* | .13* | .13* | |
| Covariance | −.86* | −.88* | −.91* | −.86* | −.88* | |
p < .10,
p < .05,
p < .01
HR: heart rate, BIS: behavioral inhibition sensitivity, BAS: behavioral activation sensitivity
Emotional Reactivity
In main effects models, emotional reactivity was not associated with systolic BP, diastolic BP, or HR. Consistent with the first hypothesis, participants who reported more pleasant interactions on average throughout the day had lower systolic BP, B = −.51 [95% confidence interval, −1.01, −.00] mmHg/10-point difference in VAS, p = .05, and lower diastolic BP, B = −.46 [−.85, −.06] mmHg/10-point difference in VAS, p = .02. Exploratory analyses of a possible interaction between emotional reactivity and average pleasantness of interactions showed that the effects of the latter did not depend on emotional reactivity. Contrary to the first hypothesis, there was no effect of average pleasantness on HR.
Again supporting the first hypothesis, results from the main effects models show that reporting a social interaction that was relatively more pleasant than one’s average pleasantness (i.e., a social interaction that was more pleasant than usual) was associated with lower systolic BP, B = −.13 [−.24, −.03] mmHg/10-point difference in VAS, p = .02. The main effects of relative pleasantness on diastolic BP and HR were not significant.
Regarding the second hypothesis, the second model (lower half of each table) revealed that total emotional reactivity significantly moderated the relationship of relative pleasantness to HR, B = .02 [.01, .04] bpm/10-point difference in VAS, p < .01 (see Figure 1). Although there was no main effect of relative pleasantness on HR, for participants with low emotional reactivity (one SD below the mean; −1SD), social interactions that were more pleasant than usual had a marginally significant association with HR, B = −.13 [−.27, .01] bpm/10-point difference in VAS, p = .07. In contrast, for participants with high emotional reactivity (+1SD), social interactions rated as more pleasant than usual were associated with higher HR, B = .16 [.04, .29] bpm/10-point difference in VAS, p = .01. These slopes were significantly different from each other, p < .01. The interaction between emotional reactivity and relative pleasantness was not statistically significant in the models predicting systolic and diastolic BP, B = .01 [−.00, .03] mmHg/10-point difference in VAS, p = .13, and, B = .00 [−.01, .02] mmHg/10-point difference in VAS, p = .74, respectively.
Figure 1.
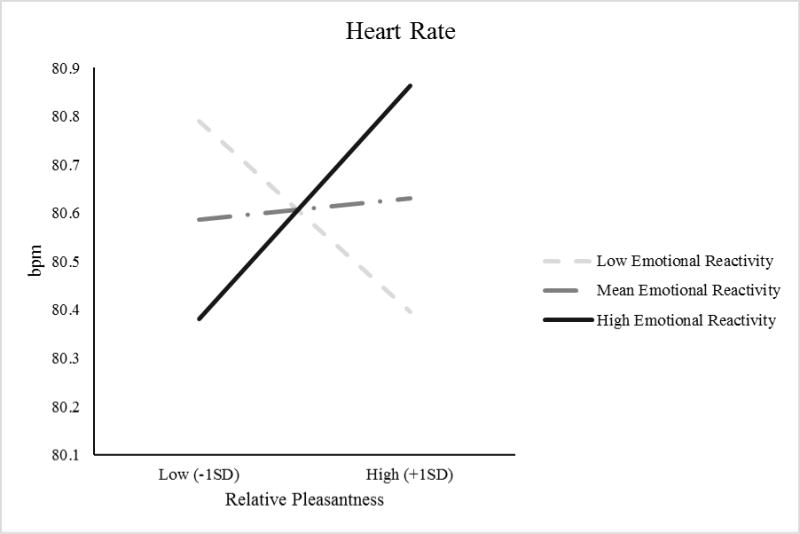
Estimated relationship of HR (beats per minute [bpm]) to relative pleasantness for individuals at different levels of emotional reactivity.
In summary, greater pleasantness of social interactions on average predicted lower systolic and diastolic BP, whereas greater relative pleasantness—an interaction that was more pleasant than usual—predicted only lower systolic BP. For participants high in emotional reactivity, an interaction that was more pleasant than usual predicted increased HR.
Subscale Tests
Consistent with the results for the total emotional reactivity score, reward responsiveness, fun-seeking, and drive moderated the relationship between relative pleasantness and HR (see Table 4). Again, similar to the primary results, participants low (−1SD) on these subscales did not exhibit an association between relative pleasantness and HR. Participants high (+1SD) on any of these three subscales exhibited a significant or marginally significant positive association: high behavioral inhibition, B = .12 [−.01, .25] bpm/10-point difference in VAS, p = .07; high reward responsiveness, B = .14 [.01, .27] bpm/10-point difference in VAS, p = .03; high fun-seeking, B = .11 [−.01, .24] bpm/10-point difference in VAS, p = .08.
Discussion
This study examined the between-person and within-person associations of the pleasantness of social interactions with blood pressure and heart rate over the course of 24 hours, as well as the potential moderating effect of emotional reactivity on these associations. The most consistent finding concerned the pleasantness of interactions. In support of our first hypothesis, people whose social interactions were on average more pleasant that day had lower average BP. Over and above the effect of average pleasantness, social interactions that were more pleasant than usual also predicted lower BP. Of particular interest, the effects of relative pleasantness on cardiac outcomes depended on emotional reactivity, although the nature of these effects were unexpected. Counter to our hypothesis (we had expected an exaggerated but parallel response amongst individuals higher versus lower in emotional reactivity), there was no evidence that emotional reactivity moderated the effect of relative pleasantness on BP, and, for people with higher emotional reactivity, heart rate increased as pleasantness increased. In contrast, people with lower emotional reactivity tended to have lower HR following interactions that were more pleasant than usual.
Pleasant interactions on average, and experiencing a particularly pleasant interaction, both predicted lower systolic BP, and average pleasantness also predicted lower diastolic BP. This is consistent with previous research finding beneficial effects of positive, social relationships on cardiovascular health (Coyne et al., 2001; Gump et al., 2001; Holt-Lunstad et al., 2003; Ruiz et al., 2008; Smith et al., 2014). There was no main effect of emotional reactivity on systolic BP, diastolic BP, or HR. Considering these null effects in light of the significant interaction effect described above, findings suggest that people who typically respond especially strongly to events that elicit positive or negative emotions do not show differences overall in cardiac activity relative to less reactive people. Rather, differences emerged specifically in the context of the pleasantness of the social interactions they experienced.
These findings raise interesting questions about emotional disposition. Why did emotional reactivity moderate the relationship between the relative pleasantness of an interaction, compared to one’s average, and HR, but not systolic or diastolic BP? In terms of HR, it may be that reactivity—positive or negative—is associated with greater physiological arousal, even if the stimuli are positive. Indeed, HR tended to increase in the context of interactions that were more pleasant than usual for people with high emotional reactivity, but tended to be lower in interactions that were more pleasant than usual for people lower in reactivity. It is conceivable that the observed HR increases during pleasant interactions among highly reactive participants may have been driven, in part, by heightened sympathetic arousal due to the positive reactivity component of our scale, or to “approach” or “reward” motivation (e.g., a developing friendship). That is, people with high reactivity may have experienced greater excitement or arousal, or appetitive motivation. Yet this interpretation does not explain why the effect of higher heart rate following pleasantness was observed when we separately examined the behavioral inhibition subscale, which is thought to measure avoidance and inhibition. Further, although the pattern observed for HR was similar across all subscales, these subscales were only moderately correlated, raising even more questions about the interrelationships between different forms of reactivity and physiological responding.
Positively valenced emotion can also vary substantially in arousal, and it may be that participants with higher emotional reactivity (either positive or negative) experienced pleasant interactions as arousing or exciting, prompting increased sympathetic arousal (i.e., elevated heart rate), whereas participants with lower reactivity may experience pleasant interactions as calming, prompting parasympathetic activity characteristic of pleasant relaxation (i.e., reduced heart rate). Future studies should consider this possibility, and should consider ways to capture a more diverse range of pleasant, unpleasant, and ambivalent interactions. Although we are somewhat limited when considering unpleasant (rather than pleasant) interactions, given that the interactions in this study were predominantly pleasant, similar possibilities arise. Although it is possible that two unipolar scales, one assessing pleasantness and the other unpleasantness, would have revealed different effects of these constructs on BP or HR than our unipolar assessment of pleasantness, our experience is that study participants resent the “same question” being asked twice with opposite adjectives in an electronic diary that they are asked to complete many times. Nevertheless, this method would have the additional advantage of better measuring valence (Kron, Goldstein, Lee, Gardhouse, & Anderson, 2013) in that it could capture ambivalent interactions (i.e., high pleasant and high unpleasant), and ambivalent interactions in particular have been linked to higher BP (Holt-Lunstad et al., 2003). Indeed, it is unclear how participants would have rated ambivalent interactions on our scale; we suspect somewhere near “neutral.” It may also be that people higher in emotional reactivity characterized ambivalent interactions as unpleasant, whereas those lower in emotional reactivity characterized them as relatively neutral. This is purely speculative; however, it is not unreasonable to assume that social interactions may be viewed differently depending on individual characteristics. For example, greater emotional reactivity to unpleasant situations is associated with a higher likelihood of experiencing conflicts with family or friends (David, Green, Martin, & Suls, 1997), and emotional sensitivity is associated with more positive and reciprocal friendships (Lopes, Salovey, Côté, Beers, & Petty, 2005). Parallels can also be drawn from research showing that support can attenuate stress reactivity (Eisenberger, Taylor, Gable, Hilmert, & Lieberman, 2007).
In this study, we were primarily interested in understanding how social interactions might influence cardiac outcomes differently for people who vary in overall reactivity to both positive and negative stimuli. Bolstering the value of this somewhat atypical approach, and the assertion that emotional reactivity in general might reflect an individual tendency towards physiological arousal, this measure demonstrated good internal consistency, and the pattern of associations observed in this study tended to replicate across the different subscales of the BIS/BAS, despite the fact that these subscales were correlated only weakly or not at all.
Strengths and Limitations
Our results should be considered in light of study strengths and limitations. One valuable aspect of the present study was its examination of individual differences in terms of broadly defined emotional reactivity to both unpleasant and pleasant events. Second, the use of 24-hour ambulatory blood pressure monitoring allowed us to examine the joint effects of social and emotional factors on cardiovascular outcomes in the context of everyday life in a large sample of 805 individuals. Third, our multilevel analytic approach enabled us to parse the separable influences of average pleasantness of social interactions and fluctuations in pleasantness, or experiencing interactions that were more or less pleasant than usual, on cardiac functioning.
There were also a number of potential limitations. First, our measure of global emotional reactivity (i.e., indexing positive and negative reactivity) was created by combining BIS and BAS subscales, which is not typically done (Carver & White, 1994). To ensure that our conceptualization of reactivity was valid, we examined results separately for each subscale and found general support for this approach given the consistency of results across subscales when predicting HR. Further, the BIS/BAS has previously been found to predict physiological responses to positive and negative social scenarios in the lab (e.g., Balconi & Bortolotti, 2012). However, study results should be interpreted with caution and replicated in other studies that assess ambulatory blood pressure over longer periods of time and include alternative measures of emotional reactivity. Second, the estimated variance in the effect of pleasantness on diastolic BP was not statistically significant, indicating that this effect did not vary much across individuals in this sample; hence, it is not surprising that the interaction of relative pleasantness with emotional reactivity predicting diastolic BP was also not significant. Finally, social interactions in this study were overwhelmingly perceived as pleasant. This range restriction may have muted significant results and obscured effects specific to unpleasant social interactions. Although this may be considered a limitation, it represents the real-world experience of a non-selected, employed, community sample. Still, future research could aim to capture more unpleasant social interactions, and use assessments that allow participants to identify ambivalent interactions.
Conclusion
Results indicated that individuals who reported more pleasant interactions on average had lower ambulatory BP, and experiencing an interaction that was more pleasant than usual was also associated with lower systolic BP. Further, emotional reactivity can shape physiological response to social interactions, specifically when considering HR. These findings contribute to the current understanding of the social and emotional context of cardiovascular health by suggesting that the pleasantness of social interactions impacts cardiovascular health, and that more emotionally reactive individuals may have an exaggerated HR response to more pleasant (vs. less pleasant) social interactions.
Days with generally pleasant interactions relate to lower average blood pressure
Emotional reactivity modifies heart rate response to social interactions
Reactivity to positive and negative events affect heart rate response similarly
Acknowledgments
We are indebted to the study participants and research staff of the Masked Hypertension Study, without whose cooperation and dedication this study would not have been possible. This work was supported by the National Heart, Lung, and Blood Institute (grant number P01-HL47540, PI: J Schwartz). The research was also supported in part by National Center for Advancing Translational Sciences (formerly the National Center for Research Resources), National Institutes of Health grants to Stony Brook University (grant number MO1-RR10710) and Columbia University Medical Center (UL1-TR000040; formerly, UL1-RR024156). The content is solely the responsibility of the authors and does not necessarily represent the official view of the NIH.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Although it is quite rare to explicitly incorporate time into models of ABP readings, we nevertheless performed a sensitivity analysis that included a sinusoidal diurnal pattern for time of day that was allowed to vary (both amplitude and location of the peak/nadir) among participants. The fixed effect is highly significant and there is also significant individual variability in the parameter estimates (when treated as random coefficients). Neither the coefficients nor the confidence intervals of the focal interaction effect (relative pleasantness with emotional reactivity) were affected by the incorporation of time into the models:
Systolic BP, as reported in the manuscript: B = .01 [-.00, .03], p = .13. With time in both the model and random statements: B = .01 [-.00, .03], p = .12.
Diastolic BP, as reported in the manuscript: B = .00 [-.01, .02], p = .74. With time in both the model and random statements: B = .00 [-.01, .02], p = .59.
HR, as reported in the manuscript: B = .02 [.01, .04], p < .01. With time in both the model and random statements: B = .02 [.01, .04], p < .01.
Competing Interest Statement
All authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf and declare that Dr. Schwartz received support from NIH/NHLBI grants during the conduct of the study.
References
- Balconi M, Bortolotti A. Resonance mechanism in empathic behavior: BEES, BIS/BAS and psychophysiological contribution. Physiology & Behavior. 2012;105(2):298–304. doi: 10.1016/j.physbeh.2011.08.002. [DOI] [PubMed] [Google Scholar]
- Brondolo E, Rieppi R, Erickson SA, Bagiella E, Shapiro PA, McKinley P, Sloan RP. Hostility, interpersonal interactions, and ambulatory blood pressure. Psychosomatic Medicine. 2003;65(6):1003–1011. doi: 10.1097/01.PSY.0000097329.53585.A1. [DOI] [PubMed] [Google Scholar]
- Brosschot JF, Geurts SAE, Kruizinga I, Radstaak M, Verkuil B, Quirin M, Kompier MAJ. Does unconscious stress play a role in prolonged cardiovascular stress recovery? Stress and Health. 2014;30(3):179–187. doi: 10.1002/smi.2590. [DOI] [PubMed] [Google Scholar]
- Campbell-Sills L, Liverant GI, Brown TA. Psychometric evaluation of the behavioral inhibition/behavioral activation scales in a large sample of outpatients with anxiety and mood disorders. Psychological Assessment. 2004;16(3):244–254. doi: 10.1037/1040-3590.16.3.244. [DOI] [PubMed] [Google Scholar]
- Carels RA, Blumenthal JA, Sherwood A. Emotional responsivity during daily life: Relationship to psychosocial functioning and ambulatory blood pressure. International Journal of Psychophysiology. 2000;36(1):25–33. doi: 10.1016/S0167-8760(99)00101-4. [DOI] [PubMed] [Google Scholar]
- Carver CS, White TL. Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS Scales. Journal of Personality and Social Psychology. 1994;67(2):319–333. [Google Scholar]
- Carver CS. Negative affects deriving from the behavioral approach system. Emotion. 2004;4(1):3–22. doi: 10.1037/1528-3542.4.1.3. [DOI] [PubMed] [Google Scholar]
- Claes L, Bijttebier P, Van Den Eynde F, Mitchell JE, Faber R, de Zwaan M, Mueller A. Emotional reactivity and self-regulation in relation to compulsive buying. Personality and Individual Differences. 2010;49(5):526–530. [Google Scholar]
- Claes L, Vertommen S, Smits D, Bijttebier P. Emotional reactivity and self-regulation in relation to personality disorders. Personality and Individual Differences. 2009;47(8):948–953. [Google Scholar]
- Coyne JC, Rohrbaugh MJ, Shoham V, Sonnega JS, Nicklas JM, Cranford JA. Prognostic importance of marital quality for survival of congestive heart failure. The American Journal of Cardiology. 2001;88(5):526–529. doi: 10.1016/s0002-9149(01)01731-3. [DOI] [PubMed] [Google Scholar]
- David JP, Green PJ, Martin R, Suls J. Differential roles of neuroticism, extraversion, and event desirability for mood in daily life: An integrative model of top-down and bottom-up influences. Journal of personality and social psychology. 1997;73(1):149–159. doi: 10.1037//0022-3514.73.1.149. [DOI] [PubMed] [Google Scholar]
- De Vogli R, Chandola T, Marmot MG. Negative aspects of close relationships and heart disease. Archives of Internal Medicine. 2007;167(18):1951–1957. doi: 10.1001/archinte.167.18.1951. [DOI] [PubMed] [Google Scholar]
- Eisenberger NI, Taylor SE, Gable SL, Hilmert CJ, Lieberman MD. Neural pathways link social support to attenuated neuroendocrine stress responses. Neuroimage. 2007;35(4):1601–1612. doi: 10.1016/j.neuroimage.2007.01.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gump BB, Polk DE, Kamarck TW, Shiffman SM. Partner interactions are associated with reduced blood pressure in the natural environment: Ambulatory monitoring evidence from a healthy, multiethnic adult sample. Psychosomatic Medicine. 2001;63(3):423–433. doi: 10.1097/00006842-200105000-00011. [DOI] [PubMed] [Google Scholar]
- Heubeck BG, Wilkinson RB, Cologon J. A second look at Carver and White’s (1994) BIS/BAS scales. Personality and Individual Differences. 1998;25(4):785–800. [Google Scholar]
- Holt-Lunstad J, Uchino BN, Smith TW, Olson-Cerny C, Nealey-Moore JB. Social relationships and ambulatory blood pressure: structural and qualitative predictors of cardiovascular function during everyday social interactions. Health Psychology. 2003;22(4):388–397. doi: 10.1037/0278-6133.22.4.388. [DOI] [PubMed] [Google Scholar]
- Kron A, Goldstein A, Lee DHJ, Gardhouse K, Anderson AK. How are you feeling? Revisiting the quantification of emotional qualia. Psychological Science. 2013;24(8):1503–1511. doi: 10.1177/0956797613475456. [DOI] [PubMed] [Google Scholar]
- Lopes PN, Salovey P, Côté S, Beers M, Petty RE. Emotion regulation abilities and the quality of social interaction. Emotion. 2005;5(1):113–118. doi: 10.1037/1528-3542.5.1.113. [DOI] [PubMed] [Google Scholar]
- Meyer B, Johnson SL, Carver CS. Exploring behavioral activation and inhibition sensitivities among college students at risk for bipolar spectrum symptomatology. Journal of Psychopathology and Behavioral Assessment. 1999;21(4):275–292. doi: 10.1023/A:1022119414440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock MK, Wedig MM, Holmberg EB, Hooley JM. The emotion reactivity scale: Development, evaluation, and relation to self-injurious thoughts and behaviors. Behavior Therapy. 2008;39(2):107–116. doi: 10.1016/j.beth.2007.05.005. [DOI] [PubMed] [Google Scholar]
- Parati G, Pomidossi G, Albini F, Malaspina D, Mancia G. Relationship of 24-hour blood pressure mean and variability to severity of target-organ damage in hypertension. Journal of Hypertension. 1987;5(1):93–98. doi: 10.1097/00004872-198702000-00013. [DOI] [PubMed] [Google Scholar]
- Ross K, Martin T, Chen E, Miller GE. Social encounters in daily life and 2-year changes in metabolic risk factors in young women. Development and Psychopathology. 2011;23(3):897–906. doi: 10.1017/S0954579411000381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruiz JM, Hutchinson JG, Terrill AL. For better and worse: Social influences on coronary heart disease risk. Social and Personality Psychology Compass. 2008;2(3):1400–1414. doi: 10.1111/j.1751-9004.2008.00108.x. [DOI] [Google Scholar]
- Schwartz JE, Burg MM, Shimbo D, Broderick JE, Stone AA, Ishikawa J, Pickering TG. Clinic blood pressure underestimates ambulatory blood pressure in an untreated employer-based US population: Results From the Masked Hypertension Study. Circulation. 2016;134(23):1794–1807. doi: 10.1161/CIRCULATIONAHA.116.023404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz JE, Stone AA. The analysis of real-time momentary data: A practical guide. In: Stone AA, Shiffman S, Atienza AA, Nebeling L, editors. The science of real-time data capture: Self-report in health research. Oxford: Oxford University Press; 2007. pp. 76–113. [Google Scholar]
- Schwartz JE, Warren K, Pickering TG. Mood, location and physical position as predictors of ambulatory blood pressure and heart rate: Application of a multi-level random effects model. Annals of Behavioral Medicine. 1994;16(3):210–222. [Google Scholar]
- Smith TW, Baron CE, Grove JL. Personality, emotional adjustment, and cardiovascular risk: Marriage as a mechanism. Journal of Personality. 2014;82(6):502–514. doi: 10.1111/jopy.12074. [DOI] [PubMed] [Google Scholar]
- Smith TW, Gallo LG. Hostility and cardiovascular reactivity during marital interaction. Psychosomatic Medicine. 1999;61(4):436–445. doi: 10.1097/00006842-199907000-00005. [DOI] [PubMed] [Google Scholar]
- Stergiou GS, Ntineri A, Kollias A, Ohkubo T, Imai Y, Parati G. Blood pressure variability assessed by home measurements: A systematic review. Hypertension Research. 2014;37(6):565–572. doi: 10.1038/hr.2014.2. [DOI] [PubMed] [Google Scholar]
- Stevens SL, Wood S, Koshiaris C, Law K, Glasziou P, Stevens RJ, McManus RJ. Blood pressure variability and cardiovascular disease: Systematic review and meta-analysis. BMJ. 2016;354:i4098. doi: 10.1136/bmj.i4098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vella EJ, Kamarck TW, Shiffman S. Hostility moderates the effects of social support and intimacy on blood pressure in daily social interactions. Health Psychology. 2008;27(2S):S155. doi: 10.1037/0278-6133.27.2(Suppl.).S155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zanstra YJ, Johnston DW. Cardiovascular reactivity in real life settings: Measurement, mechanisms and meaning. Biological Psychology. 2011;86(2):98–105. doi: 10.1016/j.biopsycho.2010.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]