

Introduction to atrial function
As specialized compartments of the heart, the atria feature unique mechanical and structural properties that differ considerably from those of the ventricular myocardium. Beyond their contribution to cardiac output as a reservoir, conduit, and booster pump at different phases of the cardiac cycle, the atria determine heart rhythm, regularity, and rate (chronotropy). They also function as mechanical sensors and exert relevant endocrine activity (e.g. natriuretic peptides). Atrial remodelling is often observed in association with ventricular remodelling in heart failure (HF) but by itself adds to the complexity of the disease.
Atrial remodelling—types and classifications
In a recent consensus statement, atrial remodelling has been defined as ‘any complex of structural, architectural, contractile or electrophysiological changes affecting the atria with the potential to produce clinically‐relevant manifestations’ and giving rise to an atrial cardiomyopathy.1 The authors have further proposed a novel classification to differentiate histological changes European Heart Rhythm Association (EHRA I–IV). In clinical settings, characterization and understanding of atrial remodelling in the context of HF and co‐morbidities currently remain dependent on cardiac imaging‐derived read‐outs, as outlined later.
Left atrial (LA) enlargement (LAE) is frequently used synonymously with atrial remodelling. However, also in HF, hypertrophy and fibrosis of the atrial wall, atrial fibrillation (AF; suggesting electrical remodelling), and atrial contractile dysfunction all may occur in the absence of LAE,2, 3, 4, 5 indicating the necessity for a more comprehensive assessment of the atrial phenotype.
Clinical diagnosis of atrial remodelling
Size and function
Individual electrocardiogram (ECG) criteria (P‐wave morphology) are not a reliable measure for LAE and right atrial (LA) enlargement (RAE) but may serve as a screening tool.6 LA size or volume by echocardiography, corrected for body size [i.e. LA volume index (LAVI)] are commonly used to describe LAE, with 2D echocardiography underestimating volumes as measured by 3D echocardiography, cardiac computed tomography, or cardiac magnetic resonance.7 Volumes relate to the reservoir function of the LA. Neither LA size nor LAVI is gender dependent, yet they increase with age.8 Measurement of atrial volumes additionally allows to calculate atrial contractility (i.e. LA emptying fraction and LA expansion index), but without differentiating between passive (conduit and reservoir) and active (booster pump) function. Atrial strain and atrial strain rate based on speckle tracking echocardiography have been recently implemented for the differentiation of LA reservoir and conduit function. Methodically more challenging, LA strain rate allows to measure active LA contraction (i.e. booster pump).9 In experimental settings, in analogy to the ventricle, pressure‐volume catheters have been used to quantify LA stiffness and atrioventricular coupling.10
Tissue composition
Cardiac magnetic resonance late gadolinium enhancement regions are used to characterize atrial fibrous remodelling.11 Magnetic resonance imaging (MRI) T1 mapping allows to assess the degree of fibrosis in ventricular remodelling; however, it has failed to convincingly do so in the LA.12 Finally, in selected patients, electro‐anatomical mapping allows the quantification and localization of low‐voltage areas to assess an additional local functional parameter of atrial remodelling. However, to date, the exact relation between the extent and severity of low‐voltage regions and the degree of LA fibrosis/remodelling needs further clarification. Biomarkers have been used as a surrogate for atrial remodelling, reflecting mechanical stress, fibrosis, or inflammation; but individual markers to date lack atrial specificity.13, 14, 15
Prevalence of atrial remodelling in heart failure
Left atrial enlargement as a sign of atrial remodelling is observed in about half of the patients with stable chronic HF with large variations between studies, likely reflecting heterogeneous disease aetiologies and stages (Table 1).
Table 1.
Atrial enlargement in heart failure
| Study | HF type (EF %) | n patients | Measure of LA size | Non‐failing group | HF group | Cut‐off abnormal LA | HF and LAE (% patients) |
|---|---|---|---|---|---|---|---|
| TOPCAT16 | HFpEF (≥45%) | 935 | LAVI (mL/m2) | n/a | 29.8 ± 12.5 | ≥29 | 46% |
| PARAMOUNT5 | HFpEF (≥45%) | 175 | LAVI (mL/m2) | 21.1 ± 5.3 | 33.4 ± 11.5 | ≥29 | 61% |
| ARIC (Jackson)17 | HFpEF (≥50%) | 85 | LA diam. (cm) | 3.4 (3.0, 3.7) | 3.4 (3.1, 3.8) | ≥4.0 | 19% |
| ARIC (Jackson)17 | HFrEF (<50%) | 31 | LA diam. (cm) | 3.4 (3.0, 3.7) | 3.8 (3.3, 4.3) | ≥4.0 | 39% |
| i‐PRESERVE Echo Substudy18 | HFpEF (≥45%) | 745 | LA area (cm2) | n/a | 23 ± 6 | ≥20 mild, ≥31 mod./sev. | 66% (51% mild) |
| Cioffi et al.19 | HFrEF (<50%) | 194 | LA max vol. (mL/m3) | 7.1 ± 2.1 | 11.0 ± 4.0 | 11.3 | 41% |
| Rossi et al.20 | HFpEF (>45%) | 310 | LA diameter (cm) | 3.7 ± 0.6 | 4.6 ± 1.0 | 5.0 | 34% |
| Zivlas et al.21 | HFrEF (<35%) | 40 | LAVI (mL/m2) | n/a | 66.6 ± 1.7 | ≥29 | n/a |
| Almodares et al.22 | HFpEF/HFrEF (NYHA III–IV) | 289 | LAVI (mL/m2) | n/a | 58 ± 22.7 | ≥29 | n/a |
EF, ejection fraction; HF, heart failure; HFpEF, HF with preserved EF; HFrEF, HF with reduced EF; LA, left atrial; LAE, LA enlargement; LAVI, LA volume index; NYHA, New York Heart Association.
Atrial contractile dysfunction
In HF with reduced ejection fraction (HFrEF), LA emptying fraction has been shown to be significantly decreased.23 LA emptying fraction and LA strain are also reduced in HF with preserved ejection fraction (HFpEF) in clinical studies9, 24, 25 and randomized controlled trials [e.g. Effect of Phosphodiesterase‐5 Inhibition on Exercise Capacity and Clinical Status in Heart Failure with Preserved Ejection Fraction (RELAX trial) substudy26 and Candesartan in Heart failure ‐ Assessment of moRtality and Morbidity (CHARM trial)‐preserved]. Regional differences in LA strain may also be an early sign of electrical remodelling leading to AF.27
Atrial fibrosis
In HFrEF, LA fibrosis has been reported to range from 13% to 27% of the LA area as compared with 1.4% in control.28 In HFpEF, LA fibrosis as assessed using histology and MRI imaging was shown to be 30.1 ± 4.6% of the LA area (n = 18 HFpEF patients).29 However, aetiology‐dependent differences in prevalence of atrial fibrosis in HF have not been systematically studied.
Electrophysiological remodelling
Signs of LA electrical remodelling in HF (HFrEF) include conduction abnormalities (as reflected by P‐wave morphology in ECG), prolonged refractoriness (in contrast to AF‐induced remodelling), and sinus node dysfunction.30 Incidental AF serves as a marker of electrophysiological remodelling. The prevalence of AF in HF has been reported from 5% in New York Heart Association (NYHA) I to 25–50% in NYHA III/IV,31, 32 with higher prevalence in HFpEF vs. HFrEF (see subsequent discussion).
Clinical impact of atrial remodelling and relevance in heart failure with preserved ejection fraction
Atrial remodelling as risk biomarker
Left atrial volume index is strongly associated with cardiovascular disease33 and a predictor of new HF irrespective of systolic left ventricular (LV) function.18, 34, 35 LAE is also an independent predictor for the development of early [American Heart Association (AHA) stage B] non‐ischaemic HF.36 With regard to secondary events, LAVI correlates with a higher incidence of congestive HF recurrence37 and sudden cardiac death.38 LA size is used as an independent marker of risk in several HF risk scores, such as the Coronary Artery Revascularization in Diabetes (CARDIA) risk score [based on the Framingham 10 year global cardiovascular (CV) Framingham risk score (FRS)39], the Redin‐SCORE,40 and the MUerte Subita en Insuficiencia Cardiaca (MUSIC) Risk score. Indexed LA diameter is increasingly being used as predictor of long‐term outcomes in patients evaluated for aortic valve replacement, and its assessment may guide patient management.41 LA function (at rest) is a predictor of exercise capacitance in HFrEF,42 and LA contractile dysfunction has been shown to be associated with a higher risk of HF hospitalization independent of potential clinical confounders.43
Atrial remodelling is of particular interest in patients with HFpEF,44 where it has been associated with increased mortality45 and has been recognized as a hallmark feature of the disease.44 Melenovsky et al. have shown that preserved LA function was significantly associated with lower mortality in HFpEF.46 Moreover, in HFpEF, impaired LA conduit function is associated with exercise intolerance, independent of LV stiffness and relaxation.47 On the other hand, in the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial, contractile LA dysfunction (reduced peak LA strain) in HFpEF was not associated with a higher risk of HF hospitalizations when also accounting for LV systolic and diastolic function.43 This is explained by the robust interrelation between peak LA strain, LV global longitudinal strain, and E/e′.25
Atrial contribution to ventricular function
The role of atrial contraction in different aetiologies and stages of HF is quantitatively not very well explored. Modelling suggests that a timely atrial contraction significantly improves LV stroke work.48 In a recent report from a cohort of HF patients (51% HFpEF), atrial remodelling in HFrEF was characterized by increased LA volumes and lower contraction amplitude (pulsatility) as compared with HFpEF, whereas HFpEF was associated with higher LA pressures and increased LA wall stiffness.46 Vice versa, in patients with HFrEF receiving cardiac synchronization therapy (CRT), a reduction in LA strain induced by atrial pacing resulted in a significant reduction in global LV strain.49 Atrial contribution to ventricular filling can decline with the progression of HF, as increased atrial mechanical load leads to atrial dysfunction.50 HFpEF is characterized by impaired LV diastolic filling, and LA ejection volume contributes to LV filling. Clearly, more work is needed to dissect the relative contribution of atrial dysfunction to impaired LV filling in different HFpEF phenotypes.
Atrial fibrillation and fibrosis
Atrial fibrillation is common HF, with reported prevalences of 21–65% in HFpEF, which is higher than what has been reported in HFrEF (<10–50%).51 AF is often linked to the presence of fibrotic remodelling, as fibrosis creates conduction obstacles that perpetuate the genesis of re‐entry circuits.52 Fibrosis is especially prevalent in atrial remodelling in patients with HFpEF.29 In the RELAX trial, HFpEF patients with AF (37%) had more advanced disease and a significantly reduced exercise capacitance, which might be also related to the development of tachy‐cardiomyopathy.53 Likewise, others reported that AF is independently associated with greater exertional intolerance, natriuretic peptide elevation, and left anterior descending artery remodelling in HFpEF.53, 54 Vice versa, in Framingham Heart Study participants, pre‐existing AF tended to be more strongly associated with new‐onset HFpEF (hazard ratio 2.34) than did HFrEF (hazard ratio 1.32), highlighting the relevance of atrial function in HFpEF.55
Endocrine activity
Physiologically, endocrine function of the heart is mainly located to the atria.56 Natriuretic peptides [e.g. atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP)] and vasopressin are secreted by atrial myocytes (and possibly fibroblasts) in response to acute stretch and neurohumoral activation (angiotensin, endothelin, and catecholamines)57, 58 and have a pivotal role in volume regulation.56 In HF, ANP and BNP production increases in the atria, and BNP is also produced in the ventricle.59 As reviewed elsewhere, atrial myocyte ANP secretion is impaired in HFrEF.60 Fibrotic atrial remodelling may contribute to the reduced amount of natriuretic peptides secreted from the atria.61
Interestingly, the increase of natriuretic peptides is less pronounced in HFpEF than in HFrEF.62 Increased BNP clearance by adipose tissue (in HFpEF) and decreased BNP production due to ‘cardiac cachexia’ have been proposed as mechanisms,62 but an impaired production or secretion in the atrial (or ventricular) myocardium in HFpEF remains to be explored.63 Beta‐blockade with metoprolol increases plasma BNP levels in HFrEF.64 BNP given subcutaneously can improve the haemodynamic response to acute volume load in patients with HFpEF,65 corroborating a relative deficit of natriuretic peptides. Likewise, increasing natriuretic peptide availability by neprilysin inhibition with simultaneous angiotensin II receptor blockade and neprilysin inhibition has been shown to be beneficial (see below ‘Atrial Reverse Remodeling with Therapy’). The role of atrial remodelling in the disproportionate levels of natriuretic peptides and their precursors in response to chronic and acute stress in particular in HFpEF warrants further research.
Chronotropic incompetence
Chronotropic incompetence is a common and likely undervalued cause of reduced exercise capacitance in HFrEF and HFpEF.66 Borlaugh et al. demonstrated that in particular in HFpEF patients, an attenuated increase in heart rate rather than inappropriate stroke volume was the cause of a reduced cardiac output reserve during exercise.67 While in patients with HFrEF, down‐regulation of myocardial beta‐adrenergic receptors and sinus node remodelling and dysfunction have been demonstrated as potential causes of chronotropic incompetence,68 its pathophysiology in HFpEF has not yet been studied in detail. As published recently in this journal, 3D echocardiography‐based assessment of stroke volume and heart rate during exercise may allow differentiating patients with reduced chronotropic reserve from others in a heterogeneous HFpEF population.69
Hypercoagulability
Left atrial enlargement has been shown to predict the risk for stroke even when adjusted for the prevalence of AF.70 The Asymptomatic Atrial Fibrillation and Stroke Evaluation in Pacemaker Patients and the Atrial Fibrillation Reduction Atrial Pacing Trial (ASSERT) and Anticoagulation Guided by Remote Rhythm Monitoring in Patients With Implanted Cardioverter‐Defibrillator and Resynchronization Devices (IMPACT) trials also suggested that stroke risk is increased in remodelled atria even if patients are in sinus rhythm. Vice versa, hypercoagulability itself may promote atrial remodelling by activation of pro‐fibrotic signalling molecules like TGF‐beta increasing thrombin. Inhibition of thrombin has been associated with attenuated atrial remodelling.71
The right atrium
Similar to the LA, RA size is strongly correlated to right ventricular end‐diastolic pressure and is thereby linked to pulmonary artery hypertension and right HF.72 RA dysfunction and the severity of right HF can be assessed using RA longitudinal strain by speckle tracking echocardiography.73 As a biomarker, an RA larger than LA is associated with increased mortality in elderly HF patients,22 and systolic blood pressure to RA pressure ratio is a marker that identifies a spectrum of complications after hospitalization of patients with decompensated systolic HF.74
Risk factors and pathophysiology of atrial remodelling in heart failure
Mechanical load
In HF, increased pressure or volume load in the ventricle is a strong trigger for atrial enlargement and remodelling. In chronic conditions, LA volume and strain correlate with LV end‐diastolic pressures irrespective of EF.75, 76 Mechanical stress induces stretching and stiffening of the atria.77 Atrial fibrosis is perpetuated by atrial distention78, 79, 80 and related to activation of pro‐fibrotic signalling cascades and apoptosis/necrosis of cells as well as activation of a foetal gene programme.81 This in turn negatively impacts atrial reservoir function (through stiffening) and active atrial kick (through over‐stretching and Frank–Starling mechanism). Increased ventricular pressures may contribute to remodelling of the LA (as in arterial hypertension) or the RA (as in pulmonary hypertension secondary to chronic pulmonary disease). Mechanical load is a strong confounder in investigating other load‐independent mechanisms for atrial remodelling in HF and arguably may diminish the role of other co‐morbidities in shaping atrial remodelling in later HF stages. On the other hand, even in advanced HFrEF, the impact of reducing mechanical load (e.g. by CRT) on myocardial remodelling is lower in the presence of other co‐morbidities, suggesting (but not proving) load‐independent effects of relevant co‐morbidities on atrial remodelling in HF.82 In early‐stage hypertensive HFpEF, LA cardiomyocyte hypertrophy, titin hyperphosphorylation, and microvascular dysfunction occur in association with increased systolic and diastolic LA chamber stiffness, impaired atrioventricular coupling and decreased LV stroke volume.10
Neuroendocrine activation triggered by low cardiac output is a hallmark of HFrEF but likely also plays a role in HFpEF.83, 84 Systemic and myocardial levels of catecholamines, aldosterone, and angiotensin are increased in HF and perpetuate atrial remodelling owing to their prohypertropic and pro‐fibrotic effects.85 , 86
In HFpEF, chronic kidney disease (CKD) is highly prevalent with the majority of patients suffering mild to moderate renal impairment.87 Others have reported similar prevalence of CKD in HFpEF and HFrEF.88 CKD‐associated renal arterial hypertension has been identified as a trigger of maladaptive LA remodelling in a model of early‐stage HFpEF.10
The prevalence of diabetes is similar in HFpEF and HFrEF88 and independently associated with LAE.89 A higher prevalence of obesity has been reported in HFpEF (51%) vs. HFrEF (37%88). LA enlargement correlates with epicardial fat thickness90 and visceral fat mass.91 In patients undergoing AF ablation (n = 236), low‐voltage areas suggestive of atrial fibrosis were much more common (46% of patients) in patients with metabolic syndrome than in those without (8%92). The pathomechanisms of atrial remodelling in metabolic syndrome are unclear and, as in ventricular metabolic remodelling, may be multifactorial including inflammation, oxidative stress, pro‐fibrotic pathways, and others.93
Atrial fibrillation in HF is a result of atrial remodelling (Figure 1). Mechanical stretch facilitates arrhythmia initiation94 and structural changes (e.g. fibrosis), thus providing the substrate for sustained arrhythmias.95 At the same time, AF itself is a strong promoter of tachyarrhythmia‐induced atrial cardiomyopathy. Electrical atrial remodelling during AF, however, differs from HF‐related atrial remodelling.7 The current understanding of the pathomechanisms underlying AF‐induced remodelling has been extensively reviewed.1, 52
Figure 1.
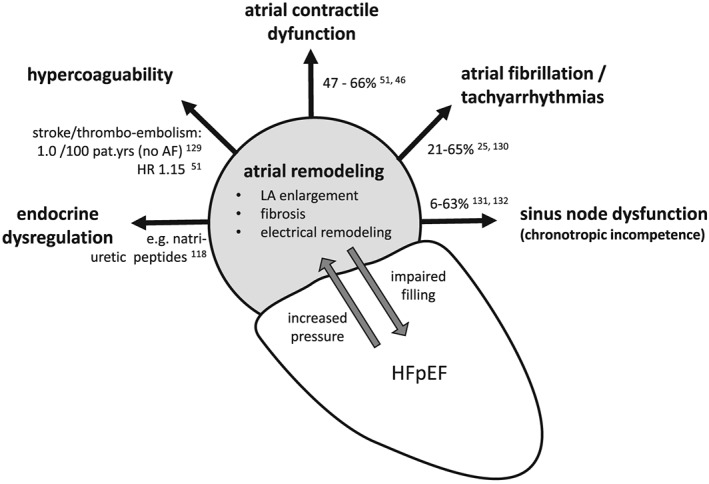
Clinical features of atrial cardiomyopathy in HFpEF. AF, atrial fibrillation; HFpEF, heart failure with preserved ejection fraction; HR, hazard ratio; LA, left atrial
Cumulative cardiovascular risk factors
The aforementioned common risk factors and other cardiovascular risk factors, including age and vascular disease, may synergistically promote atrial remodelling. Indeed, the CHA2DS2‐VASc risk score established to evaluate stroke risk in AF also reflects the risk of incidental AF96 and correlates with LA enlargement.97
Atrial reverse remodelling with therapy
Reverse atrial remodelling in patients with HF or at risk of HF has been shown to improve clinical endpoints like the incidence of AF98 and is independently associated with decreased mortality.99 Weight reduction with intensified risk factor management induces reverse atrial remodelling and reduces AF prevalence.100 Exercise training was also associated with a reduction in LA volume in HFpEF.101
Medical therapy
Several classes of classical HFrEF drugs [e.g. angiotensin‐converting enzyme (ACE) inhibitors, angiotensin‐receptor blockers, and spironolactone] have been associated with a reduction in LAE in patients with structural heart disease102 in part related to their blood‐pressure‐lowering effect.103 Treatment with ACE inhibitors and angiotensin receptor blockers also positively affects contractile function of the LA in HF.104, 105 In the absence of HF, quinapril effectively reduced LA volume independent of its effects on systolic blood pressure, suggesting direct effects on the atrial myocardium. Similarly, increasing the levels of natriuretic peptides, e.g. with neprilysin inhibition, has had beneficial effects on LA size in HFrEF106 and in HFpEF [Prospective comparison of ARNI with ARB on Management Of heart failUre with preserved ejectioN fracTion (PARAMOUNT trial107)] independent of the drug's blood‐pressure‐lowering effects.108 Lowering heart rate could improve atrial contribution to LV filling in HF. Interestingly, recent data from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE‐HF trial) registry suggest that lowering heart rate (<70 b.p.m.) has beneficial effects in HFpEF independent of atrial contribution (i.e. sinus rhythm vs. AF109).
Cardiac synchronization therapy was associated with a significantly increased LA strain, suggestive of reverse function atrial remodelling.110 Of note, maintaining intrinsic electrical atrial activation and contraction (as opposed to AV‐sequential pacing) significantly improves cardiac output with CRT.49
Specifically targeting AF as a result of atrial remodelling in HF has been proposed with the aim of reversing electrical remodelling induced by AF and preserve/restore contribution of the LA to ventricular filling in sinus rhythm.53 Indeed, surgical and catheter‐based AF ablation was associated with reverse atrial remodelling in non‐failing111, 112, 113 and also failing hearts (HFrEF114). Restoration of atrial function may contribute to the observations of the yet‐to‐be‐published Catheter Ablation vs. Conventional Therapy For Patients With AFib and LV Dysfunction (CASTLE‐AF) trial,115 where AF ablation significantly decreased the composite of all‐cause mortality and unplanned hospitalization for worsening HFrEF. In addition, in the Prevention of Early Atrial Fibrillation in Heart Failure (RACE 3) trial (n = 250), presented at the ESC Congress 2017, an early upstream therapy consisting of physical activity, dietary restrictions, statins, and ACE inhibitors or angiotensin receptor blocker was superior to conventional therapy in maintaining sinus rhythm in HF patients with AF (http://clinicaltrials.gov Identifier: NCT00877643).
Hypercoagulability is currently treated mainly in the presence of AF. In HF(rEF) alone, i.e. in the absence of AF, anticoagulation with warfarin is not recommended based on randomized trials.116 Additional risk factors such as previous stroke,117 the CHA2DS2‐VASc score,118 or LAE119 may identify HF patients at increased risk for future stroke, but further studies are needed to refine the tools for patient selection and evaluate the novel oral anticoagulants.
Outlook
Atrial function and remodelling are strongly influenced by LV haemodynamics, and atrial size may even serve as biomarker of chronically elevated LV pressure. As outlined earlier, however, accumulating evidence suggests that atrial remodelling independently adds to the complexity of the systemic dysregulation characterizing HF. The role of different co‐morbidities for atrial remodelling at later stages of HF in the context of increased mechanical load needs to be defined. The recently proposed EHRAS classification for atrial cardiomyopathy1 is a first step in establishing an aetiology‐dependent and stage‐dependent understanding of atrial remodelling as a basis for novel selective therapeutic approaches. Advanced clinical imaging, mainly MRI based, will add detailed in vivo information on function, fibrosis, inflammation, and metabolism for a better characterization of the atrial substrate. In addition, a combination of established biomarkers elevated during HF and associated with atrial remodelling might contribute to the development of risk scores: e.g. BNP54 and Galectin‐3120 have been shown to be markers of atrial remodelling and to directly correlate with the extent of LA fibrosis.121 Only recently has TNF‐alpha been suggested as a biomarker for increased fibrosis, cardiomyocyte apoptosis, and AF.122 Increases in TNF‐alpha are also associated with an increased risk of HF: in Framingham per tertile increment in TNF‐alpha, HF risk was increased by 68%.123, 124
Novel treatment approaches for atrial remodelling associated with HF have been tested in animal models. Direct thrombin inhibition has been shown to prevent HF‐related and AF‐related atrial remodelling in rats.125 Currently, following the landmark trials Amiodarone for Treatment of persistent Atrial fibrillation in patients with Congestive heart failure and an implanted device (AATAC) and CASTLE‐AF, a number of studies evaluate the role of catheter‐based AF ablation on clinical endpoints in different HF populations, and it is reasonable to assume that reverse atrial remodelling will be a key for a sustained success of AF ablation.
However, the process of reverse atrial remodelling is poorly quantified. More advanced imaging technologies like MRI‐based quantification of atrial remodelling126 and novel algorithms are needed to address this issue. The first attempts to further characterize the state of atrial remodelling using advanced imaging techniques but also basic clinical tools like resting ECGs127, 128 have been made and were able to report the degree of electrophysiological changes in the atria owing to structural remodelling.
In summary, enhancing atrial contribution to ventricular filling, preventing atrial tachyarrhythmias (restoring sinus rhythm), and improving atrial endocrine and regulatory function are equally important approaches that need to be further explored in HF.
Hohendanner, F. , Messroghli, D. , Bode, D. , Blaschke, F. , Parwani, A. , Boldt, L.‐H. , and Heinzel, F. R. (2018) Atrial remodelling in heart failure: recent developments and relevance for heart failure with preserved ejection fraction. ESC Heart Failure, 5: 211–221. doi: 10.1002/ehf2.12260.
References
- 1. Goette A, Kalman JM, Aguinaga L, Akar J, Cabrera JA, Chen SA, Chugh SS, Corradi D, D'Avila A, Dobrev D, Fenelon G, Gonzalez M, Hatem SN, Helm R, Hindricks G, Ho SY, Hoit B, Jalife J, Kim YH, Lip GY, Ma CS, Marcus GM, Murray K, Nogami A, Sanders P, Uribe W, Van Wagoner DR, Nattel S. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: definition, characterization, and clinical implication. Heart Rhythm 2017; 14: e3–e40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Bytyci I, Bajraktari G. Left atrial changes in early stages of heart failure with preserved ejection fraction. Echocardiography 2016; 33: 1479–1487. [DOI] [PubMed] [Google Scholar]
- 3. Polejaeva IA, Ranjan R, Davies CJ, Regouski M, Hall J, Olsen AL, Meng Q, Rutigliano HM, Dosdall DJ, Angel NA, Sachse FB, Seidel T, Thomas AJ, Stott R, Panter KE, Lee PM, Van Wettere AJ, Stevens JR, Wang Z, MacLeod RS, Marrouche NF, White KL. Increased susceptibility to atrial fibrillation secondary to atrial fibrosis in transgenic goats expressing transforming growth factor‐beta1. J Cardiovasc Electrophysiol 2016; 27: 1220–1229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Qureshi W, Soliman EZ, Solomon SD, Alonso A, Arking DE, Shah A, Gupta DK, Wagenknecht LE, Herrington D. Risk factors for atrial fibrillation in patients with normal versus dilated left atrium (from the Atherosclerosis Risk in Communities Study). Am J Cardiol 2014; 114: 1368–1372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Santos AB, Kraigher‐Krainer E, Gupta DK, Claggett B, Zile MR, Pieske B, Voors AA, Lefkowitz M, Bransford T, Shi V, Packer M, McMurray JJ, Shah AM, Solomon SD, Investigators P. Impaired left atrial function in heart failure with preserved ejection fraction. Eur J Heart Fail 2014; 16: 1096–1103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Tsao CW, Josephson ME, Hauser TH, O'Halloran TD, Agarwal A, Manning WJ, Yeon SB. Accuracy of electrocardiographic criteria for atrial enlargement: validation with cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2008; 10: 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Thomas L, Abhayaratna WP. Left atrial reverse remodeling: mechanisms, evaluation, and clinical significance. JACC Cardiovasc Imaging 2017; 10: 65–77. [DOI] [PubMed] [Google Scholar]
- 8. Spencer KT, Mor‐Avi V, Gorcsan J, 3rd , DeMaria AN, Kimball TR, Monaghan MJ, Perez JE, Weinert L, Bednarz J, Edelman K, Kwan OL, Glascock B, Hancock J, Baumann C, Lang RM. Effects of aging on left atrial reservoir, conduit, and booster pump function: a multi‐institution acoustic quantification study. Heart 2001; 85: 272–277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Morris DA, Takeuchi M, Krisper M, Kohncke C, Bekfani T, Carstensen T, Hassfeld S, Dorenkamp M, Otani K, Takigiku K, Izumi C, Yuda S, Sakata K, Ohte N, Tanabe K, Osmanoglou E, Kuhnle Y, Dungen HD, Nakatani S, Otsuji Y, Haverkamp W, Boldt LH. Normal values and clinical relevance of left atrial myocardial function analysed by speckle‐tracking echocardiography: multicentre study. Eur Heart J Cardiovasc Imaging 2015; 16: 364–372. [DOI] [PubMed] [Google Scholar]
- 10. Zakeri R, Moulay G, Chai Q, Ogut O, Hussain S, Takahama H, Lu T, Wang XL, Linke WA, Lee HC, Redfield MM. Left atrial remodeling and atrioventricular coupling in a canine model of early heart failure with preserved ejection fraction. Circ Heart Fail 2016: 9: pii: e003238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Oakes RS, Badger TJ, Kholmovski EG, Akoum N, Burgon NS, Fish EN, Blauer JJ, Rao SN, DiBella EV, Segerson NM, Daccarett M, Windfelder J, McGann CJ, Parker D, MacLeod RS, Marrouche NF. Detection and quantification of left atrial structural remodeling with delayed‐enhancement magnetic resonance imaging in patients with atrial fibrillation. Circulation 2009; 119: 1758–1767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hamilton‐Craig CR, Strudwick MW, Galloway GJ. T1 mapping for myocardial fibrosis by cardiac magnetic resonance relaxometry—a comprehensive technical review. Front Cardiovasc Med 2016; 3: 49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Mantymaa P, Vuolteenaho O, Marttila M, Ruskoaho H. Atrial stretch induces rapid increase in brain natriuretic peptide but not in atrial natriuretic peptide gene expression in vitro. Endocrinology 1993; 133: 1470–1473. [DOI] [PubMed] [Google Scholar]
- 14. Wakula P, Neumann B, Kienemund J, Thon‐Gutschi E, Stojakovic T, Manninger M, Scherr D, Scharnagl H, Kapl M, Pieske B, Heinzel FR. CHA2DS2‐VASc score and blood biomarkers to identify patients with atrial high‐rate episodes and paroxysmal atrial fibrillation. Europace 2017; 19: 544–551. [DOI] [PubMed] [Google Scholar]
- 15. Sonmez O, Ertem FU, Vatankulu MA, Erdogan E, Tasal A, Kucukbuzcu S, Goktekin O. Novel fibro‐inflammation markers in assessing left atrial remodeling in non‐valvular atrial fibrillation. Med Sci Monit 2014; 20: 463–470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Shah AM, Shah SJ, Anand IS, Sweitzer NK, O'Meara E, Heitner JF, Sopko G, Li G, Assmann SF, McKinlay SM, Pitt B, Pfeffer MA, Solomon SD, Investigators T. Cardiac structure and function in heart failure with preserved ejection fraction: baseline findings from the echocardiographic study of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist trial. Circ Heart Fail 2014; 7: 104–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Gupta DK, Shah AM, Castagno D, Takeuchi M, Loehr LR, Fox ER, Butler KR, Mosley TH, Kitzman DW, Solomon SD. Heart failure with preserved ejection fraction in African Americans: the ARIC (Atherosclerosis Risk In Communities) study. JACC Heart Fail 2013; 1: 156–163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Zile MR, Gottdiener JS, Hetzel SJ, McMurray JJ, Komajda M, McKelvie R, Baicu CF, Massie BM, Carson PE, Investigators IP. Prevalence and significance of alterations in cardiac structure and function in patients with heart failure and a preserved ejection fraction. Circulation 2011; 124: 2491–2501. [DOI] [PubMed] [Google Scholar]
- 19. Cioffi G, Gerdts E, Cramariuc D, Tarantini L, Di Lenarda A, Pulignano G, Sindaco DD, Stefenelli C, de Simone G. Left atrial size and force in patients with systolic chronic heart failure: comparison with healthy controls and different cardiac diseases. Exp Clin Cardiol 2010; 15: e45–e51. [PMC free article] [PubMed] [Google Scholar]
- 20. Rossi A, Cicoira M, Florea VG, Golia G, Florea ND, Khan AA, Murray ST, Nguyen JT, O'Callaghan P, Anand IS, Coats A, Zardini P, Vassanelli C, Henein M. Chronic heart failure with preserved left ventricular ejection fraction: diagnostic and prognostic value of left atrial size. Int J Cardiol 2006; 110: 386–392. [DOI] [PubMed] [Google Scholar]
- 21. Zivlas C, Triposkiadis F, Psarras S, Giamouzis G, Skoularigis I, Chryssanthopoulos S, Kapelouzou A, Ramcharitar S, Barnes E, Papasteriadis E, Cokkinos D. Left atrial volume index in patients with heart failure and severely impaired left ventricular systolic function: the role of established echocardiographic parameters, circulating cystatin C and galectin‐3. Ther Adv Cardiovasc Dis 2017; 11: 283–295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Almodares Q, Wallentin Guron C, Thurin A, Fu M, Kontogeorgos S, Thunstrom E, Johansson MC. Larger right atrium than left atrium is associated with all‐cause mortality in elderly patients with heart failure. Echocardiography 2017; 34: 662–667. [DOI] [PubMed] [Google Scholar]
- 23. Triposkiadis F, Moyssakis I, Hadjinikolaou L, Makris T, Zioris H, Hatzizaharias A, Kyriakidis M. Left atrial systolic function is depressed in idiopathic and preserved in ischemic dilated cardiomyopathy. Eur J Clin Invest 1999; 29: 905–912. [DOI] [PubMed] [Google Scholar]
- 24. Issa O, Peguero JG, Podesta C, Diaz D, De La Cruz J, Pirela D, Brenes JC. Left atrial size and heart failure hospitalization in patients with diastolic dysfunction and preserved ejection fraction. J Cardiovasc Echogr 2017; 27: 1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Morris DA, Gailani M, Vaz Perez A, Blaschke F, Dietz R, Haverkamp W, Ozcelik C. Left atrial systolic and diastolic dysfunction in heart failure with normal left ventricular ejection fraction. J Am Soc Echocardiogr 2011; 24: 651–662. [DOI] [PubMed] [Google Scholar]
- 26. Abbasi SA, Shah RV, McNulty SE, Hernandez AF, Semigran MJ, Lewis GD, Jerosch‐Herold M, Kim RJ, Redfield MM, Kwong RY. Left atrial structure and function in heart failure with preserved ejection fraction: a RELAX substudy. PLoS One 2016; 11: e0164914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Cho GY, Jo SH, Kim MK, Kim HS, Park WJ, Choi YJ, Hong KS, Oh DJ, Rhim CY. Left atrial dyssynchrony assessed by strain imaging in predicting future development of atrial fibrillation in patients with heart failure. Int J Cardiol 2009; 134: 336–341. [DOI] [PubMed] [Google Scholar]
- 28. Ohtani K, Yutani C, Nagata S, Koretsune Y, Hori M, Kamada T. High prevalence of atrial fibrosis in patients with dilated cardiomyopathy. J Am Coll Cardiol 1995; 25: 1162–1169. [DOI] [PubMed] [Google Scholar]
- 29. Duca F, Kammerlander AA, Zotter‐Tufaro C, Aschauer S, Schwaiger ML, Marzluf BA, Bonderman D, Mascherbauer J. Interstitial fibrosis, functional status, and outcomes in heart failure with preserved ejection fraction: insights from a prospective cardiac magnetic resonance imaging study. Circ Cardiovasc Imaging 2016: 9: pii: e005277. [DOI] [PubMed] [Google Scholar]
- 30. Sanders P, Morton JB, Davidson NC, Spence SJ, Vohra JK, Sparks PB, Kalman JM. Electrical remodeling of the atria in congestive heart failure: electrophysiological and electroanatomic mapping in humans. Circulation 2003; 108: 1461–1468. [DOI] [PubMed] [Google Scholar]
- 31. Neuberger HR, Mewis C, van Veldhuisen DJ, Schotten U, van Gelder IC, Allessie MA, Bohm M. Management of atrial fibrillation in patients with heart failure. Eur Heart J 2007; 28: 2568–2577. [DOI] [PubMed] [Google Scholar]
- 32. Dickstein K, Vardas PE, Auricchio A, Daubert JC, Linde C, McMurray J, Ponikowski P, Priori SG, Sutton R, van Veldhuisen DJ, Guidelines ESCCfP . Focused Update of ESC Guidelines on device therapy in heart failure: an update of the 2008 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure and the 2007 ESC guidelines for cardiac and resynchronization therapy. Developed with the special contribution of the Heart Failure Association and the European Heart Rhythm Association. Eur Heart J, 2010 2010; 31: 2677–2687. [DOI] [PubMed] [Google Scholar]
- 33. Tsang TS, Abhayaratna WP, Barnes ME, Miyasaka Y, Gersh BJ, Bailey KR, Cha SS, Seward JB. Prediction of cardiovascular outcomes with left atrial size: is volume superior to area or diameter? J Am Coll Cardiol 2006; 47: 1018–1023. [DOI] [PubMed] [Google Scholar]
- 34. Gottdiener JS, Kitzman DW, Aurigemma GP, Arnold AM, Manolio TA. Left atrial volume, geometry, and function in systolic and diastolic heart failure of persons > or =65 years of age (the cardiovascular health study). Am J Cardiol 2006; 97: 83–89. [DOI] [PubMed] [Google Scholar]
- 35. Rossi A, Temporelli PL, Quintana M, Dini FL, Ghio S, Hillis GS, Klein AL, Marsan NA, Prior DL, Yu CM, Poppe KK, Doughty RN, Whalley GA, Me RGEHFC . Independent relationship of left atrial size and mortality in patients with heart failure: an individual patient meta‐analysis of longitudinal data (MeRGE Heart Failure). Eur J Heart Fail 2009; 11: 929–936. [DOI] [PubMed] [Google Scholar]
- 36. Yang H, Negishi K, Wang Y, Nolan M, Saito M, Marwick TH. Echocardiographic screening for non‐ischaemic stage B heart failure in the community. Eur J Heart Fail 2016; 18: 1331–1339. [DOI] [PubMed] [Google Scholar]
- 37. Yamaguchi K, Yoshitomi H, Ito S, Ito S, Adachi T, Sato H, Watanabe N, Kodani N, Sugamori T, Endo A, Takahashi N, Tanabe K. Left atrial remodeling and recurrence of congestive heart failure in patients initially diagnosed with heart failure. Echocardiography 2014; 31: 936–940. [DOI] [PubMed] [Google Scholar]
- 38. Bayes‐Genis A, Vazquez R, Puig T, Fernandez‐Palomeque C, Fabregat J, Bardaji A, Pascual‐Figal D, Ordonez‐Llanos J, Valdes M, Gabarrus A, Pavon R, Pastor L, Gonzalez Juanatey JR, Almendral J, Fiol M, Nieto V, Macaya C, Cinca J, Bayes de Luna A, Group MS . Left atrial enlargement and NT‐proBNP as predictors of sudden cardiac death in patients with heart failure. Eur J Heart Fail 2007; 9: 802–807. [DOI] [PubMed] [Google Scholar]
- 39. Armstrong AC, Liu K, Lewis CE, Sidney S, Colangelo LA, Kishi S, Ambale‐Venkatesh B, Arynchyn A, Jacobs DR, Jr. , Correia LC, Gidding SS, Lima JA. Left atrial dimension and traditional cardiovascular risk factors predict 20‐year clinical cardiovascular events in young healthy adults: the CARDIA study. Eur Heart J Cardiovasc Imaging 2014; 15: 893–899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Alvarez‐Garcia J, Ferrero‐Gregori A, Puig T, Vazquez R, Delgado J, Pascual‐Figal D, Alonso‐Pulpon L, Gonzalez‐Juanatey JR, Rivera M, Worner F, Bardaji A, Cinca J, investigators of the Spanish Heart Failure N . A simple validated method for predicting the risk of hospitalization for worsening of heart failure in ambulatory patients: the Redin‐SCORE. Eur J Heart Fail 2015; 17: 818–827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Mosquera VX, Bouzas‐Mosquera A, Gonzalez‐Barbeito M, Bautista‐Hernandez V, Muniz J, Alvarez‐Garcia N, Cuenca‐Castillo JJ. Indexed left atrial size predicts all‐cause and cardiovascular mortality in patients undergoing aortic valve surgery. J Thorac Cardiovasc Surg 2017; 153: 1275–1284 e7. [DOI] [PubMed] [Google Scholar]
- 42. Donal E, Raud‐Raynier P, De Place C, Gervais R, Rosier A, Roulaud M, Ingels A, Carre F, Daubert JC, Denjean A. Resting echocardiographic assessments of left atrial function and filling pressure interest in the understanding of exercise capacity in patients with chronic congestive heart failure. J Am Soc Echocardiogr 2008; 21: 703–710. [DOI] [PubMed] [Google Scholar]
- 43. Santos AB, Roca GQ, Claggett B, Sweitzer NK, Shah SJ, Anand IS, Fang JC, Zile MR, Pitt B, Solomon SD, Shah AM. Prognostic relevance of left atrial dysfunction in heart failure with preserved ejection fraction. Circ Heart Fail 2016; 9: e002763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Olsson LG, Swedberg K, Ducharme A, Granger CB, Michelson EL, McMurray JJ, Puu M, Yusuf S, Pfeffer MA. Atrial fibrillation and risk of clinical events in chronic heart failure with and without left ventricular systolic dysfunction: results from the Candesartan in Heart failure—Assessment of Reduction in Mortality and morbidity (CHARM) program. J Am Coll Cardiol 2006; 47: 1997–2004. [DOI] [PubMed] [Google Scholar]
- 45. Rossi A, Gheorghiade M, Triposkiadis F, Solomon SD, Pieske B, Butler J. Left atrium in heart failure with preserved ejection fraction: structure, function, and significance. Circ Heart Fail 2014; 7: 1042–1049. [DOI] [PubMed] [Google Scholar]
- 46. Melenovsky V, Hwang SJ, Redfield MM, Zakeri R, Lin G, Borlaug BA. Left atrial remodeling and function in advanced heart failure with preserved or reduced ejection fraction. Circ Heart Fail 2015; 8: 295–303. [DOI] [PubMed] [Google Scholar]
- 47. von Roeder M, Rommel KP, Kowallick JT, Blazek S, Besler C, Fengler K, Lotz J, Hasenfuß G, Lücke C, Gutberlet M, Schuler G, Schuster A, Lurz P. Influence of left atrial function on exercise capacity and left ventricular function in patients with heart failure and preserved ejection fraction. Circ Cardiovasc Imaging 2017: 10: pii: e005467. [DOI] [PubMed] [Google Scholar]
- 48. Hu Y, Gurev V, Constantino J, Trayanova N. Efficient preloading of the ventricles by a properly timed atrial contraction underlies stroke work improvement in the acute response to cardiac resynchronization therapy. Heart Rhythm 2013; 10: 1800–1806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Liang HY, Cheng A, Chang KC, Berger RD, Agarwal K, Eulitt P, Corretti M, Tomaselli G, Calkins H, Kass DA, Abraham TP. Influence of atrial function and mechanical synchrony on LV hemodynamic status in heart failure patients on resynchronization therapy. JACC Cardiovasc Imaging 2011; 4: 691–698. [DOI] [PubMed] [Google Scholar]
- 50. Kono T, Sabbah HN, Rosman H, Alam M, Stein PD, Goldstein S. Left atrial contribution to ventricular filling during the course of evolving heart failure. Circulation 1992; 86: 1317–1322. [DOI] [PubMed] [Google Scholar]
- 51. Sartipy U, Dahlstrom U, Fu M, Lund LH. Atrial fibrillation in heart failure with preserved, mid‐range, and reduced ejection fraction. JACC Heart Fail 2017; 5: 565–574. [DOI] [PubMed] [Google Scholar]
- 52. Schotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial fibrillation: a translational appraisal. Physiol Rev 2011; 91: 265–325. [DOI] [PubMed] [Google Scholar]
- 53. Zakeri R, Borlaug BA, McNulty SE, Mohammed SF, Lewis GD, Semigran MJ, Deswal A, LeWinter M, Hernandez AF, Braunwald E, Redfield MM. Impact of atrial fibrillation on exercise capacity in heart failure with preserved ejection fraction: a RELAX trial ancillary study. Circ Heart Fail 2014; 7: 123–130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Lam CS, Rienstra M, Tay WT, Liu LC, Hummel YM, van der Meer P, de Boer RA, Van Gelder IC, van Veldhuisen DJ, Voors AA, Hoendermis ES. Atrial fibrillation in heart failure with preserved ejection fraction: association with exercise capacity, left ventricular filling pressures, natriuretic peptides, and left atrial volume. JACC Heart Fail 2017; 5: 92–98. [DOI] [PubMed] [Google Scholar]
- 55. Santhanakrishnan R, Wang N, Larson MG, Magnani JW, McManus DD, Lubitz SA, Ellinor PT, Cheng S, Vasan RS, Lee DS, Wang TJ, Levy D, Benjamin EJ, Ho JE. Atrial fibrillation begets heart failure and vice versa: temporal associations and differences in preserved versus reduced ejection fraction. Circulation 2016; 133: 484–492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. McGrath MF, de Bold ML, de Bold AJ. The endocrine function of the heart. Trends Endocrinol Metab 2005; 16: 469–477. [DOI] [PubMed] [Google Scholar]
- 57. Barclay JL, Kruszewski K, Croal BL, Cuthbertson BH, Oh JK, Hillis GS. Relation of left atrial volume to B‐type natriuretic peptide levels in patients with stable chronic heart failure. Am J Cardiol 2006; 98: 98–101. [DOI] [PubMed] [Google Scholar]
- 58. Lim TK, Ashrafian H, Dwivedi G, Collinson PO, Senior R. Increased left atrial volume index is an independent predictor of raised serum natriuretic peptide in patients with suspected heart failure but normal left ventricular ejection fraction: implication for diagnosis of diastolic heart failure. Eur J Heart Fail 2006; 8: 38–45. [DOI] [PubMed] [Google Scholar]
- 59. Luchner A, Stevens TL, Borgeson DD, Redfield M, Wei CM, Porter JG, Burnett JC, Jr . Differential atrial and ventricular expression of myocardial BNP during evolution of heart failure. Am J Physiol 1998; 274: H1684–H1689. [DOI] [PubMed] [Google Scholar]
- 60. Triposkiadis F, Pieske B, Butler J, Parissis J, Giamouzis G, Skoularigis J, Brutsaert D, Boudoulas H. Global left atrial failure in heart failure. Eur J Heart Fail 2016; 18: 1307–1320. [DOI] [PubMed] [Google Scholar]
- 61. Cao H, Xue L, Wu Y, Ma H, Chen L, Wang X, Zhu Q, Dai N, Chen Y. Natriuretic peptides and right atrial fibrosis in patients with paroxysmal versus persistent atrial fibrillation. Peptides 2010; 31: 1531–1539. [DOI] [PubMed] [Google Scholar]
- 62. Khalid U, Wruck LM, Quibrera PM, Bozkurt B, Nambi V, Virani SS, Jneid H, Agarwal S, Chang PP, Loehr L, Basra SS, Rosamond W, Ballantyne CM, Deswal A. BNP and obesity in acute decompensated heart failure with preserved vs. reduced ejection fraction: the Atherosclerosis Risk in Communities Surveillance Study. Int J Cardiol 2017; 233: 61–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. McKie PM, Schirger JA, Costello‐Boerrigter LC, Benike SL, Harstad LK, Bailey KR, Hodge DO, Redfield MM, Simari RD, Burnett JC, Jr. , Chen HH. Impaired natriuretic and renal endocrine response to acute volume expansion in pre‐clinical systolic and diastolic dysfunction. J Am Coll Cardiol 2011; 58: 2095–2103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Davis ME, Richards AM, Nicholls MG, Yandle TG, Frampton CM, Troughton RW. Introduction of metoprolol increases plasma B‐type cardiac natriuretic peptides in mild, stable heart failure. Circulation 2006; 113: 977–985. [DOI] [PubMed] [Google Scholar]
- 65. Wan SH, McKie PM, Schirger JA, Slusser JP, Hodge DO, Redfield MM, Burnett JC, Jr. , Chen HH. Chronic peptide therapy with B‐type natriuretic peptide in patients with pre‐clinical diastolic dysfunction (stage B heart failure). JACC Heart Fail 2016; 4: 539–547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Brubaker PH, Kitzman DW. Chronotropic incompetence: causes, consequences, and management. Circulation 2011; 123: 1010–1020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Borlaug BA, Melenovsky V, Russell SD, Kessler K, Pacak K, Becker LC, Kass DA. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation 2006; 114: 2138–2147. [DOI] [PubMed] [Google Scholar]
- 68. Sanders P, Kistler PM, Morton JB, Spence SJ, Kalman JM. Remodeling of sinus node function in patients with congestive heart failure: reduction in sinus node reserve. Circulation 2004; 110: 897–903. [DOI] [PubMed] [Google Scholar]
- 69. Kasner M, Sinning D, Lober J, Post H, Fraser AG, Pieske B, Burkhoff D, Tschope C. Heterogeneous responses of systolic and diastolic left ventricular function to exercise in patients with heart failure and preserved ejection fraction. ESC Heart Fail 2015; 2: 121–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Benjamin EJ, D'Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The Framingham Heart Study Circulation 1995; 92: 835–841. [DOI] [PubMed] [Google Scholar]
- 71. Spronk HM, De Jong AM, Verheule S, De Boer HC, Maass AH, Lau DH, Rienstra M, van Hunnik A, Kuiper M, Lumeij S, Zeemering S, Linz D, Kamphuisen PW, Ten Cate H, Crijns HJ, Van Gelder IC, van Zonneveld AJ, Schotten U. Hypercoagulability causes atrial fibrosis and promotes atrial fibrillation. Eur Heart J 2017; 38: 38–50. [DOI] [PubMed] [Google Scholar]
- 72. Do DH, Therrien J, Marelli A, Martucci G, Afilalo J, Sebag IA. Right atrial size relates to right ventricular end‐diastolic pressure in an adult population with congenital heart disease. Echocardiography 2011; 28: 109–116. [DOI] [PubMed] [Google Scholar]
- 73. Sakata K, Uesugi Y, Isaka A, Minamishima T, Matsushita K, Satoh T, Yoshino H. Evaluation of right atrial function using right atrial speckle tracking analysis in patients with pulmonary artery hypertension. J Echocardiogr 2016; 14: 30–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Omar HR, Charnigo R, Guglin M. Ratio of systolic blood pressure to right atrial pressure, a novel marker to predict morbidity and mortality in acute systolic heart failure. Am J Cardiol 2017; 119: 1061–1068. [DOI] [PubMed] [Google Scholar]
- 75. Cameli M, Sparla S, Losito M, Righini FM, Menci D, Lisi M, D'Ascenzi F, Focardi M, Favilli R, Pierli C, Fineschi M, Mondillo S. Correlation of left atrial strain and Doppler measurements with invasive measurement of left ventricular end‐diastolic pressure in patients stratified for different values of ejection fraction. Echocardiography 2016; 33: 398–405. [DOI] [PubMed] [Google Scholar]
- 76. Posina K, McLaughlin J, Rhee P, Li L, Cheng J, Schapiro W, Gulotta RJ, Berke AD, Petrossian GA, Reichek N, Cao JJ. Relationship of phasic left atrial volume and emptying function to left ventricular filling pressure: a cardiovascular magnetic resonance study. J Cardiovasc Magn Reson 2013; 15: 99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Hoit BD, Shao Y, Gabel M. Left atrial systolic and diastolic function accompanying chronic rapid pacing‐induced atrial failure. Am J Physiol 1998; 275: H183–H189. [DOI] [PubMed] [Google Scholar]
- 78. Li D, Fareh S, Leung TK, Nattel S. Promotion of atrial fibrillation by heart failure in dogs: atrial remodeling of a different sort. Circulation 1999; 100: 87–95. [DOI] [PubMed] [Google Scholar]
- 79. Schoonderwoerd BA, Ausma J, Crijns HJ, Van Veldhuisen DJ, Blaauw EH, Van Gelder IC. Atrial ultrastructural changes during experimental atrial tachycardia depend on high ventricular rate. J Cardiovasc Electrophysiol 2004; 15: 1167–117. [DOI] [PubMed] [Google Scholar]
- 80. Anne W, Willems R, Holemans P, Beckers F, Roskams T, Lenaerts I, Ector H, Heidbuchel H. Self‐terminating AF depends on electrical remodeling while persistent AF depends on additional structural changes in a rapid atrially paced sheep model. J Mol Cell Cardiol 2007; 43: 148–158. [DOI] [PubMed] [Google Scholar]
- 81. Casaclang‐Verzosa G, Gersh BJ, Tsang TS. Structural and functional remodeling of the left atrium: clinical and therapeutic implications for atrial fibrillation. J Am Coll Cardiol 2008; 51: 1–11. [DOI] [PubMed] [Google Scholar]
- 82. Zeitler EP, Friedman DJ, Daubert JP, Al‐Khatib SM, Solomon SD, Biton Y, McNitt S, Zareba W, Moss AJ, Kutyifa V. Multiple comorbidities and response to cardiac resynchronization therapy: MADIT‐CRT long‐term follow‐up. J Am Coll Cardiol 2017; 69: 2369–2379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Stahrenberg R, Duvinage A, Mende M, Gelbrich G, Auf der Heide W, Dungen HD, Binder L, Nolte K, Herrmann‐Lingen C, Hasenfuss G, Pieske B, Wachter R, Edelmann F. Determinants of submaximal exercise capacity in patients at risk for heart failure with preserved ejection fraction‐results from the DIAST‐CHF study. ESC Heart Fail 2015; 2: 76–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Kitzman DW, Little WC, Brubaker PH, Anderson RT, Hundley WG, Marburger CT, Brosnihan B, Morgan TM, Stewart KP. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA 2002; 288: 2144–2150. [DOI] [PubMed] [Google Scholar]
- 85. Weber KT, Brilla CG, Campbell SE, Guarda E, Zhou G, Sriram K. Myocardial fibrosis: role of angiotensin II and aldosterone. Basic Res Cardiol 1993; 88: 107–124. [DOI] [PubMed] [Google Scholar]
- 86. Verheule S, Sato T, Everett Tt, Engle SK, Otten D, Rubart‐von der Lohe M, Nakajima HO, Nakajima H, Field LJ, Olgin JE. Increased vulnerability to atrial fibrillation in transgenic mice with selective atrial fibrosis caused by overexpression of TGF‐beta1. Circ Res 2004; 94: 1458–1465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Damman K, Tang WH, Felker GM, Lassus J, Zannad F, Krum H, McMurray JJ. Current evidence on treatment of patients with chronic systolic heart failure and renal insufficiency: practical considerations from published data. J Am Coll Cardiol 2014; 63: 853–871. [DOI] [PubMed] [Google Scholar]
- 88. Triposkiadis F, Giamouzis G, Parissis J, Starling RC, Boudoulas H, Skoularigis J, Butler J, Filippatos G. Reframing the association and significance of co‐morbidities in heart failure. Eur J Heart Fail 2016; 18: 744–758. [DOI] [PubMed] [Google Scholar]
- 89. Bossard M, Kreuzmann R, Hochgruber T, Krisai P, Zimmermann AJ, Aeschbacher S, Pumpol K, Kessel‐Schaefer A, Stephan FP, Handschin N, Sticherling C, Osswald S, Kaufmann BA, Pare G, Kuhne M, Conen D. Determinants of left atrial volume in patients with atrial fibrillation. PLoS One 2016; 11: e0164145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Fernandes‐Cardoso A, Santos‐Furtado M, Grindler J, Ferreira LA, Andrade JL, Santo MA. Epicardial fat thickness correlates with P‐wave duration, left atrial size and decreased left ventricular systolic function in morbid obesity. Nutr Metab Cardiovasc Dis 2017; 27: 731–738. [DOI] [PubMed] [Google Scholar]
- 91. Oliver W, Matthews G, Ayers CR, Garg S, Gupta S, Neeland IJ, Drazner MH, Berry JD, Matulevicius S, de Lemos JA. Factors associated with left atrial remodeling in the general population. Circ Cardiovasc Imaging 2017; 10: pii: e005047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Dinov B, Kosiuk J, Kircher S, Bollmann A, Acou WJ, Arya A, Hindricks G, Rolf S. Impact of metabolic syndrome on left atrial electroanatomical remodeling and outcomes after radiofrequency ablation of nonvalvular atrial fibrillation. Circ Arrhythm Electrophysiol 2014; 7: 483–489. [DOI] [PubMed] [Google Scholar]
- 93. Cavalera M, Wang J, Frangogiannis NG. Obesity, metabolic dysfunction, and cardiac fibrosis: pathophysiological pathways, molecular mechanisms, and therapeutic opportunities. Transl Res 2014; 164: 323–335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Mary‐Rabine L, Albert A, Pham TD, Hordof A, Fenoglio JJ, Jr. , Malm JR, Rosen MR. The relationship of human atrial cellular electrophysiology to clinical function and ultrastructure. Circ Res 1983; 52: 188–199. [DOI] [PubMed] [Google Scholar]
- 95. Shi Y, Ducharme A, Li D, Gaspo R, Nattel S, Tardif JC. Remodeling of atrial dimensions and emptying function in canine models of atrial fibrillation. Cardiovasc Res 2001; 52: 217–225. [DOI] [PubMed] [Google Scholar]
- 96. Chao TF, Liu CJ, Chen SJ, Wang KL, Lin YJ, Chang SL, Lo LW, Hu YF, Tuan TC, Wu TJ, Chen TJ, Chen SA. CHADS2 score and risk of new‐onset atrial fibrillation: a nationwide cohort study in Taiwan. Int J Cardiol 2013; 168: 1360–1363. [DOI] [PubMed] [Google Scholar]
- 97. Fengler A, Krisper FEM, Hassfeld S, Decius I, Koehncke C, Kapl M, Pieske B, Blaschke FRH. CHADS2VASc score identifies patients with diastolic dysfunction and heart failure with preserved ejection fraction. Eur Heart J 2016; 37: 718. [Google Scholar]
- 98. Khatib R, Joseph P, Briel M, Yusuf S, Healey J. Blockade of the renin–angiotensin–aldosterone system (RAAS) for primary prevention of non‐valvular atrial fibrillation: a systematic review and meta analysis of randomized controlled trials. Int J Cardiol 2013; 165: 17–24. [DOI] [PubMed] [Google Scholar]
- 99. Kloosterman M, Rienstra M, Mulder BA, Van Gelder IC, Maass AH. Atrial reverse remodelling is associated with outcome of cardiac resynchronization therapy. Europace 2016; 18: 1211–1219. [DOI] [PubMed] [Google Scholar]
- 100. Abed HS, Wittert GA, Leong DP, Shirazi MG, Bahrami B, Middeldorp ME, Lorimer MF, Lau DH, Antic NA, Brooks AG, Abhayaratna WP, Kalman JM, Sanders P. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA 2013; 310: 2050–2060. [DOI] [PubMed] [Google Scholar]
- 101. Edelmann F, Gelbrich G, Dungen HD, Frohling S, Wachter R, Stahrenberg R, Binder L, Topper A, Lashki DJ, Schwarz S, Herrmann‐Lingen C, Loffler M, Hasenfuss G, Halle M, Pieske B. Exercise training improves exercise capacity and diastolic function in patients with heart failure with preserved ejection fraction: results of the Ex‐DHF (Exercise training in Diastolic Heart Failure) pilot study. J Am Coll Cardiol 2011; 58: 1780–1791. [DOI] [PubMed] [Google Scholar]
- 102. Tsang TS, Barnes ME, Abhayaratna WP, Cha SS, Gersh BJ, Langins AP, Green TD, Bailey KR, Miyasaka Y, Seward JB. Effects of quinapril on left atrial structural remodeling and arterial stiffness. Am J Cardiol 2006; 97: 916–920. [DOI] [PubMed] [Google Scholar]
- 103. Kokubu N, Yuda S, Tsuchihashi K, Hashimoto A, Nakata T, Miura T, Ura N, Nagao K, Tsuzuki M, Wakabayashi C, Shimamoto K. Noninvasive assessment of left atrial function by strain rate imaging in patients with hypertension: a possible beneficial effect of renin–angiotensin system inhibition on left atrial function. Hypertens Res 2007; 30: 13–21. [DOI] [PubMed] [Google Scholar]
- 104. Thomas L, McKay T, Byth K, Marwick TH. Abnormalities of left atrial function after cardioversion: an atrial strain rate study. Heart 2007; 93: 89–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. Sanders P, Morton JB, Kistler PM, Vohra JK, Kalman JM, Sparks PB. Reversal of atrial mechanical dysfunction after cardioversion of atrial fibrillation: implications for the mechanisms of tachycardia‐mediated atrial cardiomyopathy. Circulation 2003; 108: 1976–1984. [DOI] [PubMed] [Google Scholar]
- 106. McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, Rouleau JL, Shi VC, Solomon SD, Swedberg K, Zile MR, Investigators P‐H, Committees . Angiotensin‐neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014; 371: 993–1004. [DOI] [PubMed] [Google Scholar]
- 107. Solomon SD, Zile M, Pieske B, Voors A, Shah A, Kraigher‐Krainer E, Shi V, Bransford T, Takeuchi M, Gong J, Lefkowitz M, Packer M, McMurray JJ, Prospective comparison of AwARBoMOhfwpefI . The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double‐blind randomised controlled trial. Lancet 2012; 380: 1387–1395. [DOI] [PubMed] [Google Scholar]
- 108. Jhund PS, Claggett B, Packer M, Zile MR, Voors AA, Pieske B, Lefkowitz M, Shi V, Bransford T, McMurray JJ, Solomon SD. Independence of the blood pressure lowering effect and efficacy of the angiotensin receptor neprilysin inhibitor, LCZ696, in patients with heart failure with preserved ejection fraction: an analysis of the PARAMOUNT trial. Eur J Heart Fail 2014; 16: 671–677. [DOI] [PubMed] [Google Scholar]
- 109. Lam PH, Dooley DJ, Deedwania P, Singh SN, Bhatt DL, Morgan CJ, Butler J, Mohammed SF, Wu WC, Panjrath G, Zile MR, White M, Arundel C, Love TE, Blackman MR, Allman RM, Aronow WS, Anker SD, Fonarow GC, Ahmed A. Heart rate and outcomes in hospitalized patients with heart failure with preserved ejection fraction. J Am Coll Cardiol 2017; 70: 1861–1871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Donal E, Tan K, Leclercq C, Ollivier R, Derumeaux G, Bernard M, de Place C, Mabo P, Daubert JC. Left atrial reverse remodeling and cardiac resynchronization therapy for chronic heart failure patients in sinus rhythm. J Am Soc Echocardiogr 2009; 22: 1152–1158. [DOI] [PubMed] [Google Scholar]
- 111. Tops LF, Delgado V, Bertini M, Marsan NA, De Uijl DW, Trines SA, Zeppenfeld K, Holman E, Schalij MJ, Bax JJ. Left atrial strain predicts reverse remodeling after catheter ablation for atrial fibrillation. J Am Coll Cardiol 2011; 57: 324–331. [DOI] [PubMed] [Google Scholar]
- 112. Marsan NA, Tops LF, Holman ER, Van de Veire NR, Zeppenfeld K, Boersma E, van der Wall EE, Schalij MJ, Bax JJ. Comparison of left atrial volumes and function by real‐time three‐dimensional echocardiography in patients having catheter ablation for atrial fibrillation with persistence of sinus rhythm versus recurrent atrial fibrillation three months later. Am J Cardiol 2008; 102: 847–853. [DOI] [PubMed] [Google Scholar]
- 113. Santarpino G, Rubino AS, Onorati F, Curcio A, Torella D, Tucci L, Indolfi C, Renzulli A. Atrial fibrillation ablation induces reverse remodelling and impacts cardiac function. Minerva Cardioangiol 2011; 59: 17–29. [PubMed] [Google Scholar]
- 114. Nagase T, Kato R, Nakano S, Shiki Y, Tanaka S, Ikeda Y, Iwanaga S, Nishimura S, Matsumoto K. Prediction of improvement in left atrial function index after catheter ablation for atrial fibrillation. J Interv Card Electrophysiol 2015; 44: 151–160. [DOI] [PubMed] [Google Scholar]
- 115. Marrouche NF, Brachmann J, Committee C‐AS. Catheter ablation versus standard conventional treatment in patients with left ventricular dysfunction and atrial fibrillation (CASTLE‐AF)—study design. Pacing Clin Electrophysiol 2009; 32: 987–994. [DOI] [PubMed] [Google Scholar]
- 116. Lip GY, Shantsila E. Anticoagulation versus placebo for heart failure in sinus rhythm. Cochrane Database Syst Rev 2014; 3: CD003336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117. Katsanos AH, Parissis J, Frogoudaki A, Vrettou AR, Ikonomidis I, Paraskevaidis I, Triantafyllou N, Kargiotis O, Voumvourakis K, Alexandrov AV, Tsivgoulis G. Heart failure and the risk of ischemic stroke recurrence: a systematic review and meta‐analysis. J Neurol Sci 2016; 362: 182–187. [DOI] [PubMed] [Google Scholar]
- 118. Melgaard L, Gorst‐Rasmussen A, Lane DA, Rasmussen LH, Larsen TB, Lip GY. Assessment of the CHA2DS2‐VAS score in predicting ischemic stroke, thromboembolism, and death in patients with heart failure with and without atrial fibrillation. JAMA 2015; 314: 1030–1038. [DOI] [PubMed] [Google Scholar]
- 119. Yaghi S, Moon YP, Mora‐McLaughlin C, Willey JZ, Cheung K, Di Tullio MR, Homma S, Kamel H, Sacco RL, Elkind MS. Left atrial enlargement and stroke recurrence: the Northern Manhattan Stroke Study. Stroke 2015; 46: 1488–1493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120. Edelmann F, Holzendorf V, Wachter R, Nolte K, Schmidt AG, Kraigher‐Krainer E, Duvinage A, Unkelbach I, Dungen HD, Tschope C, Herrmann‐Lingen C, Halle M, Hasenfuss G, Gelbrich G, Stough WG, Pieske BM. Galectin‐3 in patients with heart failure with preserved ejection fraction: results from the Aldo‐DHF trial. Eur J Heart Fail 2015; 17: 214–223. [DOI] [PubMed] [Google Scholar]
- 121. Yalcin MU, Gurses KM, Kocyigit D, Canpinar H, Canpolat U, Evranos B, Yorgun H, Sahiner ML, Kaya EB, Hazirolan T, Tokgozoglu L, Oto MA, Ozer N, Guc D, Aytemir K. The association of serum galectin‐3 levels with atrial electrical and structural remodeling. J Cardiovasc Electrophysiol 2015; 26: 635–640. [DOI] [PubMed] [Google Scholar]
- 122. O'Neal WT, Venkatesh S, Broughton ST, Griffin WF, Soliman EZ. Biomarkers and the prediction of atrial fibrillation: state of the art. Vasc Health Risk Manag 2016; 12: 297–303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Armstrong EJ, Morrow DA, Sabatine MS. Inflammatory biomarkers in acute coronary syndromes: part I: introduction and cytokines. Circulation 2006; 113: e72–e75. [DOI] [PubMed] [Google Scholar]
- 124. Vasan RS, Sullivan LM, Roubenoff R, Dinarello CA, Harris T, Benjamin EJ, Sawyer DB, Levy D, Wilson PW, D'Agostino RB, Framingham Heart S. Inflammatory markers and risk of heart failure in elderly subjects without prior myocardial infarction: the Framingham Heart Study. Circulation 2003; 107: 1486–1491. [DOI] [PubMed] [Google Scholar]
- 125. Jumeau C, Rupin A, Chieng‐Yane P, Mougenot N, Zahr N, David‐Dufilho M, Hatem SN. Direct thrombin inhibitors prevent left atrial remodeling associated with heart failure in rats. JACC Basic Transl Sci 2016; 1: 328–339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Daccarett M, Badger TJ, Akoum N, Burgon NS, Mahnkopf C, Vergara G, Kholmovski E, McGann CJ, Parker D, Brachmann J, Macleod RS, Marrouche NF. Association of left atrial fibrosis detected by delayed‐enhancement magnetic resonance imaging and the risk of stroke in patients with atrial fibrillation. J Am Coll Cardiol 2011; 57: 831–838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127. Schotten U, Maesen B, Zeemering S. The need for standardization of time‐ and frequency‐domain analysis of body surface electrocardiograms for assessment of the atrial fibrillation substrate. Europace 2012; 14: 1072–1075. [DOI] [PubMed] [Google Scholar]
- 128. Lankveld TA, Zeemering S, Crijns HJ, Schotten U. The ECG as a tool to determine atrial fibrillation complexity. Heart 2014; 100: 1077–1084. [DOI] [PubMed] [Google Scholar]
- 129. Abdul‐Rahim AH, Perez AC, MacIsaac RL, Jhund PS, Claggett BL, Carson PE, Komajda M, McKelvie RS, Zile MR, Swedberg K, Yusuf S, Pfeffer MA, Solomon SD, Lip GYH, Lees KR, McMurray JJV, Candesartan in Heart failure Assessment of Reduction in M, Morbidity P, the Irbesartan in Heart Failure with Preserved Systolic Function Steering C . Risk of stroke in chronic heart failure patients with preserved ejection fraction, but without atrial fibrillation: analysis of the CHARM‐Preserved and I‐Preserve trials. Eur Heart J 2017; 38: 742–750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Sobue Y, Watanabe E, Lip GYH, Koshikawa M, Ichikawa T, Kawai M, Harada M, Inamasu J, Ozaki Y. Thromboembolisms in atrial fibrillation and heart failure patients with a preserved ejection fraction (HFpEF) compared to those with a reduced ejection fraction (HFrEF). Heart Vessels, 2017. [DOI] [PubMed]
- 131. Edelmann F, Gelbrich G, Duvinage A, Stahrenberg R, Behrens A, Prettin C, Kraigher‐Krainer E, Schmidt AG, Dungen HD, Kamke W, Tschope C, Herrmann‐Lingen C, Halle M, Hasenfuss G, Wachter R, Pieske B. Differential interaction of clinical characteristics with key functional parameters in heart failure with preserved ejection fraction—results of the Aldo‐DHF trial. Int J Cardiol 2013; 169: 408–417. [DOI] [PubMed] [Google Scholar]
- 132. Phan TT, Shivu GN, Abozguia K, Davies C, Nassimizadeh M, Jimenez D, Weaver R, Ahmed I, Frenneaux M. Impaired heart rate recovery and chronotropic incompetence in patients with heart failure with preserved ejection fraction. Circ Heart Fail 2010; 3: 29–34. [DOI] [PubMed] [Google Scholar]