

Abstract
Objectives:
Extracorporeal shockwave therapy (ESWT) and corticosteroid injection (CSI) are treatment options for plantar fasciitis. Their clinical outcome comparison remains a debate. Also, the thickness changes of the plantar fascia on objective evaluation under the medium energy ESWT and CSI therapy are elusive.
Methods:
A total of 97 patients with chronic plantar fasciitis were enrolled in the randomized prospective trial. Forty-seven patients received extracorporeal shock wave therapy (ESWT), and fifty patients received corticosteroid injection (CSI). The thickness of the plantar fascia was evaluated respectively before ESWT and CSI, and at the 4th and 12th week after ESWT and CSI by ultrasonography. Pain level and clinical outcomes were recorded using visual analogue scale (VAS) and 100-points scoring systems. Correlation analysis was performed between the thickness change and clinical outcome.
Results:
Under ultrasonography, we observed more increase of plantar fascia thickness of ESWT group than CSI group at 4th week (p=0.048). VAS of plantar fasciitis patients receiving ESWT was lower than those who received corticosteroid injection (0.001 and p<0.001, at 4th and 12th week). On the assessment of 100-points scoring systems, the pain level of patients with ESWT was lower than those with CSI at the 12th week (p<0.001). On the other hand, the increase of plantar fascia thickness at 4th week was positively correlated with the decrease of VAS score at 12th week follow-up (R=0.302, P=0.039).
Conclusions:
At 4th week after treatment, the thickness of plantar fascia increased. Then it decreased gradually, but not to the baseline at 12th week. On the pain level outcome at 12th week, extracorporeal shockwave therapy (ESWT) was more efficient than corticosteroid injection (CSI) on chronic plantar fasciitis. The more change of plantar fascia after ESWT, the more efficient on clinical outcome.
Keywords: Plantar Fasciitis, Extracorporeal Shock Wave Therapy, Corticosteroid Injection, Visual Analogue Scale, Ultrasonography
Introduction
Plantar fasciitis is a common musculoskeletal problem. It denotes a clinical condition of pain in the plantar aspect of the heel, characteristically worse on arising in the morning and after periods of prolonged sitting. The tender points are located at the plantar fascia origin on the medial process of the calcaneal tuberosity, and pain increases with passive stretching of the plantar fascia. The etiology of plantar fasciitis still remains unknown, and probably multifactorial, which include chronic inflammation, degeneration, and microtrauma of the plantar fascia, entrapment of lateral planter nerve, overuse syndrome, heel spurs, heel pad atrophy, and seronegative arthritis-induced inflammation[1-9]. Treatment modalities include physiotherapy, surgical release, nonsteroidal anti-inflammatory drugs (NSAIDs), extracorporeal shockwave therapy (ESWT), and corticosteroid injection (CSI)[10-13].
Recently, many studies have shown the efficacy of extracorporeal shock wave therapy (ESWT) for soft tissue. The outome may be highly dependent on machine type (electrohydraulic, electromagnetic, and piezoelectric systems) and treatment protocols[4,5,13]. The energy levels are categorized into high (>0.60 mJ/mm2), medium (0.28-0.59 mJ/mm2), and low (0.08-0.27 mJ/mm2)[14]. Animal studies hint that there is a critical dose for tissue injury of ESWT on the rat Achilles tendon, and suggest 1000 impulses of 0.28 mJ/mm2 is a reasonable safe dose[15-16]. Side effects, such as bone marrow edema, osteonecrosis, and tendon ruptures are rare but occur in high energy shock wave therapy[17-20]. Many studies reveal that low energy ESWT for plantar fasciitis don’t show evidence of clinical benefit over other non-operative modalities[2,21,22].
Marier et al. reported that the presence of calcaneal bone marrow edema on pre-therapeutic MRI was a highly predictive variable for satisfactory clinical outcome of chronic plantar fasciitis treated by ESWT[23]. Hammer and his colleagues reported that the thickness of the plantar fascia with plantar fasciitis under sonography decreased at the sixth month, and pain and walking time improved after moderate energy ESWT[11].
In 2005, Porter et al. compared the efficacy of extracorporeal shock wave therapy (ESWT) and intralesional corticosteroid injection (CSI) for the treatment of plantar fasciopathy. They revealed corticosteroid injection was more efficacious and cost-effective than ESWT in the treatment of plantar fasciopathy. However, in 2012, Saber et al. performed a randomized controlled trial, that showed ESWT was as useful as CSI for relieving symptoms of plantar fasciitis. Therefore, the outcome of corticosteroid injection (CSI) and extracorporeal shock wave therapy (ESWT) as primary treatment of plantar fasciitis remains elusive[25,26].
The purpose of the present study is not only to evaluate and compare the therapeutic effects of CSI and moderate energy ESWT in patients with chronic (>2 months duration) symptomatic plantar fasciitis, but also further examine the correlation between the thickness changes and the clinical outcomes.
Materials and methods
Inclusion criteria
We enrolled 130 patients with chronic plantar fasciitis more than two months without injection history in the study between 2013 and 2014. 20 patients were excluded due to incomplete clinical follow-up or inadequate randomization. The 110 cases were randomly assigned to receive ESWT and CSI. 55 patients received ESWT and 55 patients received CSI. Generating a random allocation sequence include using a computer software program that generates the random sequence. https://www.random.org/sequences/?min=1&max=100&col=2&format=html&rnd=new. At final follow-up, 8 patients in ESWT group and 5 patients in CSI group didn’t finish complete ultrasonography, VAS, or 100-points score records. There were 47 patients in ESWT group and 50 patients in CSI group completed the 3-months study.
These patients had been treated with plantar stretching exercise, gastrocnemius stretching, or shoe modification for one month, but showed little or no improvement before proceeding to ESTW or CSI treatment. Informed consents were obtained from all patients in accordance with the Declaration of Helsinki. This study had been approved by the ethics committee of the Institutional Review Board (IRB) in Show Chwan hospital (IRB No.1031203). Patients with a cardiac pacemaker, previous surgery involving the foot, autoimmune or systemic inflammatory disorder, coagulation disorder or anticoagulant, calcaneal fracture, infections, pregnancy and peripheral neuropathy, or accepting other therapeutic modalities were excluded. The bilateral plantar fasciitis was excluded to produce a more homogenous group. The average symptoms duration before visiting was about 2 months. After 1-month conservative treatment failure, the patients maybe enroll in this study.
Extracorporeal shock wave therapy (ESWT)
The ESWT technique followed the OrthospecTM device instrument guideline (Medispec, Montgomery Village, America). The shockwave probe of this device is wide focused type and energy level ranged from 0.07 to 0.32 mJ/mm2. All of these procedures were performed by Dr. Liu (12 years experienced orthopedic doctor). The patients started on the lowest intensity level 1 (0.07 mJ/mm2), and increased intensity level as patients’ tolerance gradually to level 6 (0.29 mJ/mm2). The stable energy level 6 (0.29 mJ/mm2) was kept for 25 minutes to achieve total 1500 shock in each treatment. The operation time of each session of ESWT was about 30 minutes. The patients came to receive 2nd section of ESWT 2 weeks after first ESWT. Two sessions of ESWT at an interval of 2 weeks was to avoid treatment induced heel pain or plantar fascia rupture due to median energy shock wave. The subjects will have temporary local tenderness subsided in three to four days after shockwave therapy.
Plantar fascia thickness evaluation
The high-resolution ultrasound (frequency transducers: 12 MHz, GE Healthcare Life Sciences, UK) used by radiologists to check the plantar fascia thickness. The plantar fascia thickness was measured at the plantar fascia insertion 5mm distal to calcaneus tuberosity. Each examination was repeated by the two radiologists independently and an average was taken. The radiologists were blinded of treatment methods (ESWT or CSI). The thickness of the plantar fascia was evaluated before ESWT or CSI, 4 weeks, and 12 weeks after first ESWT or steroid injection by radiologist using ultrasonography. Therefore, every patient received 6 times measurements from ultrasonography.
Corticosteroid injection (CSI)
CSI group after measure plantar fascia thickness, a small dot marker was made by radiologist under ultrasonography. For CSI, 20 mg triamcinolone acetonite with 2 ml 2% xylocaine were injected into the marker by Dr. Lai (10-years experience orthopedic doctor). The subjects will have temporary local pain at injection site about 2-3 days.
Outcome evaluation
Pain level and outcomes were recorded using visual analogue scale (VAS) (0-10) and 100-points scoring system (70 points for pain scores, 30 points for functional scores) at the start before ESWT or CSI, 4 weeks after first treatment, and 12 weeks after first treatment by Dr. Ma and Dr. Tan (20-years experience orthopedic doctor). In 100-points scoring system, the pain scores include pain on level walking, start up pain, and pressure pain. The functional scores include pain at work, pain during free times, and pain at night. Better function has a higher score. The details of 100-points scoring systems were demonstrated in a previous literature[9]. The clinical outcomes using the visual analog scale (VAS) and 100-points scoring systems are recorded and compared at the 4th week and 12th week follow-up visit between CSI and ESWT. The present clinical trial study is designed to examine and compare the effect of the 2 treatment options, CSI and ESWT, on chronic plantar fasciitis.
Statistic analysis
Nonparametric tests were used in this study according to hypothesis tests for thickness of the plantar fascia, 10-point VAS, and 100-points scoring systems. The Mann-Whitney u test was performed for comparison of the thickness of the plantar fascia and pain scores between ESWT and CSI group. Spearman correlation coefficients were calculated between 4th week thickness change of plantar fascia and 12th week clinical outcomes (VAS score and 100-point scoring) using SPSS software (Version 18.0 SPSS Inc., Chicago, IL).
Results
There was no statistically significant difference between ESWT and CSI group in age, gender, location and duration of symptoms. As shown in [Table 1], in ESWT patients, the mean age is 54.53±8.62, and the gender ratio is 26:21 (female: male). The left leg plantar fascia number is roughly equal to the right leg number (23:24), and the average of duration of symptoms is 7.94±2.92 weeks. In CSI patients, the mean age is 54.58±8.63, and the gender of ratio is 28:22 (female: male). The left leg plantar fascia number is roughly equal to the right leg number (24:26), and the average duration of symptoms is 8.06±2.87 weeks. During the 12-week study period, no other treatment modalities are used in the study patients except short-term acetaminophen for pain relief after ESWT or steroid injection.
Table 1.
The basic characteristics of patients.
| ESWT | Corticosteroid injections | p-value | |
|---|---|---|---|
| Clinical parameters | (N=47) | (N=50) | |
| Age (mean±SD) | 54.53±8.62 | 54.58 ±8.63 | 0.834a |
| Range | |||
| Gender | |||
| Female | 26 (55.3) | 28 (56.0) | 0.946b |
| Male | 21 (44.7) | 22 (44.0) | |
| Leg | |||
| Left | 23 (48.9) | 24 (48.0) | 0.927b |
| Right | 24 (51.1) | 26 (52.0) | |
| Duration of symptoms (weeks) | 7.94±2.92 | 8.06 ±2.87 | 0.834a |
ESWT: extracorporeal shock wave therapy.
Independent t-test for p-value.
Pearson Chi-square (x2) test for p-value.
At fourth week, the mean thickness of the plantar fascia in ESWT group was from 0.37±0.07, to 0.46±0.08 cm. The mean thickness of the plantar fascia in CSI group was from 0.38±0.06, to 0.43±0.09 cm. There was a marginally statistical significance of thickness increase of the plantar fascia under ESWT in comparison to CSI treatment at 4th week (P=0.048, Table 2). At the 12th week, the mean thickness of the plantar fascia of the ESWT group was from 0.37±0.07 to 0.38±0.07 cm, and the CSI group was from 0.38±0.06 to 0.39±0.07 cm (Table 3).
Table 2.
PF thickness, VAS, and 100-point scoring from pre-treatment to 4 weeks after treatment in patients who received ESWT and corticosteroid injections, respectively.
| 4 weeks after treatment | 4 weeks after treatment | ||||
|---|---|---|---|---|---|
| Baseline | ESWT | Baseline | Corticosteroid injections | p-value | |
| PF thickness | 0.37 ±0.07 | 0.46 ±0.08 | 0.38 ±0.06 | 0.43 ±0.09 | 0.048* |
| VAS | 6.23 ±1.11 | 3.40 ±1.08 | 6.24 ± 1.10 | 4.10 ±0.81 | 0.001** |
| 100-point scoring | 31.74 ±4.61 | 72.11 ±11.09 | 31.84 ±4.44 | 70.38 ±8.55 | 0.391 |
| Pain Scores | 21.51 ±4.17 | 52.94 ±9.25 | 21.60 ±4.27 | 51.66 ±7.90 | 0.466 |
| Functional Scores | 10.23 ±2.26 | 19.17 ±3.45 | 10.24 ±1.52 | 18.72 ±1.49 | 0.401 |
PF: plantar fascia. VAS: 10-point visual analogue scale. ESWT: extracorporeal shock wave therapy. Mann-Whitney u test for comparison of the thickness of the plantar fascia and pain scores ESWT and CSI group for p-value.
: p<0.01,
: p<0.05.
Table 3.
PF thickness, VAS, and 100-point scoring from pre-treatment to 12 weeks after treatment in patients who received ESWT and corticosteroid injections, respectively.
| 12 weeks after treatment | 12 weeks after treatment | ||||
|---|---|---|---|---|---|
| Baseline | ESWT | Baseline | Corticosteroid injections | p-value | |
| PF thickness | 0.37 ±0.07 | 0.38 ±0.07 | 0.38 ±0.06 | 0.39 ±0.07 | 0.326 |
| VAS | 6.23 ± 1.11 | 1.34 ±1.24 | 6.24 ±1.10 | 2.98 ± 0.84 | <0.001*** |
| 100-point scoring | 31.74 ±4.61 | 85.28 ±12.61 | 31.84 ±4.44 | 76.36 ±10.25 | <0.001*** |
| Pain Scores | 21.51 ±4.17 | 62.57 ±9.71 | 21.60 ±4.27 | 54.52 ±9.13 | <0.001*** |
| Functional Scores | 10.23 ±2.26 | 22.70 ±3.92 | 10.24 ±1.52 | 21.84 ±2.10 | 0.177 |
PF: plantar fascia. VAS: 10-point visual analogue scale. ESWT: extracorporeal shock wave therapy. Mann-Whitney u test for comparison of the thickness of the plantar fascia and pain scores ESWT and CSI group for p-value.
: p<0.001.
Our data show thickness of the plantar fasciitis in the measurement of baseline was not significantly associated the VAS score and 100-points scoring systems by stratifying <4 mm and >4 mm thickness of the plantar fasciitis (P=0.827 and P=0.814, respectively; data not shown). The >4 mm thickness of the plantar fasciitis could not be associated refractory cases. Presently, the previous studies have not reported that refractory cases are associated with thickness of the plantar fasciitis. Overall, the plantar fascia thickness increased in both groups at the 4th week, and more in ESWT than CSI under ultrasonography (Figure 1A). However, the thickness at 12th week decreased gradually than it at the 4th week (Figure 1A). But the average thickness remained slightly higher than the baseline. A representative plantar fascia picture of ultrasonography under ESWT at 0-week, 4-week and 12-week was shown in [Figure 1B, 1C and 1D].
Figure 1.
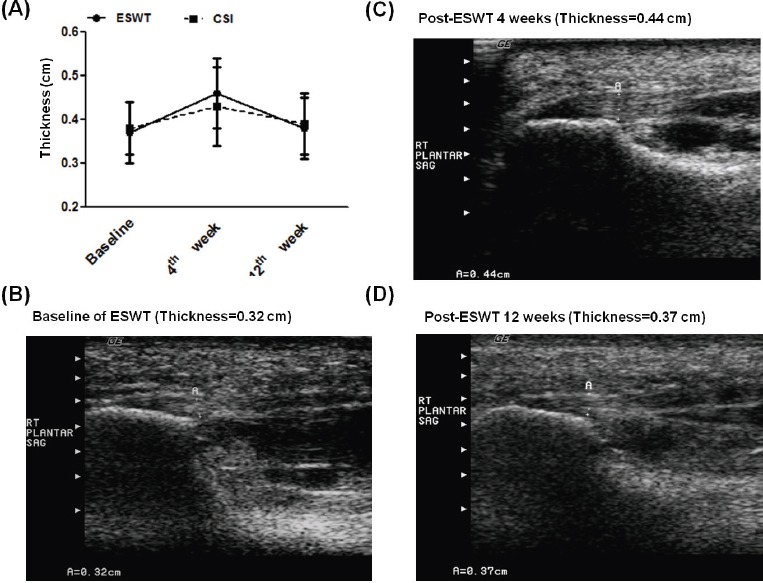
(A) The ultrasonographic trend of thickness changes of plantar fascia in the extracorporeal shockwave therapy (ESWT) and corticosteroid injection (CSI) groups. (B) (C) (D) Representative patient of ESWT-induced thickness of plantar fascia were examined by ultrasonography at 0, 4-week, and 12-week follow-up. The thickness of plantar fascia increased at first month after ESWT, than decreased at 3rd month after treatment. PF: plantar fascia.
In clinical outcome, the VAS score of ESWT group was lower than that of CSI group at 4-week and 12-week follow-up (P=0.001, P<0.001) (Table 2,3, Figure 2A). In the 100-point scoring system, the scores were higher in ESWT group than those in CSI therapy at 12-week follow-up (85.28 versus 76.36, P<0.001).
Figure 2.
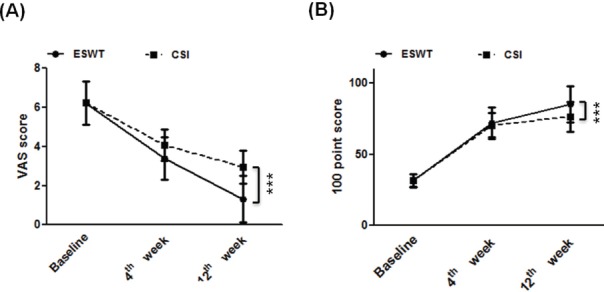
(A) The visual analog scale (VAS) score and (B) 100-points scoring systems change for plantar fascia in the extracorporeal shock wave therapy and corticosteroid injection groups at 0, 4-week, and 12-week follow-up (*, P<0.05; **, P<0.01; ***, P<0.001).
In correlation analysis, it was found that thickness increase of plantar fascia at 4th week was positively correlated with the VAS score at 12th week (R=0.302, P=0.039) (Table 4). In total, 97 patients completed the parallel-randomized trial of CSI and ESWT. Collectively, ESWT was more efficacious than CSI in the treatment of plantar fasciitis in the 12-weeks assessment of VAS and 100-point score. The plantar fascia thickness increased from the baseline to 4th week after treatment, then decreased gradually to 12th week, but not to the baseline.
Table 4.
Spearman correlation coefficients, and p value between increase of plantar fascia thickness and 12th week clinical outcomes (VAS score and 100-point scoring).
| Increase of plantar fascia thickness at 4th week versus VAS score | Increase of plantar fascia thickness at 4th week versus 100-point scoring | Increase of plantar fascia thickness at 12th week versus VAS score | Increase of plantar fascia thickness at 12th week versus 100-point scoring | |
|---|---|---|---|---|
| ESWT group | ||||
| Correlation | 0.302 | 0.121 | 0.065 | 0.133 |
| P-value | 0.039* | 0.419 | 0.664 | 0.372 |
| CSI group | ||||
| Correlation | 0.022 | 0.231 | 0.009 | 0.065 |
| P-value | 0.882 | 0.106 | 0.950 | 0.651 |
VAS: 10-point visual analogue scale. ESWT: extracorporeal shock wave therapy. Spearman’s rank correlation coefficient for correlation coefficients and p value.
p<0.05.
Discussion
The results of this study indicate that moderate energy ESWT is more effective in the management of chronic plantar fasciitis than corticosteroid injection. The difference increases gradually by time (Figure 2A). These findings support and extend previous studies examining the relationship between ESWT for plantar fasciitis and treatment outcome. Moreover, the ultrasonographic findings in our study reveal that the thickness of plantar fascia increase under ESWT in the first month (from 0.37±0.07 to 0.46±0.08 cm), then gradually decrease to the baseline at the 3rd month after treatment (Figure 1). The increase of the plantar fascia thickness is in positive correlation to the clinical outcome (Table 4).
Previous studies examining the relationship between ESWT and CSI for plantar fasciitis had diverse outcomes on different machines, energy levels, and treatment protocols[26-30]. In 2005, Hammer et al. reported the thickness decreased gradually at 6 months after ESWT, and the clinical symptoms improved. However, the short-term ultrasonographic change of plantar fascia is still not reported. In our study, the thickness of plantar fascia increased at the first 4 weeks, and then it almost restored to the baseline at the 12th week (Table 3, Table 4, and Figure 1A). We predict it will decrease contineously as Hammer’s report at 6 months after ESWT. However, we have no long term follow to come to this conclusion[12].
In 2002 and 03, Wang et al. reported molecular studies of ESWT. The rise of angiogenic markers occurred in as early as one week and only lasted for approximately 8 weeks, whereas the neovascularization was first noted in 4 weeks and persisted for 12 weeks or longer along with cell proliferation[31]. Under the mechanism, the thickness of plantar fascia should increase in the early stage after ESWT. Our study results supported this phenomenon. Additionally, shock waves have been used in the treatment of calcified tendonitis of the rotator cuff, nonunion of bone, chronic tennis elbow, and painful heel syndrome[11,13,17,19]. The efficacy of ESWT was controversial in previous studies. The success rates range from 40% to 80%[16,21,24,32], and the results are affected by symptom duration[33]. The machine type and the delivered energy level are different in different studies[34-35]. We used the moderate energy level, two-session strategy, large therapy zone ESWT machine to reduce inter-treatment bios. In clinical outcome, the results of the VAS score and 100-point scoring revealed that moderate energy ESWT was more effective than CSI in the management of chronic plantar fasciitis. No osteonecrosis or tendon rupture occurred in our study.
The ultrasonographic evaluation of plantar fasciitis is a powerful and cost-effective tool[36-37]. The cost of ultrasonography is much lower than MRI. In Taiwan, the ultrasonography was 1800 NTD (55 USD), and MRI was 8500 NTD (271 USD). Under MRI evaluation, moderate or marked hyperemia was found in the plantar fascia and surrounding tissue along the insertion in plantar fasciitis history shorter than 6 months[38]. Our study revealed increased thickness of the plantar fascia at 4th week after ESWT (Table 2).
Except plantar thickness by using ultrasonography, a similar concept in a previous study showed magnetic resonance imaging (MRI) was a desirable assessment for the increase of soft-tissue edema on acute response in that it could help a physician to control the effectiveness of the magnitude of ESWT energy[41].
Additionally, we did not attempt to measure thickness of the plantar fascia of the normal foot in these patients to reproduce the same results as previous studies. It was one of the limits of this study. Nonetheless, some aspects of comparison between ESWT and CSI remained elusive. Therefore, our study focused on the thickness change of plantar fascia before and after treatment, and clinical outcomes between ESWT and CSI in the short-time 3-month follow-up.
The systematic review of the Physiotherapy Evidence Database showed that there is no consensus in the literature about the difference between low- and high-energy ESWT devices. Generally, the safety and efficacy of ESWT is clearly supported by the cumulative data[39]. The ethnic differences of body mass index (BMI) distribution were presented within a lower and narrower BMI range for Chinese compared to Blacks and Whites, who have a higher mean BMI[40]. Therefore, we use the medium energy ESWT (1500 pulses for two sections) for chronic plantar fasciitis to avoid osteonecrosis of foot. That was consistent within a previous review study[39].
This study had other limitations. First, in the 130 cases study, twenty cases didn’t fulfill study criteria due to selection and blindness. Furthermore, there were 8 cases in ESWT and 5 cases in CSI dropped out this study. The data may be different if all the patients finish this study. Large sample size study is required to confirm this result. Second, we performed median energy ESWT (0.29 mJ/mm2) 1500 shocks for 2 sections. Could different treatment protocols or shock wave energy produce the same results remains unclear. Third, we stop assessment at 3 months not 12 months due to the limited budgets and staffs to connect with 97 plantar fasciitis patients. Therefore, we can’t compare our results with other long-term studies. We didn’t restrict patients’ activity level over 3 months due to impracticable situation in some high activity demand patients (farmers, constructors). During the 3-months study, all the patients were advised to prevent level I and II exercise or long distance walk (over 5 kilometers).
Another defect of this study is the long-term effects of ESWT and CSI. We didn’t follow these patients long enough to evaluate the recurrence rate, the possible complications of osteonecrosis of calcaneus, or plantar fascia rupture. During this study period, some patients got post-ESWT and post-CSI heel pain. Most patients’ symptoms relieved after oral acetaminophen. Further long-term follow studies are mandatory.
Conclusion
Our study revealed that ESWT is more efficacious than CSI in the treatment of plantar fasciitis in the 12-weeks assessment of VAS and 100-point score. The plantar fascia thickness increased from the baseline to 4th week after treatment, then decreased gradually, but not to the baseline. Under ESWT, the increase of plantar fascia thickness at 4th week was positively correlated with the VAS score at 12th week. It implied more change in plantar fascia at early stage after ESWT, more effective of the therapeutic effect. In CSI, no such correlation was noted.
Abbreviations:
- ESWT
Extracorporeal Shockwave Therapy
- CSI
Corticosteroid Injections
Acknowledgement
We would like to acknowledge the editorial service provide by the Research Assistantance Center, Show Chwan Health Care System.
Footnotes
The authors have no conflicto of interest.
Edited by: G. Lyritis
Ethics approval and consent to participate
Ethics approval was obtained from the Changhua Show Chwan Hospital, Taiwan. Written consent was provided by participants to be included in the study.
Authors’contributions
Authors’ Contributions Conception and design: Ta-Wei Lai. Development of methodology: Hsiao-Li. Acquisition of data: Meng-Shiunn Lee, Po-Ming Chen. Analysis and interpretation of data: Ming-Chou, Ku. Study supervision: Ta-Wei Lai.
Availability of data and materials
Data were collected from Changhua Show Chwan Hospital, Taiwan. Informed consents were obtained from all patients in accordance with the Declaration of Helsinki. This study was approved by the ethics committee of the Institutional Review Board (IRB) of Changhua Show Chwan Hospital.
References
- 1.Aldridge T. Diagnosing heel pain in adults. Am Fam Physician. 2004;70(2):332–338. [PubMed] [Google Scholar]
- 2.Buchbinder R, Ptasznik R, Gordon J, et al. Ultrasound-guided extracorporeal shock wave therapy for plantar fasciitis:a randomized controlled trial. JAMA. 2002;288(11):1364–1372. doi: 10.1001/jama.288.11.1364. [DOI] [PubMed] [Google Scholar]
- 3.May TJ, Judy TA, Conti M, et al. Current treatment of plantar fasciitis. Curr Sports Med Rep. 2002;1(5):278–284. doi: 10.1249/00149619-200210000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Ogden JA. Extracorporeal shock wave therapy for plantar fasciitis:randomised controlled multicentre trial. Br J Sports Med. 2004;38(4):382. doi: 10.1136/bjsm.2004.011601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Speed CA, Nichols D, Wies J, et al. Extracorporeal shock wave therapy for plantar fasciitis. A double blind randomised controlled trial. J Orthop Res. 2003;21(5):937–940. doi: 10.1016/S0736-0266(03)00048-2. [DOI] [PubMed] [Google Scholar]
- 6.Theodore GH, Buch M, Amendola A, et al. Extracorporeal shock wave therapy for the treatment of plantar fasciitis. Foot Ankle Int. 2004;25(5):290–297. doi: 10.1177/107110070402500503. [DOI] [PubMed] [Google Scholar]
- 7.Wang CJ. An overview of shock wave therapy in musculoskeletal disorders. Chang Gung Med J. 2003;26(4):220–232. [PubMed] [Google Scholar]
- 8.Williams SK, Brage M. Heel pain-plantar fasciitis and Achilles enthesopathy. Clin Sports Med. 2004;23(1):123–144. doi: 10.1016/S0278-5919(03)00094-2. [DOI] [PubMed] [Google Scholar]
- 9.Wang CJ, Chen HS, Huang TW. Shockwave therapy for patients with plantar fasciitis:a one-year follow-up study. Foot Ankle Int. 2002;23(3):204–207. doi: 10.1177/107110070202300303. [DOI] [PubMed] [Google Scholar]
- 10.Conflitti JM, Tarquinio TA. Operative outcome of partial plantar fasciectomy and neurolysis to the nerve of the abductor digiti minimi muscle for recalcitrant plantar fasciitis. Foot Ankle Int. 2004;25(7):482–487. doi: 10.1177/107110070402500707. [DOI] [PubMed] [Google Scholar]
- 11.Hammer DS, Adam F, Kreutz A, et al. Extracorporeal shock wave therapy (ESWT) in patients with chronic proximal plantar fasciitis:a 2-year follow-up. Foot Ankle Int. 2003;24(11):823–828. doi: 10.1177/107110070302401103. [DOI] [PubMed] [Google Scholar]
- 12.Hammer DS, Adam F, Kreutz A, et al. Ultrasonographic evaluation at 6-month follow-up of plantar fasciitis after extracorporeal shock wave therapy. Arch Orthop Trauma Surg. 2005;125(1):6–9. doi: 10.1007/s00402-003-0591-z. [DOI] [PubMed] [Google Scholar]
- 13.Speed CA, Richards C, Nichols D, et al. Extracorporeal shock-wave therapy for tendonitis of the rotator cuff. A double-blind, randomised, controlled trial. J Bone Joint Surg Br. 2002;84(4):509–512. doi: 10.1302/0301-620x.84b4.12318. [DOI] [PubMed] [Google Scholar]
- 14.Speed CA. Extracorporeal shock-wave therapy in the management of chronic soft-tissue conditions. J Bone Joint Surg Br. 2004;86(2):165–171. doi: 10.1302/0301-620x.86b2.14253. [DOI] [PubMed] [Google Scholar]
- 15.Orhan Z, Cam K, Alper M, Ozturan K. The effects of extracorporeal shock waves on the rat Achilles tendon:is there a critical dose for tissue injury? Arch Orthop Trauma Surg. 2004;124(9):631–635. doi: 10.1007/s00402-003-0598-5. [DOI] [PubMed] [Google Scholar]
- 16.Rompe JD, Kirkpatrick CJ, Küllmer K, et al. Dose-related effects of shock waves on rabbit tendo Achillis. A sonographic and histological study. J Bone Joint Surg Br. 1998;80(3):546–552. doi: 10.1302/0301-620x.80b3.8434. [DOI] [PubMed] [Google Scholar]
- 17.Durst HB, Blatter G, Kuster MS. Osteonecrosis of the humeral head after extracorporeal shock-wave lithotripsy. J Bone Joint Surg Br. 2002;84(5):744–746. doi: 10.1302/0301-620x.84b5.12282. [DOI] [PubMed] [Google Scholar]
- 18.Ikeda K, Tomita K, Takayama K. Application of extracorporeal shock wave on bone:preliminary report. J Trauma. 1999;47(5):946–950. doi: 10.1097/00005373-199911000-00024. [DOI] [PubMed] [Google Scholar]
- 19.Maier M, Milz S, Tischer T, et al. Influence of extracorporeal shock-wave application on normal bone in an animal model in vivo. Scintigraphy, MRI and histopathology. J Bone Joint Surg Br. 2002;84(4):592–599. doi: 10.1302/0301-620x.84b4.11621. [DOI] [PubMed] [Google Scholar]
- 20.Maier M, Steinborn M, Schmitz C, et al. Extracorporeal shock wave application for chronic plantar fasciitis associated with heel spurs:prediction of outcome by magnetic resonance imaging. J Rheumatol. 2000;27(10):2455–2462. [PubMed] [Google Scholar]
- 21.Haake M, Buch M, Schoellner C, et al. Extracorporeal shock wave therapy for plantar fasciitis:randomised controlled multicentre trial. BMJ. 2003;327(7406):75. doi: 10.1136/bmj.327.7406.75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lee GP, Ogden JA, Cross GL. Effect of extracorporeal shock waves on calcaneal bone spurs. Foot Ankle Int. 2003;24(12):927–930.24. doi: 10.1177/107110070302401210. [DOI] [PubMed] [Google Scholar]
- 23.Brinks A, Koes BW, Volkers AC, et al. Adverse effects of extra-articular corticosteroid injections:a systematic review. BMC Musculoskelet Disord. 2010;11:206. doi: 10.1186/1471-2474-11-206. doi:10.1186/1471-2474-11-206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ogden J, Alvarez RG. Plantar fasciopathy and orthotripsy:the effect of prior cortisone injection. Foot Ankle Int. 2005;26(3):231–233. doi: 10.1177/107110070502600308. [DOI] [PubMed] [Google Scholar]
- 25.Porter MD, Shadbolt B. Intralesional corticosteroid injection versus extracorporeal shock wave therapy for plantar fasciopathy. Clin J Sport Med. 2005;15(3):119–124. doi: 10.1097/01.jsm.0000164039.91787.dc. [DOI] [PubMed] [Google Scholar]
- 26.Nayera Saber, Hosam Diab, Wael Nassar, et al. Ultrasound guided local steroid injection versus extracorporeal shockwave therapy in the treatment of plantar fasciitis. Alexandria Journal of Medicine. 2012;46(1):35–46. [Google Scholar]
- 27.BScheuer R, Friedrich M, Hahne J, et al. Approaches to optimize focused extracorporeal shockwave therapy (ESWT) based on an observational study of 363 feet with recalcitrant plantar fasciitis. Int J Surg. 2016;27:1–7. doi: 10.1016/j.ijsu.2016.01.042. doi:10.1016/j.ijsu.2016.01.042. [DOI] [PubMed] [Google Scholar]
- 28.Karls SL, Snyder KR, Neibert PJ. Effectiveness of Corticosteroid Injections on the Treatment of Plantar Fasciitis. J Sport Rehabil. 2015 doi: 10.1123/jsr.2014-0234. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 29.Maki M, Ikoma K, Imai K, et al. Correlation between the outcome of extracorporeal shockwave therapy and pretreatment MRI findings for chronic plantar fasciitis. Mod Rheumatol. 2015;25(3):427–430. doi: 10.3109/14397595.2014.978526. [DOI] [PubMed] [Google Scholar]
- 30.Mardani-Kivi M, Karimi Mobarakeh M. Treatment Outcomes of Corticosteroid Injection and Extracorporeal Shock Wave Therapy as Two Primary Therapeutic Methods for Acute Plantar Fasciitis:A Prospective Randomized Clinical Trial. J Foot Ankle Surg. 2015;54(6):1047–1052. doi: 10.1053/j.jfas.2015.04.026. [DOI] [PubMed] [Google Scholar]
- 31.Wang FS, Yang KD, Chen RF, et al. Extracorporeal shock wave promotes growth and differentiation of bone-marrow stromal cells towards osteoprogenitors associated with induction of TGF-beta1. J Bone Joint Surg Br. 2002;84(3):457–461. doi: 10.1302/0301-620x.84b3.11609. [DOI] [PubMed] [Google Scholar]
- 32.Costa M, Donell S. Low-energy extracorporeal shock-wave treatment (ESWT) for tendinitis of the supraspinatus. J Bone Joint Surg Br. 2002;84(4):619–620. [PubMed] [Google Scholar]
- 33.Riddle DL, Pulisic M, Sparrow K. Impact of demographic and impairment-related variables on disability associated with plantar fasciitis. Foot Ankle Int. 2004;25(5):311–317. doi: 10.1177/107110070402500506. [DOI] [PubMed] [Google Scholar]
- 34.Rompe JD, Hope C, Küllmer K, et al. Analgesic effect of extracorporeal shock-wave therapy on chronic tennis elbow. J Bone Joint Surg Br. 1996;78(2):233–237. [PubMed] [Google Scholar]
- 35.Rompe JD, Schoellner C, Nafe B. Evaluation of low-energy extracorporeal shock-wave application for treatment of chronic plantar fasciitis. J Bone Joint Surg Am. 2002;84-A(3):335–341. doi: 10.2106/00004623-200203000-00001. [DOI] [PubMed] [Google Scholar]
- 36.Alvarez RG, Ogden JA, Jaakkola J, et al. Symptom duration of plantar fasciitis and the effectiveness of Orthotripsy. Foot Ankle Int. 2003;24(12):916–921. doi: 10.1177/107110070302401208. [DOI] [PubMed] [Google Scholar]
- 37.Akfirat M, Sen C, Günes T. Ultrasonographic appearance of the plantar fasciitis. Clin Imaging. 2003;27(5):353–7. doi: 10.1016/s0899-7071(02)00591-0. [DOI] [PubMed] [Google Scholar]
- 38.Maki M, Ikoma K, Imai K, et al. Correlation between the outcome of extracorporeal shockwave therapy and pretreatment MRI findings for chronic plantar fasciitis. Mod Rheumatol. 2015;25(3):427–430. doi: 10.3109/14397595.2014.978526. [DOI] [PubMed] [Google Scholar]
- 39.Schmitz C, Császár NB, Milz S, et al. Efficacy and safety of extracorporeal shock wave therapy for orthopedic conditions:a systematic review on studies listed in the PEDro database. Br Med Bull. 2015;116:115–38. doi: 10.1093/bmb/ldv047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Katz EG, Stevens J, Truesdale KP, et al. Associations of body mass index with incident hypertension in American white, American black and Chinese Asian adults in early and middle adulthood:the Coronary Artery Risk Development in Young Adults (CARDIA) study, the Atherosclerosis Risk in Communities (ARIC) study and the People's Republic of China (PRC) study. Asia Pac J Clin Nutr. 2013;22(4):626–34. doi: 10.6133/apjcn.2013.22.4.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Zhu F, Johnson JE, Hirose CB, et al. Chronic plantar fasciitis:acute changes in the heel after extracorporeal high-energy shock wave therapy - observations at MR imaging. Radiology. 2005;234(1):206–10. doi: 10.1148/radiol.2341031653. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data were collected from Changhua Show Chwan Hospital, Taiwan. Informed consents were obtained from all patients in accordance with the Declaration of Helsinki. This study was approved by the ethics committee of the Institutional Review Board (IRB) of Changhua Show Chwan Hospital.