

Abstract
Background:
Labor pain is the most severe pain women would experience, which could lead to loss of emotional control that plays a key role in creating a traumatic delivery experience and psychological disorders. The goal of this study was to evaluate the effect of acupressure on anxiety level and sedative and analgesics consumption in women during labor.
Materials and Methods:
This study was a randomized, single-blind clinical trial performed at Maryam Hospital in Tehran, Iran. One hundred and thirty-one pregnant women in Labor Ward were selected by convenience sampling. Subjects were randomly allocated to three groups, namely experimental group (pressure group), control group 1(touh group) and, control group 2 (routine care group). The study data were gathered using demographic information form, and assessed with Faces Anxiety Scale (FAS). For participants belonging to the experimental group, pressure was applied to the Spleen 6 acupoint for 30 min, and for those with only light touch was applied to the Spleen 6 acupoint for 30 min. The collected data were analyzed using Statistical Package for the Social Sciences 16 and descriptive statistics.
Results:
There was a significant difference between the three groups in terms of the mean of anxiety after 30 min of starting the intervention and 30 min after termination of the intervention; the anxiety of the experimental group was significantly decreased (p = 0.03). Sedative and analgesics consumption was significantly lower in the experimental group compared to the other groups (p = 0.006).
Conclusions:
This study showed that compression of the Spleen 6 acupoint was an effective complementary method to decrease maternal anxiety and analgesic consumption, especially pethidine.
Keywords: Acupressure, analgesic consumption, anxiety, Iran, Spleen 6 acupoint
Introduction
Birth is one of the most important events in mother's life and is a physiological process.[1] Labor pain is the most severe pain that women would experience,[2] which could lead to loss of emotional control that plays a key role in creating a traumatic delivery experience [3] and psychological disorders.[4] Labor pain and fear may also increase cesarean section.[5] These consequences necessitate the application of methods that could decrease pain. Today, various medical and nonmedical methods are used to reduce labor pain.[6] There are considerable advantages to the use of nonmedical pain management techniques, such as few side effects for mother and fetus and lack of interference with labor process.[7,8] Acupressure, as a noninvasive method, eliminates imbalance in vital energy, removes pain, reduces muscle tension, improves blood circulation and vital activities, and decreases the anxiety symptoms [9] and is one of the popular complementary therapies which is believed to improve psychological and general health.[10] Manual stimulation of acupuncture points has been shown to increase the production of serotonin and endorphin as well as improve the regulation of serum cortisol. Changes in these hormones may reduce anxiety.[11] One study indicated that acupressure at specific points could reduce preoperative anxiety.[12] A clinical trial to evaluate the effect of pressure on Bladder 32 (BL32) acupoint on women's anxiety during labor showed that acupressure at the BL32 point reduced the mother's anxiety.[13] In another study, the results showed increased level of anxiety in both groups but the amount of increase was lower in the pressure group than the touching group and the difference was significant.[14] In another study there was no significant difference in drug consumption between pressure and touching groups.[15] Furthermore, Suzuki and Tobe performed a study on pregnant woman and revealed the effectiveness of acupressure in reduction of pregnancy-related anxiety and previous depression.[16] The reduction of anxiety might be due to the effectiveness of the intervention, self-hypnosis, or even the feeling of security resulting from the presence of the researcher as one of the healthcare staff.[17] Given that, good evidence on the effectiveness of acupressure on psycho-social aspects of health is limited.[18] Only few studies about the effect of acupressure on anxiety and analgesic consumption during labor have been done on three groups. As a result, more studies are needed to establish safe and effective pain-relieving strategies to increase the comfort levels of pregnant women during labor, as labor pain is one of the most difficult experiences in a woman's life. Thus, the goal of this study was to evaluate the effect of acupressure on anxiety level and sedative and analgesics consumption in three groups of women during labor in Iran.
Materials and Methods
A randomized, controlled, single-blind clinical trial was conducted at Maryam Hospital, Tehran, Iran, registered in the Iranian Registry of Clinical Trials (ID: IRCT138812193527N1) and designed as a single-blind clinical trial with random allocation of population that consisted of 18–35-year-old women who had been referred to the Labor Ward for delivery. Sampling, as available, was done among all pregnant women who were admitted to the Labor Ward. The inclusion criteria were having singleton pregnancy, being mother's first or second delivery, term pregnancy, vaginal delivery, a cervical dilatation of 3–5 cm, and having a normal pattern of contractions repeated every 5 min or less for 20 s or more. Patients were excluded if they have any sign of fetal distress, use psychotherapeutics, or presence of any medical or obstetrical problems.
To confirm the accuracy of the acupoint location, Acuhealth TENS Pro 900 (Acuhealth Pty, Stepney, South Australia) was used. This device produces a different sound at acupoints because they have a lower electric resistance than their surrounding area. Once the point was located, the intervention was performed according to the study conducted by Lee et al.[14] using simple sample equation, with power of 80% and standard deviation of 1.0. Based on a similar study by Lee et al.,[15] at least 41 participants were needed in each group. Initially, 172 participants were randomly selected. Due to limitations in space in the labor room, if the sampling of different groups was performed on the same day, the subjects would become aware of the used method, and thus, the placebo effect would be lost. Therefore, the randomization was performed in terms of time (fortnightly), at the beginning of each two-week period, and one of the groups was selected randomly. Based on the exclusion criteria, 41 patients were excluded during or after the study; 21, 5, and 15 individuals were excluded from the pressure, touch, and conventional care groups, respectively. Ultimately, 131 participants, consisting of 41 subjects in the experimental group (pressure group), 41 in the control group 1 (touch group), and 49 in the control group 2 (routine care group), were studied. The process of the participants' allocation is shown in Figure 1. The control group 1, with the application of touch at Spleen 6 acupoint (SP6), was designed to eliminate the stress factor (the researcher's presence). Initially, the SP6 was examined to rule out any burns, eczema, and excessive edema. Subsequently, vital signs, color of tongue, uterine contractions, and vaginal examination were noted.
Figure 1.

The process of the study
During the 30-min intervention, pressure group and touch group, respectively, received pressure and light touch at SP6 on both legs simultaneously accompanied with instructions on deep breathing and relaxation. In the experimental group, pressure was applied through the rotational motion of the hand (the energy distributing method) at SP6 as follows. Pressure was applied for 2 min in a way that a pleasant feeling of pain would be experienced by the subject. The applied pressure was to an extent kept the degree of paleness of the nail at a constant level and that the subject was pleased. Subsequently, regardless of contractions, 1 min of pressure followed by 1 min of rest was applied intermittently until the pressure time equaled an overall 30 min. It took 1 h to perform this technique every time. The same technique was applied in the touch group with the application of touch instead of pressure at SP6. Given the approximate average of 24 min needed for the meridian energy-flow cycle in the body, a pressure time of 30 min was determined to guarantee a complete circulation in the body.[14] Furthermore, as the minimum pressure time was 1 min, pressure was initially applied for 2 min to guarantee that a complete cycle of pressure time was covered at every attempt. All subjects in both pressure and touch groups were in a left lateral position to prevent a sudden fall in blood pressure. To control the bias effect of analgesics, no analgesics were used before or during the intervention and the amount of sedative and analgesics consumption during labor was measured. The level of anxiety, according to a study conducted by Lee et al., was measured using the Faces Anxiety Scale (FAS) before and after 30 min of cessation of the intervention.[19] The evaluation time of anxiety in the routine care group was also considered in order to match the other groups on admission, 1 h, and 1.5 h from the beginning of sampling. The type of delivery, newborn weight, and Apgar score were recorded in the questionnaire.
The collected data were analyzed using Statistical Package for the Social Sciences version 16 and descriptive statistics. The Chi-square and Fisher's exact tests were used for the analysis of the categorical variables, and Kruskal–Wallis test was used for the following continuous variables: anxiety, age, dilatation, and effacement between the groups. p values below 0.05 were considered significant.
Ethical considerations
After explaining the study objectives to participants, informed consents were obtained from participants who were eligible and agreed with the study procedures.
Results
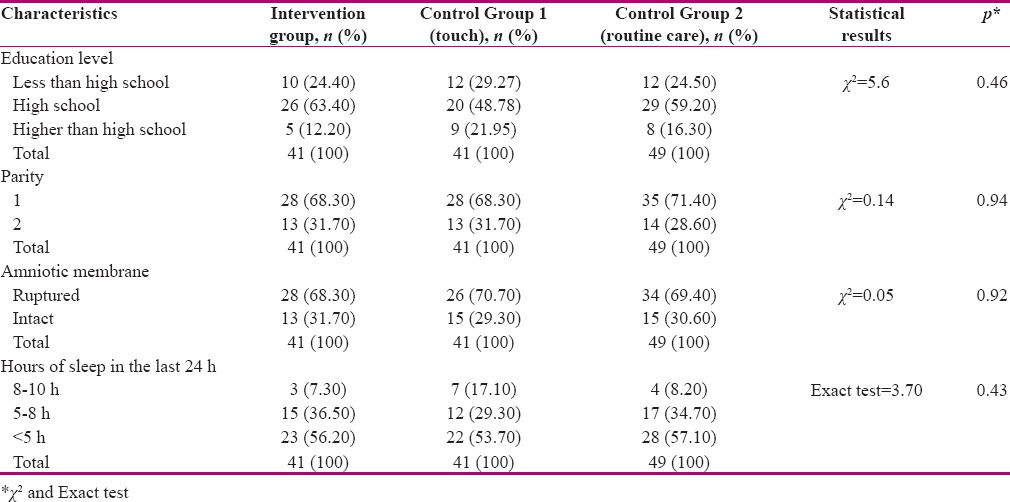
The exclusion criteria were any sign of fetal distress, the use of psychotherapeutic drugs, medications for labor induction, and the presence of any medical or obstetrical complications. Lastly, data collected from 131 patients were included for the data analysis. Before the intervention, no statistically significant differences were reported between the groups in terms of demographic and obstetrics characteristics (p > 0.05). The average age of the women in all three groups was 26 years that had no statistically significant difference between the three groups. Before the intervention, no statistically significant differences were observed between dilatation and effacement in three groups (p > 0.05). The demographic characteristics of the women were shown in Table 1.
Table 1.
Comparison of participants' characteristics according to study groups (n=131)
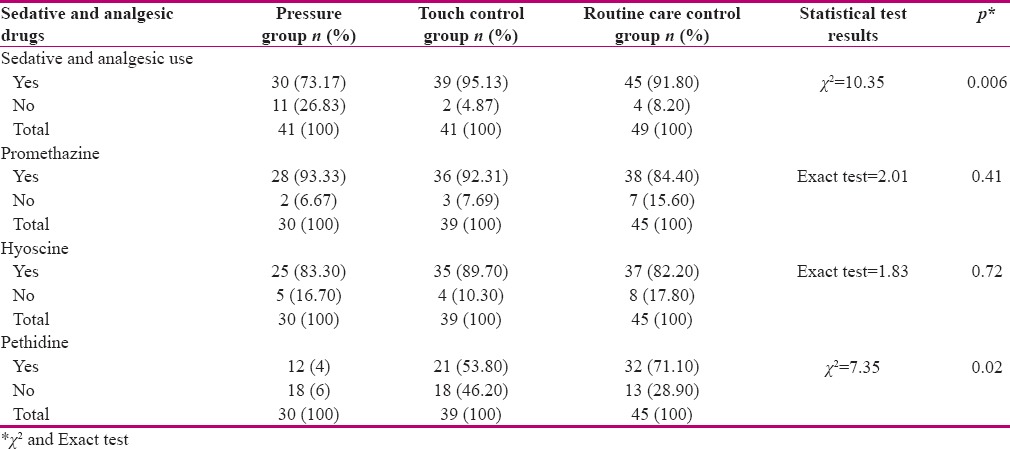
The comparison between the mean of maternal anxiety before the intervention and the mean of anxiety 30 min after the cessation of the intervention had a statistically significant difference. Statistically significant differences were reported between the mean of maternal anxiety before and after the 30 min cessation of the intervention between the groups [Table 2]. No statistically significant difference was found between pressure and touch groups in terms of level of anxiety. A statistically significant difference was reported in the use of analgesic between the groups [Table 3].
Table 2.
comparison of the maternal anxiety level before and 30 min after the termination of the intervention between study groups
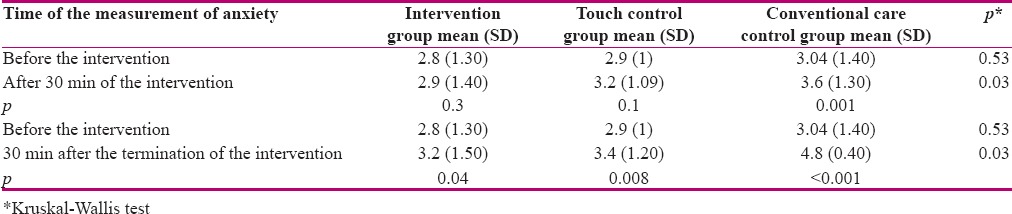
Table 3.
Comparison of use of sedative and analgesic drugs between study groups
Discussion
Anxiety in the pressure group was significantly decreased compared with the touch and routine care group. Also, the use of sedative and analgesics between the groups had a statistically significant difference. The lowest rate of sedative and analgesic use belonged to the pressure group. Accordingly, it was 73.2, 95.1, and 91.8% in the pressure, touch, and routine care group, respectively. A clinical trial evaluated the effect of pressure at BL32 on labor duration, and women's anxiety during labor.[13] It showed that anxiety in the pressure group significantly decreased during labor.[13] In two studies,[14,15] an increased level of anxiety in both groups was reported, but it was lower in the pressure group than the touch group, which was statistically significant. The findings of the present study were similar to those of other studies.[14,15] The results of a study on Gall Bladder 21 (GB-21) and SP6 acupoints showed that the anxiety level reduced in the two intervention groups, but it increased in the control group.[20] Thus, acupressure could reduce anxiety and improve the mood condition.[21] Moreover, another study showed that the stimulation of particular acupoints effectively reduced anxiety prior to the surgery.[12] It has been reported that acupressure could immediately relieve pretreatment anxiety among adults with a medium effect size.[22] Two other studies showed that acupressure led to the release of neurotransmitters such as serotonin, which had tranquil effects.[22,11] A systematic review and meta-analysis indicated a significant reduction in the use of morphine in intervention groups compared to control groups.[23] Acupressure is an alternative to acupuncture,[11] but it is less likely to cause adverse effects compared to needle acupuncture.[18] It has been demonstrated that acupressure could reduce the intensity of pain and use of morphine in patients who recovered from the lumbar spine surgery.[24] Furthermore, they reported that the application of acupressure in the perioperative period of total knee arthroplasty alleviated postoperative pain and decreased opioid consumption.[24] As the limitations of the present study, oxytocin administration was one of hospital routine that was performed on all three study groups in a similar style and timing. Also, no pain assessment tool was used to measure the effect of aupressure on pain level.
Converse to other studies, more matching and inclusion criteria were considered in the study's design. Also, identical pressure time for all women in the experimental group was applied. The use of a single-blind design, two control groups, measurement tools for pressure, and special tools to confirm the correct point of pressure were the strengths of this study. A few studies have been conducted to evaluate the effect of security feeling caused by the presence of the researcher as one of the healthcare staff. This study showed that acupressure, apart from the effect of the investigator, could reduce the anxiety level and the use of analgesics.
Conclusion
The results of this study showed that acupressure at SP6 could be considered as an alternative method that could decrease the maternal anxiety level and use of sedative and analgesics especially pethidine, which could reduce analgesic and surgical complications in pain management. Lastly, acupressure can be considered by healthcare staff as a method for reducing anxiety and the use of sedative and analgesics during labor.
Financial support and sponsorship
Tarbiat Modares University, Tehran, Iran.
Conflicts of interest
Nothing to declare.
Acknowledgement
This article was derived from a Master Thesis in Tarbiat Modares University, Tehran (Iran) (grant no: 150/75148).
References
- 1.Kashanian M, Shahali S. Effects of acupressure at the Sanyinjiao point (SP6) on the process of active phase of labor in nulliparas women. J Matern Fetal Neonatal Med. 2009:1–4. doi: 10.1080/14767050903277662. [DOI] [PubMed] [Google Scholar]
- 2.Smith CA, Collins CT, Crowther CA, Levett KM. Acupuncture or acupressure for pain management in labour. Cochrane Database Syst Rev. 2011;6:CD009232. doi: 10.1002/14651858.CD009232. [DOI] [PubMed] [Google Scholar]
- 3.Garthus Niegel S, Knoph C, Soest T, Nielsen CS, Eberhard Gran M. The Role of Labor Pain and Overall Birth Experience in the Development of Posttraumatic Stress Symptoms: A Longitudinal Cohort Study Birth. 2014;41:108–15. doi: 10.1111/birt.12093. [DOI] [PubMed] [Google Scholar]
- 4.okic-Begic N, Zigic L, Nakic Rados S. Anxiety and anxiety sensitivity as predictors of fear of childbirth: different patterns for nulliparous and parous women. J Psychosom Obstet Gynaecol. 2014;35:22–8. doi: 10.3109/0167482X.2013.866647. [DOI] [PubMed] [Google Scholar]
- 5.Azami-Aghdash S, Ghojazadeh M, Dehdilani N, Mohammadi M, Asl Amin Abad R. Prevalence and Causes of Cesarean Section in Iran: Systematic Review and Meta-Analysis. Iran J Public Health. 2014;43:545–55. [PMC free article] [PubMed] [Google Scholar]
- 6.Calik KY, Komurcu N. Effects of SP6 acupuncture point stimulation on labor pain and duration of labor. Iran Red Crescent Med J. 2014;16:e16461. doi: 10.5812/ircmj.16461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Simbar M. Complementary therapies for pregnancy and childbirth. Tehran: Community Oriented Healthy; 2009. p. 34. [Google Scholar]
- 8.Tournaire M, Theau-Yonneau A. Complementary and alternative approaches to pain relief during labor. Evid Based Complement Alternat Med. 2007;4:409–17. doi: 10.1093/ecam/nem012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kao CL, Chen CH, Lin WY, Chiao YC, Hsieh CL. Effect of auricular acupressure on peri- and early postmenopausal women with anxiety: A double-blinded, randomized, and controlled pilot study. Evid Based Complement Alternat Med. 2012;2012:567639. doi: 10.1155/2012/567639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kashefi F, Khajehei M, Ashraf AR, Jafari P. The efficacy of acupressure at the Sanyinjiao point in the improvement of women's general health. J Altern Complement Med. 2011;17:1141–7. doi: 10.1089/acm.2010.0589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Moffet HH. How might acupuncture work? A systematic review of physiologic rationales from clinical trials. BMC Complement Altern Med. 2006;7:6–25. doi: 10.1186/1472-6882-6-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Valiee S, Bassampour SS, Nasrabadi AN, Pouresmaeil Z, Mehran A. Effect of acupressure on preoperative anxiety: A clinical trial. J Perianesth Nurs. 2012;27:259–66. doi: 10.1016/j.jopan.2012.05.003. [DOI] [PubMed] [Google Scholar]
- 13.Akbarzadeh M, Masoudi Z, Zare N, Vaziri F. Comparison of the effects of doula supportive care and acupressure at the BL32 point on the mother's anxiety level and delivery outcome. Iran J Nurs Midwifery Res. 2015;20:239–46. [PMC free article] [PubMed] [Google Scholar]
- 14.Lee MK. Effects of San-Yin-Jiao (SP6) acupressure on labor pain, delivery time in women during labor. Taehan Kanho Hakhoe Chi. 2003;33:753–61. doi: 10.4040/jkan.2003.33.6.753. [DOI] [PubMed] [Google Scholar]
- 15.Lee MK, Chang SB, Kang DH. Effects of SP6 acupressure on labor pain and length of delivery time in women during labor. J Altern Complement Med. 2004;10:959–65. doi: 10.1089/acm.2004.10.959. [DOI] [PubMed] [Google Scholar]
- 16.Suzuki S, Tobe C. Effect of acupressure, acupuncture and moxibustion in women with pregnancy-related anxiety and previous depression: A preliminary study. J Clin Med Res. 2017;9:525–7. doi: 10.14740/jocmr3009w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lewith GT, Jonas WB, Walach H. Clinical research in complementary therapies E-Book: Principles, problems and solutions: Elsevier Health Sciences. 2010 [Google Scholar]
- 18.Robinson N, Lorenc A, Liao X. The evidence for Shiatsu: A systematic review of Shiatsu and acupressure. BMC Complement Altern Med. 2011;7:88. doi: 10.1186/1472-6882-11-88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lee Mk, Chang SB, Lee HS, Kim HS. Effects of Treatment with San-yin-jiao (SP6)Acupressure for Labor Women on Labor Pain, Length Time for Delivery and Anxiety-A Clinical Pilot Study. J Korean Women Health Nurs. 2002;8:348–58. [Google Scholar]
- 20.Moradi Z, Akbarzadeh M, Moradi P, Toosi M, Hadianfard MJ. The effect of acupressure at GB-21 and SP-6 acupoints on anxiety level and maternal-fetal attachment in primiparous women: A randomized controlled clinical trial. Nurs Midwifery Stud. 2014;3:e19948. doi: 10.17795/nmsjournal19948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Horiuchi S, Tsuda A, Honda Y, Kobayashi H, Naruse M, Tsuchiyagaito A. Mood changes by self-administered acupressure in Japanese college students: A randomized controlled trial. Glob J Health Sci. 2014;7:40–4. doi: 10.5539/gjhs.v7n4p40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Au DW, Tsang HW, Ling PP, Leung CH, Cheung WM, Ip P, Cheung W. Effects of acupressure on anxiety: A systematic review and meta-analysis. Acupunct Med. 2015;33:353–9. doi: 10.1136/acupmed-2014-010720. [DOI] [PubMed] [Google Scholar]
- 23.Liu XL, Tan JY, Molassiotis A, Suen LK, Shi Y. Acupuncture-point stimulation for postoperative pain control: A systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2015;2015:657809. doi: 10.1155/2015/657809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chung YC, Chien HC, Chen HH, Yeh ML. Acupoint stimulation to improve analgesic quality for lumbar spine surgical patients. Pain Manag Nurs. 2014;15:738–47. doi: 10.1016/j.pmn.2013.07.010. [DOI] [PubMed] [Google Scholar]