

Abstract
Background
In the last year of life, many older people rather avoid admissions to inpatient care facilities. We describe and compare such admissions in the last year of life of 5092 community-dwelling older people in 15 European countries (+Israel).
Methods
Proxy-respondents of the older people, who participated in the longitudinal SHARE study, reported on admissions to inpatient care facilities (hospital, nursing home or hospice) during the last year of their life. Multivariable regression analyses assessed associations between hospitalizations and personal/contextual characteristics.
Results
The proportion of people who had been admitted at least once to an inpatient care facility in the last year of life ranged from 54% (France) to 76% (Austria, Israel, Slovenia). Admissions mostly concerned hospitalizations. Multivariable analyses showed that especially Austrians, Israelis and Poles had higher chances of being hospitalized. Further, hospitalizations were more likely for those being ill for 6 months or more (OR:1.67, CI:1.39–2.01), and less likely for persons aged 80+ (OR:0.54, CI:0.39–0.74; compared with 48–65 years), females (OR:0.74, CI:0.63–0.89) and those dying of cardiovascular diseases (OR:0.66, CI:0.51–0.86; compared with those dying of cancer).
Conclusions
Although healthcare policies increasingly stress the importance that people reside at home as long as possible, admissions to inpatient care facilities in the last year of life are relatively common across all countries. Furthermore, we found a striking variation concerning the proportion of admissions across countries which cannot only be explained by patient needs. It suggests that such admissions are at least partly driven by system-level or cultural factors.
Introduction
Most people prefer to receive care and to die at home.1,2 However, many people are admitted to inpatient care facilities at the end of their life, such as a hospital, nursing home or hospice.3–7 A study conducted in Belgium, the Netherlands, Italy and Spain (2009–11) showed that transitions between care sites are rather common in the last 3 months of life, with 55% (the Netherlands) to 60% (Italy) of patients having been transferred at least once.6 Especially transitions to a hospital occurred rather frequently in the last phase of life in all studied countries (Belgium, the Netherlands, Italy and Spain).5
In line with these findings, several studies showed that the majority of people dies in a hospital.8–10 Pivodic et al.8 compared the place of death of people dying from diseases indicative of palliative care need in 14 countries and concluded that between 25% (the Netherlands) and 85% (South Korea) of people died in a hospital. In a study among older patients who died with cancer, a higher proportion of decedents (38–52%) died in acute care hospitals in Canada, Belgium, England, Germany and Norway than in the USA (22%) and the Netherlands (29%).11 Hospitalizations in the last 3 months of life have been found to be associated with male gender and residing at home rather than in a care home.5 Further, being aged less than 85 years, having an infection and the absence of a palliative treatment goal were associated with hospitalization in the last week of life.4
Hospitalizations do not always align with the wishes of patients at the end of their life1 and carry the risk of patients receiving poor quality of end-of-life care and of poor coordination or planning of follow-up care after discharge from the inpatient care facility.5,12–15 Currently, in many countries health policy is aiming at reducing hospitalizations at the end of life and encouraging end-of-life care in the community for as long as possible.16
Cross-country comparisons of admissions to inpatient care facilities in the last phase of life can help to identify similarities and differences concerning the frequencies and duration of admissions and its causes. Previous international comparative research on such admissions is mainly limited to place of death studies based on restricted and sometimes inaccurate or incomplete death certificate data.8–10 Further, most of these studies focused on the last 3 months of life and incorporated just a few countries.4–7 This is the first cross-national study to describe and compare admissions of community-dwelling older people to inpatient care facilities in 15 European countries (+Israel), focussing on the last year of their life. We will address the following research questions:
How often and how long do community-dwelling older people spend time in inpatient care facilities in the last year of life of and does this vary between the studied countries?
Which personal and contextual characteristics are associated with hospitalizations in the last year of life of community-dwelling older people and do these associations vary between the studied countries?
Methods
Study design and sample
We used data from the Survey of Health, Ageing and Retirement in Europe (SHARE). SHARE is an ongoing longitudinal study in which data are collected on health, socio-economic status and social and family networks of community-dwelling older people (aged 50 years or over) from a number of European countries and Israel. People are excluded if they are incarcerated, hospitalized or out of the country during the entire survey period, unable to speak the country’s language(s) or have moved to an unknown address. The first wave of data was collected in 2004; the fifth in 2013. The weighted average of household response rates in 2004 was 62% (38% in Switzerland and 74% in France). The corresponding participation rate was 39% (17% in Switzerland and 60% in Denmark). The weighted average of individual response rates in 2004 was 48% (33% in Switzerland and 69% in France). Analyses revealed only small differences in the patterns of survey participation by gender and age group.17 Survey continuation in wave 2 was higher among participants aged 59–74, those having a good health and those living in free standing homes.18 More information on SHARE can be found elsewhere.18–25
We used data from 16 countries: Austria, Belgium, the Czech Republic, Denmark, Estonia, France, Germany, Greece, Israel, Italy, the Netherlands, Poland, Spain, Sweden, Slovenia and Switzerland. If a SHARE participant died, interviewers conducted a structured end-of-life interview with a proxy-respondent (n = 5095). Proxy-respondents were mostly relatives, but also neighbours or friends.18 For 3 deceased people, 2 interviews were available of which one of them was excluded from the analyses. This leads to a final sample of 5092. A total of 716 interviews were held in wave 2,26 1137 in wave 3,27 1110 in wave 428 and 2129 in wave 5.29 The average time between the participant’s death and the interview varied between 14 (wave 3) and 18 months (wave 4) across waves. In wave 2, end-of-life interviews were conducted in somewhat more than 60% of the cases of deceased persons.18 In wave 3, the lowest participation rate for end-of-life interviews was 41% in Austria, followed by 51% in the Netherlands, 52% in Sweden, 56% in France, 64% in Germany, 65% in Denmark and Belgium (Dutch), 67% in Switzerland, 73% in Belgium (French), 75% in the Czech Republic, 82% in Italy, 85% in Poland and 86% in Spain and Greece.21 For wave 4 and 5, no information on the participation rates for end-of-life questionnaires is available.
Procedures and measurements
Data were collected in computer assisted personal- or telephone interviews conducted by professional interviewers. Proxy-respondents were asked to provide information on:
the number and the duration of admissions to inpatient care facilities in the last year of life of the deceased person;
whether or not the deceased had been admitted to a hospital, a nursing home and/or a hospice in the last year of life;
personal characteristics of the deceased, the following of which were selected for this study as they were found relevant for admissions to inpatients care facilities in previous research4,8–10,30: age, gender, education level (International Standard Classification of Education, ISCED-97),31 living alone, main cause of death, place of dying, duration of the illness before death, number of difficulties with activities in daily living (ADL) in the last year of life for at least 3 months, help with ADL during the last year of life and the overall time the deceased received help by relatives and/or professional helpers during the last 12 months (Supplementary table).
Analyses
We compared the characteristics of the deceased and the time spent in inpatient care facilities across countries using Pearson’s χ2 tests and ANOVA. Furthermore, we calculated percentages of hospitalizations for subgroups. To determine which personal characteristics were associated with hospitalizations in the last year of life we conducted a multivariable binary logistic regression analysis with the dependent variable being: hospitalized in the last year of life vs. not hospitalized. Independent variables were simultaneously entered. Analyses were conducted for each country separately and for the whole study population altogether (n = 5092). Moreover we performed a ‘test for interaction’ to study whether the odds ratios differed across countries. We did this for every characteristic separately by including all countries and adding an interaction term for country*characteristic. Finally we conducted a multivariable binary logistic regression analysis for all countries together, with country as an independent variable. All statistical tests were performed with a significance level of α < 0.05.
Ethics
Until July 2011, SHARE has been reviewed and approved by the Ethics Committee of the University of Mannheim. Since then, the Ethics Council of the Max-Planck-Society for the Advancement of Science (MPG) is responsible for ethical reviews and the approval of the study.
Results
Characteristics
The mean age at death (table 1) ranged from 74 years in Poland to 81 years in Sweden. Between 40% (the Netherlands, Poland) and 54% (Austria) of deceased people were female. Concerning the level of education we observed much variation between countries (25% in Germany and 94% in Spain had a low education). This also holds for the percentage of people who lived alone (14% in Poland and 50% in Denmark). In all countries, cancer (ranging between 23% in Estonia and Greece and 38% in the Netherlands) or cardiovascular diseases (ranging between 17% in Belgium, Denmark and the Netherlands and 35% in Greece) were the most common cause of death, as reported by the proxy. The percentage of people dying in the hospital ranged from 31% in the Netherlands up to 67% in Slovenia. In total 57% of people had been ill for 6 months or more before they died, 43% had had difficulties with more than 2 ADL in the last 12 months of life and 57% received assistance with ADL a full year before death.
Table 1.
Characteristics of the study population (n, %) (n = 5092)
| Characteristic | AT (n = 293) | BE (n = 377) | CH (n = 139) | CZ (n = 371) | DE (n = 193) | DK (n = 388) | EE (n = 329) | ES (n = 577) | FR (n = 405) | GR (n = 197) | IT (n = 386) | IL (n = 356) | NL (n = 272) | PL (n = 250) | SE (n = 507) | SI (n = 52) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age, mean (SD)a | 76 (11) | 78 (11) | 80 (12) | 76 (10) | 76 (10) | 78 (11) | 76 (10) | 80 (10) | 79 (12) | 79 (12) | 78 (10) | 77 (10) | 76 (11) | 74 (10) | 81 (10) | 77 (10) |
| 48–65 | 52 (19) | 61 (16) | 17 (12) | 75 (21) | 28 (15) | 57 (15) | 60 (18) | 57 (10) | 67 (17) | 27 (14) | 53 (14) | 50 (16) | 54 (20) | 51 (21) | 38 (8) | 7 (14) |
| 66–80 | 124 (44) | 128 (34) | 51 (37) | 144 (40) | 97 (51) | 151 (39) | 145 (45) | 216 (38) | 129 (33) | 76 (39) | 167 (44) | 132 (43) | 122 (45) | 125 (51) | 173 (35) | 26 (51) |
| 81–104 | 103 (37) | 185 (50) | 71 (51) | 143 (40) | 66 (35) | 177 (46) | 121 (37) | 293 (52) | 200 (51) | 90 (47) | 162 (42) | 127 (41) | 93 (35) | 71 (29) | 287 (58) | 18 (35) |
| Gender, femaleb | 157 (54) | 164 (44) | 57 (41) | 171 (46) | 89 (46) | 204 (53) | 145 (44) | 272 (47) | 195 (48) | 90 (46) | 168 (44) | 162 (46) | 109 (40) | 100 (40) | 237 (47) | 20 (39) |
| Educationb | ||||||||||||||||
| Low | 108 (38) | 217 (59) | 55 (42) | 228 (64) | 48 (25) | 148 (39) | 168 (51) | 523 (94) | 301 (76) | 160 (83) | 331 (87) | 172 (49) | 167 (63) | 160 (69) | 356 (72) | 28 (55) |
| Middle | 137 (48) | 81 (22) | 72 (55) | 102 (29) | 99 (52) | 144 (38) | 126 (38) | 16 (3) | 70 (18) | 20 (10) | 40 (11) | 116 (33) | 56 (21) | 61 (26) | 88 (18) | 20 (39) |
| High | 39 (14) | 73 (20) | 5 (4) | 28 (8) | 44 (23) | 87 (23) | 35 (11) | 18 (3) | 27 (7) | 12 (6) | 10 (3) | 62 (18) | 43 (16) | 11 (5) | 54 (11) | 3 (6) |
| Living aloneb | 116 (40) | 120 (32) | 59 (42) | 130 (35) | 61 (32) | 193 (50) | 83 (25) | 107 (19) | 148 (37) | 86 (44) | 61 (16) | 87 (25) | 74 (27) | 34 (14) | 215 (43) | 13 (25) |
| Cause deathb | ||||||||||||||||
| Cancer | 66 (24) | 115 (31) | 46 (33) | 90 (25) | 64 (34) | 117 (31) | 74 (23) | 135 (24) | 119 (31) | 45 (23) | 138 (36) | 98 (31) | 102 (38) | 65 (26) | 145 (29) | 17 (33) |
| Cardiovascular | 66 (24) | 63 (17) | 32 (23) | 104 (29) | 62 (33) | 65 (17) | 95 (30) | 150 (26) | 69 (18) | 68 (35) | 94 (25) | 56 (18) | 45 (17) | 84 (34) | 108 (22) | 13 (25) |
| Stroke | 40 (14) | 32 (9) | 7 (5) | 53 (15) | 12 (6) | 27 (7) | 59 (18) | 51 (9) | 44 (11) | 30 (16) | 42 (11) | 36 (12) | 19 (7) | 36 (15) | 38 (8) | 5 (10) |
| Respiratory | 7 (3) | 11 (3) | 4 (3) | 15 (4) | 4 (2) | 21 (6) | 13 (4) | 45 (8) | 22 (6) | 10 (5) | 21 (6) | 4 (1) | 5 (2) | 10 (4) | 14 (3) | 0 (0) |
| Infectious | 20 (7) | 22 (6) | 9 (7) | 16 (4) | 9 (5) | 22 (6) | 5 (2) | 23 (4) | 12 (3) | 1 (1) | 12 (3) | 11 (4) | 14 (5) | 4 (2) | 30 (6) | 3 (6) |
| Other | 79 (28) | 130 (35) | 41 (30) | 84 (23) | 40 (21) | 129 (34) | 75 (23) | 169 (30) | 121 (31) | 39 (20) | 76 (20) | 107 (34) | 84 (31) | 50 (20) | 164 (33) | 14 (27) |
| Place of dyingb | ||||||||||||||||
| Hospital | 139 (50) | 172 (47) | 58 (42) | 231 (64) | 90 (48) | 158 (42) | 155 (49) | 306 (54) | 210 (55) | 77 (43) | 169 (44) | 210 (62) | 83 (31) | 127 (52) | 191 (39) | 33 (67) |
| Home | 100 (36) | 118 (32) | 33 (24) | 85 (23) | 64 (34) | 98 (26) | 123 (39) | 220 (39) | 105 (28) | 96 (54) | 189 (50) | 104 (31) | 101 (38) | 108 (44) | 113 (23) | 14 (29) |
| Nursing home | 23 (8) | 59 (16) | 36 (26) | 21 (6) | 23 (12) | 107 (28) | 24 (8) | 31 (6) | 45 (12) | 2 (1) | 12 (3) | 22 (7) | 64 (24) | 1 (0) | 161 (33) | 2 (4) |
| Hospice | 6 (2) | 12 (3) | 6 (4) | 16 (4) | 5 (3) | 9 (2) | 4 (1) | 2 (0) | 8 (2) | 0 (0) | 2 (1) | 1 (0) | 12 (5) | 6 (2) | 22 (5) | 0 (0) |
| Other | 8 (3) | 7 (2) | 4 (3) | 10 (3) | 6 (3) | 8 (2) | 13 (4) | 8 (1) | 13 (3) | 3 (2) | 9 (2) | 1 (0) | 5 (2) | 4 (2) | 6 (1) | 0 (0) |
| Ill before deathb | ||||||||||||||||
| < 6 months | 110 (40) | 161 (45) | 78 (57) | 153 (42) | 73 (39) | 157 (42) | 133 (43) | 265 (47) | 158 (42) | 103 (59) | 169 (45) | 94 (29) | 127 (48) | 116 (47) | 202 (42) | 18 (36) |
| > 6 months | 162 (60) | 200 (55) | 59 (43) | 209 (58) | 115 (61) | 220 (58) | 179 (57) | 298 (53) | 218 (58) | 73 (42) | 210 (55) | 228 (71) | 138 (52) | 129 (53) | 281 (58) | 32 (64) |
| Difficulties ADLbc | ||||||||||||||||
| None | 138 (50) | 134 (36) | 67 (49) | 162 (45) | 82 (43) | 153 (40) | 149 (47) | 206 (36) | 156 (41) | 102 (53) | 128 (34) | 136 (41) | 110 (41) | 119 (48) | 187 (38) | 22 (42) |
| 1–2 | 35 (13) | 71 (19) | 37 (27) | 75 (21) | 24 (13) | 71 (19) | 49 (15) | 75 (13) | 47 (12) | 23 (12) | 49 (13) | 42 (13) | 46 (17) | 39 (16) | 105 (21) | 4 (8) |
| > 2 | 105 (38) | 169 (45) | 34 (25) | 121 (34) | 84 (44) | 159 (42) | 121 (38) | 293 (51) | 179 (47) | 68 (35) | 205 (54) | 155 (47) | 111 (42) | 91 (37) | 203 (41) | 26 (50) |
| Assistance ADLbc | ||||||||||||||||
| No | 14 (10) | 8 (3) | 8 (11) | 8 (4) | 5 (4) | 9 (4) | 14 (8) | 8 (2) | 6 (3) | 3 (3) | 13 (5) | 12 (6) | 7 (4) | 8 (5) | 28 (8) | 3 (10) |
| Yes, < 3 months | 11 (8) | 27 (11) | 4 (5) | 33 (16) | 11 (9) | 39 (16) | 15 (8) | 48 (13) | 25 (10) | 21 (19) | 36 (14) | 21 (10) | 33 (20) | 24 (16) | 34 (10) | 7 (24) |
| Yes, ≥ 3 months | 36 (25) | 59 (23) | 26 (35) | 65 (32) | 32 (27) | 59 (24) | 64 (34) | 95 (25) | 62 (26) | 34 (31) | 86 (33) | 49 (23) | 42 (26) | 32 (21) | 64 (19) | 6 (21) |
| Yes, a full year | 81 (57) | 162 (63) | 37 (49) | 99 (48) | 69 (59) | 144 (57) | 93 (50) | 230 (60) | 149 (62) | 52 (47) | 129 (49) | 130 (61) | 83 (50) | 88 (58) | 212 (63) | 13 (45) |
| Any hospital carebc | 196 (71) | 219 (59) | 76 (55) | 221 (61) | 127 (67) | 244 (64) | 181 (56) | 360 (63) | 201 (52) | 104 (54) | 253 (66) | 242 (73) | 158 (59) | 173 (70) | 301 (61) | 31 (61) |
| Any nursing home carebc | 35 (13) | 61 (16) | 34 (25) | 37 (10) | 29 (15) | 88 (23) | 30 (9) | 47 (8) | 67 (17) | 3 (2) | 19 (5) | 38 (12) | 42 (16) | 2 (1) | 110 (22) | 2 (4) |
| Any hospice carebc | 10 (4) | 45 (12) | 12 (9) | 31 (9) | 6 (3) | 14 (4) | 12 (4) | 8 (1) | 62 (16) | 0 (0) | 4 (1) | 8 (3) | 12 (5) | 8 (3) | 72 (15) | 1 (2) |
Missing data on age n = 125, gender n = 12, education n = 123, living alone n = 23, main cause of death n = 130, place of dying n = 74, how long been ill before death n = 135, difficulties with ADL n = 125, anyone helped with ADL n = 150, hospital care n = 122, nursing home care n = 116, hospice care n = 135. AT, Austria; BE, Belgium; CH, Switzerland; CZ, Czech Republic; DE, Germany; DK, Denmark; EE, Estonia; ES, Spain; FR, France; GR, Greece; IT, Italy; IL, Israel; NL, the Netherlands; PL, Poland; SE, Sweden; SI, Slovenia. P-value ≤ 0.05 based on
Anova or b: Chi-squared test on difference between countries.
In last 12 months.
Admissions in the last year of life
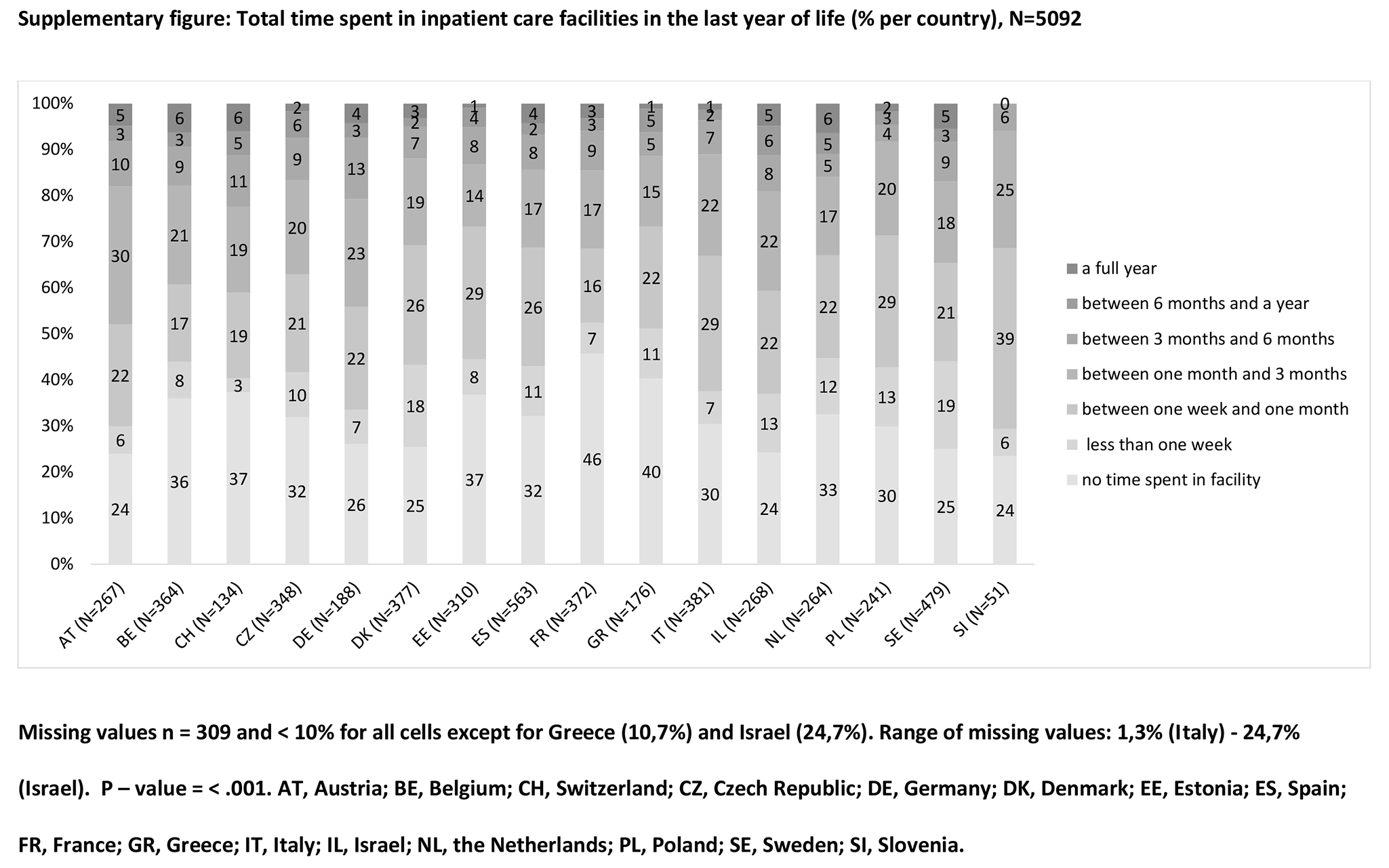
Between 52% (France) and 73% (Israel) of people had at least 1 hospital admission in the last year of life, between 1% (Poland) and 25% (Switzerland) had received any care in a nursing home and between 0% (Greece) and 16% (France) stayed in a hospice at least once (table 1). The proportion of people with any admission to an inpatient care facility in the last year of life ranged from 54% (France) to 76% (Austria, Israel, Slovenia) (Supplementary figure). Overall, 42% were admitted for 1 month or more (ranging from 27% in Estonia and Greece to 48% in Austria), with considerable variation in the total duration of admissions among the countries (P < 0.001).
Hospitalizations
Table 2 shows that, overall, the oldest age group was admitted less often to hospitals in the last year of life (58% for ≥ 81 years vs. 66% for 66–80 years and 62% for 48–65 years). In total 63% of males vs. 62% of females were hospitalized. Of people living alone, 60% were hospitalized vs. 63% of people living together. 78% of people who died from cancer were hospitalized in the last year of life, followed by 60% of those who died from a stroke. Furthermore, 73% of people who had been ill for 6 months or more were hospitalized vs. 50% for having been ill for less than 6 months. People with more than 2 ADL difficulties in the last year of life were admitted more often to hospital (70%) compared with people with 1 or 2 ADL difficulties (65%) or no difficulties (53%). People who received assistance with ADL for 3 months or more in the last year of life were hospitalized more often (78%) than people who received assistance for a full year (64%), assistance for less than 3 months (74%) or no assistance (56%). Finally, people who had received care in a nursing home were more often admitted to a hospital (82%) than people who did not receive nursing home care (59%). This also applies to people who stayed in a hospice (88% vs. 60% respectively).
Table 2.
Unadjusted hospitalization rates in the last year of life by country (n=5092)
| Characteristic | AT (n = 293) % | BE (n = 377) % | CH (n = 139) % | CZ (n = 371) % | DE (n = 193) % | DK (n = 388) % | EE (n = 329) % | ES (n = 577) % | FR (n = 405) % | GR (n = 197) % | IT (n = 386) % | IL (n = 356) % | NL (n = 272) % | PL (n = 250) % | SE (n = 507) % | SI (n = 52) % | Total (n = 5092) n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | |||||||||||||||||
| 48–65 | 65 | 62 | 65 | 49 | 64 | 82a | 57 | 65 | 54 | 26a | 72 | 55a | 76a | 67 | 66 | 86 | 465 (62) |
| 66–80 | 74 | 67a | 56 | 65 | 73 | 69 | 57 | 60 | 56 | 63a | 73a | 75 | 63 | 73 | 66 | 58 | 1312 (66)a |
| 81–104 | 70 | 53a | 52 | 64 | 58 | 55a | 55 | 64 | 50 | 54 | 57a | 72 | 45a | 63 | 57 | 56 | 1261 (58)a |
| Gender | |||||||||||||||||
| Male | 70 | 60 | 54 | 58 | 68 | 65 | 58 | 64 | 53 | 49 | 70 | 71 | 63 | 71 | 62 | 55 | 1676 (63) |
| Female | 71 | 58 | 56 | 65 | 65 | 64 | 55 | 62 | 52 | 60 | 61 | 76 | 53 | 67 | 59 | 70 | 1409 (62) |
| Education | |||||||||||||||||
| Low | 76 | 59 | 47 | 63 | 57 | 63 | 56 | 63 | 51 | 58a | 64 | 70 | 56 | 69 | 62 | 67 | 1898 (61) |
| Middle | 65 | 59 | 59 | 64 | 72 | 62 | 57 | 81 | 55 | 30a | 83 | 78 | 64 | 72 | 62 | 60 | 783 (64) |
| High | 73 | 60 | 60 | 46 | 67 | 70 | 57 | 50 | 63 | 36 | 70 | 73 | 63 | 55 | 53 | 33 | 331 (62) |
| Living alone | |||||||||||||||||
| No | 72 | 59 | 58 | 59 | 64 | 68 | 56 | 63 | 53 | 56 | 67 | 71 | 63a | 69 | 64 | 56 | 2164 (63)a |
| Yes | 68 | 57 | 51 | 67 | 72 | 60 | 57 | 60 | 50 | 52 | 60 | 82 | 49a | 74 | 57 | 75 | 908 (60)a |
| Cause death | |||||||||||||||||
| Cancer | 86a | 73a | 84a | 72 | 86a | 79a | 72a | 75a | 71a | 82a | 77a | 83a | 80a | 91a | 78a | 77 | 1112 (78)a |
| Cardiovascular | 59a | 49 | 22a | 57 | 55a | 59 | 51 | 59 | 39a | 34a | 60 | 59a | 38a | 60a | 48a | 69 | 608 (52)a |
| Stroke | 67a | 34a | 29 | 66 | 50 | 59 | 62 | 61 | 50 | 77a | 62 | 82 | 37a | 67 | 61 | 0a | 315 (60) |
| Other | 71 | 58 | 54 | 55 | 60 | 57a | 46a | 59 | 44a | 42a | 59 | 65 | 52 | 63 | 55a | 53 | 1008 (56)a |
| Ill before death | |||||||||||||||||
| < 6 months | 52a | 42a | 39a | 48a | 52a | 53a | 46a | 58a | 33a | 46a | 52a | 58a | 46a | 65 | 50a | 39a | 1039 (50)a |
| ≥ 6 months | 83a | 73a | 76a | 72a | 76a | 73a | 67a | 68a | 66a | 71a | 78a | 80a | 70a | 73 | 70a | 74a | 1979 (73)a |
| Difficulties ADL | |||||||||||||||||
| None | 60a | 47a | 39a | 48a | 60 | 63 | 44a | 55a | 40a | 39a | 58a | 61a | 53 | 64 | 57 | 46a | 1066 (53)a |
| 1–2 | 77 | 55 | 78a | 62 | 83 | 63 | 71a | 67 | 49 | 52 | 61 | 71 | 59 | 85a | 66 | 50 | 515 (65)a |
| > 2 | 81a | 70a | 62 | 77a | 68 | 66 | 66a | 67a | 64a | 77a | 72a | 82a | 65 | 70 | 62 | 76a | 1469 (70)a |
| Assistance ADL | |||||||||||||||||
| No | 79 | 50 | 63 | 71 | 40 | 44 | 50 | 63 | 50 | 33 | 31a | 67 | 43 | 75 | 54 | 100 | 86 (56)a |
| Yes, < 3 months | 91 | 78 | 50 | 70 | 82 | 77 | 67 | 63 | 68 | 76 | 75 | 81 | 70 | 83 | 77 | 100 | 288 (74)a |
| Yes, ≥ 3 months | 92 | 68 | 73 | 78 | 81 | 71 | 73 | 79a | 69 | 77 | 80a | 89 | 83a | 84 | 78a | 67 | 628 (78)a |
| Yes, a full year | 74 | 65 | 68 | 69 | 68 | 62 | 65 | 61a | 55 | 58 | 65 | 75 | 53a | 72 | 59a | 54 | 1122 (64)a |
| Any nursing home care | |||||||||||||||||
| No | 69 | 55a | 48a | 59a | 65 | 59a | 55 | 61a | 43a | 54 | 65 | 70a | 57 | 70 | 55a | 59 | 2252 (59)a |
| Yes | 80 | 82a | 77a | 83a | 76 | 83a | 68 | 83a | 93a | 67 | 84 | 91a | 71 | 50 | 81a | 100 | 516 (82)a |
| Any hospice care | |||||||||||||||||
| No | 69a | 55a | 51a | 60 | 65 | 64 | 55 | 62a | 43a | 54 | 66 | 72 | 58a | 69 | 56a | 60 | 2787 (60)a |
| Yes | 100a | 89a | 100a | 74 | 100 | 79 | 82 | 100a | 97a | 0 | 50 | 71 | 100a | 75 | 86a | 100 | 267 (88)a |
AT, Austria; BE, Belgium; CH, Switzerland; CZ, Czech Republic; DE, Germany; DK, Denmark; EE, Estonia; ES, Spain; FR, France; GR, Greece; IT, Italy; IL, Israel; NL, the Netherlands; PL, Poland; SE, Sweden; SI, Slovenia. Bold text indicate significant differences.
P ≤ 0.05 based on Chi-squared test; adjusted residuals are used to identify the categories responsible for a significant chi-square statistic.
Multivariable binary logistic regression analyses were performed for each country to assess the independent association between personal characteristics and hospitalizations (table 3). The analyses confirmed that hospitalizations were less likely for persons aged 80 or over (overall OR: 0.56, CI: 0.41–0.76) compared with persons aged 48–65 years. However, in Switzerland, France, Greece and Israel the reverse pattern was observed. Furthermore, females had lower chances of being hospitalized (overall OR: 0.77, CI: 0.65–0.91) except in France and Israel. Those dying of cardiovascular diseases (OR: 0.70, CI: 0.54–0.90) and ‘other’ diseases (OR: 0.55, CI: 0.44–0.69) also had lower chances of being hospitalized compared with those dying of cancer. Hospitalizations were more likely for those who had been ill for 6 months or more (OR: 1.70, CI: 1.42–2.05). People who received assistance with ADL for 3 months or more had higher chances of being hospitalized compared with people who received no assistance or assistance a full year (OR: 2.52, CI: 1.70–3.74 and OR: 1.77, CI: 1.43–2.19 respectively). Furthermore, hospitalizations were more likely for people who stayed in a nursing home (OR: 2.51, CI: 1.95–3.22) and for people who stayed in a hospice (OR: 2.24, CI: 1.48–3.41). We found an interaction between some characteristics (age, ill before death and difficulties with ADL) and country (P < 0.05). For instance, hospitalizations were especially common for Greece people aged 66–80 (OR: 4.55, CI: 1.45–14.31) or 80 or over (OR: 4.05, CI: 1.34–12.24) and Israeli people aged 80 or over (OR: 2.50, CI: 1.02–6.11).
Table 3.
Associations between personal characteristics and hospitalizations in the last year of life by country (adjusted odds ratios) (n = 5092)
| Characteristic | AT (n = 293) | BE (n = 377) | CH (n = 139) | CZ (n = 371) | DE (n = 193) | DK (n = 388) | EE (n = 329) | ES (n = 577) | FR (n = 405) | GR (n = 197) | IT (n = 386) | IL (n = 356) | NL (n = 272) | PL (n = 250) | SE (n = 507) | SI (n = 52)d | Total (n = 5092) | Test for interaction, P; (n = 5092)e |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.001 | |||||||||||||||||
| 48–65 | Ref | Ref | Ref | Ref | – | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| 66–80 | 3.20 | 0.54 | 0.46 | 1.31 | – | 0.52 | 0.89 | 0.88 | 1.10 | 8.38 | 0.58 | 6.61b | 0.46 | 0.06 | 0.72 | – | 0.95 | |
| 81–104 | 0.87 | 0.20b | 1.17 | 0.91 | – | 0.23a | 0.52 | 0.92 | 1.05 | 1.16 | 0.29 | 2.38 | 0.14b | 0.05 | 0.36 | – | 0.56c | |
| Gender | 0.50 | |||||||||||||||||
| Male | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| Female | 0.84 | 0.80 | 0.70 | 0.99 | 0.28 | 0.69 | 0.66 | 0.78 | 1.17 | 0.98 | 0.48a | 1.52 | 0.37a | 0.22b | 0.61 | – | 0.77b | |
| Education | 0.24 | |||||||||||||||||
| Low | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| Middle | 0.24a | 0.47 | 3.19 | 1.28 | 1.00 | 0.98 | 0.96 | 0.98 | 1.00 | 0.35 | 0.98 | 1.45 | 0.47 | 2.16 | 0.58 | – | 0.92 | |
| High | 1.65 | 0.50 | 3.52 | 0.55 | 4.05 | 0.88 | 1.33 | 0.64 | 0.36 | 1.55 | 1.10 | 1.35 | 1.25 | 0.15 | 0.49 | – | 0.89 | |
| Living alone | 0.17 | |||||||||||||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| Yes | 1.16 | 1.09 | 1.43 | 1.24 | 5.27a | 0.48 | 0.94 | 1.29 | 1.36 | 5.98a | 1.33 | 1.82 | 0.87 | 1.06 | 1.31 | – | 1.06 | |
| Cause death | 0.06 | |||||||||||||||||
| Cancer | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| Cardiovascular | 1.18 | 1.80 | 0.07a | 0.65 | 0.64 | 0.61 | 1.03 | 0.77 | 0.79 | 0.08a | 1.73 | 1.57 | 0.11b | 0.16a | 0.41a | – | 0.70b | |
| Stroke | 1.27 | 0.28 | 0.25 | 0.70 | 1.68 | 0.74 | 0.81 | 0.95 | 1.21 | 29.70 | 0.86 | 1.24 | 0.15a | 0.23 | 0.75 | – | 0.82 | |
| Other | 1.04 | 0.72 | 0.27 | 0.34a | 1.02 | 0.54 | 0.40 | 0.80 | 0.88 | 0.09a | 0.84 | 0.62 | 0.18b | 0.09b | 0.59 | – | 0.55c | |
| Ill before death | 0.02 | |||||||||||||||||
| < 6 months | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| ≥ 6 months | 2.40 | 1.90 | 3.61 | 1.17 | 3.31 | 1.15 | 1.32 | 1.38 | 3.21b | 6.03a | 2.73b | 1.45 | 0.48 | 0.83 | 2.19b | – | 1.70c | |
| Difficulties ADL | 0.002 | |||||||||||||||||
| None | – | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| 1–2 | – | 0.66 | 35.31a | 1.08 | 0.13 | 0.49 | 1.68 | 1.32 | 0.69 | 1.53 | 1.12 | 1.58 | 0.74 | 0.68 | 0.71 | – | 0.92 | |
| > 2 | – | 0.68 | 9.70 | 2.50 | 0.12 | 0.41 | 1.27 | 1.34 | 0.75 | 3.76 | 1.70 | 6.25a | 1.21 | 0.25 | 0.48 | – | 0.97 | |
| Assistance ADL | 0.99 | |||||||||||||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| Yes, < 3 months | 1.73 | 5.31 | 0.22 | 1.62 | 2.01 | 3.81 | 1.61 | 1.43 | 1.78 | >100b | 6.91a | 6.24 | 1.75 | 9.30 | 2.34 | – | 2.32c | |
| Yes, ≥ 3 months | 2.44 | 2.23 | 1.46 | 2.36 | 12.42 | 5.12 | 2.06 | 2.90 | 1.64 | 24.44 | 6.42a | 6.97a | 7.66 | 10.61 | 2.63 | – | 2.52c | |
| Yes, a full year | 0.45 | 2.33 | 1.43 | 1.44 | 2.03 | 4.44 | 2.03 | 1.09 | 0.94 | 26.13 | 2.78 | 1.77 | 2.86 | 10.90 | 1.39 | – | 1.42 | |
| Any nursing home care | 0.11 | |||||||||||||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| Yes | 1.16 | 5.26b | 1.88 | 1.67 | 3.05 | 6.37c | 1.16 | 2.32 | 9.94c | 0.003a | 2.75 | 1.77 | 2.85a | 0.10 | 2.26a | – | 2.51c | |
| Any hospice care | 0.054 | |||||||||||||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref | – | Ref | Ref | Ref | Ref | Ref | – | Ref | |
| Yes | >100 | 2.96a | >100 | 0.45 | >100 | 0.39 | 1.83 | >100 | 42.00b | – | 0.39 | 0.20 | >100 | 10.41 | 4.16b | 2.24c |
AT, Austria; BE, Belgium; CH, Switzerland; CZ, Czech Republic; DE, Germany; DK, Denmark; EE, Estonia; ES, Spain; FR, France; GR, Greece; IT, Italy; IL, Israel; NL, the Netherlands; PL, Poland; SE, Sweden; SI, Slovenia. Bold text indicate significant differences.
P ≤ 0.05.
P < 0.01.
P < 0.001.
Analysis for Slovenia not possible due to a low number of included participants.
We performed a ‘test for interaction’ to study whether the odds ratios differed significantly across countries. We did this for every characteristic separately by including all the countries and adding an interaction term for country*characteristic.
Finally, we performed a multivariable binary logistic regression analysis for all countries together to assess whether there is an association between country of residence and hospitalization while taking into account personal characteristics (age, gender, education, living alone, main cause of death, duration of illness, difficulties with ADL, assistance with ADL, nursing home care and hospice stays, table 4). People from France (reference) and the Netherlands (OR: 1.12, CI: 0.72–1.77) had the lowest probability of being hospitalized. People from Slovenia (OR: 2.31, CI: 0.93–5.73), Poland (OR: 2.61, CI: 1.59–4.30), Israel (OR: 2.65, CI: 1.65–4.26) and Austria (OR: 3.46, CI: 2.03–5.90) had the highest probability of being hospitalized.
Table 4.
Associations between personal characteristics and hospitalizations in the last year of life (adjusted odds ratios) (n=5092)
| Characteristic | Total population (n =5092) OR (CI) |
|---|---|
| Age | |
| 48-65 | Ref |
| 66-80 | 0.90 (0.66–1.24) |
| 81-104 | 0.54c(0.39–0.74) |
| Gender | |
| Male | Ref |
| Female | 0.74b(0.63–0.89) |
| Education | |
| Low | Ref |
| Middle | 0.88 (0.70–1.10) |
| High | 0.90 (0.67–1.22) |
| Living alone | |
| No | Ref |
| Yes | 1.13 (0.92–1.38) |
| Cause death | |
| Cancer | Ref |
| Cardiovascular | 0.66b(0.51–0.86) |
| Stroke | 0.79 (0.58–1.10) |
| Other | 0.55c(0.44–0.70) |
| Ill before death | |
| < 6 months | Ref |
| ≥ 6 months | 1.67c(1.39–2.01) |
| Difficulties ADL | |
| None | Ref |
| 1–2 | 0.93 (0.65–1.32) |
| > 2 | 0.95 (0.68–1.33) |
| Assistance ADL | |
| No | Ref |
| Yes, < 3 months | 2.44c(1.57–3.77) |
| Yes, ≥ 3 months | 2.64c(1.77–3.95) |
| Yes, a full year | 1.49a(1.02–2.17) |
| Any nursing home care | |
| No | Ref |
| Yes | 2.69c(2.08–3.48) |
| Any hospice care | |
| No | Ref |
| Yes | 2.55c(1.66–3.91) |
| Country | |
| FR | Ref |
| NL | 1.12 (0.72–1.77) |
| DK | 1.50 (0.99–2.29) |
| BE | 1.52a(1.01–2.29) |
| EE | 1.53 (0.98–2.39) |
| SE | 1.55a(1.05–2.27) |
| CH | 1.58 (0.86–2.92) |
| GR | 1.84a(1.09–3.12) |
| ES | 1.93b(1.33–2.82) |
| IT | 1.99b(1.32–2.99) |
| CZ | 2.15b(1.37–3.37) |
| DE | 2.15b(1.26–3.68) |
| SI | 2.31 (0.93–5.73) |
| PL | 2.61c(1.59–4.30) |
| IL | 2.65c(1.65–4.26) |
| AT | 3.46c(2.03–5.90) |
FR, France; NL, the Netherlands; DK, Denmark; BE, Belgium; EE, Estonia; SE, Sweden; CH, Switzerland; GR, Greece; ES, Spain; IT, Italy; CZ, Czech Republic; DE, Germany; SI, Slovenia; PL, Poland; IL, Israel; AT, Austria. Bold text indicate significant differences.
P ≤ 0.05.
P < 0.01.
P < 0.001.
Discussion
In all studied countries, between half and three quarters of all older people were at least once admitted to an inpatient care facility in their last year of life. The average duration of the total time spent in care facilities varied considerably between countries with 42% of all older people spending 1 month or more in an inpatient care facility (ranging from 27% in Estonia and Greece to 48% in Austria). The large majority of admissions concerned hospitalizations. People from eastern and southern European countries (especially Slovenia, Poland and Israel) had higher chances of hospitalizations in the last year of life compared with northern and western European countries (like France, the Netherlands, Estonia, Belgium, Denmark and Sweden).
Our study confirms findings of previous studies showing that many countries face the challenge that a high number of older people are admitted to inpatient care facilities in the last phase of life, even though healthcare policies are more and more focused on residing at home as long as possible.4–7 The large variance in the occurrence of hospitalizations between countries in our study suggests that non-medical factors affect the decision to hospitalize a person, especially since this variance cannot be fully explained by the differences in people’s illness-related factors. First of all, differences in the organization of care for older community-dwelling people may play a role. In some countries, like the Netherlands and Estonia, general practitioners (GPs) work as gatekeepers to secondary and tertiary care.32 It has been suggested that a gatekeeping system could contribute to a lower proportion of hospitalizations at the end of life.33 Indeed, the Netherlands and Estonia had relatively low hospitalization rates in our study. However, other study countries with full gatekeeping systems (Spain, Italy and Slovenia)32 had relatively high hospitalization rates. This needs further investigation. Second, medical decision-making in the last phase of life could be affected by cultural issues. Bosshard et al.34 concluded that cultural factors affect non-treatment decisions (=decisions to withhold or withdraw treatment) and that important cultural differences can have country-specific effects on end-of-life practices. The authors found that Swiss physicians reported more non-treatment decisions than Dutch, Belgian, Danish and Swedish physicians, while Italian physicians reported the lowest occurrence of non-treatment decisions. Likewise, we found that Italians had higher hospitalization rates than people from the other countries. Third, the availability of long-term care services may be an important factor. The number of residential facilities and formal home care services is still relatively limited in southern European countries. For example, Italy has the lowest number of long-term care beds of all OECD-countries.35 Southern European countries are often considered to be ‘strong-family-ties countries’36; however, the availability and expectation of informal support may actually hinder the organization of residential facilities and formal home care.5,37 In our study, we indeed observed higher hospitalization rates among southern European countries compared with hospitalization rates of northern and western European countries.
In all countries except Switzerland, France, Greece and Israel, the oldest age group was less likely to be hospitalized in the last year of life compared with younger people (48–65 years). Some hospital-based medical or surgical interventions may be considered less appropriate for the oldest old due to frailty or comorbidities.38 In most countries, hospitalizations were more likely for those being ill for a longer period of time and those receiving assistance with ADL. However, overall, people who received assistance a full year had a lower probability of being hospitalized than people who received assistance for a shorter period of time. Maybe these people relied on regular, professional help, making a hospitalization unnecessary in case of illness. In addition, hospitalizations were more likely for people receiving nursing home or hospice care in most countries. The process of institutionalization itself may promote continued institutionalization.39 For instance, it could be easier for older patients to get access to other care organizations while hospitalized. Based on other study findings,3 we can indeed assume that hospital care often preceded nursing home care. However, in our study, we miss information on whether the hospital use was before or after the use of nursing home- or hospice care. The study has other limitations as well. In some countries, the participation rate for end-of-life interviews was rather low (e.g. 41% in Austria). This may have resulted in some overestimation of the number of hospitalizations. Another limitation is the recall bias of proxy-respondents: the average time between the participant’s death and the end-of-life interview was relatively long. However, research suggests that hospitalizations can usually be recalled quite accurately as they are often salient events with large impact.40 Finally, we miss information on people without close relatives or friends nearby who could report on end-of-life circumstances of the deceased. This study has several strengths. We were able to study many European countries and included many participants leading to a representative sample. The 16 selected countries are a balanced representation of countries on several parameters; they cover e.g. countries with different healthcare systems and varying histories of economic growth.
Conclusion
Admissions to hospitals of older people in their last year of life are rather common throughout Europe. The large variation in admissions of older people across the 16 studied countries is striking and suggests that admissions are at least partly driven by system-level or cultural factors rather than by patient needs only.
Supplementary data
Supplementary data are available at EURPUB online.
Supplementary Material
{kind=link}
Acknowledgements
We would like to thank Caspar Looman for his statistical advice.
Funding
This article uses data from SHARE wave 2 release 2.6.0 (DOI:10.6103/SHARE.w2.260), wave 3 release 1 (SHARELIFE, DOI: 10.6103/SHARE.w3.100), wave 4 release 1.1.1 (DOI: 10.6103/SHARE.w4.111) and wave 5 release 1.0.0 (DOI: 10.6103/SHARE.w5.100), see Börsch-Supan et al. (2013) for methodological details. This work has been presented orally at the 9th World Research Congress of the European Association of Palliative care in Dublin (10 June 2016). The SHARE data collection was supported by the European Commission through the 5th Framework Programme [QLK6-CT-2001-00360]; through the 6th Framework Programme [SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812] and through the 7th Framework Programme [SHARE-PREP: No. 211909, SHARE-LEAP: No. 227822, SHARE M4: No. 261982]. Additional funding from the German Ministry of Education and Research; the U.S. National Institute on Aging [U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064] and from various national funding sources is gratefully acknowledged (see www.share-project.org for a full list of funding institutions).
Conflicts of interest: None declared.
Key points
In the 16 studied countries, between half and three quarters of older SHARE participants who died between 2004 and 2013 were at least once admitted to an inpatient care facility in their last year of life.
Although healthcare policies increasingly stress the importance that people reside at home as long as possible, admissions to inpatient care facilities in the last year of life are relatively common across all countries.
People from eastern and southern European countries have much higher chances of being hospitalized in their last year of life compared with people from northern and western European countries.
Hospitalizations were more likely for those being ill for 6 months or more, those receiving assistance with activities of daily living in their last year of life and those receiving any nursing home care or hospice care in their last year of life.
Further, hospitalizations were less likely for persons aged 80+, females and those dying of cardiovascular diseases.
References
- 1. Gomes B, Calanzani N, Gysels M, et al. Heterogeneity and changes in preferences for dying at home: a systematic review. BMC Palliat Care 2013;12:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Gomes B, Higginson I, Calanzani N, et al. Preferences for place of death if faced with advanced cancer: a population survey in England, Flanders, Germany, Italy, the Netherlands, Portugal and Spain. Ann Oncol 2012;23:2006–15. [DOI] [PubMed] [Google Scholar]
- 3. Penders YW, Van den Block L, Donker GA, et al. Comparison of end-of-life care for older people living at home and in residential homes: a mortality follow-back study among GPs in the Netherlands. Br J Gen Pract 2015;65:e724–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Abarshi E, Echteld M, Van den Block L, et al. Transitions between care settings at the end of life in the Netherlands: results from a nationwide study. Palliat Med 2010;24:166–74. [DOI] [PubMed] [Google Scholar]
- 5. Pivodic L, Pardon K, Miccinesi G, et al. Hospitalisations at the end of life in four European countries: a population-based study via epidemiological surveillance networks. J Epidemiol Community Health 2016;70:430–436. [DOI] [PubMed] [Google Scholar]
- 6. Van den Block L, Pivodic L, Pardon K, et al. Transitions between health care settings in the final three months of life in four EU countries. Eur J Public Health 2015;25:569–75. [DOI] [PubMed] [Google Scholar]
- 7. Van den Block L, Deschepper R, Drieskens K, et al. Hospitalisations at the end of life: using a sentinel surveillance network to study hospital use and associated patient, disease and healthcare factors. BMC Health Serv Res 2007;7:69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Pivodic L, Pardon K, Morin L, et al. Place of death in the population dying from diseases indicative of palliative care need: a cross-national population-level study in 14 countries. J Epidemiol Community Health 2016;70:17–24. [DOI] [PubMed] [Google Scholar]
- 9. Houttekier D, Cohen J, Pepersack T, Deliens L. Dying in hospital: a study of incidence and factors related to hospital death using death certificate data. Eur J Public Health 2014;24:751–6. [DOI] [PubMed] [Google Scholar]
- 10. Cohen J, Pivodic L, Miccinesi G, et al. International study of the place of death of people with cancer: a population-level comparison of 14 countries across 4 continents using death certificate data. Br J Cancer 2015;113:1397–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Bekelman JE, Halpern SD, Blankart CR, et al. Comparison of site of death, health care utilization, and hospital expenditures for patients dying with cancer in 7 developed countries. JAMA 2016;315:272–83. [DOI] [PubMed] [Google Scholar]
- 12. Boockvar K, Fishman E, Kyriacou CK, et al. Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and long-term care facilities. Arch Intern Med 2004;164:545–50. [DOI] [PubMed] [Google Scholar]
- 13. Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc 2003;51:549–55. [DOI] [PubMed] [Google Scholar]
- 14. Walling AM, Asch SM, Lorenz KA, et al. The quality of care provided to hospitalized patients at the end of life. Arch Intern Med 2010;170:1057–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Huynh TN, Kleerup EC, Wiley JF, et al. The frequency and cost of treatment perceived to be futile in critical care. JAMA Intern Med 2013;173:1887–94. [DOI] [PubMed] [Google Scholar]
- 16. Beek KV, Woitha K, Ahmed N, et al. Comparison of legislation, regulations and national health strategies for palliative care in seven European countries (Results from the Europall Research Group): a descriptive study. BMC Health Serv Res 2013;13:275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Alcser KH, Benson G, Börsch-Supan A, et al. The Survey of Health, Aging, and Retirement in Europe–Methodology. Mannheim: Mannheim Research Institute for the Economics of Aging (MEA; ), 2005. [Google Scholar]
- 18. Börsch-Supan A, Brugiavini A, Jürges H, et al. First Results from the Survey of Health, Ageing and Retirement in Europe (2004-2007). Starting the Longitudinal Dimension. Mannheim: Mannheim Research Institute for the Economics of Aging (MEA), 2008. [Google Scholar]
- 19. Börsch-Supan A, Brandt M, Hunkler C, et al. Data resource profile: the Survey of Health, Ageing and Retirement in Europe (SHARE). Int J Epidemiol 2013;42:992–1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Börsch-Supan A, Brandt M, Hank K, Schröder M. The Individual and the Welfare State: Life Histories in Europe. Heidelberg: Springer Science & Business Media, 2011. [Google Scholar]
- 21. Schröder M. Retrospective data collection in the Survey of Health, Ageing and Retirement in Europe . SHARELIFE Methodology Mannheim: Mannheim Research Institute for the Economics of Aging (MEA; ), 2011. [Google Scholar]
- 22. Börsch-Supan A, Brandt M, Litwin H, Weber G. Active ageing and solidarity between generations in Europe: First results from SHARE after the economic crisis. Berlin: Walter de Gruyter, 2013. [Google Scholar]
- 23. Malter F, Börsch-Supan A. SHARE Wave 4: Innovations and Methodology. Munich: MEA, Max Planck Institute for Social Law and Social Policy, 2013. [Google Scholar]
- 24. Malter F, Börsch-Supan A. SHARE Wave 5: Innovations and Methodology. Munich: MEA, Max Planck Institute for Social Law and Social Policy, 2015. [Google Scholar]
- 25. Börsch-Supan A, Kneip T, Litwin H, Myck M, Weber G. Ageing in Europe-Supporting Policies for an Inclusive Society. Berlin: Walter de Gruyter, 2015. [Google Scholar]
- 26. Börsch-Supan A. Survey of Health, Aging and Retirement in Europe (SHARE) Wave 2. Release version: 2.6.0. SHARE-ERIC. Data set. DOI: 10.6103/SHARE.w2.260, 2013.
- 27. Börsch-Supan A. Survey of Health, Aging and Retirement in Europe (SHARE) Wave 3 - SHARELIFE. Release version: 1.0.0. SHARE-ERIC. Data set. DOI: 10.6103/SHARE.w3.100, 2010.
- 28. Börsch-Supan A. Survey of Health, Aging and Retirement in Europe (SHARE) Wave 4. Release version: 1.1.1. SHARE-ERIC. Data set. DOI: 10.6103/SHARE.w4.111, 2013.
- 29. Börsch-Supan A. Survey of Health, Aging and Retirement in Europe (SHARE) Wave 5. Release version: 1.0.0. SHARE-ERIC. Data set. DOI: 10.6103/SHARE.w5.100, 2015.
- 30. Weitzen S, Teno JM, Fennell M, Mor V. Factors associated with site of death: a national study of where people die. Med Care 2003;41:323–35. [DOI] [PubMed] [Google Scholar]
- 31. Schneider SL, Kogan I. The International Standard Classification of Education 1997: Challenges in the Application to National Data and the Implementation in Cross-National Surveys. Mannheim: MZES, 2008.
- 32. Kringos DS, Boerma WG, Hutchinson A, Saltman RB. Building Primary Care in a Changing Europe. World Health Organization, European Observatory on Health Systems and Policies, 2015. [PubMed] [Google Scholar]
- 33. Reyniers T, Houttekier D, Pasman HR, et al. The family physician’s perceived role in preventing and guiding hospital admissions at the end of life: a focus group study. Ann Fam Med 2014;12:441–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Bosshard G, Nilstun T, Bilsen J, et al. Forgoing treatment at the end of life in 6 European countries. Arch Intern Med 2005;165:401–7. [DOI] [PubMed] [Google Scholar]
- 35. OECD. Available at: http://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2013/long-term-care-beds-in-institutions-and-hospitals_health_glance-2013-78-en (3 February 2016, date last accessed).
- 36. Bolin K, Lindgren B, Lundborg P. Informal and formal care among single‐living elderly in Europe. Health Econ 2008;17:393–409. [DOI] [PubMed] [Google Scholar]
- 37. Beccaro M, Costantini M, Rossi PG, et al. Actual and preferred place of death of cancer patients. Results from the Italian survey of the dying of cancer (ISDOC). J Epidemiol Commun Health 2006;60:412–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Brameld KJ, Holman C, Bass AJ, et al. Hospitalisation of the elderly during the last year of life: an application of record linkage in Western Australia 1985-1994. J Epidemiol Commun Health 1998;52:740–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Goodwin JS, Howrey B, Zhang DD, Kuo Y-F. Risk of continued institutionalization after hospitalization in older adults. J Gerontol A Biol Sci Med Sci 2011;66:1321–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Addington-Hall J, McPherson C. After-death interviews with surrogates/bereaved family members: some issues of validity. J Pain Symptom Manage 2001;22:784–90. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.