

Abstract
The purpose of this study was to test a model of the factors influencing physical activity, physical function and physical performance at 2 months post hip fracture and compare model fit between men and women. ge, cognitive status, comorbidities, pain, resilience, bone mineral density, total body lean mass, total body fat and grip strength were hypothesized to be directly and/or indirectly related to physical activity, physical function and physical performance. This analysis used data from the seventh Baltimore Hip Studies (BHS-7), a prospective cohort study that included 258 community-dwelling participants, 125 (48%) men and 133 (52%) women, hospitalized for treatment of a hip fracture; survey and objective data were obtained at 2 months post hip fracture. In addition to age, sex and comorbidities (modified Charlson scale), data collection included body composition from dual-energy x-ray absorptiometry (DXA) scans, grip strength, and physical activity, function and performance based on the Yale Physical Activity Survey, the Short Physical Performance Battery and the Lower Extremity Gain Scale. Age, cognition, and comorbidities were not significantly associated with resilience; and, resilience was not associated with pain. In addition, bone mineral density was not associated with physical activity, physical performance or physical function. Total lean body mass, resilience and pain were associated with physical activity, physical function and physical performance in women, but were not consistently associated with physical and functional outcomes in men. Future research should consider evaluation of muscle quality and additional psychosocial factors (e.g., depression, social supports) in model testing.
Despite attempts to improve the recovery process post hip fracture1, at least 25% of older adults do not ever regain their baseline functional ability, especially with regard to transfers, ambulation and stair climbing 2–4. The return to baseline physical function is influenced by many factors including cognitive status, surgical intervention, age, sex, other comorbid conditions, course following surgery, psychosocial factors such as pain, mood, resilience, and having positive social supports3,5–9. he impact of body composition, particularly total body fat and lean mass, on the recovery process has also been studied. Losses of both bone mineral density (BMD) and lean mass, and increases in body fat have been observed in the year following hip fracture, and the rate of decline in BMD is greater than expected compared to similarly aged older women4,10. Normal aging also results in changes in body composition including a persistent decrease in muscle mass and increase in fat mass11 and these changes were noted to be associated with declines in physical activity and functional performance12–14. It is anticipated, therefore that body composition is likely to influence the recovery process among older adults post hip fracture.
The Impact of Body Composition (Fat and Lean Muscle Mass) on Function and Physical Activity
Although there is evidence to support the association between body composition and function and physical activity, findings regarding the relative importance of body composition to function or activity are inconsistent. Moreover, the relationship between these components and outcomes may vary between men and women. One study reported that lower extremity fat-free mass was associated with a decline in function in both men and women15, while other research found the relationship was only significant among women16–18. Muscle quality, defined as power per unit of muscle size, is significantly associated with function or performance among both men and women. In women, muscle quality was associated with both endurance and performance tasks including the 6 minute walk and chair rise test17,19. In men, muscle quality and physical activity were the best predictors of lower extremity function (e.g., getting up from a chair) while in women, muscle quality and the percentage of body fat were the factors that were most predictive of function17. With regard to muscle quality, healthy older men, in addition to having higher levels of overall physical activity, lower visceral adiposity, greater lean mass and higher leg extension power, also have better muscle quality when compared to women.
Differential Recovery Post Hip Fracture among Men and Women
The major focus of hip fracture research has been on older women, given the higher incidence of fracture among these individuals20,21. Repeatedly, it has been noted that older men who experience a hip fracture tend to have more comorbidities and are more likely to die within the 6 months post hip fracture20–25. Differences in recovery of function between men and women vary based on the sample and the specific outcomes considered. For example, a recent study of men and women in the first few months post hip fracture showed that there was no difference in recovery of walking based on self-report by participating men and women22. Conversely, a study comparing observations of functional differences between men and women at approximately the same time point post fracture noted that there was a significant difference with regard to ambulation and ability to transfer such that men were more likely to be independent than women3.
Additional Factors that Influence Function and Physical Activity Post Hip Fracture
Pain and resilience have also been noted to be associated with recovery of function and physical activity in the post hip fracture period. Pain, and management of pain, are particularly relevant in the early period post hip fracture following surgery23 as well as being associated with long-term endurance and ambulation in the community24. Resilience, defined as “the process of adapting well in the face of adversity, trauma, tragedy, threats or significant sources of stress” 25, helps individuals manifest adaptive behavior, especially with regard to social and physical functioning, morale, and somatic health. Resilient individuals are less likely to succumb to illness or disability26,27 and to develop into stronger more resilient individuals. In the post hip fracture period resilience has been associated with disability, overall function and quality of life such that those who are more resilient had less disability, better function and better quality of life28,29.
Based on these prior findings, we proposed and tested a model of the factors influencing overall physical activity, physical function and physical performance at 2 months post hip fracture. Further, we tested whether or not the model fit would be similar among men and women. As shown in Figure 1, it was hypothesized that age, cognitive status, comorbidities, pain, physical resilience, bone mineral density, total body lean mass, total body fat and grip strength would all be directly and/or indirectly related to time spent in all physical activity, physical function and physical performance.
Figure 1.
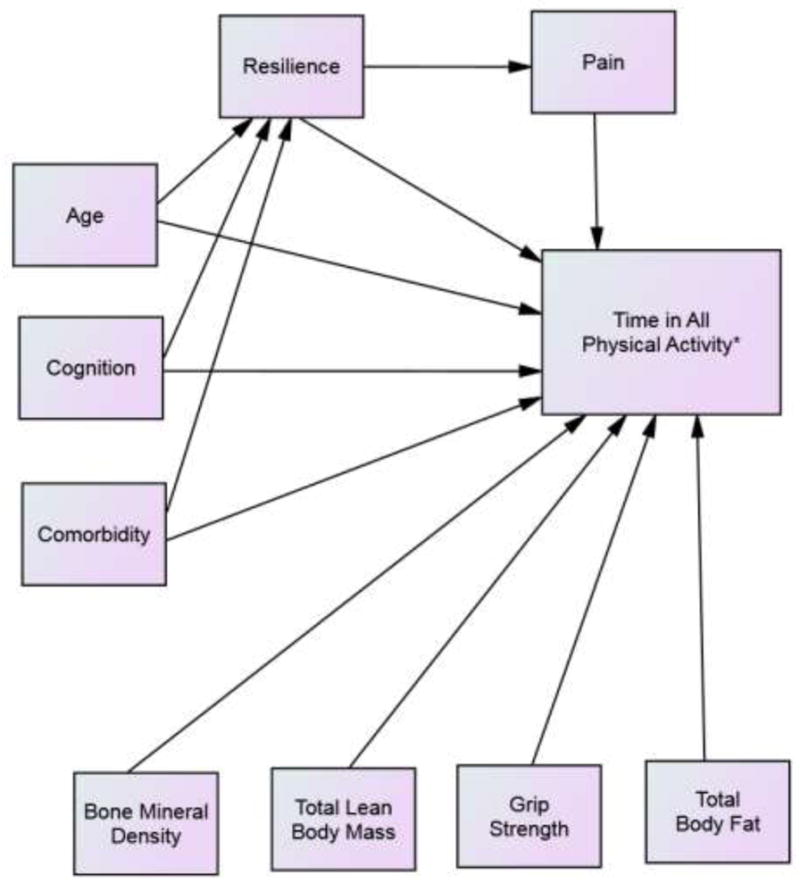
Full Model Testing
*(Same model tested for Short Physical Performance Battery; Lower Extremity Gain Scale)
Methods
This analysis used data from the seventh Baltimore Hip Studies (BHS-7). BHS-7 was an observational prospective study and was carried out in eight hospitals that were part of the BHS hospital network. The study was approved by the University of Maryland Institutional Review Board and review boards at each of the study hospitals. Community-dwelling patients with a hip fracture were screened and enrolled within 15 days of admission to the hospital. Female enrollment was frequency- and temporally-matched to males within each hospital so that females were only screened for enrollment when a male had been enrolled. Demographic data were obtained at baseline and all other measures were obtained at 2 months post hip fracture. For verbal reporting of data, a proxy was asked to respond for participants with a score <36 on the Modified Mini-Mental State Examination (3MS).30
Sample
Eligible patients were community-dwelling, aged 65 years or older and admitted for surgical repair of a hip fracture to one of eight study hospitals. Individuals were excluded if they were not community dwelling, lived more than 70 miles from the hospital, not English speaking, had a pathologic fracture, were bed-bound or wheel chair dependent for 6 months prior to the fracture, weighed more than 300 pounds, or had some type of hardware in the contralateral non-fractured hip (either due to hip fracture or hip replacement) leaving no unaffected hip for bone mineral density measurement. A total of 1705 hip fracture patients were screened and 917 (54%) were eligible (405 males, 512 females). Of those eligible, 180 men and 182 women consented to participate in the study. Twenty-three participants were withdrawn from the study. Specifically, five of these individuals failed to provide data at the baseline and 2-month follow-up visit and another 18 participants were removed from the analysis sample as a result of an IRB-requested post procedure audit. The audit identified six participants who were found to be ineligible because they did not meet study inclusion criteria and 12 participants were determined to be ineligible secondary to failures in the informed consent process. The remaining 339 participants were included in the final analytic sample (168 men, 171 women). At 2 months, 258 participants (125 (48%) men and 133 (52%) women) provided data. Based on Little’s Missing Completely at Random test for the 2 month follow up data, complete responses on each measure ranged from 11% to 32% and data were not missing at random31. The observed measures such as the Lower Extremity Gain Score and the Short Physical Performance Battery had the greatest amount of missing data and this may have been because these individuals were unable or unwilling to perform these measures. There was no difference, however, between those who were recruited into the study at baseline and those who had follow up data obtained with regard to demographic factors, cognition or comorbidities (data not shown). Missing data was handled by the AMOS statistical program and the use of a maximum likelihood solution as described below.
Measures
Demographic and descriptive factors, including age, sex, comorbidities (modified Charlson scale)32 and cognition based on the Modified Mini-Mental State Examination30, were collected using a face-to-face survey. Resilience was measured using a modified version of the 25-Item Resilience Scale 33,34. Pain was evaluated based on total number of areas in which the individual experienced pain (upper extremity, hip, knee, back or ankle pain). Measures of body composition were based on dual-energy x-ray absorptiometry (DXA) scans using either Lunar or Hologic equipment, depending on the particular hospital to which the patient had been admitted. No differences were noted between the different machine types for any of the study outcomes (total body fat, total lean mass and total bone mineral density), although we controlled for type of machine used in all model testing. Total lean mass and body fat are reported in kilograms (kg).
Physical Activity, Physical Function, Physical Performance and Strength Outcomes
Measurement of time spent in all physical activity was based on the Yale Physical Activity Survey (YPAS) 35. The YPAS is a self-report measure with input from the participant or proxy. Questions focus on five categories of physical activity: housework, yard work, caretaking, recreational activities and exercise (moderate intensity activity, such as brisk walking, biking, dance, etc.) performed during a typical week. Prior use provided evidence of two week repeatability (r=0.63, p<.001), and the YPAS has been validated against several physiological variables that are indicative of habitual activity35,36. Time spent across all of these types of physical activity was summed and reported in hours per week.
Physical function was evaluated using the Lower Extremity Gain Scale (LEGS)37. LEGS is an observed, timed measure that focuses on clinically relevant aspects of functioning for hip fracture patients. Completion of the LEGS included observing the participant reach for an item on the ground from a sitting position, putting a sock and shoe on the fractured lower extremity, stepping down four stairs, and getting on and off the toilet. Prior use provided evidence of reliability based on a significant correlation with performance over a two day period (intra-class correlations ranging from 0.63 to 0.96) and validity based on evidence of functional improvement over time37.
Physical performance was measured using the Short Physical Performance Battery (SPPB)38. The SPPB is an observed measure and focuses on the performance of three physical activities: balance based on multiple stances, time to walk three meters, and chair rise. There is prior evidence of reliability and validity of this measure when used with older adults38,39. Lastly, grip strength was measured using the reliable and valid JAMAR Hydraulic Hand Dynamometer 40,41. Three measures of right hand and three measures of left hand grip strength were taken and the maximum measure across both was used as the optimal grip strength recording.
Data Analysis
Descriptive analyses were performed to characterize the sample and Analysis of Variance was done to evaluate differences between men and women for all model variables. With the exception of time in physical activity which was negatively skewed, the variables included in the models were normally distributed. A log transformation for the negatively skewed variable was performed. Multi-collinearity was evaluated based on the variance inflation factor (VIF); the VIFs of all of the model variables were less than 3 indicating no significant multi-collinearity42. Model testing was performed using structural equation modeling and the AMOS statistical program43. he sample covariance matrix was used as input and a maximum likelihood solution sought. The chi-square statistic divided by degrees of freedom was used to estimate model fit. The larger the probability associated with the chi-square divided by degrees of freedom the better the fit of the model to the data. ratio of ≤ 3 was considered to be a good fit44. Path significance (i.e., significance of the Lambda values) was based on the Critical Ratio (CR), which is the parameter estimate divided by an estimate of the standard error. A CR > 2 in absolute value was considered significant43. Significance for path estimates was set at p ≤ 0.055. A squared multiple correlation (R2) was calculated for each of the dependent variables or outcomes (total areas of pain, total pain intensity, and upper and lower extremity function). The R2 indicates the proportion of variance in the dependent variable accounted for by the set of independent variables in the model. Invariance testing to determine if there were differences in model fit between models with nonsignificant paths included or removed and between males and females were based on significant changes between the χ2 and degrees of freedom of each model44.
Results
Means and standard deviations for all model variables and comparisons between sexes are shown in Table 1. There was a significant difference between men and women at 2 months post hip fracture as noted by the fact that men had more comorbidities, less cognitive impairment, spent less time in physical activity, and had higher grip strength, greater bone mineral density, and higher total lean body mass.
Table 1.
Model Variables by Sex
| Variable | Men | Women | Total Sample | Sex Comparison |
|---|---|---|---|---|
|
| ||||
| Mean (SD) | Mean(SD) | Mean (SD) | F(p)* | |
| Age | 80.41(7.70) | 80.96(7.66) | 80.96(7.67) | .37(.54) |
| Charlson comorbidity index** | 2.47(1.88) | 1.70(1.61) | 2.08(1.79) | 14.11(.001) |
| Total activity (hours/week)** | 7.80(8.70) | 10.79(11.34) | 9.43(10.32) | 4.67(.03) |
| Resilience | 5.86(.81) | 5.76(.95) | 5.80(.89) | .65(.42) |
| Cognition (Modified Mini-mental State Examination) | 80.50(18.50) | 87.26(14.58) | 83.97(16.90) | 9.96(.002) |
| Lower Extremity Gains Score | 14.92(10.65) | 17.11(9.54) | 16.07(10.11) | .65(.42) |
| Short Physical Performance Scale | 3.11(2.64) | 3.69(2.63) | 3.40(2.65) | 2.33(.13) |
| Grip Strength (kg)** | 29.49(8.47) | 18.70(5.81) | 23.97(9.01) | 117.35(.001) |
| Bone Mineral Density (gm/cm2)** | .80(.14) | .72(.14) | .76(.15) | 17.55(.001) |
| Total Body Fat (kg) | 21.66(8.54) | 22.99(9.90) | 22.32(9.23) | .96(.33) |
| Total Lean Mass (kg)** | 50.34(7.31) | 35.83(5.97) | 43.21(9.87) | 215.72(.001) |
| Pain | 2.05(1.39) | 2.40(1.39) | 2.24(1.40) | 3.43(.07) |
p≤.055
Variable is either Physical activity (PA); Lower Extremity Gains Score (LEGS); Short Physical Performance Battery (SPPB) depending on the model being tested
Model testing results for men and women are shown in Tables 2 and 3. Across all of the models, in both men and women, age, cognition, and comorbidities were not significantly associated with resilience; and, resilience was not associated with pain. In addition, bone mineral density was not associated with physical activity, physical performance as measured by the SPPB or physical function as measured by the LEGS. Total lean body mass was associated with physical activity, physical function and physical performance in women, although it was only associated with the physical function in men. Among women, those with higher lean mass were less physically active and did worse on physical function and physical performance testing based on the LEGS and the SPPB, respectively. Among men, those with higher lean mass did better with regard to physical function. In women, grip strength was significantly associated with both physical function and physical performance such that those who were stronger did better performing the functional tasks on the LEGS and physical performance activities on the SPPB. Total fat mass was only associated with physical activity among men such that those with higher total fat mass were less physically active. In men, cognition and age were associated with physical activity, physical performance and physical function (except for a trend rather than statistical significance in the relationship between age and physical function). Those who were more intact cognitively were more physically active and did better with regard to physical function and physical performance. Those who were older consistently did worse across all outcomes.
Table 2.
Model Testing in Men
| Parameter | Physical Activity (PA) | Physical Function: Lower Extremity Gains Score (LEGS) Physical | Physical Performance: Short Performance Battery (SPPB) | |||||
|---|---|---|---|---|---|---|---|---|
| Parameter | p* | Parameter | p* | Parameter | p* | |||
| Resilience | <--- | Age | .018 | .860 | .021 | .840 | .021 | .836 |
| Resilience | <--- | Cognition | −.012 | .909 | .032 | .754 | .093 | .359 |
| Resilience | <--- | Comorbidity | −.075 | .461 | −.075 | .463 | −.074 | .469 |
| Pain | <--- | Resilience | .078 | .445 | .075 | .462 | .075 | .464 |
| PA; LEGS; or SPPB** | <--- | Bone Mineral Density | −.009 | .862 | .030 | .614 | −.052 | .221 |
| PA; LEGS; or SPPB | <--- | Total Lean Mass | −.049 | .332 | −.171 | .004 | −.037 | .382 |
| PA; LEGS; or SPPB | <--- | Grip Strength | .113 | .019 | .322 | .001 | .116 | .004 |
| PA; LEGS; or SPPB | <--- | Total Fat Mass | −.175 | .001 | .076 | .202 | −.011 | .807 |
| PA; LEGS; or SPPB | <--- | Comorbidity | .000 | .995 | −.044 | .435 | −.106 | .007 |
| PA; LEGS; or SPPB | <--- | Cognition | .857 | .001 | .776 | .001 | .903 | .001 |
| PA; LEGS; or SPPB | <--- | Age | −.090 | .052 | −.098 | .081 | −.111 | .005 |
| PA; LEGS; or SPPB | <--- | Resilience | .095 | .043 | −.003 | .955 | −.025 | .564 |
| PA; LEGS; or SPPB | <--- | Pain | .021 | .652 | .053 | .370 | .002 | .955 |
| Model Fit | X2/df | 115/41=2.80 | 115/41=2.80 | 117/41=2.86 | ||||
| % Variance Accounted for | 80% | 76% | 88% | |||||
p≤.055
Variable is either Physical activity (PA); Lower Extremity Gains Score (LEGS); Short Physical Performance Battery (SPPB) depending on the model being tested
Table 3.
Model Testing in Women
| Physical Activity (PA) | Physical Function: Lower Extremity Gains Score (LEGS) | Physical Performance: Short Physical Performance Battery (SPPB) | ||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | p* | Parameter | p* | Parameter | p* | |||
| Resilience | <--- | Age | −.049 | .594 | −.051 | .578 | −.050 | .589 |
| Resilience | <--- | Cognition | .098 | .288 | .086 | .355 | .097 | .295 |
| Resilience | <--- | Comorbidity | −.117 | .205 | −.110 | .232 | −.118 | .202 |
| Pain | <--- | Resilience | −.165 | .074 | −.160 | .082 | −.160 | .083 |
| PA; LEGS; or SPPB** | <--- | Bone Mineral Density | .139 | .070 | −.083 | .365 | .094 | .216 |
| PA; LEGS; or SPPB | <--- | Total Lean Mass | −.146 | .051 | −.223 | .013 | −.396 | .001 |
| PA; LEGS; or SPPB | <--- | Grip Strength | .086 | .228 | .334 | .001 | .196 | .004 |
| PA; LEGS; or SPPB | <--- | Total Fat Mass | −.090 | .242 | −.062 | .496 | −.025 | .745 |
| PA; LEGS; or SPPB | <--- | Comorbidity | −.179 | .007 | .012 | .884 | −.119 | .079 |
| PA; LEGS; or SPPB | <--- | Cognition | .504 | .001 | .311 | .001 | .395 | .001 |
| PA; LEGS; or SPPB | <--- | Age | −.275 | .001 | −.278 | .001 | −.350 | .001 |
| PA; LEGS; or SPPB | <--- | Resilience | .131 | .050 | .221 | .008 | .183 | .009 |
| PA; LEGS; or SPPB | <--- | Pain | .170 | .012 | −.157 | .054 | −.050 | .206 |
| Model Fit | X2/df | 182/41=4.44 | 181/41=4.33 | 183/41=4.47 | ||||
| % Variance Accounted for | 50% | 48% | 59% | |||||
p≤.055
Variable is either Physical activity (PA); Lower Extremity Gains Score (LEGS); Short Physical Performance Battery (SPPB) depending on the model being tested
Resilience was associated with physical activity, physical performance and physical function among women, but only associated with physical activity in men. Those that were more resilient spent more time in physical activity and among women did better with regard to physical function and physical performance. Lastly, pain was only associated with physical activity and physical function in women. Women who experienced pain in more areas were more physically active but did worse with regard to physical function based on the LEGS.
With the exception of time spent in physical activity for females, there was improvement in model fit when nonsignificant paths were removed (Table 4). With regard to comparisons of model testing between men and women, all of the models fit the male subsample better than the female subsample. Further, the amount of variance accounted for by the proposed models was consistently higher for the male subsample. Specifically, the proposed model for physical activity explained 80% of the variance in men versus 50% in women, 76% of the variance was explained for physical function based on the LEGS when used with men and this dropped to 48% for women, and 88% of the variance for physical performance based on the SPPB was explained when used with men versus only 59% for women.
Table 4.
Model Comparisons between Full Models and Significant Paths Only and Between Men and Women
| Men Only | Women Only | Male to Female Comparison | |||||||
|---|---|---|---|---|---|---|---|---|---|
| X2 | df | p* | X2 | df | p* | X2 | df | p* | |
| Model Comparisons Full Models to Significant Paths Only | |||||||||
| Full model PA → significant paths only | 89 | 31 | .001 | 32 | 26 | .20 | |||
| Full model SPPB → significant paths only | 84 | 35 | .001 | 126 | 31 | .001 | |||
| Full model LEGS → significant paths only | 88 | 31 | .001 | 99 | 20 | .001 | |||
| Model Comparisons of Significant Paths Only Between Men and Women | |||||||||
| Male to Female PA Models | 23 | 5 | .001 | ||||||
| Male to Female SBBP Models | 34 | 4 | .001 | ||||||
| Male to Female LEGS Models | 55 | 11 | .001 | ||||||
p≤.055
Discussion
The findings from this study provide new information about factors that influence recovery between men and women post hip fracture. They support some, but not all, of the prior work considering the relationship between body composition and physical activity, physical function and physical performance among older adults. Our findings add to what is currently known in this area and support prior work with hip fracture patients indicating that men post hip fracture had more comorbidities, were more intact cognitively, engaged in less overall physical activity, had stronger grip strength and higher bone mineral density than women3,22,45,46. As would be expected, there was a difference between men and women at 2 months with regard to total lean body mass such that the men had a higher total lean body mass than the women.
Our proposed model fit the data across all of the outcomes, although the fit was consistently better in men than women (χ2/df being less than 3 among men and less than 5 among women)44. Further the models all explained approximately 50% or more of the variance in physical activity, physical function or physical performance. Other factors that might help to more comprehensively explain these outcomes that might be added in future research are mood, surgical intervention, type of fracture, medications, social supports and motivation3,47,48. Women particularly, given differences in model fit, may be more likely to be influenced by these additional psychosocial factors.
Our findings support prior work with patients post hip fracture in that there was no association between physical activity, physical function, or physical performance with bone mineral density and generally limited associations between physical activity, physical function, and physical performance with total fat mass49. In contrast, our findings were not consistent when compared to studies exploring these associations among healthy older adults in the community with regard to lean body mass12,17. Lean body mass among our study participants, particularly the women, was significantly associated with physical activity, physical performance, and physical function (particularly lower extremity function as per the LEGS) such that those with higher lean mass spent less time in physical activity and had lower levels of physical function and physical performance. This may have been due to the psychosocial factors noted above including motivation, mood and social supports. Conversely, in studies with community based healthy participants, lean body mass was associated with upper extremity rather than lower extremity function and the percentage of body fat was associated with both lower extremity performance and endurance4,12,17,50,51.
The importance of lean body mass post hip fracture, particularly in women, may be due to the deconditioning that occurs during the post fracture recovery process and thus a decreased ability overall to compensate. Others have also suggested that variation in body composition may actually be more important for women than men and this includes total lean mass51,52. Increasingly there has been a focus on muscle quality (defined as power per unit of muscle size) and the relationship between muscle and fat rather than just absolute muscle quantity17,51. Focusing on muscle quality, specifically muscle power and strength, may help to explain the inverse association we noted between lean muscle mass and physical activity, physical function and physical performance in both women and men.
Model comparisons across sexes provide strong support for evidence of differences between the two groups. Specifically, there were differences in significance of the paths between psychosocial factors and physical activity and physical function in men versus women. Resilience and pain were associated with physical activity, physical function and physical performance in women (with the exception of pain and physical performance) versus resilience being significantly associated only with physical activity in men. Resilience may be more relevant for women with regard to recovery and future testing in this area should be considered. Prior work has also shown that pain tends to be more commonly noted and reported in women post hip fracture versus men and is more likely to influence behavior3. As would be expected, pain in our sample was negatively associated with physical function. Pain was, however, positively associated with physical activity such that women with more areas of pain engaged in more physical activity. It is possible that these individuals were experiencing pain due to osteoarthritis in multiple areas and thus may have increased their physical activity as one strategy to manage their pain. Conversely, these women may have experienced more pain due to engagement in physical activity.
Study Limitations and Conclusions
Although one of the strengths of this study was the inclusion of equal numbers of men and women, the study was relatively small in size and included hip fracture patients from a single metropolitan area. We did not directly measure muscle quality which should certainly be considered in future work. Although missing data was controlled for using maximum likelihood estimation in the Amos statistical program, the findings may be biased in that those who had missing data may have been sicker or impaired functionally to the point that they were unable or unwilling to perform particularly the observed measures. Lastly, physical activity was based on recall and subjective input which may have been inflated and in some situations proxy reporting was done when participants were significantly cognitively impaired. Despite these limitations, this study adds to what is currently known about body composition and the impact it has on physical activity, physical function and physical performance across both sexes and provides recommendations to guide future research particularly the inclusion of mood, muscle quality, social supports and motivation in model testing.
Highlights.
Men post hip fracture had more comorbidities, were more intact cognitively, engaged in less overall physical activity, had stronger grip strength and higher bone mineral density than women.
There was a difference between men and women at 2 months post hip fracture with regard to total lean body mass such that the men had a higher total lean body mass than the women.
There was no association between physical activity, physical function, or physical performance with bone mineral density and generally limited associations between physical activity, physical function, and physical performance with total fat mass.
Lean body mass among our study participants, particularly the women, was significantly associated with physical activity, physical performance, and physical function (particularly lower extremity function as per the LEGS) such that those with higher lean mass spent less time in physical activity and had lower levels of physical function and physical performance.
Resilience and pain were associated with physical activity, physical function and physical performance in women (with the exception of pain and physical performance) versus resilience being significantly associated only with physical activity in men.
Acknowledgments
This research was supported by grants from the National Institute on Aging (R37 AG09901, R01 AG029315, P30 AG028747). We would also like to thank all hospital personnel for their support of the research and the participants and their families for their generous commitment to this project.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Barbara Resnick, University of Maryland School of Nursing, 655 West Lombard Street, Baltimore, MD 21201.
J. Richard Hebel, University of Maryland School of Medicine, Department of Epidemiology and Public Health, Baltimore, MD 21201.
Ann L. Gruber-Baldini, University of Maryland School of Medicine, Department of Epidemiology and Public Health, Baltimore, MD 21201.
Gregory E. Hicks, University of Delaware, Department of Physical Therapy, University of Delaware, STAR Health Sciences Complex, 540 S. College Ave, Suite 210E, Newark, DE 19713.
Marc C. Hochberg, University of Maryland School of Medicine, Departments of Medicine and Epidemiology and Public Health, Baltimore, MD 21201.
Denise Orwig, University of Maryland School of Medicine, Department of Epidemiology and Public Health, Baltimore, MD 21201.
Marty Eastlack, Assistant Professor and Director of PT Admissions, Arcadia University, Department of Physical Therapy, 450 S. Easton Rd., Glenside, PA 19038.
Jay Magaziner, University of Maryland, School of Medicine, Department of Epidemiology and Public Health, Baltimore, MD 21201.
References
- 1.Besdine R. [Last accessed January, 2018];Promitiong a better way to manage hip fracture. Available at: https://news.brown.edu/articles/2015/08/besdine.
- 2.Alarcon T, Gonzalez-Montalvo I, Gotor P, Madero R, Otero A. Activities of daily living after hip fracture: Profile and rate of recovery during 2 years of follow up. Osteoporosis International. 2011;22:1609–1613. doi: 10.1007/s00198-010-1314-2. [DOI] [PubMed] [Google Scholar]
- 3.Arinzon Z, Shabat S, Peisakh A, Gepstein R, Berner Y. Gender differences influence the outcome of geriatric rehabilitation following hip fracture. Archives of Gerontology and Geriatrics. 2010;50:86–91. doi: 10.1016/j.archger.2009.02.004. [DOI] [PubMed] [Google Scholar]
- 4.Visser M, Harris T, Fox K, et al. Change in muscle mass and muscle strength after a hip fracture: Relationship to mobility recovery. Journals of Gerontology Series A: Biological Sciences & Medical Sciences. 2000;55A(8):M434–M448. doi: 10.1093/gerona/55.8.m434. [DOI] [PubMed] [Google Scholar]
- 5.Ariza-Vega P, Jiménez-Moleón J, Tange Kristensen M. Non-Weight-bearing status compromises the functional level up to 1 yr after hip fracture surgery. American Journal of Physical Medicine & Rehabilitation. 2014;93(8):641–648. doi: 10.1097/PHM.0000000000000075. [DOI] [PubMed] [Google Scholar]
- 6.Beaupre L, Jones C, Johnston D, Wilson D, Majumdar S. Recovery of function following a hip fracture in geriatric ambulatory persons living in nursing homes: Prospective cohort study. Journal of the American Geriatrics Society. 2012;60(7):1268–1273. doi: 10.1111/j.1532-5415.2012.04033.x. [DOI] [PubMed] [Google Scholar]
- 7.Ortiz-Alonso F, Vidán-Astiz M, Alonso-Armesto M, et al. The pattern of recovery of ambulation after hip fracture differs with age in elderly patients. Journals of Gerontology Series A: Biological Sciences & Medical Sciences. 2012;67(6):690–697. doi: 10.1093/gerona/glr231. [DOI] [PubMed] [Google Scholar]
- 8.Taraldsen K, Sletvold O, Thingstad P, et al. Physical behavior and function early after hip fracture surgery in patients receiving comprehensive geriatric care or orthopedic care--a randomized controlled trial. Journals of Gerontology Series A: Biological Sciences & Medical Sciences. 2014;69(3):338–345. doi: 10.1093/gerona/glt097. [DOI] [PubMed] [Google Scholar]
- 9.Gruber-Baldini A, Zimmerman S, Morrison R, et al. Cognitive impairment in hip fracture patients: Timing of detection and longitudinal follow-up. Journal of the American Geriatrics Society. 2003;51(9):1227–36. doi: 10.1046/j.1532-5415.2003.51406.x. [DOI] [PubMed] [Google Scholar]
- 10.Magaziner J, Wehren L, Hawkes WG, et al. Women with hip fracture have a greater rate of decline in bone mineral density than expected: Another significant consequence of a common geriatric problem. Osteoporosis International. 2006;17(7):971–77. doi: 10.1007/s00198-006-0092-3. [DOI] [PubMed] [Google Scholar]
- 11.Raguso C, Kyle U, Kossovsky M, et al. A longitudinal study on body composition changes in the elderly: Role of physical exercise. Clinical Nutrition. 2006;25:573–80. doi: 10.1016/j.clnu.2005.10.013. [DOI] [PubMed] [Google Scholar]
- 12.Charlton K, Batterham M, Langford K, et al. Lean body mass associated with upper body strength in healthy older adults while higher body fat limits lower extremity performance and endurance. Nutrients. 2015;7:7126–42. doi: 10.3390/nu7095327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Woo J, Leung J, Kwok T. BMI, body composition and physical functioning in older adults. Obesity. 2007;15:1886–94. doi: 10.1038/oby.2007.223. [DOI] [PubMed] [Google Scholar]
- 14.McGregor R, Cameron-Smith D, Poppitt S. It is not just muscle mass: A review of muscle quality, composition and metabolism during ageing as determinatns of muscle function and mobility in later life. [Last accessed January, 2018];Longevity & Healthspan. 2014 doi: 10.1186/2046-2395-3-9. Available at: http://www.longevityandhealthspan.com/content/3/1/9. [DOI] [PMC free article] [PubMed]
- 15.Fantin R, Francesco V, Fontana G, et al. Longitudinal body composition changes in old men and women: Interrelationships with worsening disability. Journal of Gerontology A: Biological Sciences Medicine and Science. 2007;62:1375–81. doi: 10.1093/gerona/62.12.1375. [DOI] [PubMed] [Google Scholar]
- 16.Zoico E, Di Francesco V, Mazzali G, et al. High baseline values of fat mass, indepedently of appendicular skeletal mass, predict 2-year onset of disability in elderly subjects as the high end of the functional spectrum. Aging Clinical and Experimental Research. 2007;19:154–59. doi: 10.1007/BF03324682. [DOI] [PubMed] [Google Scholar]
- 17.Straight C, Brady A, Evans E. Muscle quality and relative adiposity are the strongest predictors of lower extremity physical function in older women. Maturitas. 2015;80(1):95–9. doi: 10.1016/j.maturitas.2014.10.006. [DOI] [PubMed] [Google Scholar]
- 18.Riebe D, Blissmer B, Greaney M, Garber C, Lees F, Clark P. The relationship between obesity, physcial activity and physical function in older adults. Journal of Aging and Health. 2009;21:1159–78. doi: 10.1177/0898264309350076. [DOI] [PubMed] [Google Scholar]
- 19.Brady A, Straight C, Schmidt M, Evans E. Impact of body mass index on the relationship between muscle quality and physical function in older women. Journal of Nutrition and Health in Aging. 2014;18(4):378–82. doi: 10.1007/s12603-013-0421-0. [DOI] [PubMed] [Google Scholar]
- 20.Abrahamsen B, van Staat, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: systematic epidemiological review. Osteoporosis International. 2009;20(10):1633–50. doi: 10.1007/s00198-009-0920-3. [DOI] [PubMed] [Google Scholar]
- 21.Adams A, Shi J, Takayanagi M, Dell R, Funahashi T, Jacobsen S. Ten-year hip fracture incidence rate trends in a large California population, 1997–2006. Osteoporosis International. 2013;24(1):373–76. doi: 10.1007/s00198-012-1938-5. [DOI] [PubMed] [Google Scholar]
- 22.Beaupre L, Carson J, Noveck H, Magaziner J. Recovery of walking ability and return to community living within 60 Days of hip fracture does not differ between male and female survivors. Journal of the American Geriatrics Society. 2015;63(8):1640–44. doi: 10.1111/jgs.13535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Morrison RS, Dickman E, Hwang U, et al. Regional nerve blocks improve pain and functional outcomes in hip fracture: A randomized controlled trial. Journal of the American Geriatrics Society. 2016;64(12):2433–39. doi: 10.1111/jgs.14386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Peiris C, Shields N, Kingsley M, Yeung J, Hau R, Taylor N. Maximum tolerated dose of walking for community-dwelling people recovering from hip fracture: A dose-response trial. Archives of Physical Medicine and Rehabilitation. 2017;98(12):2533–39. doi: 10.1016/j.apmr.2017.03.027. [DOI] [PubMed] [Google Scholar]
- 25.American Psychological Association Help Center. [Last accessed January, 2018];The road to resilience. 2018 Available at: http://www.apa.org/helpcenter/road-resilience.aspx.
- 26.Battalio SL, Silverman Am, Ehde Dm, Amtmann D, Edwards KA, Jensen MP. Resilience and function in adults with physical disabilities: An observational study. Archives of Physical Medicine and Rehabilitation. 2017;98:1158–64. doi: 10.1016/j.apmr.2016.11.012. [DOI] [PubMed] [Google Scholar]
- 27.Bolton KW, Osborne AS. Resilience protective factors in an older adults population: A qualitative interpretive meta-synthesis. Social Work Research. 2016;40(3):171–81. [Google Scholar]
- 28.Rebagliati GA, Sciumè L, Iannello P, et al. Frailty and resilience in an older population. The role of resilience during rehabilitation after orthopedic surgery in geriatric patients with multiple comorbidities. Functional Neurology. 2016;31(3):171–77. doi: 10.11138/FNeur/2016.31.3.171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Huang TT, Acton GJ. Ways to maintain independence among Taiwanese elderly adults with hip fractures: qualitative study. Geriatric Nursing. 2009;30(1):28–35. doi: 10.1016/j.gerinurse.2008.03.006. [DOI] [PubMed] [Google Scholar]
- 30.Bassuk S, Murphy J. Characteristics of the Modified Mini-Mental State Exam among elderly persons. Journal of Clinical Epidemiology. 2003;56(7):622–28. doi: 10.1016/s0895-4356(03)00111-2. [DOI] [PubMed] [Google Scholar]
- 31.Cheng L. Little’s missing at random test. Journal of the American Statistical Association. 1988;83:1198–1202. [Google Scholar]
- 32.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Prognostic development and validation. Journal of Chronic Disease. 1987;40(5):373–383. doi: 10.1016/0021-9681(87)90171-8. [DOI] [PubMed] [Google Scholar]
- 33.Wagnild G. Resilience and successful aging. Comparison among low and high income older adults. Journal of Gerontological Nursing. 2003;29(12):42–9. doi: 10.3928/0098-9134-20031201-09. [DOI] [PubMed] [Google Scholar]
- 34.Wagnild G, Young H. Development and psychometric evaluation of the Resilience Scale. Journal of Nursing Measurement. 1993;1(2):165–177. [PubMed] [Google Scholar]
- 35.Dipietro L, Caspersen CJ, Ostfeld AM, Nadel ER. A survey for assessing physical activity among older adults. Medicine Science Sports and Exercise. 1993;25(5):628–42. [PubMed] [Google Scholar]
- 36.Pescatello L, DiPietro L, Fargo A, Ostfeld A, Nadel E. The impact of physical activity and physical fitness on health indicators among older adults. Journal of Aging and Physical Activity. 1994;2:2–13. [Google Scholar]
- 37.Zimmerman SI, Williams G, Lapuerta P, et al. The lower extremity gain scale (LEGS): performance-based measure to assess hip fracture recovery. The Gerontologist. 2002;42(10):238. [Google Scholar]
- 38.Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. Journals of Gerontology: Medical Sciences. 1994;49(2):M85–M94. doi: 10.1093/geronj/49.2.m85. [DOI] [PubMed] [Google Scholar]
- 39.Freire A, Guerra R, Alvarado B, Guralnik J, Zunzunegui M. Validity and reliability of the short physical performance battery in two diverse older adult populations in Quebec and Brazil. Journal of Aging and Health. 2012;24(5):863–78. doi: 10.1177/0898264312438551. [DOI] [PubMed] [Google Scholar]
- 40.Ashford R, Nagelburg S, Adkins R. Sensitivity of the Jamar Dynamometer in detecting submaximal grip effort. Journal of Hand Surgery. 1996;21:4-2-5. doi: 10.1016/S0363-5023(96)80352-2. [DOI] [PubMed] [Google Scholar]
- 41.Roberts H, Denison H, Martin H, et al. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age and Ageing. 2011;40:423–29. doi: 10.1093/ageing/afr051. [DOI] [PubMed] [Google Scholar]
- 42.Grewal R, Cote J, Baumgartner H. Multicollinearity and measurement error in structural equation models: Implications for theory testing. Marketing Science. 2004;23(4):519–29. [Google Scholar]
- 43.Arbuckle J. Amos users’ guide version 3.6. Chicago: Small Waters Corporation; 1997. [Google Scholar]
- 44.Bollen K. Structural equations with latent variables. Wiley-Interscience; 1989. [Google Scholar]
- 45.Di Manaco M, Castiglioni C, Vallero F, Di Monaco R, Tap[ero R. Men recover ability function less than women do. American Journal of Physicial Medicine & Rehabilitation. 2012;91(4):309–15. doi: 10.1097/PHM.0b013e3182466162. [DOI] [PubMed] [Google Scholar]
- 46.Messen J, Pisani S, Gambino S, Michele F. Assessment of mortality risk in elderly patients after proximal femoral fracture. Orthopedics. 2014;37(2):194–200. doi: 10.3928/01477447-20140124-25. [DOI] [PubMed] [Google Scholar]
- 47.Miller LE, Gondusky JS, Bhattacharyya S, Kamath AF, Boettner F, Wright J. Does surgical approach affect outcomes in total hip arthroplasty through 90 days of follow-up? systematic review with meta-analysis. [Last accessed January 21, 2018];Journal of Arthroplasty. 2017 doi: 10.1016/j.arth.2017.11.011. Available at: https://www.ncbi.nlm.nih.gov/pubmed/29195848. [DOI] [PubMed]
- 48.Iaboni A, Rawson K, Burkett C, Lenze EJ, Flint AJ. Potentially inappropriate medications and the time to full functional recovery after hip fracture. Drugs and Aging. 2017;34(9):723–28. doi: 10.1007/s40266-017-0482-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Wehren L, Hawkes W, Hebel J, Orwig D, Magaziner J. Bone mineral densty, soft tissue body composition, strength and functioning after hip fracture. Journal of Gerontology: Medical Sciences. 2005;60A(1):80–4. doi: 10.1093/gerona/60.1.80. [DOI] [PubMed] [Google Scholar]
- 50.Cesari M, Rolland Y, Abellan Van Kan G, Bandinelli S, Vellas B, Ferrucci L. Sarcopenia-related parameter and incident disability in older persons: Results from the “Invecchiare in Chianti” Study. Journals of Gerontology Series A: Biological Sciences & Medical Sciences. 2015;70(4):457–63. doi: 10.1093/gerona/glu181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Valentine R, Misic M, Rosengren K, Woods J, Evans E. Sex impacts the relation between body composition and physical function in older adults. Menopause. 2009;16(3):518–23. doi: 10.1097/gme.0b013e31818c931f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Wray L, Blaum C. Explaining the role of of sex on disability: population based study. The Gerontologist. 2001;41:499–510. doi: 10.1093/geront/41.4.499. [DOI] [PubMed] [Google Scholar]