

Abstract
Background
Food fortification is one approach for addressing anemia, but information on program effectiveness is limited.
Objective
We evaluated the impact of Costa Rica’s fortification program on anemia in women aged 15–45 y and children aged 1–7 y.
Design
Reduced iron, an ineffective fortificant, was replaced by ferrous fumarate in wheat flour in 2002, and ferrous bisglycinate was added to maize flour in 1999 and to liquid and powdered milk in 2001. We used a one-group pretest-posttest design and national survey data from 1996 (baseline; 910 women, 965 children) and 2008–2009 (endline; 863 women, 403 children) to assess changes in iron deficiency (children only) and anemia. Data were also available for sentinel sites (1 urban, 1 rural) for 1999–2000 (405 women, 404 children) and 2008–2009 (474 women, 195 children), including 24-h recall data in children. Monitoring of fortification levels was routine.
Results
Foods were fortified as mandated. Fortification provided about one-half the estimated average requirement for iron in children, mostly and equally through wheat flour and milk. Anemia was reduced in children and women in national and sentinel site comparisons. At the national level, anemia declined in children from 19.3% (95% CI: 16.8%, 21.8%) to 4.0% (95% CI: 2.1%, 5.9%) and in women from 18.4% (95% CI: 15.8%, 20.9%) to 10.2% (95% CI: 8.2%, 12.2%). In children, iron deficiency declined from 26.9% (95% CI: 21.1%, 32.7%) to 6.8% (95% CI: 4.2%, 9.3%), and iron deficiency anemia, which was 6.2% (95% CI: 3.0%, 9.3%) at baseline, could no longer be detected at the endline.
Conclusions
A plausible impact pathway suggests that fortification improved iron status and reduced anemia. Although unlikely in the Costa Rican context, other explanations cannot be excluded in a pre/post comparison.
Keywords: anemia, Costa Rica, food fortification, hemoglobin, women and children
INTRODUCTION
Anemia is endemic throughout the world. In 2011, 29% of nonpregnant women, 38% of pregnant women, and 43% of children aged 6–59 mo were anemic, with estimates improving only modestly since 1995 (1). Maternal anemia has serious consequences, among them increased maternal mortality, adverse birth outcomes, poor mental health and fatigue, and delayed child development (2). Anemia in children affects child development, but this is less clear in children younger than 3 y, among whom only effects on motor development are consistent (2). The most common cause of anemia is iron deficiency, and worldwide, the proportion of all anemia amenable to iron supplementation is estimated to be ~50% in nonpregnant and pregnant women and 42% in children (1).
Food fortification is described as one of the most cost-effective strategies available to improve micronutrient status, including iron status (3). A variety of food vehicles have been fortified with iron and other nutrients, and these can be grouped in 3 broad categories: staples, condiments, and processed commercial foods (4). Systematic reviews of mostly efficacy studies show that iron status improves and anemia declines when foods fortified with iron are consumed (4–6). However, evidence from national fortification programs is limited and inconsistent (7–9). In an analysis of the characteristics of 78 national wheat flour fortification programs, it was concluded that only 9 could be expected to have the desired impact; the problems identified were common use of atomized and hydrogen-reduced iron powders, which have poor bioavailability, and inadequate levels of fortification given levels of consumption of wheat flour (7). An example is Brazil, where hemoglobin levels in children remained essentially constant after fortification of wheat and maize flour became mandatory; this was attributed to the use of low bioavailability fortificants and weak enforcement mechanisms (10).
We searched for relevant data to carry out an evaluation of the national food fortification program in Costa Rica, where wheat and maize flour and liquid and powdered milk are mandated by law to be fortified with iron and other micronutrients. We use a one-group pretest-posttest design (11) to assess the impact on anemia in women and children and on iron status in children. We also identify pathways leading to impact.
SUBJECTS AND METHODS
Food Fortification Program
Costa Rica has been a pioneer and a model for mass fortification (Table 1). It is distinguished by fortifying several staples. Salt has been fortified with iodine since 1972 and sugar with vitamin A during 1974 through 1981 and then reinitiated in 2003. Wheat flour was fortified with 45 mg/kg of reduced iron starting in 1958; since 2002, 55 mg/kg of a more bioavailable fortificant, ferrous fumarate, has been used instead. Ferrous bisglycinate was added to maize flour (22 mg/kg) in 1999 and to milk (1.4 mg/250 mL) in 2001; powdered milk is also fortified with ferrous bisglycinate. Rice is not fortified with iron. Wheat and maize flour and rice are fortified with several water-soluble vitamins, including folic acid. Milk is also fortified with folic acid and vitamins A and D.
TABLE 1.
Fortification of staple foods and condiments in Costa Rica
| Staple | Year started | Nutrient | Content |
|---|---|---|---|
| Wheat flour1 | 2002 | Thiamin | 6.2 mg/kg |
| Riboflavin | 47.2 mg/kg | ||
| Niacin | 55.0 mg/kg | ||
| Folic acid | 1.8 mg/kg | ||
| Iron (ferrous fumarate) | 55.0 mg/kg | ||
| Milk2 | 2001 | Iron (ferrous bisglycinate) | 1.4 mg/250 mL |
| Vitamin A | 180.0 μg/250 mL | ||
| Folic acid | 40.0 μg/250 mL | ||
| Maize flour | 1999 | Iron (ferrous bisglycinate) | 22.0 mg/kg |
| Niacin | 45.0 mg/kg | ||
| Thiamin | 4.0 mg/kg | ||
| Riboflavin | 2.5 mg/kg | ||
| Folic acid | 1.3 mg/kg | ||
| Rice | 2002 | Folic acid | 1.8 mg/kg |
| Thiamin | 6.0 mg/kg | ||
| Vitamin B-12 | 10.0 μg/kg | ||
| Niacin | 50.0 mg/kg | ||
| Vitamin E | 15.0 IU/kg | ||
| Selenium | 105.0 μg/kg | ||
| Zinc | 19.0 mg/kg | ||
| Salt3 | 1972 | Iodine | 30–60 mg/kg |
| Fluoride | 175–225 mg/kg | ||
| Sugar4 | 2003 | Vitamin A | 5.0 mg/kg |
Wheat flour had been fortified with reduced iron since 1958. In 2002, the fortificant was changed to ferrous fumarate. The extraction rate was ~76%.
Powdered milk is also fortified with ferrous bisglycinate at 11.0 times the content of liquid milk, or 62.8 mg/kg, to provide an equivalent amount when reconstituted. Powdered milk also contains vitamin C.
Fluoride was added in 1987.
Sugar was fortified with vitamin A from 1974 to 1981; it was reinitiated in 2003.
INCIENSA (Costa Rican Institute of Research and Teaching in Nutrition) supports the Ministry of Health in enforcing and supervising compliance with fortification regulations. Yearly, professionals from INCIENSA visit each food factory and, as part of the auditing/inspection, take samples of the fortified foods. Other samples are taken from the market. Samples are analyzed for their micronutrient content and other chemical and microbiologic parameters in INCIENSA’s laboratories. Total iron is determined by atomic absorption spectrophotometry. Around 100 samples of each type of food are analyzed every year. In a special study in 2008, 246 samples of wheat flour were collected from bakeries in all counties, allowing examination of variation in iron fortification content by mill, brand of flour, and county.
Study design
The major changes in the fortification of staples with iron occurred between 1999 and 2002. We analyze national representative surveys carried out before and after these changes, in 1996 (12) and 2008–2009, respectively (13), and sentinel site surveys, one rural and one urban, collected in 1999–2000 (14) and 2008–2009 (13), respectively. The national surveys were cross-sectional, combining geographical stratification and cluster sampling within each stratum (12, 13). Accordingly, the country was classified into 3 regions: metropolitan, urban, and rural, followed by 2-stage cluster sampling. The first stage involved random sampling of census segments, and the second stage comprised systematic random sampling of clusters of 3 households from the selected segments. Only one person of the target age groups was selected per household, and when more than one was available, the youngest was selected. The sentinel sites surveys were also cross-sectional and followed the same sampling procedure but without stratification. Of the target age groups, only pregnant and nonpregnant women aged 15–45 y (those breastfeeding a child <6 mo of age were excluded from the surveys) and children aged 1–7 y had relevant pre/post data. Data collection nationally and in the sentinel sites included hemoglobin in women aged 15–45 y and children aged 1–7 y; ferritin was available at both time points for a random subsample of children only. Single 24-h recall data were collected in the sentinel sites in 2008–2009 in children, permitting estimation of the contribution of fortification to iron intakes.
All national and sentinel surveys were reviewed and approved by INCIENSA’s Scientific Ethics Committee; the 2008–2009 surveys were also reviewed and approved by the National Health Research Council. Adults were read a consent statement, and those agreeing to participate signed the consent form; a copy was given to the participant, and another was kept by the Ministry of Health. The caretaker provided signed, informed consent for children.
Sample sizes
Inclusion criteria were the availability of hemoglobin for children and women. We excluded pregnant women because few were included. Sample sizes are given in Table 2 and Table 3; sample sizes for children were lower in 2008 because a large decline in anemia prevalence was expected relative to 1996.
TABLE 2.
Descriptive data for preschool children (aged 1–7 y)
| Descriptors | National surveys
|
Sentinel sites
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1996 (n = 965)
|
2008–2009 (n = 403)
|
Difference, P value1 | 1999–2000 (n = 404)
|
2008–2009 (n = 195)
|
Difference, P value1 | |||||
| n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | |||
| Continuous | ||||||||||
| Age, y | 965 | 4.2 (4.1, 4.3) | 403 | 4.2 (4.0, 4.4) | 0.976 | 404 | 4.0 (3.9, 4.2) | 195 | 4.0 (3.7, 4.2) | 4.2 (4.1, 4.3) |
| Hemoglobin, g/dL | 965 | 12.1 (12.1, 12.2) | 403 | 12.8 (12.7, 12.9) | <0.001 | 404 | 12.1 (12.0, 12.2) | 195 | 12.6 (12.5, 12.8) | <0.001 |
| Serum ferritin,2 μg/L | 227 | 20.5 (18.0, 23.1) | 370 | 32.1 (30.3, 34.5) | <0.001 | 391 | 19.9 (18.2, 21.7) | 90 | 31.5 (25.7, 38.6) | <0.001 |
| Categorical | ||||||||||
| Male sex | 462 | 47.9 (44.7, 51.0) | 228 | 56.6 (51.7, 61.4) | 0.003 | 198 | 49.0 (44.1, 53.9) | 93 | 47.7 (40.7, 54.7) | 0.766 |
| Area of residence | ||||||||||
| Urban | 341 | 35.3 (32.3, 38.3) | 174 | 43.2 (38.3, 48.0) | 0.008 | 197 | 49.0 (43.9, 53.6) | 98 | 50.3(43.2, 57.3) | 0.732 |
| Rural | 318 | 33.0 (30.0, 36.0) | 130 | 32.2 (27.7, 36.8) | 207 | 51.0 (46.4, 56.1) | 97 | 49.7 (42.7, 56.8) | ||
| Metropolitan | 306 | 31.7 (28.8, 34.7) | 99 | 24.6 (20.4, 28.8) | — | — | ||||
| Anemia3 | 19.3 (16.8, 21.8) | 4.0 (2.1, 5.9) | <0.001 | 20.0 (16.1, 13.9) | 9.7 (5.6, 13.9) | 0.002 | ||||
| Iron deficiency4 | 26.9 (21.1, 32.7) | 6.8 (4.2, 9.3) | <0.001 | 28.6 (24.2, 33.1) | 13.3 (6.3, 20.4) | <0.001 | ||||
| Iron deficiency anemia | 6.2 (3.0, 9.3) | 0.0 | <0.001 | 9.0 (6.1, 11.8) | 0.0 | <0.001 | ||||
P values were obtained from t tests for continuous variables, χ2 tests for area of residence, and z tests for 2 independent proportions for anemia, iron deficiency, and iron deficiency anemia.
Values are geometric means.
Anemia was adjusted for altitude and defined as hemoglobin <11 g/dL for children aged <5 y and <11.5 g/dL for children aged 5–7 y.
Deficiency was defined as serum ferritin <12 μg/L for children aged <5 y and <15 μg/L for children aged ≥5 y. Serum ferritin was available in only a subset of children; n = 227, 370, 391, and 90 for national surveys in 1996 and 2008 and sentinel surveys in 1999–2000 and 2008–2009, respectively.
TABLE 3.
Descriptive data for women of reproductive age (15–45 y)
| Descriptors | National surveys
|
Sentinel sites
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1996 (n = 965)
|
2008–2009 (n = 403)
|
Difference, P value1 | 1999–2000 (n = 404)
|
2008–2009 (n = 195)
|
Difference, P value1 | |||||
| n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | |||
| Continuous | ||||||||||
| Age, y | 910 | 30.9 (30.4, 31.4) | 863 | 31.3 (30.7, 31.8) | 0.315 | 405 | 31.2 (30.6, 31.8) | 474 | 30.6 (29.8, 31.4) | 0.250 |
| Hemoglobin, g/dL | 910 | 12.9 (12.8, 13.0) | 863 | 13.3 (13.2, 13.4) | <0.001 | 405 | 12.9 (12.8, 13.0) | 474 | 13.4 (13.3, 13.5) | <0.001 |
| Categorical | ||||||||||
| Area of residence | ||||||||||
| Urban | 305 | 34.3 (31.2, 37.4) | 299 | 43.7 (40.4, 47.0) | 0.001 | 198 | 51.1 (46.2, 56.0) | 199 | 58.0 (53.6, 62.5) | 0.040 |
| Rural | 293 | 33.5 (30.4, 36.6) | 187 | 34.6 (31.5, 37.8) | 207 | 48.9 (44.0, 53.8) | 275 | 42.0 (37.5, 46.4) | ||
| Metropolitan | 312 | 32.2 (29.2, 35.2) | 377 | 21.7 (18.9, 24.4) | — | — | ||||
| Anemia2 | 18.4 (15.8, 20.9) | 10.2 (8.2, 12.2) | <0.001 | 18.0 (14.3, 21.8) | 8.7 (6.1, 11.2) | <0.001 | ||||
P values were obtained from t tests for continuous variables, x2 tests for area of residence, and z tests for 2 independent proportions for anemia.
Anemia was adjusted for altitude and defined as hemoglobin <12 g/dL.
Hemoglobin and ferritin
All assessments were made at INCIENSA’s laboratories by using venous blood. Hemoglobin was measured with a photometric cyanmethemoglobin method at baseline (12) and an automated hematology analyzer (KX-21; Sysmex) by using colorimetric methods at endline (13); both hemoglobin methods are accurate and precise and produce similar results (15). Serum ferritin was evaluated with an immunoradiometric assay at baseline (12) and an immunoassay analyzer (Immulite 1000; Siemens Medical Solutions Diagnostics) at endline (13); both ferritin methods produce highly correlated values (r = 0.99) with mean values within 5 μg/L (16). Anemia was defined as hemoglobin <11 g/dL for children aged 6–59 mo, <11.5 g/dL for 5- to 11-y-olds, and <12 mg/L for women of reproductive age. Anemia was adjusted for altitude by using WHO cutoff recommendations (17). Low iron stores included ferritin levels <12 μg/L for children aged <5 y and <15 μg/L for children aged ≥5 y. Iron deficiency anemia was defined as the presence of anemia plus low iron stores.
Analyses
Descriptive statistics are presented as percentages for categorical variables and as means or geometric means, with 95% CIs. Serum ferritin was not normally distributed and thus was presented as a geometric mean and log transformed for all parametric analyses. We checked for outliers (±5 SD) and excluded one improbable hemoglobin value of 43.9 g/dL in women. We used t tests to examine mean differences in continuous variables, whereas for independent proportions, we used χ2 and z test to test for differences in categorical variables across surveys. In addition, analyses of covariance were used to examine differences in means across surveys for hemoglobin and ferritin after adjustment for age, sex (children), area of residence, and age. Kernel density estimations were used to display distributional shifts for hemoglobin and ferritin across surveys (18, 19).
Dietary recall data (24 h) for preschool children in the 2008–2009 sentinel survey were analyzed to assess the percentage of estimated average requirements (EARs) met from fortification, following methods used by Imhoff-Kunsch and colleagues (20). The iron provided by foods containing wheat and maize flour and milk (liquid/powdered) was obtained by multiplying the amount of food consumed in grams or milliliters by the corresponding iron fortification content. Contribution of fortified foods to a child’s EAR is presented as a percentage of the daily requirement (medians and 25th and 75th percentiles). The reference EAR values for iron were 3.0 and 4.1 mg/d for children aged 1–3 y and 4–7 y, respectively, on the assumption that availability is 18% as in the U.S. diet (21). We assumed a bioavailability of 10%, more appropriate for the higher-fiber diet of countries such as Costa Rica (22). Thus, after multiplying by 1.8 (18/10), the adjusted EAR values are 5.4 and 7.4 mg/d for younger and older children, respectively.
The national surveys used multistage, probabilistic sampling, but sample weights were not generated in 1996 because of uncertainties about the size of the primary sampling units. Sample weights were available for 2008. We carried out the analyses without using sample weights for 1996 and 2008 to have a similar methodologic approach across surveys. Although the variance estimation may be inaccurate, the very large size of the differences found (see Results) makes this potential problem less of an issue. For 2008, we did run weighted and unweighted analyses, and use of sample weights gave identical results to those obtained without them (results not shown). All statistical analyses were conducted with R 3.0.3 (R Core Team) and SAS 9.3 (SAS Institute).
RESULTS
Descriptive statistics are shown in Tables 2 and 3. On average, children were aged 4 y and women aged 31 y in all surveys. In 1996, the country was divided into nearly equal thirds of urban, rural, and metropolitan areas, but in 2008, the country became more urban and less metropolitan.
Hemoglobin and serum ferritin improved, whereas anemia and iron deficiency were reduced in children at national and sentinel site levels (Table 2, Supplemental Figure 1); notably, iron deficiency anemia was not detected at the endline. From a baseline mean of 12.1 g/dL in children, hemoglobin improved by 0.7 g/dL at the national level and by 0.5 g/dL in the sentinel sites (Table 2). Hemoglobin increased and anemia decreased in women (Table 3, Supplemental Figure 2). In women, the hemoglobin starting point was 12.9 g/dL, and means improved by 0.4 and 0.5 g/dL at national and sentinel site levels, respectively (Table 3). The shift to the right in hemoglobin values of women and children occurred along the entire distribution, as indicated by the test for equal densities (Supplemental Figures 3 and 4). Identical results to those in Tables 2 and 3 were obtained in models that added age, sex (children), and area of residence dummy indicator variables as covariates (results not shown). Nationally, anemia (Table 4) and iron deficiency (Supplemental Table 1) in children declined in both sexes, in urban and rural areas, and in those older and younger than 3 y. In women, anemia declined in all areas (Table 5). Declines in anemia in the sentinel sites were consistent with national declines (Tables 4 and 5, Supplemental Table 1).
TABLE 4.
Prevalence of anemia in preschool children (aged 1–7 y) by sex, area of residence, and age1
| Descriptors | National surveys
|
Sentinel sites
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1996 (n = 965)
|
2008–2009 (n = 403)
|
Difference, P value2 | 1999–2000 (n = 404)
|
2008–2009 (n = 195)
|
Difference, P value2 | |||||
| n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | |||
| Sex | ||||||||||
| Male | 462 | 19.9 (16.3, 23.6) | 228 | 4.4 (1.7, 7.1) | <0.001 | 198 | 23.2 (17.3, 29.1) | 93 | 10.8 (4.4, 17.1) | <0.001 |
| Female | 503 | 18.7 (15.3, 22.1) | 175 | 3.4 (0.7, 6.1) | <0.001 | 206 | 17.0 (11.8, 22.1) | 102 | 8.8 (3.3, 14.4) | 0.049 |
| Area of residence | ||||||||||
| Urban | 341 | 24.1 (19.6, 28.7) | 174 | 4.6 (1.5, 7.7) | <0.001 | 197 | 16.2 (11.1, 21.4) | 98 | 3.1 (20.4, 6.5) | <0.001 |
| Rural | 318 | 21.7 (17.1, 26.2) | 130 | 1.5 (−0.6, 3.7) | <0.001 | 207 | 23.7 (17.9, 29.5) | 97 | 16.5 (9.1, 23.9) | 0.050 |
| Metropolitan | 306 | 11.4 (7.9, 15.0) | 99 | 6.1 (1.3, 10.8) | <0.003 | — | — | |||
| Child age, y | ||||||||||
| 1–3 | 265 | 30.0 (24.3, 35.6) | 111 | 4.6 (0.6, 8.5) | <0.001 | 122 | 36.1 (27.5, 44.6) | 65 | 16.9 (7.7, 26.1) | <0.001 |
| >3–7 | 700 | 15.4 (12.7, 18.1) | 292 | 3.7 (1.6, 5.9) | <0.001 | 282 | 13.1 (9.2, 17.1) | 130 | 6.2 (2.0, 10.3) | 0.011 |
| Total | 19.3 (16.8, 21.8) | 4.0 (2.1, 5.9) | <0.001 | 20.0 (13.9, 16.1) | 9.7 (5.6, 13.9) | 0.008 | ||||
Anemia was adjusted for altitude and defined as hemoglobin <11 g/dL for children aged <5 y and <11.5 g/dL for children aged 5–7 y.
P values were obtained from z tests for 2 independent proportions of anemia.
TABLE 5.
Anemia prevalence by area of residence for women of reproductive age (15–45 y)1
| Descriptors | National surveys
|
Sentinel sites
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1996 (n = 910)
|
2008–2009 (n = 863)
|
Difference, P value2 | 1999–2000 (n = 405)
|
2008–2009 (n = 474)
|
Difference, P value2 | |||||
| n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | n | Mean (95% CI) | |||
| Area of residence | ||||||||||
| Urban | 305 | 19.9 (15.4, 24.3) | 299 | 10.1 (7.0, 13.1) | <0.001 | 198 | 20.3 (14.8, 25.8) | 199 | 6.2 (3.3, 9.0) | <0.001 |
| Rural | 293 | 18.4 (14.0, 22.7) | 187 | 9.7 (6.3, 13.1) | <0.001 | 207 | 15.7 (10.6, 20.7) | 275 | 12.1 (7.5, 16.6) | 0.123 |
| Metropolitan | 312 | 16.7 (12.4, 21.0) | 377 | 11.2 (6.7, 15.8) | <0.001 | — | — | |||
| Total | 18.4 (15.8, 20.9) | 10.2 (8.2, 12.2) | <0.001 | 18.0 (14.3, 21.8) | 8.7 (6.1, 11.2) | <0.001 | ||||
Anemia was adjusted for altitude and defined as hemoglobin <11 g/dL for children aged <5 y and <11.5 g/dL for children aged 5–7 y.
P values were obtained from z tests for 2 independent proportions of anemia.
Dietary data from the sentinel site sites in 2008–2009 for children were used to estimate consumption of wheat and maize flour equivalents and milk, amount of iron from fortification provided by these foods, and percentage of the EAR (Table 6). Maize flour contributed little to iron intakes; the contribution from wheat flour and milk was important and about equal. More iron was consumed in the urban site, due to greater consumption of wheat flour. Combining both sentinel sites, children obtained 3.3 mg of iron from fortification. Overall, fortification provided the equivalent of about half the EAR, with the interquartile range being 29–80%. The percentage contribution to the EAR in children aged <3 y was 54%, slightly higher than for children aged 3–7 y (47%).
TABLE 6.
Estimated daily iron contribution added from fortification for children aged 1–7 y in the 2008–2009 sentinel site survey1
| Food | Consumption, g or mL/d | Iron, mg/d | Percentage of EAR |
|---|---|---|---|
| Urban community (n = 117) | |||
| Wheat flour | 56.2 (31.1–93.8) | 1.9 (1.0–3.1) | 26.7 (17.7–45.1) |
| Maize flour | 0.0 (0.0–7.5) | 0.0 (0.0–0.2) | 0.0 (0.0–2.8) |
| Milk | |||
| Powdered | 0.0 (0.0–11.6) | 1.5 (0.6–2.7) | 21.4 (8.4–39.2) |
| Liquid | 104.2 (14.7–312.5) | ||
| All fortified foods | 3.9 (2.5–5.9) | 56.6 (35.8–88.4) | |
| Rural community (n = 106) | |||
| Wheat flour | 25.0 (10.3–40.9) | 0.8 (0.3–1.4) | 12.5 (4.4–19.4) |
| Maize flour | 0.0 (0.0–24.4) | 0.0 (0.0–0.4) | 0.0 (0.0–5.6) |
| Milk | |||
| Powdered | 14.4 (0.0–43.8) | 1.3 (0.5–3.0) | 18.4 (7.5–41.7) |
| Liquid | 0.0 (0.0–53.6) | ||
| All fortified foods | 2.8 (1.6–4.5) | 38.1 (22.4–67.7) | |
| Children aged <3 y (n = 77) | |||
| Wheat flour | 30.0 (19.5–52.8) | 1.0 (0.6–1.5) | 18.2 (10.6–27.4) |
| Maize flour | 0.0 (0.0–6.3) | 0.0 (0.0–0.1) | 0.0 (0.0–2.0) |
| Milk | |||
| Powdered | 0.0 (0.0–38.0) | 1.3 (0.4–3.5) | 24.4 (8.1–65.6) |
| Liquid | 14.7 (0.0–112.5) | ||
| All fortified foods | 2.9 (1.3–5.2) | 54.3 (24.4–96.8) | |
| Children aged 3–7 y (n = 146) | |||
| Wheat flour | 45.5 (18.8–79.2) | 1.4 (0.6–2.8) | 18.6 (7.9–38.1) |
| Maize flour | 0.0 (0.0–22.1) | 0.0 (0.0–0.4) | 0.0 (0.0–6.0) |
| Milk | |||
| Powdered | 0.0 (0.0–28.2) | 1.4 (0.6–2.6) | 19.3 (7.8–35.3) |
| Liquid | 50.0 (0.0–225.0) | ||
| All fortified foods | 3.5 (2.1–5.1) | 46.6 (28.8–69.1) | |
| Pooled sample (n = 223) | |||
| Wheat flour | 38.8 (18.8–71.7) | 1.2 (0.6–2.3) | 18.5 (9.7–35.3) |
| Maize flour | 0.0 (0.0–15.0) | 0.0 (0.0–0.3) | 0.0 (0.0–4.4) |
| Milk | |||
| Powdered | 0.0 (0.0–32.5) | 1.4 (0.5–2.8) | 21.2 (8.1–41.4) |
| Liquid | 31.3 (0.0–175.0) | ||
| All fortified foods | 3.3 (1.9–5.2) | 48.6 (28.6–80.4) |
Values are medians; 25th–75th percentiles in parentheses. The EAR is 5.4 mg/d for children aged 1–3 y and 7.4 mg/d for children aged >3–7 y, respectively, assuming 10% bioavailability. EAR, estimated average requirement.
Periodic monitoring showed that the iron content of fortified foods met levels mandated by law (Supplemental Table 2). Special sampling from 2008 showed that the iron content in flour samples collected in bakeries was in compliance, with little variation by county (Figure 1) and by mill and brand (Supplemental Figures 5 and 6). The mean ± SD iron content in the flour samples was 67.5 ± 8.1 mg/kg, and the mean ± SD deviation from the mandated content of 55 mg/kg was 12.0 ± 8.1 mg/kg.
FIGURE 1.
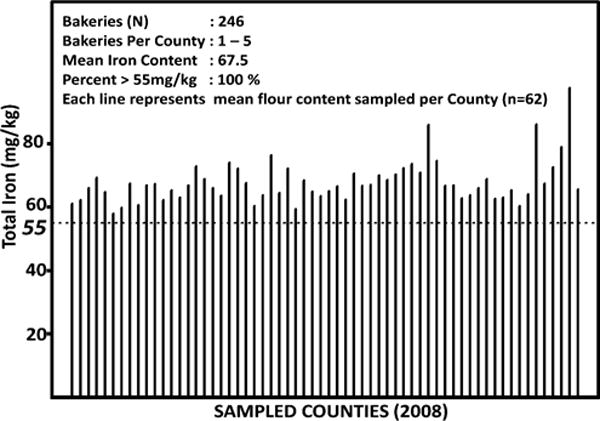
Total iron content of wheat flour sampled from bakeries across all counties in Costa Rica in 2008. Total iron content includes intrinsic iron as well as iron added as ferrous fumarate. The dotted line represents the mandated fortification content, 55 mg/kg.
DISCUSSION
We have documented a plausible impact pathway (Figure 2) that suggests that the fortification program in Costa Rica improved iron status and decreased anemia. The baseline data were collected in 1996 before the fortification program was strengthened and expanded; at that time, there was evidence of potential to benefit, as indicated by iron deficiency. Reduced iron, which has not been shown to be efficacious (7), was replaced by ferrous fumarate in wheat flour in 2002, and ferrous bisglycinate was added to maize flour in 1999 and to liquid and powdered milk in 2001. These iron compounds are fortificants with very good bioavailability and proven efficacy (7). The endline survey was conducted in 2008–2009, confidently after the program was fully matured and established. Monitoring data of the fortification program consistently showed that there was compliance with the legislation. Dietary intake data from children showed that the fortification program provided the equivalent of about half the EAR for iron, assuming 10% bioavailability. Finally, the prevalence of anemia in children and women dropped significantly nationally. Iron status improved in children but was not measured in women. At the national level, anemia in children aged <7 y was reduced from 19% to 4%, whereas in women, the decline was from 18% to 10%. In children, iron deficiency was reduced from 27% to 7%, and iron deficiency anemia was not detected at the endline.
FIGURE 2.
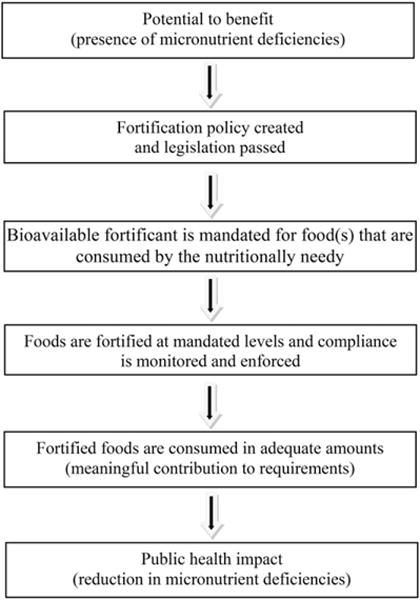
Program impact pathway for mass fortification programs.
The most likely nutrient driving the improvement in anemia is iron because of the substantial drop in iron deficiency. However, other nutrients that also improve hemoglobin (23) were provided through fortification and could have contributed to the reduction in anemia; these include vitamin A to milk and sugar; folic acid to wheat and maize flour, milk, and rice; and vitamin B-12 to rice. Helminthic infections were low, with ~2.5% of children aged 1– 7 y infected in 2008 (24), and can be dismissed as a significant cause of anemia.
It is sometimes said that young children are unlikely to benefit as much as adults from fortification because they consume smaller amounts of staple foods. However, children aged 1–3 y in Costa Rica consumed almost as much iron from fortification as did children aged 3–7 y, 2.9 and 3.5 mg/d, respectively (Table 6). Had only wheat flour been fortified with iron, only approximately one-half to one-third of these amounts would have been consumed, an indication of the value of milk as a vehicle for young children, particularly where milk is distributed to poor households as in Costa Rica. In the rural sentinel site, where the logistics of providing liquid milk are difficult, powdered milk was mostly consumed. We are uncertain as to the exact percentage of the EAR met by fortification. The EAR recommendations come from the United States, where it is assumed that 18% of the iron in the mixed diet is absorbed (21). Bioavailability is assumed to be poor (5%) where diets are primarily cereal and plant based, intermediate (10%) where some refined products and animal protein are consumed, and good (15%) in more developed countries where the diet is very low in fiber and high in animal products (22). We considered that 10% bioavailability was appropriate for Costa Rica, but perhaps this could be higher because of the use of ferrous bisglycinate, an iron–amino acid chelate with good bioavailability (25). We estimate that 54% of the EAR in children aged 1–3 y was provided by fortification compared with 47% in children older than 3–7 y (Table 6). In both age groups, these levels seem large enough relative to the probable nutrient gap to have an impact. Anemia declined nationally from 30.0% to 4.6% in children aged 1–3 y and from 15.4% to 3.7% in children aged 3–7 y (Table 4).
Fortification, particularly wheat flour fortification, has been described as an intervention more likely to benefit the better off, who have access to and can afford fortified foods (8). In Guatemala, the poorest, rural, indigenous populations with the highest burden of nutritional deficiencies likely benefit the least from wheat flour fortification because they are maize consumers (20). The solution lies in fortifying a food or a basket of foods that are consumed by the needy. Wheat flour consumption in children aged 1–7 y was twice as large in the urban compared with the rural sentinel site (Table 6); nonetheless, children aged 1–7 y obtained 2.8 mg daily iron from fortification in the rural sentinel site compared with 3.9 mg in the urban site. This was possible because milk provided similar amounts of iron in both sites. The fortification of rice, albeit not with iron, is a step in the right direction because it is widely consumed by all social groups and in greater amounts than wheat and maize flour. Estimates from per capita household consumption for 2001 in Costa Rica are 130 g rice, 74 g wheat flour, and 18 g maize flour (26). Fortification of rice with iron is feasible but faces some barriers: high initial investment, lack of government initiative, and consumer hesitation to accept variations in appearance (27). Micronized ferric pyrophosphate may be used as the source of iron, but it has not been tried in Costa Rica yet.
The key strength of our study is that we had the data to demonstrate a plausible pathway linking the fortification program to improvements in iron status and reductions in anemia (Figure 2). These findings suggest causal effects. However, the key weakness of our study is the nature of our design, a pre/post comparison. We are unable to exclude the possibility that factors other than fortification that also changed from baseline to endline could be responsible for the decline in anemia. The 2008–2009 evaluation occurred ~6 y after full implementation of the fortification program. Efficacy studies show that responses to iron-fortified products can occur in a matter of months (4–6), but programs require longer to get established. Our findings would be more persuasive if the endline had been carried out 1–2 y after strengthening of the program was completed in 2002—namely, in 2003–2004.
We think it is unlikely that other factors caused the declines in anemia. There were modest improvements in sociodemographic factors and in nutrition in Costa Rica between 1996 and 2008 (Supplemental Table 3). For example, the percentage of the population in extreme poverty dropped from 6.9% to 3.5%. The percentage of the population with improved drinking water sources went from 94% to 96% and that with improved sanitation facilities from 90% to 94%. Expenditures on health remained similar from 1996 to 2008.
World experience with anemia is that declines occur slowly without specific nutrition interventions (1). Over the period of study, Costa Rica has had a program on iron/folate supplementation during pregnancy but no other interventions that deliver iron besides food fortification. A national survey was conducted in Costa Rica in 1982; unfortunately, the data were lost, but descriptive statistics indicate little change in anemia prevalence between 1982 and 1996. Anemia in nonpregnant women was 20.0% in 1982 (28) compared with our reported values of 18.4% for 1996 and 10.2% for 2008. These data suggest that anemia started to decline only after changes were made to the fortification program in 1999–2002. On the other hand, the prevalence of stunting (< −2 z of the WHO standards) (29), the lowest in Central America, has changed little in recent decades (30). Analyses using the WHO standards indicate that stunting was 28.9% in 1966 (30), 8.5% in 1982 (30), 7.6% in 1996 (30), and 5.6% in 2008 (31).
Our study has limitations. Ferritin was not available for women at baseline. There were no data on changes in other iron status indicators (transferrin receptor and zinc protoporphyrin), markers of inflammation (C-reactive protein and α1-acid glycoprotein), and other micronutrient indicators (zinc, vitamin A, folic acid, and vitamin B-12) to characterize fully the impact of the fortification program and to adjust for inflammation at both endpoints. We lack dietary information for women to estimate the percentage of iron requirement met. These weaknesses, but primarily our pre/post design, suggest caution in interpreting our results as causal. However, the most plausible explanation for the decline in anemia in Costa Rica is the fortification program. We believe our results support the implementation of mass fortification programs to address identified micronutrient deficiencies. Such programs should be designed to be effective, supplying sufficient iron with adequate bioavailability, and be capable of reaching the needy, including young children; this may require use of several vehicles. Our findings suggest that where micronutrient deficiencies exist and where fortification programs are designed, implemented, and monitored adequately, impact will be achieved. As many have noted (4, 7, 8), there is an urgent need for food fortification effectiveness evaluations.
Acknowledgments
We thank Lawrence Grummer-Strawn, Lynette Neufeld, and Helena Pachón for valuable comments on an early draft; Humberto Méndez for responding to data queries; and Sandra Smith for manuscript preparation.
Footnotes
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of USAID or the U.S. government or the official position of the CDC.
Supported by The Micronutrient Initiative, Ottawa, Canada. This is a free access article, distributed under terms (http://www.nutrition.org/publications/guidelines-and-policies/license/) that permit unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Supplemental Figures 1–6 and Tables 1–3 are available from the “Supplemental data” link in the online posting of the article and from the same link in the online table of contents at http://ajcn.nutrition.org.
The authors’ responsibilities were as follows—RM: obtained funding, had full access to the data, wrote the first draft of the manuscript, and had final responsibility for the decision to submit for publication; MA, LT, and TA: were involved in implementing and monitoring the food fortification program in Costa Rica and provided data, government manuals, and reports; RM and MFY: reviewed the literature; RM, MFY, OYA, OD, and RF-A: designed the analyses; OYA: conducted the analyses; and OD: collated food fortification monitoring data. All authors contributed to later versions of the manuscript and read and approved the final version. None of the authors reported a conflict of interest related to the study. The sponsor of the study had no role in study design, data collection, data interpretation, or writing of the manuscript.
References
- 1.Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, Peña-Rosas JP, Bhutta ZA, Ezzati M, on behalf of Nutrition Impact Model Study Group (Anaemia) Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Global Health. 2013;1:e16–25. doi: 10.1016/S2214-109X(13)70001-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R, Uauy R, the Maternal and Child Nutrition Study Group Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382:427–51. doi: 10.1016/S0140-6736(13)60937-X. [DOI] [PubMed] [Google Scholar]
- 3.Horton S, Alderman H, Rivera J, Hunger and malnutrition . Copenhagen consensus 2008: Malnutrition and Hunger. In: Lomborg B, editor. Global crises, global solutions. Cambridge (United Kingdom): Cambridge University Press; 2009. pp. 305–33. [Google Scholar]
- 4.Das JK, Salam RA, Kumar R, Bhutta ZA. Micronutrient fortification of food and its impact on woman and child health: a systematic review. Syst Rev. 2013;2:67. doi: 10.1186/2046-4053-2-67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eichler K, Wieser S, Rüthemann I, Brügger U. Effects of micronutrient fortified milk and cereal food for infants and children: a systematic review. BMC Public Health. 2012;12:506. doi: 10.1186/1471-2458-12-506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gera T, Sachdev HS, Boy E. Effect of iron-fortified foods on hematologic and biological outcomes: systematic review of randomized controlled trials. Am J Clin Nutr. 2012;96:309–24. doi: 10.3945/ajcn.111.031500. [DOI] [PubMed] [Google Scholar]
- 7.Hurrell R, Ranum P, de Pee S, Biebinger R, Hulthen L, Johnson Q, Lynch S. Revised recommendations for iron fortification of wheat flour and an evaluation of the expected impact of current national wheat flour fortification programs. Food Nutr Bull. 2010;31:S7–21. doi: 10.1177/15648265100311S102. [DOI] [PubMed] [Google Scholar]
- 8.Victora CG, Barros FC, Assunção MC, Restrepo-Méndez MC, Matijasevich A, Martorell R. Scaling up maternal nutrition programs to improve birth outcomes: a review of implementation issues. Food Nutr Bull. 2012;33(2 Suppl):S6–26. doi: 10.1177/15648265120332S102. [DOI] [PubMed] [Google Scholar]
- 9.Rivera JA, Shamah T, Villalpando S, Monterrubio E. Effectiveness of a large-scale iron-fortified milk distribution program on anemia and iron deficiency in low-income young children in Mexico. Am J Clin Nutr. 2010;91:431–9. doi: 10.3945/ajcn.2009.28104. [DOI] [PubMed] [Google Scholar]
- 10.Assunção MC, Santos IS, Barros AJ, Gigante DP, Victora CG. Flour fortification with iron has no impact on anaemia in urban Brazilian children. Public Health Nutr. 2012;15:1796–801. doi: 10.1017/S1368980012003047. [DOI] [PubMed] [Google Scholar]
- 11.Shadish WR, Cook TD, Campbell DT. The one-group pretest-posttest design: experimental and quasi-experimental designs for generalized causal inference. New York: Houghton Mifflin; 2002. [Google Scholar]
- 12.Ministerio de Salud Instituto Costarricense de Investigación y Enseñanza en Nutrición y Salud. Encuesta Nacional de Nutrición, 1996 [Internet] Fascículo 2. Micronutrientes; San José (Costa Rica): 1997. [cited 2014 Oct 27]. Available from: http://www.ministeriodesalud.go.cr/index.php/centro-de-informacion/material-publicado/descargas/doc_download/25-en-cuesta-nacional-de-nutricion-fasciculo-micronutrientes. [Google Scholar]
- 13.Ministerio de Salud Instituto Costarricense de Investigación y Enseñanza en Nutrición y Salud, Caja Costarricense de Seguro Social, Instituto Nacional de Estadística y Censos, INCAP/OPS [Internet] Encuesta Nacional de Nutrición 2008. Manual Operativo; San José (Costa Rica): 2008. [cited 2014 Oct 27]. Available from: http://www.ministeriodesalud.go.cr/index.php/centro-de-informacion/material-publicado/descargas/doc_download/626-encuesta-nacional-de-nutricion-2008-manual-operativo. [Google Scholar]
- 14.Ministerio de Salud. Instituto Costarricense de Investigación y Enseñanza en Nutrición y Salud, Caja Costarricense de Seguro Social, Ministerio de Educación Pública. Desarrollo de Comunidades Centinelas sobre alimentacion y nutricion [Internet]. Apendice No. 2. Módulo de Micronutrients; San José (Costa Rica): 2000. [cited 2014 Oct 27 ]. Available from: http://www.ministeriodesalud.go.cr/index.php/centro-de-informacion/material-publicado/descargas/doc_download/387-desarrollo-de-comunidades-centinela-sobre-alimentacion-y-nutricion-micronutrientes-. [Google Scholar]
- 15.Azim W, Parveen S. Comparison of photometric cyanmethemoglobin and automated methods for hemoglobin estimation. J Ayub Med Coll Abbottabad. 2002;14:22–3. [PubMed] [Google Scholar]
- 16.Siemens Medical Solutions Diagnostics. Immulite/Immulite 1000 Ferritin. PILKFE-8 [Internet] 2006 [cited 2014 Oct 27]. Available from: http://www.healthcare.siemens.co.kr/immunoassay/systems/immulite-1000-immunoassay-system/assays.
- 17.World Health Organization. Iron deficiency anaemia: assessment, prevention, and control: a guide for programme managers [Internet] Geneva (Switzerland): World Health Organization; 2001. [cited 2014 Oct 27]. WHO/NHD/01.3. Available from: http://apps.who.int/iris/bitstream/10665/66914/1/WHO_NHD_01.3.pdf?ua=1. [Google Scholar]
- 18.Bowman AW, Azzalini A. R package ‘sm’: nonparametric smoothing methods (version 2.2-5) Vienna (Austria): 2013. [Google Scholar]
- 19.Bowman AW, Azzalini A. Applied smoothing techniques for data analysis: the kernel approach with S-plus illustrations. Oxford (United Kingdom): Oxford University Press; 1997. [Google Scholar]
- 20.Imhoff-Kunsch B, Flores R, Dary O, Martorell R. Wheat flour fortification is unlikely to benefit the neediest in Guatemala. J Nutr. 2007;137:1017–22. doi: 10.1093/jn/137.4.1017. [DOI] [PubMed] [Google Scholar]
- 21.Institute of Medicine. Dietary Reference Intakes: for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium and zinc. Washington (DC): National Academy of Sciences; 2001. [PubMed] [Google Scholar]
- 22.Allen L, de Benoist B, Dary O, Hurrell R, WHO guidelines on food fortification with micronutrients, editors. Department of Nutrition for Health and Development. Geneva (Switzerland): World Health Organization; 2006. [Google Scholar]
- 23.World Health Organization. Focusing on anaemia: towards an integrated approach for effective anaemia control [Internet] Joint statement by the World Health Organization and the United Nations Children’s Fund. [cited 2014 Oct 27]. Available from: http://whqlibdoc.who.int/hq/2004/anaemiastatement.pdf.
- 24.Ministerio de Salud. Instituto Costarricense de Investigación y Enseñanza en Nutrición y Salud, Caja Costarricense de Seguro Social, Instituto Costarricense de Estadísta y Censos, Instituto Costarricense sobre Drogras, Instituto Nacional de Estadística y Censos. Encuesta Nacional de Nutrición 2008–2009 [Internet]. Fascículo 5: Parásitos Intestinales. San José (Costa Rica): 2010. [cited 2014 Oct 27]. Available from: http://www.ministeriodesalud.go.cr/index.php/centro-de-informacion/material-publicado/descargas/doc_download/1048-encuesta-nacional-de-nutricion-2008-2009parasitos-intestinales. [Google Scholar]
- 25.van Stuijvenberg ME, Smuts CM, Wolmarans P, Lombard CJ, Dhansay MA. The efficacy of ferrous bisglycinate and electrolytic iron as fortificants in bread in iron-deficient school children. Br J Nutr. 2006;95:532–8. doi: 10.1079/bjn20051669. [DOI] [PubMed] [Google Scholar]
- 26.Comisión Intersectorial de Guías Alimentarias para Costa Rica. Actualización de lineamientos técnicos para la elaboración de las Guías Alimentarias de la población costarricense [Internet] San José (Costa Rica): 2007. [cited 2014 Oct 27]. Available from: http://www.ministeriodesalud.go.cr/gestores_en_salud/guiasalimentarias/actualizacion%20lineamientos.pdf. [Google Scholar]
- 27.Piccoli NB, Grede N, de Pee S, Singhkumarwong A, Roks E, Moench-Pfanner R, Bloem MW. Rice fortification: its potential for improving micronutrient intake and steps required for implementation at scale. Food Nutr Bull. 2012;33(4 Suppl):S360–72. doi: 10.1177/15648265120334S312. [DOI] [PubMed] [Google Scholar]
- 28.Ministerio de Salud. Instituto Costarricense de Investigación y Enseñanza en Nutrición y Salud, Caja Costarricense de Seguro Social, Instituto Costarricense de Estadísta y Censos, Instituto Costarricense sobre Drogras. Encuesta Nacional de Nutrición 2008–2009 [Internet]. Fascículo 2: Micronutrientes. San José (Costa Rica): 2012. [cited 2014 Oct 27]. Available from: http://www.ministeriodesalud.go.cr/index.php/centro-de-informacion/material-publicado/descargas/doc_download/1030-encuesta-nacional-de-nutricion-2008-2009-micronutrientes. [Google Scholar]
- 29.WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. 2006;450S:S76–85. [Google Scholar]
- 30.Palmieri MS, Méndez HC, Delgado HV, Flores RA, Palma de Fulladolsa P. Monografía, Programa Regional de Seguridad Alimentaria y Nutricional para Centroamérica. Managua (Nicaragua): PRESANCA; 2009. Ha crecido Centroamérica? Análisis de la situación antropométrica-nutricional en niños menores de 5 años de edad en Centroamérica y República Dominicana para el periodo 1965–2006. [Google Scholar]
- 31.Ministerio de Salud, Instituto Costarricense de Investigación y Enseñanza en Nutrición y Salud, Caja Costarricense de Seguro Social, Instituto Costarricense de Estadísta y Censos, Instituto Costarricense sobre Drogras, Instituto Nacional de Estadística y Censos. Encuesta Nacional de Nutricion 2008–2009 [Internet] Antropometría; San José (Costa Rica): 2010. Available from: http://www.ministeriodesalud.go.cr/index.php/centro-de-informacion/material-publicado/descargas/doc_download/1028-encuesta-nacional-de-nutricion-2008-2009-antropometria. [Google Scholar]