

Abstract
Objective
To investigate the prevalence and pattern of calcification of the stylohyoid complex in Libyan population.
Material and methods
Archived digital panoramic radiographs of 3343 patients were collected; 181 images were excluded for underage or poor image quality. Thus, the images of 3162 patients (1081 men, 2081 women; women-to-men ratio, 2:1; age range, 16–68 years; mean age, 36.7 years) retrieved and assigned to one of four morphological patterns of the stylohyoid complex: regular, elongated, calcified, and undetected. Data were analyzed with the Χ2 test using SPSS (Chicago, IL, USA); P values lower than 0.05 were considered statistically significant.
Results
Out of 3162 images studied, the styloid process was demonstrated to be regular in 1935 (61.2%), elongated in 541 (17.2%), calcified in 565 (17.8%), and undetected in 121 (3.8%). Symmetric patterns were demonstrated on 2580 (81.6%) images. An elongated stylohyoid complex was significantly more common in women than in men (P = .0404).
Conclusion
The anatomical patterns of the stylohyoid complex in Libyans were highly variable. Dental clinicians should recognize the various morphological patterns of the stylohyoid complex on panoramic radiographs. Computed tomography studies are recommended for further morphometric analysis of the stylohyoid complex.
Keywords: Calcification, Radiography, Panoramic, Stylohyoid
1. Introduction
The stylohyoid complex (chain) consists of the styloid process, stylohyoid ligament and the lesser cornu (horn) of the hyoid bone. It is derived from the second pharyngeal arch (Reichart’s cartilage). The stylohyoid process projects downward, forward, and slightly medially so that its tip is positioned between the internal carotid artery, internal jugular vein, and cranial nerves V, IX, and Langlais et al. reported that the styloid process varies in length between patients and often between the two sides of the same individual (Langlais et al., 1995). They suggested that an elongated styloid process results from ossification in the stylohyoid ligament.
Calcification of the stylohyoid complex is usually detected as an incidental finding on panoramic radiographs (Monsour et al., 1986). However, this finding may also be associated with a group of clinical symptoms that require surgical intervention (Eagle, 1948). O’Carroll reported that 8 of 103 (8%) patients with an elongated styloid process presented with related symptoms of deep neck pain, foreign body sensation in the throat, pain on turning the head, and odynophagia (O’Carroll, 1984).
Langlais et al. proposed a radiographic classification for the calcified stylohyoid complex, including three patterns of radiographic presentation (elongated, pseudoarticuated, segmented) and four patterns of calcification (calcified outline, partially calcified, nodular complex, completely calcified) (Langlais et al., 1986). However, only a few studies have presented the calcification of the stylohyoid complex in a manner that would be useful for clinicians. Therefore, the aim of this study was to investigate the prevalence and pattern of calcification of the stylohyoid complex in a Libyan population.
2. Material and methods
Records of digital panoramic radiographs treated at the University of Benghazi College of Dentistry between January 2010 and December 2013, were retrieved and evaluated for the prevalence and pattern of calcification of the stylohyoid complex. Patients younger than 16 years of age were excluded from the analysis as these patients would not have reached skeletal maturity. Radiographs with positioning or exposure errors were also excluded from the study. The panoramic images were generally obtained as part of routine radiographic screening for oral diagnosis. Therefore, no specific history related to the stylohyoid complex, e.g., tonsillectomy or cervical trauma, was obtained, so that it was not possible to diagnose Eagle syndrome or stylohyoid syndrome. The images were taken using paX-i (Vatech, Seoul, Korea) set at 60–80 kVp, 8–10 mA, and 10.1 s.
The native population of Libya is mainly a mixture of Arab-Imazighen ethnicities, with large minorities descending from African and Turkish origin. However, it was not possible to determine the ethnic background of each patient.
The classification of the stylohyoid complex used in this study was modified from MacDonald-Jankowski’s study (MacDonald-Jankowski, 2001). He classified the stylohyoid complex according to the center of calcification as following: Region 1, tympanohyal; Region 2, stylohyal; Region 3, ceratohyal; Region 4, hypohyal.
The classification used in this study is as following: the styloid process was considered “regular” when it did not extend below the mandibular foramen (Patterns A to D); “elongated” when it extended below the mandibular foramen and appeared to be continuous with skull base (Pattern E); “calcified” when it extended below the mandibular foramen and did not appear to be continuous with the cranial base (Patterns F to K); “undetected” when it could not be seen on the panoramic image (Fig. 1, Fig. 2). All radiographs were de-identified and reviewed by a board-certified oral and maxillofacial radiologist under ambient room lighting using the standardized Apple software—iPhoto (Apple, Cupertino, CA, USA) on a 27-in. monitor (iMac, Apple) with a screen resolution of 2560 × 1440 pixels.
Fig. 1.
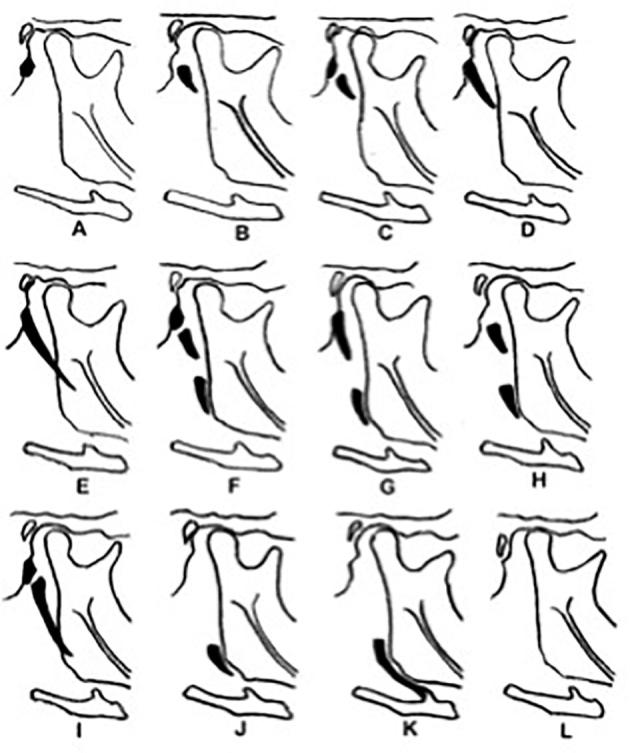
O’Carroll’s classification of the stylohyoid complex: Patterns A through D, regular; Pattern E, elongated; Patterns F through K, calcified; and Pattern L, absent.
Fig. 2.

Classification of the stylohyoid complex used in this study: a, regular; b, elongated; c, calcified; d, undetected.
3. Results
The digital panoramic radiographs of 3343 patients were collected; 181 images were excluded because the patient was younger than 16 or because the image quality was poor as the result of errors in positioning or exposure. Thus, the images of 3162 patients (1081 men, 2081 women; women-to-men ratio, 2:1; age range, 16–68 years; mean age, 36.7 years) were included in the study.
The detailed distribution of the 12 patterns of O’Carroll’s classification4 is shown in Table 1. The styloid process was classified as regular (Patterns A, B, C, and D) in 1935 images (61.2%), elongated (Pattern E) in 541 (17.2%), calcified (Patterns F, G, H, I, J, K) in 565 (17.8%), and undetected (Pattern L) in 121 (3.8%). However, 2580 (81.6%) of the regular, elongated, calcified, or undetected patterns were symmetrical on both sides. According to O’Carroll’s classification, Pattern D was the most common symmetrical pattern (964, 30.5%), whereas Pattern D-C was the most common asymmetrical pattern (180, 5.7%). The elongated stylohyoid complex pattern occurred significantly more frequently among women (P = .0404). However, there was no significant difference between men and women in the occurrence of the calcified stylohyoid complex (P = .0669).
Table 1.
Patterns of calcification of the stylohyoid complex in Libyans.
| Pattern | A |
B |
C |
D |
E |
F |
G |
H |
I |
J |
K |
L |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Side | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt | Rt | Lt |
| Number | 99 | 93 | 263 | 246 | 309 | 403 | 1297 | 1160 | 528 | 554 | 54 | 57 | 122 | 121 | 21 | 15 | 203 | 251 | 64 | 69 | 76 | 77 | 126 | 116 |
| Total | 192 | 509 | 712 | 2457 | 1082 | 111 | 243 | 36 | 454 | 133 | 153 | 242 | ||||||||||||
| Percentage | 3 | 8 | 11 | 39 | 17 | 2 | 4 | 0.5 | 7 | 2 | 2.5 | 4 | ||||||||||||
RT, right; LT, left.
4. Discussion
This study evaluated the calcification pattern of the stylohyoid complex on panoramic radiographs as this imaging modality is widely used by dental clinicians. To the best of the author’s knowledge, the size of the sample in this study is the largest ever included in studies of the stylohyoid complex. The frequency of a calcified stylohyoid complex in this analysis was relatively higher than that found in previous studies (MacDonald-Jankowski, 2001, Jung et al., 2004, Oztas and Orhan, 2012). A relatively recent study reported that only 6% of subjects with a calcified stylohyoid complex had related symptoms (Ilguy et al., 2005). Therefore, the calcification of the stylohyoid complex on panoramic radiographs should be based on clinical findings.
Various classification techniques have been used to evaluate the stylohyoid complex (MacDonald-Jankowski, 2001, Oztas and Orhan, 2012, Okabe et al., 2006, Kursuoglu et al., 2005). In the present study, the stylohyoid complex was simply classified according to 4 patterns (regular, elongated, calcified, and undetected). This classification system is of more clinical value than sorting the stylohyoid complex into one of 12 anatomic patterns, as in O’Carroll’s classification (Fig. 1). For instance, in the context of related symptoms, the clinician will essentially need to ascertain the pattern of the stylohyoid complex in terms of elongation and calcification. The current study used the term regular rather than normal, because it is unclear whether other patterns of the stylohyoid complex are in essence pathologic conditions; instead, they seem to be normal variants commonly observed on panoramic radiographs. However, the criteria of definitions used in this study corresponded to those used in MacDonald-Jankowski’s study (MacDonald-Jankowski, 2001). The elongated and calcified patterns of the stylohyoid complex occured at quite similar rates in this study (elongated, 17.2%; calcified, 17.8%). The frequency of the calcified pattern was similar to that reported among the Hong Kong Chinese (MacDonald-Jankowski, 2001). However, the frequencies at which other patterns occurred were generally different from those reported in studies investigated subjects of different ethnic backgrounds including Hong Kong Chinese, Londoners, and Turkish populations (MacDonald-Jankowski, 2001, Alpoz et al., 2014). However, O’Carroll reported no particular ethnic predilection in his study involving subjects from the United States (O’Carroll, 1984). Interestingly, the frequency of Pattern L (absent stylohyoid complex) was similar among Libyans, Hong Kong Chinese, Londoners, and Turkish populations (2.5–3.8%) (Monsour et al., 1986, MacDonald-Jankowski, 2001). However, it is unclear whether this type of stylohyoid complex was actually absent or was simply unseen because of technical reasons; hence, the current study used the term undetected rather than absent. However, a cadaveric study did not find a single case in which the styloid process was completely absent, although a vestigial process was identified (Frommer, 1974).
The elongated stylohyoid complex was significantly more common among females than among males. However, there was no significant difference between males and females in the frequency of the calcified stylohyoid complex. In agreement with other reports (Monsour et al., 1986, Omnell et al., 1998), MacDonald-Jankowski found no significant difference between males and females in the frequency of the elongated or the calcified stylohyoid complex (MacDonald-Jankowski, 2001). However, other studies reported a slight predilection among elderly females for the elongated styloid process (O’Carroll, 1984, Oztas and Orhan, 2012). However, this study did not include gender- or age-based evaluation of the styoyhyoid complex, as this approach appears to have little diagnostic value. A study that reviewed 1162 panoramic radiographs obtained from the population of the Aseer region of Saudi Arabia found that the prevalence of the elongated styloid process was as high as 93% (Shaik et al., 2013). A similar study from Northern India found that the prevalence of the elongated styloid process was (Bagga et al., 2012). However, the authors used a different classification technique from that in the present study. In some studies, when asymmetry was present, the side with the most advanced pattern was used to measure the stylohyoid complex (MacDonald-Jankowski, 2001, Oztas and Orhan, 2012). However, in the current analysis, the right and left sides were classified separately so that bias could be avoided. In accordance with other reports, this study has shown a high degree of symmetry in the patterns of stylohyoid complex (MacDonald-Jankowski, 2001, Okabe et al., 2006, Akar et al., 2016).
A calcified stylohyoid complex that appears as a radiopaque nodule on a panoramic radiograph may simulate a sialolith or a calcified carotid atheroma (Langlais et al., 1995). Therefore, dental professionals should carefully evaluate the location and morphology of soft tissue calcifications in the mandibular angle area. However, additional 3D imaging may be necessary for further evaluation. Clinical symptoms associated with Eagle syndrome are likely related to the elongation as well as the medial inclination of the stylohoid complex. Buyuk et al. found a significant correlation between the length of the stylohyoid complex and its sagittal angle by using cone beam computed tomographic imaging (Buyuk et al., 2017). However, the length and angulation of the stylohyoid complex were not measured in this study, as linear measurements on panoramic radiographs are not reliable.
In conclusion, this study has shown significant differences in the morphology of the stylohyoid complex between Libyans and other ethnic groups. It is of utmost importance for dental clinicians to cope with the various morphological patterns of the stylohyoid complex as demonstrated on panoramic radiographs. Computed tomography studies are necessary for further morphometric analysis of the stylohyoid complex. To the best of the author’s knowledge, this is the first study to investigate the prevalence and pattern of calcification of the stylohyoid complex in a Libyan population Because of its large sample size and its clinically oriented classification technique, this study presents important information for dental practitioners.
Conflict of interest
The author declared that there is no conflict of interest.
Footnotes
Peer review under responsibility of King Saud University.
References
- Akar G.C. Does the state of dentition affect the type of stylohyoid chain calcification pattern? Surg. Radiol. Anat. 2016;38:817–823. doi: 10.1007/s00276-016-1624-y. [DOI] [PubMed] [Google Scholar]
- Alpoz E. Prevalence and pattern of stylohyoid chain complex patterns detected by panoramic radiographs among Turkish population. Surg. Radiol. Anat. 2014;36:39–46. doi: 10.1007/s00276-013-1137-x. [DOI] [PubMed] [Google Scholar]
- Bagga M.B. Clinicoradiologic evaluation of styloid process calcification. Imag. Sci. Dent. 2012;42:155–161. doi: 10.5624/isd.2012.42.3.155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buyuk C. Morphological assessment of the stylohyoid complex variations with cone beam computed tomography in a Turkish population. Folia. Morphol. (Warsz) 2017 doi: 10.5603/FM.a2017.0061. [DOI] [PubMed] [Google Scholar]
- Eagle W.W. Elongated styloid process: further observations and a new syndrome. Arch. Otolaryngol. 1948;47:630–640. doi: 10.1001/archotol.1948.00690030654006. [DOI] [PubMed] [Google Scholar]
- Frommer J. Anatomic variations in the stylohyoid chain and their possible clinical significance. Oral Surg. Oral Med. Oral Pathol. 1974;8:659–667. doi: 10.1016/0030-4220(74)90382-x. [DOI] [PubMed] [Google Scholar]
- Ilguy M. Incidence of the type and calcification patterns in patients with elongated styloid process. J. Int. Med. Res. 2005;33:96–102. doi: 10.1177/147323000503300110. [DOI] [PubMed] [Google Scholar]
- Jung T. Elongated styloid process: when is it really elongated? Dentomaxillofac. Radiol. 2004;33:119–124. doi: 10.1259/dmfr/13491574. [DOI] [PubMed] [Google Scholar]
- Kursuoglu P. Radiological evaluation of the styloid process in young adults resident in Turkey’s Yeditepe University Faculty of Dentistry. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2005;100(4):491–494. doi: 10.1016/j.tripleo.2005.05.061. [DOI] [PubMed] [Google Scholar]
- Langlais R.P. Soft Tissue Radiopacities. In: Langlais R.P., editor. Diagnostic Imaging of the Jaws. Williams & Wilkins; Baltimore: 1995. pp. 617–648. [Google Scholar]
- Langlais R.P. Elongated and mineralized stylohyoid ligament complex: a proposed classification and report of a case of Eagle's syndrome. Oral Surg. Oral Med. Oral Pathol. 1986;61(5):527–532. doi: 10.1016/0030-4220(86)90400-7. [DOI] [PubMed] [Google Scholar]
- MacDonald-Jankowski D.S. Calcification of the stylohyoid complex in Londoners and Hong Kong Chinese. Dentomaxillofac. Radiol. 2001;30(1):35–39. doi: 10.1038/sj/dmfr/4600574. [DOI] [PubMed] [Google Scholar]
- Monsour P.A. Variability of the styloid process and stylohyoid ligament in panoramic radiographs. Oral Surg. Oral Med. Oral Pathol. 1986;61:522–526. doi: 10.1016/0030-4220(86)90399-3. [DOI] [PubMed] [Google Scholar]
- O’Carroll M.K. Calcification in the stylohyoid ligament. Oral Surg. Oral Med. Oral Pathol. 1984;58:617–621. doi: 10.1016/0030-4220(84)90089-6. [DOI] [PubMed] [Google Scholar]
- Okabe S. Clinical significance and variation of the advanced calcified stylohyoid complex detected by panoramic radiographs among 80-year-old subjects. Dentomaxillofac. Radiol. 2006;5:191–199. doi: 10.1259/dmfr/12056500. [DOI] [PubMed] [Google Scholar]
- Omnell K.A. Ossification of the human stylohyoid ligament. A longitudinal study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998;85:226–232. doi: 10.1016/s1079-2104(98)90431-0. [DOI] [PubMed] [Google Scholar]
- Oztas B., Orhan K. Investigation of the incidence of stylohyoid ligament calcifications with panoramic radiographs. J. Investig. Clin. Dent. 2012;3(1):30–35. doi: 10.1111/j.2041-1626.2011.00081.x. [DOI] [PubMed] [Google Scholar]
- Shaik M.A. Prevalence of elongated styloid process in Saudi population of Aseer region. Eur. J. Dent. 2013;7:449–454. doi: 10.4103/1305-7456.120687. [DOI] [PMC free article] [PubMed] [Google Scholar]