

Abstract
Objectives:
To evaluate the effectiveness of peer education on changing the smoking behavior of high schoolage children’s.
Methods:
In this interventional study; transtheoretical model, which is one of the cognitive-behavioral models was used for application of the peer education. Study was conducted in Izmir during 2011-2012 education period and included 338 students from 2 high schools The independent variable of the study is peer training. Descriptive variables for a student are age, gender, tendecy of friends to smoke inside and outside the school, the age they have first experienced the habit, reasons for nicotine consumption, levels of addiction, chatting about smoking and related harms. Family descriptive variables are education level of parents and whether their smoking tendency is present or not.
Results:
Approximately 18.3% of the students were current smoker. A positive behavioral change of smoking quitting among smoker students was observed after peer education. The number of students in precontemplation stage was reduced while the number of students in stages of preparation/determination action and maintenance was increased.
Conclusion:
Peer education was observed to be an effective method in the behavioral change of smoking teens. Authors strongly suggest peer education to be one of the preferred tools in changing the teen behavior in use of tobacco.
Smoking is a global problem and one of the leading causes of preventable mortalities. Approximately 6 million people die due to diseases caused by tobacco consumption every year, this number is increase to 10 million by 2030.1-4 In Turkey, the number of deaths caused by cigarette use is approximately 100 thousand per year and this number is expected to reach 240 thousand in 2030.5 Although global cigarette use has been declining. The percentage of cigarette users in Turkish youth still remains high. According to the Turkey Global Youth Tobacco Survey 2009, smoking rates of high school age children’s increased 8.4% in the last 6 years.1,3 Softa et al6 found that 26.5% of high school students in Kastamonu were using cigarettes.6 In a similar study in Romania, Trofor et al7 documented 52.4% of students smoked regularly. Influence of easy access to tobacco-produced items, peer pressure, tobacco commercials and price policies in cigarette, cigar and narghile on adolescents starting to smoke is important. There is a variety of different models of education and behavior to minimize tobacco consumption among young people and change their perception of behaviors concerning smoking.1,8-12 Cognitive-behavioristic models and theories including Health Belief Model, Planned Behavior Theory, Reasoned Action Theory and Transtheoretical model (TTM) are generally found effective in practices of education and regulation and achievement of preventive health behaviors for adolescent peers.13-17 Transtheoretical model is an intentional behavior change model that focuses on individual decisions. Prochaska15 define change as a gradual, continuous and dynamic structure, while change is a sharp and direct conclusion. Prochaska15 describe change as a gradual, continuous, and dynamic structure. Transtheoretical model has been used in smoking cessation programs. They claim that individuals do not go directly from old behavior (namely, smoking) with a new behaviors (quit smoking), progress gradually through the sequence of change. The individual sets out to resolve problem-interaction patterns and problem-solving strategies, using an organizational scheme of theoretical models, change phases, change processes, decision-making balance, and self-efficacy.13,15-17 In this study, we focused on peer influence as an agent in TTM based change. Influence of peers on youth is certainly of great importance. A peer role model is a friend whose behaviors and suggestions can convince others and that he or she is aware of the meaning and the difficulties of being a fellow peer.17,18 Education of peers aims at using positive peer influence on other fellow peers.3,18,19 Peer educators and trainers have to be chosen from among highly respected individuals who are capable of listening and communicating. They also should have practical and scholar leadership and role modelling skills, as well as being able to provide voluntary and energetic interference in positive and negative situations when needed and show non-judgemental or unprejudiced attitude towards their colleagues and clients.20 However, the process of peer education/training can be negatively affected when the above is not taken into account.21-23 The aim of this study is to assess the efficiency of peer education/training in changing the tobacco consumption behavior in high school students.
Methods
In this interventional study; transtheoretical model, which is one of the cognitive-behavioral models was used for application of the peer education. To ensure that answers were not seen by parents and school administrations; questionnaires were given in a closed envelopes to the students (338 students). The interventional study was conducted in 2 high school in Balçova District, Izmir. The data of the study was collected between September and October 2011. Four hundred forty-four students were targeted and 338 of this (76.1%) participated in the initial survey. In the study, 61 students were smokers (18.3%). Enable these students to achieve change in attitudes towards smoking cessation they underwent 6 months peer education. Changes in the behavior of smoking cessation after 6 months was evaluated according to the transtheoretical model stage.
Selecting peer volunteers
A situation-determining questionnaire performed in 2 schools was included in the study in which students were asked such questions as “Would you like to work with us actively in processes to be performed at school?” and “Which friend of yours would you want to contribute to in-school activities” to determine voluntary students. Forty-three volunteers were identified from 2 schools.
Exclusion criteria
None of the students who took the first survey were excluded from the study.
Training peer volunteers
Two training groups were formed in both schools. Students were told about the purposes of training programs, how to use tools and what is being expected from them. They were also asked why they volunteered in the groups and what their expectations were. Training programs were provided to voluntary peers who than started talks and chats in the canteen, garden, and classrooms of both schools about present and potential harms of tobacco consumption. The voluntary peers hung the billboards, brochures and posters where students could easily see them, shared their experiences with their classmates to try to learn what they thought; and they created an account group on facebook to enable them to share their own experiences, emotions, and approaches. The dependent variable of the study is behavioral change, which is assessed whether by any progressions or regressions based on TTM. Phases of behavioral changes progression to a higher level was assessed as progress. The independent variable of the study is peer training. Transtheoretical model stages are: 1) precontemplation, in which an individual may or may not be aware that a behavior change is warranted and has no intention of changing within the next 6 months; 2) contemplation, in which an individual is aware that a change is warranted and is intending to change within the next 6 months; 3) preparation, in which an individual is planning to change within the next 4 weeks; 4) action, which begins the day an individual makes the behavior change and lasts until they have maintained the change for 6 months; 5) maintenance, which begins after an individual has successfully maintained a behavior change for 6 months.24,25 Descriptive variables for a student are age, gender, smoking status, tendency of friends to smoke inside and outside the school, the age they have first smoking, level of nicotine dependence, chatting about smoking and related harms. Family descriptive variables are education level of parents, their employment and whether their smoking tendency is present or not. Smoking status was defined as being a current smoker, an ex-smoker and a never smoker. Current smokers were those reported cigarette smoking every day or some days at the last one month. Never smokers were those reported who never smoke during their lifetime. Ex-smokers were those reported cigarette smoking during their lifetime, but currently did not smoke at least one year. Smoking cigarette, cigars, pipes, and water pipe were asked to the participant for characterizing their smoking status. Nicotine dependency was revealed by the The Fagerstrom dependency test. The Fagerstrom Test for Nicotine Dependence (FTND) was developed in 1978 by Fagerstrom to examine nicotine dependency using self-assessment methods.26 Mermer et al26 developed the Turkish version of the scale. The FTND is composed of 6 questions. If the total test score is above 4, it indicates a probability of dependence. The 5 degrees of nicotine dependency according to the test scores include very low dependency (0-2), low dependency (3-4), medium dependency (5), high dependency (6-7), and very high dependency (8-10).26
Statistical analysis
Data of the study was analyzed by using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) Version 18.0 to evaluate the mean and standard deviation, and the frequency for descriptive findings. We used Chi-square test for establishing the influence of independent variables on smoking status. The FTND changes and behavioral changes was evaluated by Mc Nemar Chi-square test. Ethics Committee approval was obtained from the Ethics Committee of Dokuz Eylül University Non-Interventional Researches. This study was carried out in accordance with the principles of Helsinki Declaration.
Results
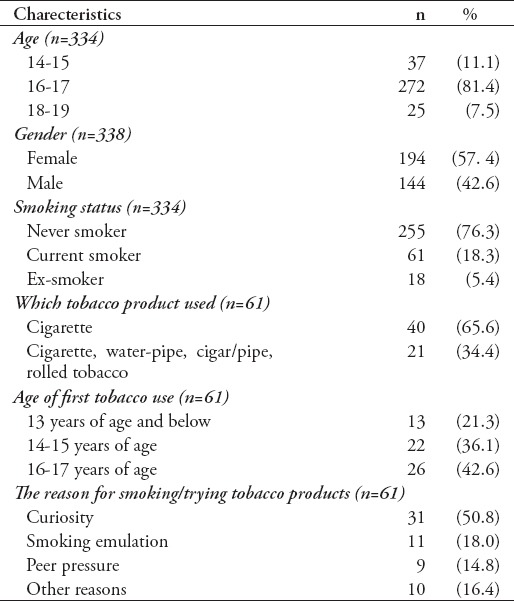
In this study, 81.4% of the participants were 16-17 years old, 57.4% were females and 18.3% were current smoker. Approximately 65.6% of the smokers were use cigarettes, 21.3% of smokers were 13 years of age and below and 50.8% had started smoking because of mere curiosity (Table 1).
Table 1.
Distribution of students’ demographic characteristics (N=338).
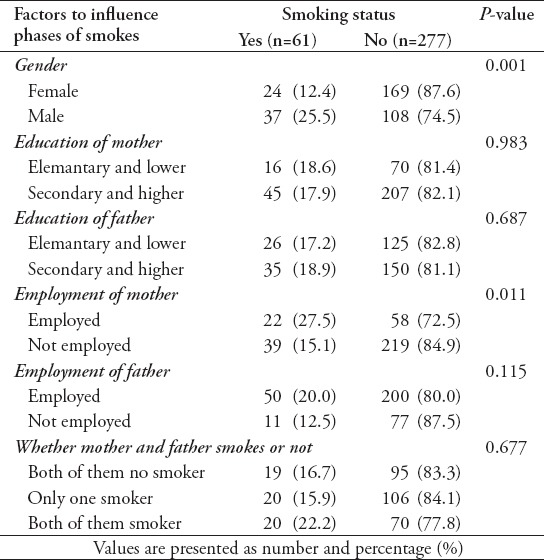
In this study, there is a significant relationship between gender and students ‘mothers’ work and smoking status. Male students smoke more than female students. Students who working mother smoked more cigarettes (Table 2).
Table 2.
Relationship between students smoking status and some factors.
In the study 24.6% of pre-peer smokers were in the precontemplation phase, and 31.1% were in the contemplation phase and 6.6% of smokers were in the maintenance phases, respectively (Table 3).
Table 3.
Distribution of students’ answers to the questions about of behavioral changes before and after 6 months peer education (N=61).
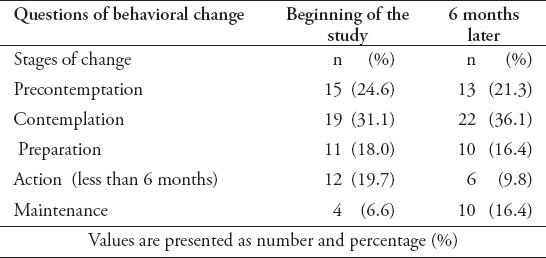
In the study 21.3% of after-peer smokers were in the precontemplation phase, and 36.1% were in the contemplation phase and 16.4% of smokers were in the maintenance phases, respectively (Table 3).
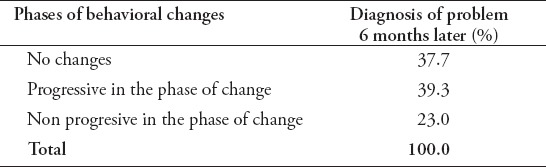
Students were found to show change of behavior to non-smoking at the rates of 39.3 (Table 4). There were no significance stage behavioral changes after sixth months.
Table 4.
Comparison of phases of behavioral changes during diagnosis of the problem, begining of the survey than 6 months later for students (N=61).
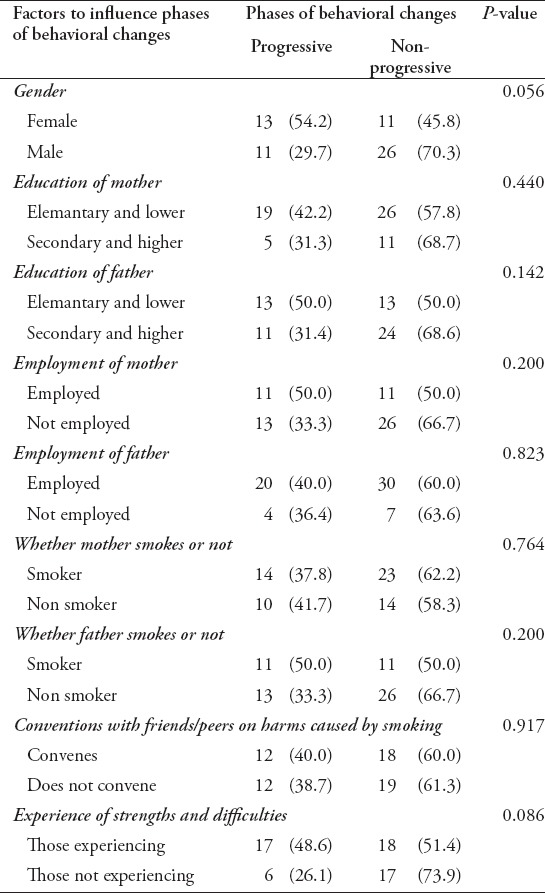
After peer education intervention, nicotine dependence of students were decreased significantly (p=0.0001). There were no significant associations between gender, daily living hardship, difficulties and education, employment and tobacco consumption of their parents during the phase of behavioral change of students (Table 5).
Table 5.
Comparison of factors to influence phases of behavioral changes in students after the sixth months later.
Discussion
In this study, the effectiveness of peer education in changing the smoking behavior of high school students was assessed. In many studies on the effectiveness of peer education, it is emphasized that most of the participants feel more confident and knowledgeable, their learning capacities and the exam performances increase. The peer education process was shown to increase student satisfaction, motivation, learning desire in the studies. Researches on peer education application show that this education has effects on many fields (education, health, and so forth) and in all age groups. It is also defined as an effective training method that enables peer education to change positively the risk factors and risk taking behaviors of adolescents.27-32 Bilateral learning is thought to take place through a learning-teaching approach based on peer education. In the study of Kenna and French, first grade students in nursing school develop more comfortable learning skills with their senior peers, expressing their emotions more comfortable;31 in Can’s study, it was seen that in the course of students receiving peer teaching among guitar students, their responsibilities and respect for authority were improved in terms of attendance, participation, preparation, continuity and study subjects;33 in Cebeci’s study, it was seen that the feedbacks of headworker and apprentice students in the peer teaching method applied to medical students benefit from the peer-assisted education. It has been estimated that peer-assisted education provides a gain for both the educator and the educated student.34 In the studies conducted in high school, university and community examples, mostly friends were reported as information sources. The influence of their peer group on the risky and safe behaviors of young people is observed. Because each individual is in communication with similar individuals, especially in terms of age and developmental periods.30 It was shown that smoking frequency in Turkey starts at an early age, the frequency of drinking increases with age, friend effect is effective in starting smoking, and peer education programs to be applied to schools will affect students’ smoking condition.11 The peer education model created for anti-smoking education should also be planned by taking into consideration the effect of the group of friends on the adolescent’s health-related attitudes and behaviors.
In our study, it was determined that peers’ talking to each other about the harm of cigarette did not increase significantly after peer education. However, peer group stated that peer education has added positive knowledge and skills to them. Peer education seems to have contributed significantly to the development of peer relations, which has increased the confidence and motivation of the students themselves. These students are able to transfer the knowledge and skills they have acquired during peer education to their daily lives and use these skills for the life. The effort of peer educators became a model to others in the application of peer education (with the principle of social learning) is also an important achievement.29
In this study, it is thought that peer education affects the smoking cessation behavior of the students positively. In the study, the peer group interacted with all the students, not just the smokers, to ensure that smokers are not known. For this reason, the effect of peer education on smoking students has not been fully determined. A third of the smokers showed behavioral changes after 6 months of evaluation. Because peer education is assessed 6 months later, it is considered that there is not enough time for evaluation. In Doğan’s study, it was found that peer education students constantly exchange information with each other, thus ensuring the continuity of education, positive role models are created and ‘social learning’ encourages their friends to take an attitude against cigarette;11 according to the Yaşlı’s study, peer education programs which are not long-term and continuous, were found to have no effect on youngsters’ smoking behavior;12 in the study of Karayurt et al32 it was found that group and peer education had positive effects; in the study of Koyun, it was determined that the increase in the number of interviews for cigarette cessation improved the results for the activities, the percentage of women at the stage of not thinking decreased from the first stage and the decrease tendency at the beginning of the study showed increase as the interviews continue during the preparation phase.27 According to these results, it is necessary to extend the study period of peer education to a long time and to maintain continuity. Before peer education, 17.6% of the students had moderate, high and very high nicotine dependence level, whereas 11.1% had moderate and high nicotine dependence afterwards. Nicotine dependence is effective in deciding which method to choose in smoking cessation treatment. Studies have shown that peer education is effective in smoking cessation behavior, that post-peer addiction knowledge scores are significantly higher than the control group, and that peer education is superior to other methods in the level of knowledge.29,30 In Andersson’s Blekinges project, it is stated that peer education should be used effectively to get rid of cigarette addiction.35 In the study, 18.3% of the students group were smokers. According to the Turkey Global Youth Tobacco Survey (GYTS) 2009, smoking rates of high school age children’s were 8.4%.3 According to GYTS data 2009, one third of youngsters started smoking before the age of 10 and smoking increased with the age, 19,5% of the students started using tobacco products under the age of 13, all started under the age of 17 and younger.3,9,10,19 In this study, there is a significant relation between the smoking status of male students and female students. Male students smoke more than female students. The fact that smoking is considered to be inappropriate for women in some countries is considered to be a factor in the low rate of smoking among women.5 The reasons why students use tobacco products are ranked according to their frequency count as; being curious about, imitating, being angry with his/her family, being stressed and friend pressure. In the study performed by Doğan et al11 students smoke with the reasons such as not to be separated from friends, curiosity, feeling better and habit. In researches made by WHO in various countries, among the reasons for starting smoking are peer pressure, stress, curiosity, being considered favourable by parents.1,2,4,5,21 “Peer pressure” is important in our country for starting smoking. In this study, while effect of friends was important, curiosity has been found to be in the lead.3
Students, in their conversations with their friends, talk about using tobacco, its damages and quitting every day, at least once in a week or a month. The students’ conversations with their friends have increased at the end of the study period. However, in our study, it could not have been fully determined how much these conversations affected the change of behavior. In our study, while they have been asked how often they talked, its context and the messages given have been evaluated according to the notifications of the peer educators.
The working status and the use of tobacco products of the students’ mothers do not affect their smoking status. It is known that the presence of alcohol, cigarettes and drug users in the family increases the tendency of these young people to imitate family elders.5,11 The peer group students stated that similar qualifications apply to their families at the meetings held.
In this study, 61 students evaluated according to their thinking stage constitute the focal point of the study. Because the last follow-up has been carried out 6 months later, the students in maintaining stage have been considered to have left the cigarette. For those, who were in the stage of action (have quieted, less than 6 months), it could not be followed up whether they have passed to maintaining stage or not, because of the completion of the work.
In the follow-up of the 61 students who were the focal point of the study, before peer education and after 6 months, it has been determined that there was a positive behavioral change after the peer education. Those who were in the pre-contemplation thinking stage have decreased, those who were in the maintaining stage have increased. Accordingly, it can be said that, the behaviors of the students have changed positively and that they have quieted smoking.
Transtheoretical model focuses on change fact developed optionally rather than change imposed through pressure from outside. It is less common for individuals to return to their former behavior because the initiatives made for behavior change. In TTM are individualized and evaluated by assessing the individual’s level of change. Transtheoretical model says that the most appropriate initiatives at the stage of change the individual experiences must be used in order to facilitate change.27 Including peers into anti-smoking trainings can enhance the effectiveness of these programs.11 This study was limited by the students were requested to write their names in the questionnaires. The students stated that they did not want to write with the thought that the school administration and their families would be informed. Two groups could not be brought together with the reason that the students were from different schools and the course hours could not be arranged.
In conclusion, following the peer education, the smoking behavior of the students has changed positively. Those among the students who were in the precontemptation stage have decreased, those who were in the contemptation, action (have quieted, less than 6 months) and maintaining stage have increased. Peer education is an appropriate method for providing behavioral change. Because the students show very low and low dependences according to the nicotine dependence scale, primarily behavioral cognitive initiatives should be planned. The educations should be held intensively and continuously with long durations, to increase the effectiveness of peer educations. While forming a peer group, the personal characteristics, friends and communications of the youngsters should be taken into consideration.
Processes of peer education should be conducted on constant, intensive and long-term basis so as to increase their efficiencies. Formation of peer groups requires trainers to consider individual differences in students and their communications with their peers. Group training should be supported by peer trainers and school principals, and its efficiency and functionality thus be constantly increased. Skills of students to manage difficulties they have encountered in the process of quitting smoking and saying “no” to any type of tobacco consumption should be supported. Young people should be encouraged to avoid passive smoking and easy access to tobacco products. School administrators should support peer education. Peer education should be regularly and consistently applied to society.
Footnotes
Disclosure.
References
- 1.World Health Organization. Health in 2015: from MDGs to SDGs. Geneva: World Health Organization; 2015. Available from URL: http://www.who.int/gho/publications/mdgs-sdgs/en/ [Google Scholar]
- 2.World Health Organization. WHO report on the global tobacco epidemic 2015. World Health Organization. 2015. Available from URL: http://www.who.int/tobacco/global_report/2015/en/
- 3.The Ministry of Health of Turkey. Global Adult Tobacco Survey Turkey Report - 2010. The Ministry of Health of Turkey. 2010 [Google Scholar]
- 4.World Health Organization. NCI Tobacco Control Monograph Series 21 - The Economics of Tobacco and Tobacco Control. Available from URL: http://www.who.int/tobacco/publications/economics/nci-monograph-series-21/en/
- 5.Çalışkan Ş. Factors Affecting Smoking of University Students (Econometric Approach) Usak University Journal of Social Sciencesi. 2015;8/2:23–48. [Google Scholar]
- 6.Softa HK, Karaahmetoğlu GU, Ergun S. Evaluation of substance use among high school students and related factors (Subject City: Kastamonu) Journal of Dependence. 2015;16:67–174. [Google Scholar]
- 7.Trofor A, Mihaicuta S, Man MA, Miron R, Esanu V, Trofor L. Approaching tobacco dependence in youngsters: impact of an interactive smoking cessation program in a population of Romanian adolescents. Journal of Clinical and Experimental Investigations. 2010;1:150–155. [Google Scholar]
- 8.Arslan HN, Terzi Ö, Dabak Ş, Pekşen Y. Substance cigarette and alcohol use among high school students in the Provincial Center of Samsun Turkey. Erciyes Medicine Journal. 2012;34:79–84. [Google Scholar]
- 9.Çan G. Prevalence of tobacco use. Turkey Health Report. 2012:201–204. [Google Scholar]
- 10.Akdur R. Youth smoking epidemic. Ankara (TR): Ankara University Medical School of Public Health Publications; 2010. [Google Scholar]
- 11.Doğan DG, Ulukol B. Factors affecting adolescent smoking and non-anti-effectiveness of two educational model. Inonu University Medical Faculty Journal. 2010;17:179–185. [Google Scholar]
- 12.Yaslı G. Effectiveness of peer education program regarding non youth protection. Manisa (TR): Manisa Celal Bayar University; 2009. [Google Scholar]
- 13.Sharma M. 3rd ed. Burlington (MA): Jones&Barlett Learning; 2016. Theoretical Foundations of Health Education And Health Promotion. [Google Scholar]
- 14.Glanz K, Rimer KB, Viswanath K. Health behavior theory, research, and practise. 5th ed. San Francisco (USA): John Wiley & Sons; 2015. [Google Scholar]
- 15.Prochaska JO. Transtheoretical model of behavior change. Encyclopedia of Behavioral Medicine. New York (NY): Springer; 2013. [Google Scholar]
- 16.Alvermann DE, Unrav NJ, Ruddell RB. Theoretical Models And Processes of Reading. 6th ed. Newark, Delaware (USA): International Reading Association; 2013. [Google Scholar]
- 17.Taş F, Seviğ EÜ, Güngörmü Z. Use of motivational interview technique with transtheoretical model for behavioral change in smoking addiction. Current Approaches in Psychiatry. 2016;8:380–393. [Google Scholar]
- 18. Peer Education Trainers Manual, the UN, Europe and Central Asia Region “Promotion and Protection of Young People's Health” Inter-agency Group Peer Education Subcommittee in November 2004; Ankara. [Google Scholar]
- 19.Özcebe H. Adolescents and Tobacco. Ankara: Ministy of Health; 2008. [Google Scholar]
- 20.Bilgiç N, Günay T. A method for supporting smoking cessation in adolescents: Peer education, descrıptıon of research methods. Turkish Thoracic Journal. 2014;15:102–105. [Google Scholar]
- 21.National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. Preventing Tobacco Use Among Youth and Young Adults. Atlanta (GA): Centers for Disease Control and Prevention (US); 2012. [PubMed] [Google Scholar]
- 22.Tekin ÇS, Kurçer MA. Role of motivation in smoking cessation at the Ankara University Faculty of Health Sciences Students. National Public Health Congress. 2012:14. [Google Scholar]
- 23.Ergül Ş. Evaluation of smoking habits effectiveness of nursing interventions for adolescents with opposing positive behavior development. Izmir (TR): Ege University, Institute of Health Sciences School of Nursing; 2005. [Google Scholar]
- 24.Spencer L, Wharton C, Moyle S, Adams T. The transtheoretical model as applied to dietary behaviour and outcomes. Nutr Res Rev. 2007;20:46–73. doi: 10.1017/S0954422407747881. [DOI] [PubMed] [Google Scholar]
- 25.Prochaska JO, Di Clemente CC. Transtheoretical therapy: Toward a more integrative model of change. Psychotherapy:-Theory, Research & Practice. 1982;19:276–288. [Google Scholar]
- 26.Mermer G, Dağhan Ş, Bilge A, Dönmez RÖ, Özsoy S, Günay T. Prevalence of tobacco use among school teachers and effect of training on tobacco use in western Turkey. Cent Eur J Public Health. 2016;24:137–143. doi: 10.21101/cejph.a4217. [DOI] [PubMed] [Google Scholar]
- 27.Koyun A. The effect of stage of change model based education given for smoking cessation to adult women [dissertation] Hacettepe (TR): Hacettepe University; 2013. [Google Scholar]
- 28.Ünver V, Akbayrak N. Peer tutoring model in nursing education. İzmir (TR): Dokuz Eylül University; 2013. [Google Scholar]
- 29.Akkuş D, Eker F, Karaca A, Kapısız Ö, Açıkgöz F. High School youth peer education program. An effective model to prevent substance abuse happen? Journal of Psychiatric Nursing. 2016;7:34–44. [Google Scholar]
- 30.Kırmızıtoprak E, Şimşek Z. The effect of peer-education on sexually transmitted diseases and safer sexual life knowledge and behaviour of young people. TAF Preventive Medicine Bulletin. 2011;10:463–472. [Google Scholar]
- 31.Ercan H, Yıldırım Orhan Ş. Peer teachıng-based learnıng teachıng approach in indıvıdual instrument and its instructıon course. Bolu (TR): Abant İzzet Baysal University; 2016. pp. 2269–2281. [Google Scholar]
- 32.Karayurt Ö, Dicle A, Malak AT. Effects of peer and group education on knowledge, beliefs and breast self examination practice among university students in Turkey. Turk J Med Sci. 2009;39:59–66. [Google Scholar]
- 33.Can ÜK. Test of the effectiveness of the peer teaching program developed for music teachers guitar students. İstanbul (TR): Marmara University Institute; 2009. [Google Scholar]
- 34.Cebeci S. The effect of peer-assisted education in pre-graduate medical education on student achievement in theoretical lectures. Ankara (TR): Hacettepe University; 2015. [Google Scholar]
- 35.Andersson E, Lindström E. Ambassadors in tobacco prevention - a qualitative study on peer education [dissertations] Kristianstad: Kristianstad University; 2017. [Google Scholar]