

Sir
A 26-year-old female presented with a history of asymptomatic red lesions over the right upper limb since 5 years. Lesions initially appeared on the right forearm and progressed to involve the outer aspect of the right upper limb and right side of the chest insidiously. There was no associated history of itching, vesiculation, or any limb anomaly. None of the family members had similar disorders.
General and systemic examination was essentially normal. Cutaneous examination revealed multiple, minute, pinpoint, grouped, bright red, nonblanchable macules, and irregular patches distributed in a patchy blaschkoid pattern over the right upper limb and right side of the chest [Figure 1]. Lesions were nonblanchable on diascopy. Dermoscopy revealed multiple red oval to round lagoons [Figure 2]. Mucocutaneous examination was unremarkable. Ophthalmological examination did not reveal any vascular abnormality.
Figure 1.

Presence of bright red, nonblanchable macules and irregular patches in a blaschkoid pattern over the right upper limb and right side of the chest
Figure 2.
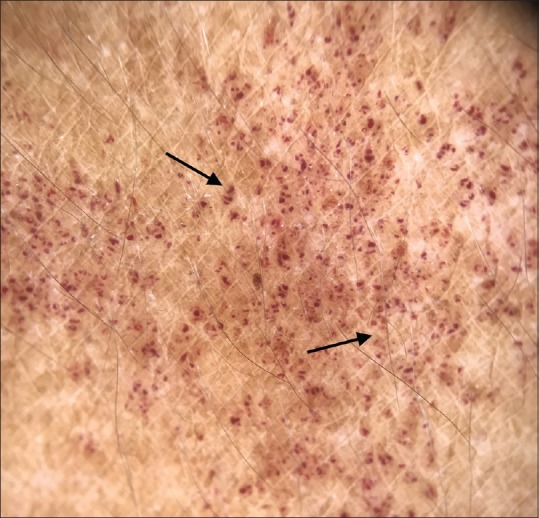
Dermoscopy revealed multiple red oval to round lagoons (3Gen Dermlite DL4 Polarized Dermoscope)
Routine hematological, biochemical, serum estrogen, and testosterone levels were normal. Histopathology revealed presence of multiple dilated capillaries with normal endothelial lining in the papillary and superficial reticular dermis [Figure 3]. There were neither epidermal changes nor extravasation of red blood cells. Based on the clinical, dermoscopic, and histopathological features, she was diagnosed as a case of blaschkoid angioma serpiginosum (AS). The patient was counseled regarding the benign nature of the disease and advised pulsed dye laser (PDL) treatment.
Figure 3.
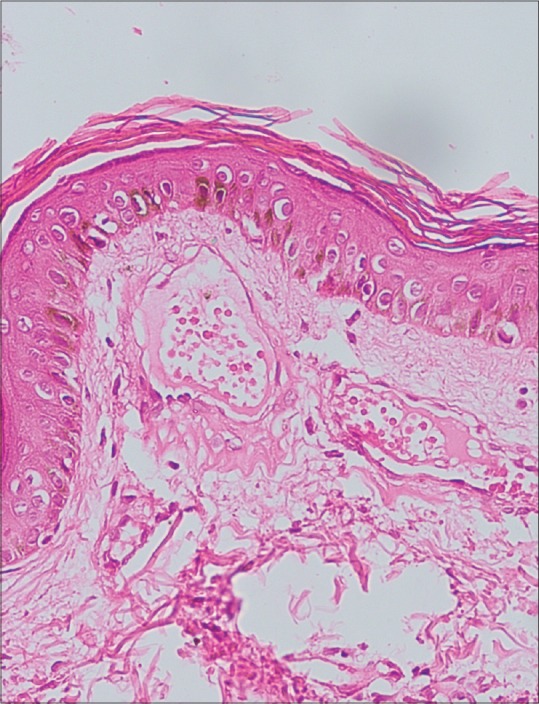
(H and E, ×40) Histopathology revealed presence of multiple dilated capillaries with normal endothelial lining in papillary and superficial reticular dermis
AS was first described by Hutchinson in 1889, and Radcliffe–Crocker proposed the term angioma serpiginosum in 1893.[1] It is a vascular anomaly with 90% of cases occurring in females classically beginning in childhood and adolescent age with 80% cases occurring before 20 years of age.[2] Clinically, it presents with characteristic multiple, small, asymptomatic, nonpalpable, deep-red punctate macules organized in small clusters and sheets forming a serpiginous and gyrate pattern.[1,2] It commonly appears on extremities, often starting unilaterally over blaschko's lines Although dissemination can occur, palms, soles, and mucosa are rarely affected. Plantar involvement has been reported.[3] The pathogenesis of AS is unknown. Female predominance, adolescent age of onset, and rapid progression in pregnancy might be indirect evidence of the role of estrogen in its pathogenesis.[1] Histopathology lacks epidermal changes or extravasation of red blood cells and reveals dilated, thin-walled capillaries in the dermal papillae and upper dermis.[2] Dermoscopy reveals characteristic well-demarcated red lagoons owing to dilated vascular spaces within the papillary or superficial reticular dermis. In addition to these typical dermoscopic feature, hairpin-like vessels scattered among red lagoons may also be present in AS.[4]
Morphological differential diagnosis includes pigmented purpura, unilateral nevoid telangiectasia (UNT), port-wine stain, and angiokeratoma corporis diffusum. All these diseases have dilated capillaries in the dermis on HPE. Pigmented purpura is characterized histopathologically by extravasation of erythrocytes, hemosiderin pigment, and features of inflammation, which are not seen in AS. UNT and port-wine stain have similar histopathological features as AS with solitary or grouped dilated thick-wall capillary vessels in the papillary dermis. UNT is characterized by the dermatomal distribution of telangiectasia, which are distributed unilaterally and frequently found in C3,–C4 or the trigeminal dermatomal areas.[4] Acquired port-wine stain is an uncommon vascular malformation entity developing later in life. Dermoscopic findings for vascular malformations include a superficial pattern known as blob pattern, consisting of red globules and dots that correspond to dilated capillaries in the papillary dermis and a deeper pattern composed of reddish ring-like structures that correspond to ectatic vessels located deep in the horizontal vascular plexus.[5] Angiokeratoma lesions on histopathology show orthokeratosis, epidermal acanthosis, and superficial ectatic and dilated capillaries lined by normal appearing endothelial cells in the dermis, whereas dermoscopic pattern most often consists of dark lacunae and a whitish veil.[4]
Our case showed typical clinical presentation, histopathological correlation, and characteristic red round to oval lagoons on dermoscopy consistent with the diagnosis of AS.
Segmental patterns of lesions, as seen in our case, may reflect cutaneous mosaicism, and it has been suggested that AS might be best categorized as a vascular nevus.[6]
In conclusion, AS is a rare vascular anomaly with dermoscopy offering a simple, noninvasive modality to help in the diagnosis of this uncommon entity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Sancheti K, Das A, Podder I, Gharami RC. Angioma serpiginosum in a patchy and blaschkoid distribution: A rare condition with an unconventional presentation. Indian J Dermatol. 2016;61:570–2. doi: 10.4103/0019-5154.190114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Das D, Nayak CS, Tambe SA. Blaschko-linear angioma serpiginosum. Indian J Dermatol Venereol Leprol. 2016;82:335–7. doi: 10.4103/0378-6323.175916. [DOI] [PubMed] [Google Scholar]
- 3.Freites-Martinez A, Martinez-Sanchez D, Moreno-Torres A, Huerta-Brogeras M, Hernández-Núñez A, Borbujo J. Angioma serpiginosum: Report of an unusual acral case and review of the literature. An Bras Dermatol. 2015;90:26–8. doi: 10.1590/abd1806-4841.20153794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ghanadan A, Kamyab-Hesari K, Moslehi H, Abasi A. Dermoscopy of angioma serpiginosum: A case report. Int J Dermatol. 2014;53:1505–7. doi: 10.1111/j.1365-4632.2012.05805.x. [DOI] [PubMed] [Google Scholar]
- 5.Shirakawa M, Ozawa T, Wakami S, Ishii M, Harada T. Utility of Dermoscopy before and after Laser Irradiation in Port Wine Stains. Ann Dermatol. 2012;24:7–10. doi: 10.5021/ad.2012.24.1.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chen W, Liu TJ, Yang YC, Happle R. Angioma serpiginosum arranged in a systematized segmental pattern suggesting mosaicism. Dermatology. 2006;213:236–8. doi: 10.1159/000095043. [DOI] [PubMed] [Google Scholar]