

Abstract
Importance
Few prospective longitudinal studies have evaluated the progression of Parkinson disease (PD) in patients with the leucine-rich repeat kinase 2 (LRRK2 [OMIM 609007]) mutation. Knowledge about such progression will aid clinical trials.
Objective
To determine whether the longitudinal course of PD in patients with the LRRK2 mutation differs from the longitudinal course of PD in patients without the mutation.
Design, Setting, and Participants
A prospective comprehensive assessment of a large cohort of patients from 3 sites with LRRK2 PD or with nonmutation PD was conducted from July 21, 2009, to September 30, 2016. All patients of Ashkenazi Jewish ancestry with PD were approached at each site; approximately 80% agreed to an initial visit. A total of 545 patients of Ashkenazi Jewish descent with PD who had 1 to 4 study visits were evaluated. A total of 144 patients (26.4%) had the LRRK2 G2019S mutation. Patients with GBA (OMIM 606463) mutations were excluded from the analysis.
Main Outcomes and Measures
Linear mixed-effects models for longitudinal motor scores were used to examine the association of LRRK2 mutation status with the rate of change in Unified Parkinson’s Disease Rating Scale III scores using disease duration as the time scale, adjusting for sex, site, age, disease duration, cognitive score, and levodopa-equivalent dose at baseline. Mixed-effects models were used to assess change in cognition, as measured by Montreal Cognitive Assessment scores.
Results
Among the 545 participants, 233 were women, 312 were men, and the mean (SD) age was 68.2 (9.1) years for participants with the LRRK2 mutation and 67.8 (10.7) years for those without it. Seventy-two of 144 participants with the LRRK2 mutation and 161 of 401 participants with no mutation were women. The estimate (SE) of the rate of change in the Unified Parkinson’s Disease Rating Scale III motor score per year among those with the LRRK2 mutation (0.689 [0.192] points per year) was less than among those without the mutation (1.056 [0.187] points per year; difference, −0.367 [0.149] points per year; P = .02). The estimate (SE) of the difference in the rate of change of the Montreal Cognitive Assessment score between those with the LRRK2 mutation (–0.096 [0.090] points per year) and those without the mutation (−0.192 [0.102] points per year) did not reach statistical significance (difference, 0.097 [0.055] points per year; P = .08).
Conclusions and Relevance
Prospective longitudinal follow-up of patients with PD with or without the LRRK2 G2019S mutation supports data from a cross-sectional study and demonstrates a slower decline in motor Unified Parkinson’s Disease Rating Scale scores among those with LRRK2 G2019S–associated PD.
This longitudinal study examines whether the course of Parkinson disease in patients with the LRRK2 mutation differs from the course of Parkinson disease in patients without the mutation.
Key Points
Question
What is the longitudinal progression of Parkinson disease in carriers of the LRRK2 mutation, and does it differ from the progression of idiopathic Parkinson disease?
Findings
In this longitudinal study, the rate of change in Unified Parkinson’s Disease Rating Scale III motor score was less among patients with the LRRK2 mutation than among patients without the mutation. There was no statistically significant difference between carriers and noncarriers in change in cognition as measured by the Montreal Cognitive Assessment score.
Meaning
Patients with the LRRK2 mutation demonstrate slower decline in motor functioning than do patients without the mutation, which may have implications for the use of emerging disease-modifying agents.
Introduction
Disease-modifying agents for leucine-rich repeat kinase 2 (LRRK2 [OMIM 609007]) are being developed, and clinical trials for patients with Parkinson disease (PD) who carry the LRRK2 mutation are on the horizon.1 As personalized genomic medicine gains traction in PD, understanding differences in the clinical course of genetic forms of parkinsonism may also aid clinicians in symptomatic treatment and counseling.2 Thus, there is a need to characterize progression markers of LRRK2-associated PD, specifically to evaluate the most frequent LRRK2 mutations.
Whether and how the motor progression of LRRK2-associated PD differs from that of idiopathic PD (IPD) is debated3,4,5 and may differ among LRRK2 genotypes. A cross-sectional study supports the premise that LRRK2 G2019S mutation PD among patients of Ashkenazi Jewish descent is milder and may progress more slowly compared with IPD.4 Most reports on patients with PD who carry the LRRK2 G2019S mutation are limited in assessing progression differences because they are cross-sectional or retrospective,3,4 and data on the rate of progression in these patients compared with those who do not have the mutation are varied.5,6,7 We report the longitudinal follow-up assessment of a large cohort of patients with PD, with or without the LRRK2 G2019S mutation, followed up prospectively for up to 5 years.
Methods
Study Design and the Ashkenazi Jewish Cohort With the LRRK2 Mutation
This prospective comprehensive assessment of a large cohort of patients with LRRK2-associated PD or IPD was conducted from July 21, 2009, to September 30, 2016. Participants were recruited from 3 LRRK2 Ashkenazi Jewish Consortium sites (Tel Aviv Medical Center, Tel Aviv, Israel; Columbia University Medical Center, New York, New York; or Mount Sinai Beth Israel, New York, New York), and ethical approval was obtained from the Tel Aviv Medical Center Ethical Committee, Columbia University Medical Center Institutional Review Board, and Mount Sinai Beth Israel Institutional Review Board. All participants provided written informed consent prior to participating in this study.
Participants included individuals previously ascertained for studies of LRRK2 and newly ascertained individuals who either answered an advertisement for the study or learned about it from their physicians. Newly ascertained individuals initially agreed to a short screening visit. As planned under the study protocol, all of the individuals with the LRRK2 G2019S mutation, as well as a subset of those with newly ascertained PD without LRRK2 mutations, were subsequently invited to participate in in-depth yearly follow-up visits. All previously ascertained individuals (those cases with the LRRK2 G2019S mutation and those cases without it) were asked to undergo in-depth yearly visits. Baseline data in the subgroups were previously reported.4,8,9
Participants and Visit Methods
All participants were screened for the LRRK2 G2019S mutation and for the common glucocerebrosidase 1 (GBA1 [OMIM 606463]) mutations among those of Ashkenazi Jewish descent, as previously reported.10,11 Individuals with the GBA1 mutation, including those who also carried the LRRK2 G2019S mutation, were excluded from the analyses.
Visits were performed at a LRRK2 Ashkenazi Jewish Consortium site or at the participants’ homes and included the following: complete Unified Parkinson’s Disease Rating Scale (UPDRS) motor features12 as assessed by UPDRS III12 and the Hoehn and Yahr stage,13 subjective reporting of status as reported by the Schwab England Activity of Daily Living Scale score14 and UPDRS II,12 and cognitive status as measured with the Montreal Cognitive Assessment (MoCA).15 Because a comprehensive neuropsychological battery was performed only in a subset of individuals and visits, it is not reported here. Visits occurred in the practically defined “on” state, and reviewers were blinded to individuals’ carrier status. Participants who had undergone deep brain stimulation were excluded from analysis; if there was incident deep brain stimulation, the last visit without this procedure was included as the final study visit.
Statistical Analysis
The main analysis included all participants who had at least 1 study visit with complete UPDRS III motor features assessed. This approach avoided potential bias in the estimation of model parameters that might have occurred if the analysis were limited only to those with at least 2 visits.16 The primary outcomes of interest were longitudinal change in motor scores (UPDRS III) and change in cognition (MoCA). In subanalyses, the UPDRS III was divided into total rest tremor score (UPDRS items 20 a-e), rigidity (items 22 a-e), bradykinesia (items 23-26 and item 31), and posture, gait, and balance items (items 27-30). Total UPDRS, UPDRS I, and UPDRS II scores were also evaluated. Linear mixed-effects models17 were used to compare the rate of change in these motor scores between patients with PD who were carriers of the LRRK2 G2019S mutation and those who did not carry the mutation. Disease duration was used as the time scale because of its strong association with UPDRS score and cognition. The participant-specific random effect was used to account for correlations among repeated measurements from the same participant. The linear mixed-effect models take into account the correlations among repeated measurements within the same participant and can accommodate unbalanced data resulting from missing data points, unequal numbers of follow-up visits due to dropouts, and staggered time of first visit (as well as unequal intervals among visits), and these models are commonly used to determine the trajectory of the longitudinal markers. Known and potential confounders, including age at baseline, duration of disease at baseline, sex, levodopa-equivalent dose,18 and study site, were adjusted. In UDPRS subanalyses except UPDRS I, MoCA scores were also included as a covariate for cognitive impairment.19,20,21 Similar to the motor assessments, linear mixed-effects models17 were used to compare the rate of change in cognition scores (MoCA) between patients with PD who were carriers of the LRRK2 G2019S mutation and those who did not carry the mutation, and these models were adjusted for known and potential confounders, including age at baseline, duration of disease at baseline, sex, levodopa-equivalent dose,18 and study site.
As secondary analyses, sensitivity analyses were performed for UDPRS III and MoCA, including only individuals who had 2 or more visits (eTable and eFigures 1 and 2 in the Supplement). In addition, linear mixed-effect models were used to assess change in Hoehn and Yahr stage, and time-to-event analyses were performed using left-truncated Cox proportional hazards regression models.22 These models included the development of Hoehn and Yahr stage III; the onset of freezing when walking, which was defined as change in UPDRS II item 14 score from a baseline of 0 to the development of a score of 1 or greater; and the onset of falls unrelated to freezing, which was defined as a change in UPDRS II item 14 score from 0 or 1 to 2 or greater. Covariates included age at baseline, sex, and study site. P < .05 was considered significant.
Results
A total of 576 participants were identified as having available data. Of these, 545 who did not receive deep brain stimulation at the time of their baseline visit were included in the main analysis (151 participants at Mount Sinai Beth Israel; 128 participants at Columbia University Medical Center; and 266 participant at the Tel Aviv Medical Center), and 144 of these 545 participants (26.4%) carried the LRRK2 G2019S mutation. The demographic and clinical characteristics for carriers and noncarriers are presented in Table 1. A total of 179 patients had follow-up visits (97 noncarriers and 82 carriers), with a median of 3 follow-up visits per participant (range, 2-5 visits). Twenty-four patients with PD who carried the LRRK2 mutation and 33 patients with IPD had 2 years of follow-up, 27 patients with PD who carried the LRRK2 mutation and 36 patients with IPD had 3 years of follow-up, 24 patients with PD who carried the LRRK2 mutation and 20 patients with IPD had 4 years of follow-up, and 7 patients with PD who carried the LRRK2 mutation and 8 patients with IPD had 5 years of follow-up. The mean (SD) duration between visits among those with at least 1 follow-up visit was about 13 months and was not different between those carrying the LRRK2 G2019S mutation (12.74 [5.08] months) and those not carrying the mutation (12.71 [5.15] months; P = .83).
Table 1. Clinical and Demographic Features of the Cohort Comparing Patients With PD Who Carry the LRRK2 Mutation With Patients With IPDa,b.
| Characteristic | Patients, No./Total No. (%) | P Value | |
|---|---|---|---|
| LRRK2-Associated PD | IPD | ||
| Age at examination, mean (SD), y | 68.2 (9.1) | 67.8 (10.7) | .70 |
| Age at onset, mean (SD), y | 60.0 (9.3) | 61.5 (10.7) | .12 |
| Duration of disease, mean (SD), y | 8.2 (6.0) | 6.3 (5.5) | <.001 |
| Male | 72/144 (50.0) | 240/401 (59.9) | .04 |
| Site | |||
| CUMC | 33/144 (22.9) | 95/401 (23.7) | .67 |
| TA | 67/144 (46.5) | 199/401 (49.6) | |
| MSBI | 44/144 (30.6) | 107/401 (26.7) | |
| College or greater education | 108/132 (81.8) | 307/389 (78.9) | .48 |
| MoCA score, mean (SD) | 25.14 (2.85) | 24.71 (3.90) | .25 |
| H&Y baseline stage, mean (SD) | 2.07 (0.88) | 2.11 (0.84) | .69 |
| H&Y stage | |||
| 1 | 31/130 (23.8) | 67/339 (19.8) | .35 |
| 1.5 | 16/130 (12.3) | 35/339 (10.3) | |
| 2 | 35/130 (26.9) | 116/339 (34.2) | |
| 2.5 | 13/130 (10.0) | 50/339 (14.7) | |
| 3 | 28/130 (21.5) | 50/339 (14.7) | |
| 4 | 3/130 (2.3) | 15/339 (4.4) | |
| 5 | 2/130 (1.5) | 5/339 (1.5) | |
| UPDRS subscores, mean (SD) | |||
| I | 1.69 (1.55) | 1.80 (1.70) | .53 |
| II | 8.42 (6.06) | 9.01 (5.94) | .32 |
| III | 19.38 (12.02) | 20.29 (12.08) | .44 |
| Rest tremor (item 20) | 1.17 (1.63) | 1.52 (1.73) | .04 |
| Rigidity (item 22) | 4.16 (3.33) | 4.14 (3.35) | .95 |
| Posture (item 30) | 0.77 (0.96) | 0.70 (0.90) | .42 |
| Bradykinesia (item 31) | 8.41 (6.03) | 8.53 (5.71) | .83 |
| Schwab-England ADL | 86.65 (18.92) | 86.26 (20.55) | .85 |
| Falling (item 13) | 0.39 (0.61) | 0.31 (0.62) | .23 |
| Freezing (item 14) | 0.37 (0.73) | 0.38 (0.71) | .91 |
| Type of PD | .02 | ||
| PIGD | 97/142 (68.3) | 218/396 (55.1) | |
| Tremor predominant | 22/142 (15.5) | 73/396 (18.4) | |
| Intermediate | 23/142 (16.2) | 105/396 (26.5) | |
| LEDD at baseline, mean (SD), mg levodopa | 407.39 (410.23) | 337.10 (367.58) | .06 |
| Receiving levodopa at baseline | 103/140 (73.6) | 248/396 (62.6) | .02 |
Abbreviations: ADL, activities of daily living; CUMC, Columbia University Medical Center; H&Y, Hoehn and Yahr; IPD, idiopathic Parkinson disease; LEDD, Levodopa equivalent daily dose; LRRK2, leucine-rich repeat kinase 2; MoCA, Montreal Cognitive Assessment; MSBI, Mount Sinai Beth Israel; PD, Parkinson disease; PIGD, Postural Instability Gait Disturbance; TA, Tel Aviv; UPDRS, Unified Parkinson’s Disease Rating Scale.
Among individuals with complete UPDRS III data at baseline.
Participants with baseline UPDRS data were included in the group total. Other rating scales were included in the analysis when available, although the number of participants with available baseline ratings in each group (in addition to the UPDRS) may be less than the presented group total.
Consistent with a previous report of baseline features,4 those carrying the LRRK2 G2019S mutation and those not carrying the mutation were similar in age at examination, UPDRS I-III subscale scores, Schwab and England Activity of Daily Living Scale score, Hoehn and Yahr rating, and total MoCA score. Individuals carrying the LRRK2 G2019S mutation were more likely than those not carrying the mutation to be women (72 of 144 [50.0%] vs 161 of 401 [40.1%]; P = .04) and to be classified with postural instability gait disturbance (PIGD) (97 of 142 [68.3%] vs 218 of 396 [55.1%]; P = .02). They also had longer mean (SD) duration of disease (8.2 [6.0] vs 6.3 [5.5] years; P < .001) and a higher mean (SD) daily equivalent dose of levodopa (407.4 [410.2] vs 337.1 [367.6] mg levodopa; P = .06). There was no difference between individuals carrying the LRRK2 G2019S mutation and those not carrying the mutation in age at onset of PD or frequency of falling unrelated to freezing. Site differences are similar to those previously reported.4
Linear mixed-effects models examined the association of LRRK2 mutation status with the rate of change in UPDRS III score, adjusting for baseline age, sex, site, duration of disease at baseline, MoCA score, and levodopa-equivalent dose (Table 2). Male sex (β = 3.55; 95% CI, 1.85-5.25; P < .001), older age (β = 0.21; 95% CI, 0.12-0.30; P < .001), and MoCA score (β = −0.48; 95% CI, −0.67 to −0.30; P < .001) at baseline were associated with a higher UPDRS III score. The estimate (SE) of the rate of change in UPDRS III motor score per year among individuals carrying the LRRK2 G2019S mutation (estimate, 0.689 [0.192] points per year) was less than among those not carrying the mutation (estimate, 1.056 [0.187] points per year; P < .001) (difference, −0.367 [0.149] points per year) (Figure 1). In an additional model that included baseline PIGD score, the rate of UPDRS III change per year remained significant between groups. We included in the analysis individuals who did not return for follow-up visits, together with those with more than 1 visit, because this method was the statistically least biased. However, we also performed sensitivity analyses, including only individuals who had 2 or more visits (n = 179). In this subset, individuals carrying the LRRK2 mutation also had a slower decrease in motor UPDRS scores (eTable in the Supplement), and the magnitude of the effects was similar to that in the overall group.
Table 2. Models Comparing Rate of Change in UPDRS-III Score (Model 1), H&Y Stage (Model 2), and MoCA Score (Model 3) Among Patients With PD Who Carry the LRRK2 Mutation vs Patients With IPD.
| Characteristic | UPDRS III Score (n = 545) | H&Y Stage (n = 488) | MoCA Score (n = 522) | |||
|---|---|---|---|---|---|---|
| β (95% CI) | P Value | β (95% CI) | P Value | β (95% CI) | P Value | |
| Rate difference, ya | −0.37 (−0.66 to −0.07) | .02 | −0.01 (−0.03 to 0.01) | .24 | 0.10 (−0.01 to 0.21) | .08 |
| Baseline age, y | 0.21 (0.12 to 0.30) | <.001 | 0.02 (0.01 to 0.02) | <.001 | −0.14 (−0.17 to −0.11) | <.001 |
| Sex (reference: female) | 3.55 (1.85 to 5.25) | <.001 | 0.04 (−0.08 to 0.16) | .60 | −0.87 (−1.44 to −0.31) | .003 |
| Baseline duration by LRRK2 status (reference: IPD)b | 1.13 (−1.95 to 4.21) | .47 | −0.04 (−0.26 to 0.17) | .68 | 0.03 (−0.90 to 0.96) | .95 |
| Site | ||||||
| MSBI | −5.33 (−7.33 to −3.33) | <.001 | −0.09 (−0.22 to 0.04) | .18 | 0.95 (0.25 to 1.65) | .008 |
| CUMC (reference: TA) | −1.85 (−3.95 to 0.26) | .09 | 0.11 (−0.07 to 0.28) | .23 | 1.60 (0.89 to 2.31) | <.001 |
| Baseline duration, y | −0.32 (−0.69 to 0.05) | .09 | −0.05 (−0.07 to −0.02) | .001 | 0.08 (−0.11 to 0.27) | .42 |
| LEDD | 0 | .77 | 0 | .70 | 0 | <.001 |
| MoCA | −0.48 (−0.67 to −0.30) | <.001 | −0.03 (−0.05 to −0.01) | <.001 | NA | NA |
| PD duration at visit, yc | 1.06 (0.69 to 1.42) | <.001 | 0.10 (0.07 to 0.12) | <.001 | −0.19 (−0.39 to 0.01) | .060 |
Abbreviations: CUMC, Columbia University Medical Center; H&Y, Hoehn and Yahr; IPD, idiopathic Parkinson disease; LEDD, levodopa-equivalent daily dose; LRRK2, leucine-rich repeat kinase 2; MoCA, Montreal Cognitive Assessment; MSBI, Mount Sinai Beth Israel; NA, not applicable; PD, Parkinson disease; TA, Tel Aviv; UPDRS, Unified Parkinson’s Disease Rating Scale.
The difference in rate of change in UPDRS score, H&Y stage, or MoCA score in the respective models between LRRK2 carriers and patients with IPD, which is the predictor of concern in this model.
Described the comparison of the mean difference of duration of disease at baseline between LRRK2 and IPD.
Relative to IPD.
Figure 1. Longitudinal Trajectories of Mean Unified Parkinson’s Disease Rating Scale III (UPDRS III) Scores for Patients With Parkinson Disease (PD) Who Carry the Leucine-Rich Repeat Kinase 2 (LRRK2) Mutation Compared With Patients With Idiopathic PD (IPD).
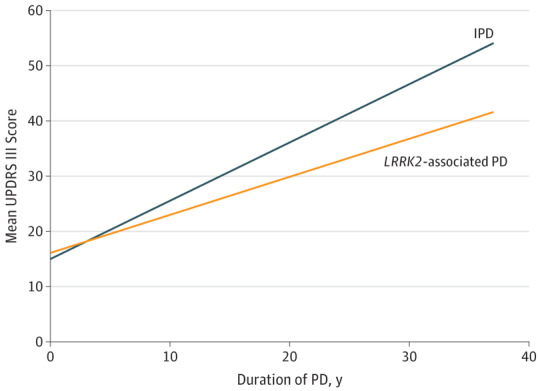
Longitudinal trajectories of mean UPDRS III scores show slower progression for patients with PD who carry the LRRK2 mutation than for patients with IPD. This included individuals sampled at different time points in the course of the disease. Individuals were followed up between 0 and 6 follow-up visits. Thus, no individual was followed up for the full duration described on the x-axis. The graphs demonstrate the mean UDPRS III score change in the IPD and LRRK2 PD groups with covariates fixed at the following values: baseline age = 67 years, baseline disease duration = 0 years, Montreal Cognitive Assessment score = 25, levodopa-equivalent dose = 457 mg levodopa, sex = female, and site = Tel Aviv. Trajectories are adjusted for the covariates described in Table 2. Spaghetti plots demonstrating the change for individual participants are shown in eFigure 5 in the Supplement.
In subanalyses evaluating differences in change in motor domains, the estimate (SE) of the rate of change in rigidity score per year among individuals carrying the LRRK2 mutation (estimate, 0.091 [0.071] points per year) was lower than among those not carrying the mutation (0.193 [0.068] points per year; P = .02) (difference, −0.102 [0.042] points per year). In addition, the rate of change in the estimate (SE) of the posture and gait score per year among individuals carrying the LRRK2 mutation (estimate, 0.169 [0.052] points per year) was lower than among those not carrying the mutation (0.273 [0.048] points per year; P = .01) (difference, −0.104 [0.041] points per year). Finally, the mean (SE) rate of change in bradykinesia motor score among individuals carrying the LRRK2 mutation (estimate, 0.297 [0.106] points per year) was lower than among those not carrying the mutation (0.396 [0.112] points per year; P = .15) (difference, 0.099 [0.069] points per year), although the difference was not significant. The rate of change of rest tremor score did not differ between groups.
Linear mixed-effects models examined the association of LRRK2 mutation status with the rate of change in MoCA, adjusting for baseline age, sex, site, duration of disease at baseline, and levodopa-equivalent dose (Table 3 and Figure 2). The estimate (SE) of the rate of change in MoCA score per year among individuals carrying the LRRK2 mutation (estimate, −0.096 [0.090] points per year) did not reach statistical significance compared with those not carrying the mutation (−0.192 [0.102] points per year; P = .08) (difference, 0.097 [0.055] points per year).
Table 3. Summary of Adjusted Models Comparing UPDRS Rates of Change in Patients With PD Who Carry the LRRK2 Mutation vs Patients With Idiopathic PDa.
| Outcome | β (95% CI) | P Value |
|---|---|---|
| Total UPDRS score | 0.50 (−0.95 to −0.05) | .03 |
| UPDRS I subscore | −0.05 (−0.10 to −0.01) | .01 |
| UPDRS II subscore | −0.10 (−0.28 to 0.09) | .30 |
| UPDRS III subscore | −0.37 (−0.66 to −0.07) | .02 |
| Rigidity subscore | −0.10 (−0.19 to 0.02) | .02 |
| Bradykinesia subscore | −0.10 (−0.24 to 0.04) | .15 |
| Resting tremor subscore | −0.03 (−0.08 to 0.03) | .31 |
| Posture subscore | −0.10 (−0.18 to −0.02) | .01 |
| Total MoCA scoreb | 0.10 (−0.01 to 0.21) | .08 |
Abbreviations: LRRK2, leucine-rich repeat kinase 2; MoCA, Montreal Cognitive Assessment; PD, Parkinson disease; UPDRS, Unified Parkinson’s Disease Rating Scale.
Each model includes baseline age, sex, site, baseline duration of disease, levodopa-equivalent daily dose, and MoCA.
Included in the model as the outcome.
Figure 2. Longitudinal Trajectories of Montreal Cognitive Assessment (MoCA) Scores in Patients With Parkinson Disease (PD) Who Carry the Leucine-Rich Repeat Kinase (LRRK2) Mutation Compared With Patients With Idiopathic PD (IPD).
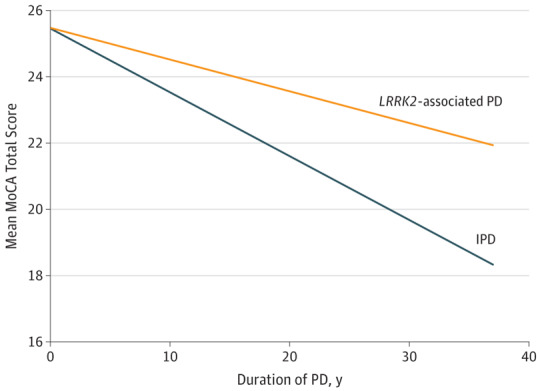
Longitudinal trajectories of MoCA scores show slower progression for patients with PD who carry the LRRK2 mutation than for patients with IPD. This included individuals sampled at different time points in the course of the disease. Individuals were followed up between 0 and 6 follow-up visits. Thus, no individual was followed for the full duration described on the x-axis. Spaghetti plots demonstrating the change for individual participants are shown in eFigure 5 in the Supplement.
The estimate (SE) of the rate of change in the Hoehn and Yahr stage per year among individuals carrying the LRRK2 mutation (estimate, 0.085 [0.014] points per year) was not different compared with those not carrying the mutation (0.097 [0.014]; P = .24) (difference, –0.013 [0.011] points per year). Of the 143 patients with follow-up data who had a Hoehn and Yahr stage less than 3 at enrollment, 22 progressed to stage 3 or above. Adjusting for baseline age, sex, and site, we found that individuals carrying the LRRK2 mutation (n = 64) showed a trend toward a lower risk of progression to Hoehn and Yahr stage 3 (hazard ratio, 0.45; 95% CI, 0.19-1.09; P = .08) compared with those not carrying the mutation (n = 79). There was no difference between risk of onset of falls (22 incident cases) for individuals with PD who carried the LRRK2 mutation vs those with IPD (hazard ratio, 0.42; 95% CI, 0.15-1.17) and risk of onset of freezing (36 incident cases) for individuals with PD who carried the LRRK2 mutation vs those with IPD (hazard ratio, 0.85; 95% CI, 0.41-1.76).
Discussion
Although a milder progression in motor symptoms in individuals with PD who carry the LRRK2 G2019S mutation has been posited in cross-sectional studies,3,4 the present study is the first, to our knowledge, to demonstrate this milder progression using prospective analysis. The slower progression estimates could inform clinical trial design for emerging LRRK2-targeted agents. Although the difference between PD with the LRRK2 mutation and IPD was modest, more precise estimates of progression could improve power at the same sample size. Furthermore, in a study with IPD and LRRK2-associated PD, the association might be magnified if patients with LRRK2-associated PD were not randomized by group, and if a disproportionate group was in the control arm rather than the treatment arm. A therapeutic effect would thus be underestimated. We expand on prior longitudinal studies of PD associated with LRRK2 G2019S in that data on visits were systematically and prospectively collected from a large multicenter cohort across 3 sites and 2 continents, and the patients were followed up for up to 5 years.
Our rate of change in the UPDRS for patients with IPD is within the range of that seen in other studies, which reported a progression on the UPDRS III motor score ranging from approximately 0.7 to 2.7 points per year.23,24,25 Our overall motor finding also contrasts with that in a smaller prospective longitudinal study focused on the change in UPDRS score.6 In a Tunisian cohort of patients with PD, patients with PD who carry the LRRK2 G2019S mutation were compared with patients with genetically undetermined PD. Baseline and 6-year time points were compared, and there was no difference between groups.6 However, this analysis may have been affected by survival bias for individuals who were able to return for a year 6 visit (58 of 147 individuals with LRRK2-associated PD and 54 of 267 individuals with IPD). Furthermore, sampling limited to 2 time points precludes the use of the linear mixed-effects models used herein and by others.7
Both higher-penetrance causative mutations and lower-penetrance risk variants have been identified in LRRK2.26,27,28 Our findings also diverge from the other prospective longitudinal study of LRRK2 that similarly used a random intercept linear mixed-effects model but focused on different LRRK2 genotypes—G2385R, R1628P, and S1647T risk variant PD.7 In that cohort, there was more rapid progression of disease with these LRRK2 genotypes than of IPD,7 a finding that is consistent with cross-sectional data supporting a worse clinical course for patients with PD who carry the LRRK2 G2385R mutation.29 Our methods differed in that the follow-up by Oosterveld et al7 was longer (approximately 6 years) and because we included all baseline visits in our mixed-effects model. However, our findings of a slower decrease in motor UPDRS score remained consistent even in sensitivity analyses that included only individuals who had 2 or more visits. Therefore, we believe that methodological differences could not explain the discrepant findings and that these are more likely attributable to genotype. In contrast to risk-variant LRRK2 studies, cross-sectional and longitudinal studies of patients with PD who carry the LRRK2 R1441G mutation show similar penetrance and clinical features to those found in patients with PD who carry the LRRK2 G2019S mutation.30 Longitudinal studies of carriers of the LRRK2 R1441G mutation will help better discern whether their clinical course differs from that of patients with IPD or that of patients with PD who carry the LRRK2 G2019S mutation.
Although we did not find a significant difference in the change in MoCA score, the direction of change is in support of a better cognitive course in individuals carrying the LRRK2 mutation. Analysis of a more sensitive cognitive battery in a subset of participants will be reported separately.
Our study did show a potentially provocative finding with regard to patients with PD who carry the LRRK2 mutation—namely, slower progression of disease in the setting of a higher frequency of classification as PIGD. This slower progression includes a slower decrease in total UPDRS, UPDRS I, and UPDRS III and posture, gait, and balance scores. Moreover, the difference in the change in UPDRS score remained significant in models adjusting for PIGD. Contrary to the prevailing idea that PIGD correlates with rapid decline, the co-occurrence of PIGD and less rapid decline in the LRRK2 group suggests that the PIGD vs tremor-dominant dichotomy may have more limited application in this setting. Although patients with tremor-dominant PD with more benign outcomes (and less levodopa sensitivity) may be detected in the classification scheme, it is insensitive to the heterogeneity of PIGD, and criticisms about the schema are widely raised.31,32 This heterogeneity may be especially applicable for LRRK2 G2019S, where variable, chronic, and slow pathologic changes may be at play, as well as compensatory mechanisms, as suggested by functional imaging and sensitive measurements of gait in carriers of the LRRK2 G2019S mutation without PD.33,34
Although, overall, PD may progress more slowly in patients who carry the LRRK2 G2019S mutation than in patients with IPD, there is heterogeneity in the pathologic findings of PD35,36 and even in LRRK2 G2019S PD.37 Some cases of LRRK2 G2019S PD demonstrate only isolated nigral degeneration without associated Lewy body deposition,38 and olfactory data suggest that there may be subgroups of LRRK2 PD, with some LRRK2 G2019S PD having normal olfaction.9 The more benign pathologic phenotype also correlates inversely with some of the nonmotor features typically attributed to Lewy body–predominant pathologic findings, including impaired olfaction as well as rapid eye movement sleep behavior disorder, which is a less frequent feature of LRRK2-associated PD.39,40,41 However, it is unclear whether the overall milder course represents an average of divergent LRRK2 pathologic findings or less overall synuclein burden.
Limitations
There are limitations to our study. One is that, because we did not have extensive follow-up data, we chose linear models. However, the course of PD may not be not linear,42,43 especially during the late stage of the disease. To address whether this choice of model might have affected our interpretation, we performed a sensitivity analysis limited to individuals with a disease duration of 20 years or less (eFigures 3 and 4 in the Supplement), and, as noted, the overall association with UPDRS score was maintained. Spaghetti plots demonstrating individual data are described in eFigure 5 in the Supplement.
Conclusions
Our prospective analysis of a large cohort of patients with PD with and without the LRRK2 G2019S mutation shows slower motor progression in the group with the LRRK2 G2019S mutation. Larger and longer-duration longitudinal studies, including those evaluating pathologic findings and nonmotor features, are warranted.
eTable. Models Comparing Rate Change in UPDRS III, MoCA, and H&Y; LRRK2 PD vs IPD (Among Participants With ≥ 2 Visits)
eFigure 1. Longitudinal Trajectories of Mean UPDRS III Scores in LRRK2 PD Compared With IPD Restricted to Those With at Least Two Visits
eFigure 2. Longitudinal Trajectories of MoCA Scores in LRRK2 PD Compared With IPD Restricted to Those With at Least Two Visits
eFigure 3. Longitudinal Trajectories of Mean UPDRS III Scores in LRRK2 PD Compared With IPD Among Those With 20 Years of Disease or Less: Mean Trajectories From Models Restricted to Disease Duration ≤ 20 Years
eFigure 4. Longitudinal Trajectories of MoCA Scores in LRRK2 PD Compared With IPD Among Those With 20 Years of Disease or Less
eFigure 5. Spaghetti Plots Demonstrating Change in UPDRS III Scores Relative to Time Since Baseline in LRRK2 PD and IPD
References
- 1.West AB. Ten years and counting: moving leucine-rich repeat kinase 2 inhibitors to the clinic. Mov Disord. 2015;30(2):180-189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Giladi N, Mirelman A, Thaler A, Orr-Urtreger A. A personalized approach to Parkinson’s disease patients based on founder mutation analysis. Front Neurol. 2016;7(7):71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Healy DG, Falchi M, O’Sullivan SS, et al. ; International LRRK2 Consortium . Phenotype, genotype, and worldwide genetic penetrance of LRRK2-associated Parkinson’s disease: a case-control study. Lancet Neurol. 2008;7(7):583-590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Alcalay RN, Mirelman A, Saunders-Pullman R, et al. Parkinson disease phenotype in Ashkenazi Jews with and without LRRK2 G2019S mutations. Mov Disord. 2013;28(14):1966-1971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yahalom G, Orlev Y, Cohen OS, et al. Motor progression of Parkinson’s disease with the leucine-rich repeat kinase 2 G2019S mutation. Mov Disord. 2014;29(8):1057-1060. [DOI] [PubMed] [Google Scholar]
- 6.Nabli F, Ben Sassi S, Amouri R, Duda JE, Farrer MJ, Hentati F. Motor phenotype of LRRK2-associated Parkinson’s disease: a Tunisian longitudinal study. Mov Disord. 2015;30(2):253-258. [DOI] [PubMed] [Google Scholar]
- 7.Oosterveld LP, Allen JC Jr, Ng EY, et al. Greater motor progression in patients with Parkinson disease who carry LRRK2 risk variants. Neurology. 2015;85(12):1039-1042. [DOI] [PubMed] [Google Scholar]
- 8.Alcalay RN, Mejia-Santana H, Mirelman A, et al. ; LRRK2 Ashkenazi Jewish Consortium . Neuropsychological performance in LRRK2 G2019S carriers with Parkinson’s disease. Parkinsonism Relat Disord. 2015;21(2):106-110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Saunders-Pullman R, Mirelman A, Wang C, et al. Olfactory identification in LRRK2 G2019S mutation carriers: a relevant marker? Ann Clin Transl Neurol. 2014;1(9):670-678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gan-Or Z, Giladi N, Rozovski U, et al. Genotype-phenotype correlations between GBA mutations and Parkinson disease risk and onset. Neurology. 2008;70(24):2277-2283. [DOI] [PubMed] [Google Scholar]
- 11.Orr-Urtreger A, Shifrin C, Rozovski U, et al. The LRRK2 G2019S mutation in Ashkenazi Jews with Parkinson disease: is there a gender effect? Neurology. 2007;69(16):1595-1602. [DOI] [PubMed] [Google Scholar]
- 12.Fahn S, Elton RL; Members of the UPDRS Development Committee . Unified Parkinson’s Disease Rating Scale. In: Fahn S, Marsden CD, Goldstein M, Calne DB, eds. Recent Developments in Parkinson’s Disease. Florham Park, NJ: Macmillan Healthcare Information; 1987:153-163. [Google Scholar]
- 13.Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology. 1967;17(5):427-442. [DOI] [PubMed] [Google Scholar]
- 14.Schwab R, England A. Projection technique for evaluating surgery in Parkinson’s disease. In: Gillingham F, Donaldson I, eds. Third Symposium on Parkinson’s Disease. Edinburgh, Scotland: E&S Livingstone, 1969:152-157. [Google Scholar]
- 15.Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695-699. [DOI] [PubMed] [Google Scholar]
- 16.Diggle P, Heagerty P, Liang K-Y, Zeger Sl. Analysis of Longitudinal Data. New York, NY: Oxford University Press; 2002. [Google Scholar]
- 17.Laird NM, Ware JH. Random-effects models for longitudinal data. Biometrics. 1982;38(4):963-974. [PubMed] [Google Scholar]
- 18.Tomlinson CL, Stowe R, Patel S, Rick C, Gray R, Clarke CE. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord. 2010;25(15):2649-2653. [DOI] [PubMed] [Google Scholar]
- 19.Zadikoff C, Fox SH, Tang-Wai DF, et al. A comparison of the Mini Mental State Exam to the Montreal Cognitive Assessment in identifying cognitive deficits in Parkinson’s disease. Mov Disord. 2008;23(2):297-299. [DOI] [PubMed] [Google Scholar]
- 20.Nazem S, Siderowf AD, Duda JE, et al. Montreal Cognitive Assessment performance in patients with Parkinson’s disease with “normal” global cognition according to Mini-Mental State Examination score. J Am Geriatr Soc. 2009;57(2):304-308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hoops S, Nazem S, Siderowf AD, et al. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology. 2009;73(21):1738-1745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cox DR. Regression models and life-tables. J R Stat Soc B. 1972;34(2):187-220. [Google Scholar]
- 23.Jankovic J, Kapadia AS. Functional decline in Parkinson disease. Arch Neurol. 2001;58(10):1611-1615. [DOI] [PubMed] [Google Scholar]
- 24.Goetz CG, Stebbins GT, Blasucci LM. Differential progression of motor impairment in levodopa-treated Parkinson’s disease. Mov Disord. 2000;15(3):479-484. [DOI] [PubMed] [Google Scholar]
- 25.Schrag A, Dodel R, Spottke A, Bornschein B, Siebert U, Quinn NP. Rate of clinical progression in Parkinson’s disease: a prospective study. Mov Disord. 2007;22(7):938-945. [DOI] [PubMed] [Google Scholar]
- 26.Bonifati V. LRRK2 low-penetrance mutations (Gly2019Ser) and risk alleles (Gly2385Arg)—linking familial and sporadic Parkinson’s disease. Neurochem Res. 2007;32(10):1700-1708. [DOI] [PubMed] [Google Scholar]
- 27.Marder K, Wang Y, Alcalay RN, et al. ; LRRK2 Ashkenazi Jewish Consortium . Age-specific penetrance of LRRK2 G2019S in the Michael J. Fox Ashkenazi Jewish LRRK2 Consortium. Neurology. 2015;85(1):89-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wang C, Cai Y, Zheng Z, et al. ; Chinese Parkinson Study Group (CPSG) . Penetrance of LRRK2 G2385R and R1628P is modified by common PD-associated genetic variants. Parkinsonism Relat Disord. 2012;18(8):958-963. [DOI] [PubMed] [Google Scholar]
- 29.Marras C, Alcalay RN, Caspell-Garcia C, et al. ; LRRK2 Cohort Consortium . Motor and nonmotor heterogeneity of LRRK2-related and idiopathic Parkinson’s disease. Mov Disord. 2016;31(8):1192-1202. [DOI] [PubMed] [Google Scholar]
- 30.Simón-Sánchez J, Martí-Massó JF, Sánchez-Mut JV, et al. Parkinson’s disease due to the R1441G mutation in Dardarin: a founder effect in the Basques. Mov Disord. 2006;21(11):1954-1959. [DOI] [PubMed] [Google Scholar]
- 31.von Coelln R, Shulman LM. Clinical subtypes and genetic heterogeneity: of lumping and splitting in Parkinson disease. Curr Opin Neurol. 2016;29(6):727-734. [DOI] [PubMed] [Google Scholar]
- 32.Fereshtehnejad S-M, Romenets SR, Anang JB, Latreille V, Gagnon J-F, Postuma RB. New clinical subtypes of Parkinson disease and their longitudinal progression: a prospective cohort comparison with other phenotypes. JAMA Neurol. 2015;72(8):863-873. [DOI] [PubMed] [Google Scholar]
- 33.Mirelman A, Gurevich T, Giladi N, Bar-Shira A, Orr-Urtreger A, Hausdorff JM. Gait alterations in healthy carriers of the LRRK2 G2019S mutation. Ann Neurol. 2011;69(1):193-197. [DOI] [PubMed] [Google Scholar]
- 34.Thaler A, Helmich RC, Or-Borichev A, et al. ; LRRK2 Ashkenazi Jewish Consortium . Intact working memory in non-manifesting LRRK2 carriers—an fMRI study. Eur J Neurosci. 2016;43(1):106-112. [DOI] [PubMed] [Google Scholar]
- 35.Halliday GM, McCann H. The progression of pathology in Parkinson’s disease. Ann N Y Acad Sci. 2010;1184(1):188-195. [DOI] [PubMed] [Google Scholar]
- 36.Compta Y, Parkkinen L, O’Sullivan SS, et al. Lewy- and Alzheimer-type pathologies in Parkinson’s disease dementia: which is more important? Brain. 2011;134(pt 5):1493-1505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kalia LV, Lang AE, Hazrati LN, et al. Clinical correlations with Lewy body pathology in LRRK2-related Parkinson disease. JAMA Neurol. 2015;72(1):100-105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Gaig C, Martí MJ, Ezquerra M, Rey MJ, Cardozo A, Tolosa E. G2019S LRRK2 mutation causing Parkinson’s disease without Lewy bodies. J Neurol Neurosurg Psychiatry. 2007;78(6):626-628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Saunders-Pullman R, Alcalay RN, Mirelman A, et al. ; AJ LRRK2 Consortium . REM sleep behavior disorder, as assessed by questionnaire, in G2019S LRRK2 mutation PD and carriers. Mov Disord. 2015;30(13):1834-1839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pont-Sunyer C, Iranzo A, Gaig C, et al. Sleep disorders in parkinsonian and nonparkinsonian LRRK2 mutation carriers. PLoS One. 2015;10(7):e0132368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Trinh J, Amouri R, Duda JE, et al. Comparative study of Parkinson’s disease and leucine-rich repeat kinase 2 p.G2019S parkinsonism. Neurobiol Aging. 2014;35(5):1125-1131. [DOI] [PubMed] [Google Scholar]
- 42.Marras C, Rochon P, Lang AE. Predicting motor decline and disability in Parkinson disease: a systematic review. Arch Neurol. 2002;59(11):1724-1728. [DOI] [PubMed] [Google Scholar]
- 43.Alves G, Wentzel-Larsen T, Aarsland D, Larsen JP. Progression of motor impairment and disability in Parkinson disease: a population-based study. Neurology. 2005;65(9):1436-1441. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable. Models Comparing Rate Change in UPDRS III, MoCA, and H&Y; LRRK2 PD vs IPD (Among Participants With ≥ 2 Visits)
eFigure 1. Longitudinal Trajectories of Mean UPDRS III Scores in LRRK2 PD Compared With IPD Restricted to Those With at Least Two Visits
eFigure 2. Longitudinal Trajectories of MoCA Scores in LRRK2 PD Compared With IPD Restricted to Those With at Least Two Visits
eFigure 3. Longitudinal Trajectories of Mean UPDRS III Scores in LRRK2 PD Compared With IPD Among Those With 20 Years of Disease or Less: Mean Trajectories From Models Restricted to Disease Duration ≤ 20 Years
eFigure 4. Longitudinal Trajectories of MoCA Scores in LRRK2 PD Compared With IPD Among Those With 20 Years of Disease or Less
eFigure 5. Spaghetti Plots Demonstrating Change in UPDRS III Scores Relative to Time Since Baseline in LRRK2 PD and IPD