

Abstract
Background
Ambient and home exposure to nitrogen dioxide (NO2) causes asthma symptoms and decreased lung function in children with asthma. Little is known about the health effects of school classroom pollution exposure.
Objective
We aimed to determine the effect of indoor classroom NO2 on lung function and symptoms of inner-city schoolchildren with asthma.
Methods
Children enrolled in the School Inner City Asthma Study were followed for one academic year. Subjects performed spirometry and fractional exhaled nitric oxide (FeNO) twice during the school year, at school. Classroom NO2 was collected by passive sampling for 1 week periods, twice per year coinciding with lung function testing. Generalized estimating equation models assessed lung function and symptom relationships with the temporally nearest classroom NO2 level.
Results
NO2 mean values were 11.1ppb (range 4.3 – 29.7ppb). In total, exposure data was available for 296 subjects; 188 with complete spirometry data. Above a threshold of 8ppb NO2, and after adjusting for race and season (spirometry standardized by age, height, and gender), NO2 was highly associated with airflow obstruction such that each 10ppb rise in NO2 was associated with a 5% decline in FEV1/FVC (β: −0.05, 95% confidence interval (CI) [−0.08, −0.02], p=0.01). FEF25-75% predicted was also inversely associated with higher NO2 exposure (β: −22.8, 95%CI [−36.0, −9.7], p=0.01). There was no significant association of NO2 with FEV1% predicted, FeNO or asthma symptoms. Additionally, there was no effect modification of atopy on lung function or symptom outcomes.
Conclusion
In children with asthma, indoor classroom NO2 may be associated with increased airflow obstruction.
Keywords: Asthma, indoor air pollution, obstructive lung disease, nitrogen dioxide, spirometry, exhaled nitric oxide
Introduction
Exposure to ambient air pollutants has been associated with asthma development, asthma exacerbations, and reduction in lung function1–8. Moreover, home-based measurements of nitrogen dioxide (NO2) and other pollutants with indoor sources have been associated with asthma symptom severity9 and lower lung function2, 10, 11 in children, even at modest levels of exposure10.
NO2, a gaseous pollutant generated from fossil fuel combustion, has emerged as one of the most notable pollutants associated with health effects. In urban environments NO2 is generated by traffic related combustion, home heating and cooking with fossil fuels (gas, oil, coal), and tobacco smoke12, 13. It is a prevalent indoor pollutant in homes, where heating and cooking are common activities, and during these exposures asthma symptoms worsen 11, 14. However, little is known about the effect of NO2 in indoor environments aside from the home.
Urban schools represent a unique and important microenvironment for indoor pollution. In most schools, there is no cooking, tobacco smoke is prohibited, and the centralized furnace system minimizes the combustion exposure to any individual classroom. However, exposure to combustion-related pollutants from outside sources may enter through traditional ventilation and intrusion through doors, windows and structural imperfections of the school building. The school classroom represents the occupational setting for children, the environment in which they spend 6–10 hours per day. Therefore, exposures encountered in this environment may have a substantial health effect.
Several studies have cataloged indoor air quality in schools15–19 and associations with respiratory19–21 and neurodevelopmental measures22. However, variation in source and type of pollutants varies significantly by geographic region16 and few studies have focused on US inner city schools23. Furthermore, few studies have specifically evaluated lung function in relation to the school based exposure24. In this study, we examine the symptomatic effects of NO2 and objective assessment of lung function in inner city children with asthma.
We hypothesized that exposure to NO2 in schools would be associated with lung function deficits and higher rates of asthma symptoms in children with asthma.
Methods
Study Population
The School Inner City Asthma Study (SICAS) is a single center epidemiologic study of the effect of school classroom environmental exposures on asthma morbidity in inner city school children with asthma. Methods have been previously published25. Briefly, children with asthma were recruited from inner city school classrooms from 2008 – 2013 for participation. Screening surveys were distributed school-wide to participating schools the spring prior to the study year. Children with a physician’s diagnosis of asthma or with report of signs and symptoms consistent with persistent asthma, and at least one asthma symptom within the past year were invited to participate. This study was approved by the Boston Children’s Hospital institutional review board. Written informed consent was obtained from the subject’s guardian and assent was obtained from the subject prior to enrollment.
Study procedures
Figure 1 illustrates the study schema. Baseline characterization of study subjects was performed at a formal research clinic visit during the summer prior to the academic year in which sociodemographic information, medical history and baseline symptom profiles were assessed by questionnaire. Subjects performed spirometry with a Koko spirometer (Ferraris Respiratory, Louisville, CO) using ATS guidelines26, Fractional exhaled nitric oxide (FeNO) with the Niox Mino device (Aerocrine, Solna, Sweden) and aeroallergen sensitization testing by allergy skin testing (MultiTest device, Lincoln Diagnostics, Decatur, IL) and/or serum specific IgE (ImmunoCAP, Phadia AB, Uppsala, Sweden). Sensitization was defined by a wheal 3 mm or larger than the negative saline control on skin prick testing or a specific-IgE level of 0.35 kU/L or greater. The tested allergens included tree pollen, grass, ragweed, dust mites, cat, dog, mouse, rat, cockroach, and molds (Greer, Lenoir, NC).
Figure 1.
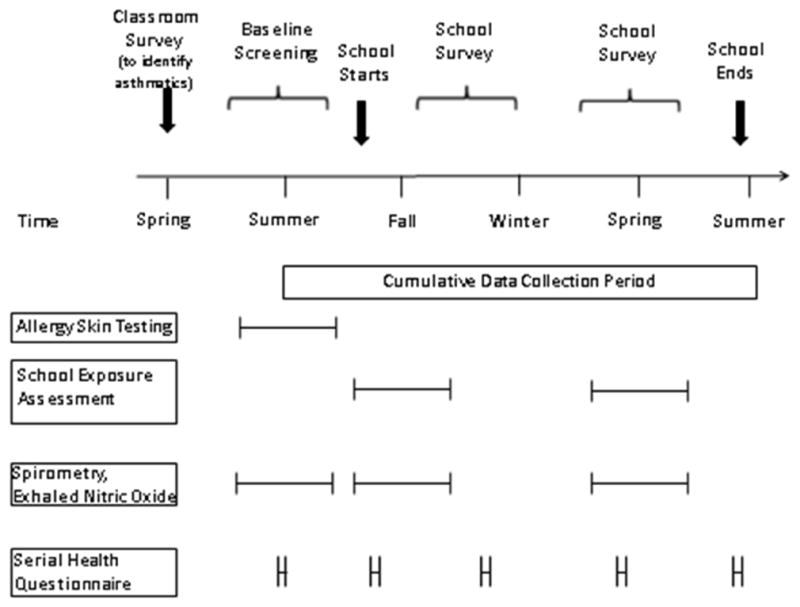
Schema of Assessments in the School Inner City Asthma Study
Subsequently, questionnaire based symptom assessments were performed up to 4 times throughout the academic school year by telephone interviews at 3,6,9, and 12 months. Spirometry and FeNO was assessed at two in-school visits that coincided with school environmental assessments, approximately 6 months apart. Testing occurred throughout the day with 90% of tests occurring after 10am, and the majority occurring between 10am and 3PM.
Exposure assessment
Classrooms of participating students were sampled twice during the academic yearwhile school was in session, approximately 6 months apart. NO2 was collected via passive monitoring with Ogawa samplers27 for 1 week periods. NO2 analysis was performed using ion chromatography. Average NO2 levels per assessment period were determined and used for analyses.
Outcome measures
The ratio of forced expiratory volume in 1 second (FEV1) per forced vital capacity ratio (FEV1/FVC) was chosen as the primary spirometric outcome of interest because it is the most sensitive marker of airflow obstruction in children with asthma28, 29. FEV1 percent predicted, FVC percent predicted and the forced expiratory flow rate between the 25th and 75th percent of FVC (FEF25-75), a measure of medium and small caliber airways, were also assessed. All spirometry measures were assessed for acceptability and repeatability by study physicians per ATS guidelines26, 30. Reference values were derived from the NHANES III31 reference equations which account for age, race, and gender. FeNO was measured per standardized methodology. Both spirometry and FeNO measurements were performed in the school during the same season (fall or spring) of exposure measurement.
Symptom outcomes were measured as maximum symptom days, as used in prior urban home-based studies32, 33 and school studies34, 35. To define this outcome, three variables of symptoms in the 2 weeks prior to each survey were evaluated: (a) number of days with wheezing, chest tightness, or cough, (b) number of days on which child had to slow down or discontinue play activities due to wheezing, chest tightness, or cough, or (c) number of nights with wheezing, chest tightness, or cough leading to disturbed sleep. The greatest result of these three variables was used as the asthma symptom days outcome. As such, this outcome was a score from 0–14 days.
Statistical analysis
Characteristics of the cohort are expressed with descriptive statistics. Variability of NO2 levels between schools and between classrooms within schools was determined with random effects linear regression. All clinical outcomes were linked to the temporally closest measured exposure during the academic school year. Only outcome measures obtained during the academic school year were used for analysis. The relationship between NO2 and lung function testing was evaluated with locally weighted regression (Lowess) to examine possible non-linear relationships. Based on these smoothers, we then fit a linear spline of NO2 with a single knot at 8ppb to be used in all subsequent models. Relationships between NO2 and the lung function outcomes are presented as the effect of a 10ppb change in NO2 above the threshold of 8ppb. The exposure-outcome relationship was evaluated using generalized estimating equations (GEE) with an exchangeable correlation structure, robust variance estimates, with clustering defined at the participant level. We considered clustering at the school level in addition to the participant level within a multilevel random effects model containing both subject and school random effects, but this was deemed unnecessary because there was little to no between school variability in all outcomes (intra-class correlations between 0.00 and 0.04). All models included linear and quadratic terms for the number of days since school started to address the time variation of asthma activity across the study period. Symptom outcomes were adjusted for age, race, and gender due to a priori assumptions that these may be important confounders. Age and gender were part of the NHANES III reference equations and so were not used as further adjustment for spirometry outcomes. Binomial family GEEs with a logit link and an overdispersion parameter were used for two-week outcomes (i.e., two-week outcomes were modeled as the sum of 14 binomial “successes”). Spirometry and FeNO were modeled using Gaussian family and identity link. Potential confounders that were not included in models due to a lack of association with the NO2 (P>0.1) included vacuumed dust mouse allergen and endotoxin from the classrooms, income, environmental tobacco smoke (ETS) exposure, Body Mass Index (BMI), time (hour of the day) of lung function testing, and use of asthma controller medication at baseline visit.
A term for “Any Sensitization” was created to indicate subjects with ≥1 sensitization by skin prick test or specific IgE >0.35 kU/L at baseline assessment. Based on prior literature, any sensitization was examined as a potential moderator of the NO2 effects on asthma morbidity. Post-hoc analysis stratified by sensitization status was performed to further evaluate main effects by group. Statistical computations were performed using STATA software, version 13.1 (StataCorp). All tests were 2-tailed, and P < .05 was considered significant.
Results
In total, 296 participants had assessments of classroom NO2 and were included in the analysis. Subjects were predominantly Black or Hispanic and 49% were from impoverished households (Table 1). Baseline lung function was normal and non-obstructed.
Table 1.
Characteristics of Study Population.
| Characteristic | No. (%) |
|---|---|
| Demographic | |
| Age, median (range), | 8 (4–13) |
| Female sex | 143 (48) |
| Race or ethnic group | |
| White | 13 (4) |
| Black | 102 (34) |
| Hispanic | 107 (36) |
| Mixed race | 52 (18) |
| Other | 22 (7) |
| Annual income<$25,000 | 120 (49) |
| Pulmonary Testinga | |
| FVC% predicted, mean (SD) | 98 (15.5) |
| FEV1% predicted, mean (SD) | 100 (17.9) |
| FEV1/FVC, mean (SD) | 0.87 (0.08) |
| FEF25-75% predicted, mean (SD) | 118 (103.2) |
| FeNO, ppb, Mean (SD) (n=73) | 19.6 (20.9) |
| Allergy sensitization ≥ 1 allergen | 197 (69) |
| Maximum symptom daysb, mean (sd) | 3.0 (4.2) |
| Controller medication over prior 12 months | 167 (56%) |
| Environmental tobacco smoke exposure | 97 (33%) |
n=188 for pulmonary testing
Maximum symptom days = the greatest result of the following three variables in the 2 weeks prior to each follow-up survey: 1) number of days with wheezing, chest tightness, or cough 2) number of days on which child had to slow down or discontinue play activities due to wheezing, chest tightness, or cough 3) number of nights with wheezing, chest tightness, or cough leading to disturbed sleep.
FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; FEF25-75: forced expiratory flow between the 25th and 75th percent of FVC; FeNO: fractional exhaled Nitric Oxide.
NO2 was measured in 218 classrooms across 37 schools. Mean NO2 levels were 11.1ppb, median 10.4ppb, and range 4.3 to 29.7ppb. Figure 2 shows the distribution of NO2 by school for fall and spring measurements, demonstrating the variability between classrooms within schools and between schools for the spring season. School to school variability accounted for 75% of the variance in NO2 measures, leaving 25% of the variability attributable to the classroom level.
Figure 2.

Distribution of NO2 concentrations by school, by season. X axis represents each individual school, number of subjects attending each school is in parentheses (). Box and whiskers plots represent the distribution of NO2 across multiple classrooms within each school. Box parameters are the IQR, hash mark is the median, whiskers extend to 1.5 times the IQR above the 75th and below the 25th percentile.
One hundred eighty eight participants had complete data for NO2 and acceptable spirometry for analysis. In adjusted analyses, NO2 exposure above 8ppb was significantly associated with airflow obstruction as measured by FEV1/FVC ratio and FEF25-75, a measure of small airways dysfunction. For each 10ppb increase in NO2, there was a 5% decline in FEV1/FVC ratio with ratios crossing the clinically relevant normal value for FEV1/FVC ratio of 0.85 36 at approximately 16ppb of NO2 (Table 2; unadjusted correlations can be found in supplementary table 1 in the online repository). Figure 3 depicts the relationship between NO2 level and FEV1/FVC ratio within the range of our data. Allergic sensitization did not modify the effect of this association (p=0.55 for the interaction). However, in post-hoc stratified analysis, non-atopic children demonstrated a decreased FEV1% predicted in association with NO2 exposure whereas atopic subjects did not (see supplementary table 2 in the online repository). There was a 22.8% decline in FEF25-75 for each 10ppb increase in NO2. While FEV1 and FVC percent predicted were negatively associated with NO2 exposure, associations were not significant at P<0.05. There was no significant association of NO2 with FeNO, a measure of airway inflammation, which was also measured at the time of exposure assessment.
Table 2.
Effect of NO2 above 8ppb on spirometry and asthma outcomes in school age children with asthma
| Univariate model | Multivariate modelb | |||
|---|---|---|---|---|
| Odds ratio | 95% Confidence interval (CI) | Odds ratio | 95% Confidence interval (CI) | |
| Maximum Symptom Daysa | 1.31 | 0.90, 1.90 | 1.15 | 0.80, 1.64 |
| Beta | 95% CI | Beta | 95% CI | |
| FEV1/FVC | −0.049* | −0.077, −0.021 | −0.049* | −0.078, −0.021 |
| FEV1% | −5.5 | −12.0, 0.9 | −5.5 | −11.7, 0.8 |
| FVC% | −0.7 | −5.8, 4.4 | −0.5 | −5.5, 4.5 |
| FEF25-75% | −22.8* | −36.0, −9.7 | −22.8* | −36.0, −9.7 |
| FeNO | 3.5 | −6.9, 13.9 | −0.5 | −12.0, 11.0 |
Maximum symptom days = the greatest result of the following three variables in the 2 weeks prior to each follow-up survey: 1) number of days with wheezing, chest tightness, or cough; 2) number of days on which child had to slow down or discontinue play activities due to wheezing, chest tightness, or cough, and; 3) number of nights with wheezing, chest tightness, or cough leading to disturbed sleep;
Multivariate model: Maximum symptom days adjusted for Age, Race, Gender and season; spirometry and FeNO adjusted for race and time. Results scaled to each 10 ppb increment of NO2 above 8ppb.
p-value = 0.001.
FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; FEF25-75: forced expiratory flow between the 25th and 75th percent of FVC; FeNO: fractional exhaled Nitric Oxide.
Figure 3.

Effect of classroom NO2 on FEV1/FVC. Association of NO2 and FEV1/FVC using piecewise linear regression with breakpoint at NO2 level of 8ppb. Shaded area represents 95% confidence intervals.
There was no significant association of NO2 exposure with maximum symptom days, the main symptom-based outcome (Table 2). Additionally, allergic sensitization did not modify the relationship between NO2 and asthma symptoms (p=0.59 for the interaction).
Discussion
In this study, we demonstrate a temporally distinct association of school classroom measured NO2 with airflow obstruction in inner city school children with asthma. As children spend the majority of their day in the school environment, this microenvironment for potential respiratory insults is equivalent to an occupational exposure in adults.
There are several important findings highlighted by these analyses. First, the levels of NO2 detected in the classrooms were relatively low compared to the US Environmental Protection Agency national ambient air quality standards for NO2 currently set at a 1 hour maximum level of 100ppb and annual average level of 53ppb37. Despite overall low levels, there was a clear signal of lung function impairment and a trend toward more symptoms associated with higher NO2 exposures in this vulnerable pediatric population. This finding complements work by Belanger et al.10 who found respiratory health effects at relatively low home levels of NO2 and Pilotto and colleagues15 who found health effects of NO2 in Australian school classrooms with unflued gas heaters, though the exposure in our school classrooms was far less. In sum, this suggests that there is a concentration – response relationship of NO2 that adversely affects health at levels below existing standards, especially in vulnerable populations. Furthermore, our data indicate a threshold level at which physiologic effects of NO2 may occur in children with asthma. To our knowledge, this has not been previously demonstrated in other studies, which may be a reflection of our unique study design measuring levels in schools of asthmatic children– where there is no cooking, smoking, or other immediate sources of NO2 emissions, so that the range of our data was able to elicit this level of detail. Interventional exposure studies typically use high concentrations of NO2 for short periods of time which may not elicit the same responses as prolonged exposure to lower levels38. It may also be due to differences in statistical methodology in used to evaluate non-linear associations between NO2 and respiratory outcomes39.
Second, we did not find any interaction between NO2 exposure and atopy, measured by specific sensitization to a battery of common aeroallergens, in relation to asthma outcomes. Furthermore, there was no association between NO2 exposure and FeNO, a marker of allergic airway inflammation. While some prior studies have found that air pollution differentially affects allergen sensitized children with asthma40–43, others have found that non-atopic children are more affected11. While our stratified analysis did find a significant association between NO2 and FEV1% in non-sensitized subject, this does not reflect a significant difference between the atopic and non-atopic groups in response to the exposure, which is reflected by the lack of significant interaction term. Our finding, that the relationship of NO2 and airflow obstruction is not modified by allergic sensitization, suggests that it may influence lung function through a direct effect on the respiratory epithelium and smooth muscle by induction of oxidative stress and non-allergic inflammation. Previous literature on the biologic effects of NO2 support the stimulation of innate immune responses rather than the TH2 driven inflammation more characteristic of asthma44, 45. Human exposure studies demonstrate bronchial washings enriched for IL6, IL8, neutrophilic infiltration and acute phase reactions within 24 hours of NO2 inhalant exposure45. Simultaneously, oxidative stress induction as evidenced by increased HMOX1 gene expression following NO2 exposure to human bronchial epithelial cells is also likely to play a significant role44, 46. Summation of these study results with the current epidemiologic findings of our study suggest that respiratory effects caused by inhalation of NO2 are not mediated by the TH2 inflammatory paradigm that is primarily implicated in pediatric asthma.
Third, we found significant variability in NO2 levels between schools that were not seasonally dependent. The school microenvironment, particularly the school classroom, is unique in that there are few indoor sources of NO2. Primary sources of indoor combustion leading to elevated levels of NO2 in homes include home heating and cooking and cigarette smoking. Among the schools included in this study, there was only one with a kitchen that cooked food for lunches and all prohibited smoking on school property. Similarly, the effect of a central furnace heating multiple classrooms – when the heat is on – is unlikely to account for significant classroom to classroom variation in NO2 exposure. In this case, differences in NO2 levels between classrooms and between schools likely represent variable penetration and ventilation of outdoor generated ambient gases through the school classroom envelope along with local differences in traffic related emissions near each school. Similar associations of inner city school measures of NO2 were reported by Rivas et al. in the BREATHE study of indoor pollutants in Barcelona, Spain17. These are potentially modifiable school classroom characteristics that may be amenable to remediation of structural imperfections, ventilation systems, or altering local traffic patterns.
The association of classroom NO2 level with asthma symptoms was suggestive of a positive relationship but did not reach statistical significance. The lack of precision of the effect estimates may, in part, be due to exposure misclassification. By the nature of the study design, lung function testing was carried out at the time exposure measurement devices were deployed in the schools, twice per year; however, symptom outcomes were collected by phone on a quarterly basis and not necessarily in close temporal relation to the exposure measure. As such, the temporal variability significantly limits the ability to find acute health effects on asthma symptoms related to the exposure. A larger sample size may have elicited a significant long-term relationship between exposure and outcome that was not found here. It is also possible that NO2 found in classrooms is a marker for other, unmeasured, pollutants produced by the same processes or for other pollutants chemically related to NO2, such as ozone (O3) or particulate matter. While this is possible, NO2 is known to be associated with biologically plausible mechanisms to induce airway inflammation44, hyper-responsiveness and airflow obstruction2 in its own right. Our data is limited in the ability to tease apart NO2 from other co-pollutants that may also be present. Additionally, unmeasured confounding factors, such as viral URIs or specific characteristics influencing susceptibility to the exposure, may have influenced our results. However, we attempted to address any seasonal variation in asthma morbidity, such as viral seasons, by including a variable for time in each analytical model, and known factors related to asthma morbidity, such as low socioeconomic status and environmental tobacco smoke, among others, were evaluated as potential confounders. Notably, time was not significantly associated with lung function or asthma symptoms within our models. Finally, our exposure measure is an average of NO2 collected over a one-week timeframe, which limits our ability to determine the potential effect of peak levels and our ability to specify the personal exposure during school hours only. As such, this runs the risk of some element of exposure misclassification, which may have biased our findings toward the null. Despite this, we found compelling evidence linking exposure to decrements in lung function.
Additional evidence to support the association between NO2 and health effects exists in the form of few interventional studies in schools with high pollution levels due to poor venting of furnaces20. In population-based studies, ambient NO2 has been associated with the development of childhood asthma47 and asthma exacerbations requiring emergency services48, as well as abnormal lung function testing in asthmatic cohorts49. Modeled assessments of effects and benefits of reducing NO2 near primary schools in London indicate that a significant improvement in the number of childhood asthma exacerbations, costs to schools, and costs to parents, would be achieved by lowering exposure50.
In conclusion, we demonstrate that exposure to NO2 in the school classroom microenvironment is significantly related to airflow limitation in children with asthma, through a pathway that is not dependent on allergy nor production of allergic inflammation. Intervention studies are needed to determine whether reducing inhaled pollutants in the school environment may produce health benefits for vulnerable populations of children.
Supplementary Material
Clinical implications.
Nitrogen dioxide in the urban school environment is associated with airflow obstruction in children with asthma. Environmental interventions at schools may improve the health of children with asthma.
Acknowledgments
Funding source: This study was supported by NIH grants K23AI106945 (PI Gaffin), R01 AI 073964, R01AI 073964-02S1, K24 AI 106822, U01 AI 110397, U10HL098102 (PI: Phipatanakul), NIH-NIEHS K23ES023700 (PI Lai), K23AI104780 (PI Sheehan), P01 ES009825, and P30ES000002 (Gold). This study was also supported by EPA center grants RD-834798 and RD-83587201. This work was conducted with support from Harvard Catalyst | The Harvard Clinical and Translational Science Center (National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health Award UL1 TR001102) and financial contributions from Harvard University and its affiliated academic healthcare centers. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University and its affiliated academic healthcare centers, or the National Institutes of Health. This publication was also made possible by US Environmental Protection Agency (USEPA) grant RD-83479801 and was also funded (in part) by the cooperative agreement award number FAIN: U61TS000237 from the Agency for Toxic Substances and Disease Registry (ATSDR). The USEPA supports the Pediatric Environmental Health Specialty Units by providing partial funding to the ATSDR under Inter-Agency Agreement number DW-75-92301301. Its contents are solely the responsibility of the grantee and do not necessarily represent the official views of the ATSDR or USEPA. Further, USEPA or ATSDR do not endorse the purchase of any commercial products or services mentioned in the publication. Additional acknowledgment to The Allergy and Asthma Awareness Initiative, Inc. We thank the following companies for their generous donations. Lincoln Diagnostics, Inc., Decatur, IL, USA, Multi-Test II devices; Greer, Inc, Lenoir, NC allergenic extracts for skin testing; Thermo Fisher, Inc. ImmunoCAP® testing; Monaghan Medical, Inc aerochambers; Aeorcrine, Inc., NiOx Machines.
We are thankful for the thoughtful guidance provided by Sachin Baxi, Perdita Permaul, and Lisa Bartnikas, and for the study staff, participants and families who contributed to this research.
Abbreviations
- NO2
Nitrogen dioxide
- FEV1
forced expiratory volume in 1 second
- FVC
forced vital capacity
- FEF25-75
forced expiratory flow between the 25th and 75th percent of forced vital capacity
- FeNO
Fractional exhaled nitric oxide
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Franklin PJ. Indoor air quality and respiratory health of children. Paediatr Respir Rev. 2007;8:281–6. doi: 10.1016/j.prrv.2007.08.007. [DOI] [PubMed] [Google Scholar]
- 2.O’Connor GT, Neas L, Vaughn B, Kattan M, Mitchell H, Crain EF, et al. Acute respiratory health effects of air pollution on children with asthma in US inner cities. J Allergy Clin Immunol. 2008;121:1133–9. e1. doi: 10.1016/j.jaci.2008.02.020. [DOI] [PubMed] [Google Scholar]
- 3.Brunekreef B. Health effects of air pollution observed in cohort studies in Europe. J Expo Sci Environ Epidemiol. 2007;17(Suppl 2):S61–5. doi: 10.1038/sj.jes.7500628. [DOI] [PubMed] [Google Scholar]
- 4.Rice MB, Rifas-Shiman SL, Oken E, Gillman MW, Ljungman PL, Litonjua AA, et al. Exposure to traffic and early life respiratory infection: A cohort study. Pediatr Pulmonol. 2014 doi: 10.1002/ppul.23029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Litonjua AA, Gold DR. Early-Life Exposures and Later Lung Function. Add Pollutants to the Mix. Am J Respir Crit Care Med. 2016;193:110–1. doi: 10.1164/rccm.201510-1963ED. [DOI] [PubMed] [Google Scholar]
- 6.Ierodiakonou D, Zanobetti A, Coull BA, Melly S, Postma DS, Boezen HM, et al. Ambient air pollution, lung function, and airway responsiveness in asthmatic children. J Allergy Clin Immunol. 2016;137:390–9. doi: 10.1016/j.jaci.2015.05.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Habre R, Moshier E, Castro W, Nath A, Grunin A, Rohr A, et al. The effects of PM2.5 and its components from indoor and outdoor sources on cough and wheeze symptoms in asthmatic children. J Expo Sci Environ Epidemiol. 2014;24:380–7. doi: 10.1038/jes.2014.21. [DOI] [PubMed] [Google Scholar]
- 8.Neophytou AM, White MJ, Oh SS, Thakur N, Galanter JM, Nishimura KK, et al. Air Pollution and Lung Function in Minority Youth with Asthma in the GALA II (Genes-Environments and Admixture in Latino Americans) and SAGE II (Study of African Americans, Asthma, Genes, and Environments) Studies. Am J Respir Crit Care Med. 2016;193:1271–80. doi: 10.1164/rccm.201508-1706OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Belanger K, Holford TR, Gent JF, Hill ME, Kezik JM, Leaderer BP. Household levels of nitrogen dioxide and pediatric asthma severity. Epidemiology. 2013;24:320–30. doi: 10.1097/EDE.0b013e318280e2ac. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Belanger K, Gent JF, Triche EW, Bracken MB, Leaderer BP. Association of indoor nitrogen dioxide exposure with respiratory symptoms in children with asthma. Am J Respir Crit Care Med. 2006;173:297–303. doi: 10.1164/rccm.200408-1123OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kattan M, Gergen PJ, Eggleston P, Visness CM, Mitchell HE. Health effects of indoor nitrogen dioxide and passive smoking on urban asthmatic children. J Allergy Clin Immunol. 2007;120:618–24. doi: 10.1016/j.jaci.2007.05.014. [DOI] [PubMed] [Google Scholar]
- 12.Asthma CotAo, Air I, Promotion DoH, Prevention D, Medicine Io. Clearing the Air:Asthma and Indoor Air Exposures. The National Academies Press; 2000. [Google Scholar]
- 13.Wallace LA, Mitchell H, O’Connor GT, Neas L, Lippmann M, Kattan M, et al. Particle concentrations in inner-city homes of children with asthma: the effect of smoking, cooking, and outdoor pollution. Environ Health Perspect. 2003;111:1265–72. doi: 10.1289/ehp.6135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hansel NN, Breysse PN, McCormack MC, Matsui EC, Curtin-Brosnan J, Williams DL, et al. A longitudinal study of indoor nitrogen dioxide levels and respiratory symptoms in inner-city children with asthma. Environ Health Perspect. 2008;116:1428–32. doi: 10.1289/ehp.11349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pilotto LS, Douglas RM, Attewell RG, Wilson SR. Respiratory effects associated with indoor nitrogen dioxide exposure in children. Int J Epidemiol. 1997;26:788–96. doi: 10.1093/ije/26.4.788. [DOI] [PubMed] [Google Scholar]
- 16.Mazaheri M, Reche C, Rivas I, Crilley LR, Alvarez-Pedrerol M, Viana M, et al. Variability in exposure to ambient ultrafine particles in urban schools: Comparative assessment between Australia and Spain. Environ Int. 2016;88:142–9. doi: 10.1016/j.envint.2015.12.029. [DOI] [PubMed] [Google Scholar]
- 17.Rivas I, Viana M, Moreno T, Pandolfi M, Amato F, Reche C, et al. Child exposure to indoor and outdoor air pollutants in schools in Barcelona, Spain. Environ Int. 2014;69:200–12. doi: 10.1016/j.envint.2014.04.009. [DOI] [PubMed] [Google Scholar]
- 18.Mi YH, Norback D, Tao J, Mi YL, Ferm M. Current asthma and respiratory symptoms among pupils in Shanghai, China: influence of building ventilation, nitrogen dioxide, ozone, and formaldehyde in classrooms. Indoor Air. 2006;16:454–64. doi: 10.1111/j.1600-0668.2006.00439.x. [DOI] [PubMed] [Google Scholar]
- 19.Smedje G, Norback D. New ventilation systems at select schools in Sweden--effects on asthma and exposure. Arch Environ Health. 2000;55:18–25. doi: 10.1080/00039890009603380. [DOI] [PubMed] [Google Scholar]
- 20.Pilotto LS, Nitschke M, Smith BJ, Pisaniello D, Ruffin RE, McElroy HJ, et al. Randomized controlled trial of unflued gas heater replacement on respiratory health of asthmatic schoolchildren. Int J Epidemiol. 2004;33:208–14. doi: 10.1093/ije/dyh018. [DOI] [PubMed] [Google Scholar]
- 21.McConnell R, Islam T, Shankardass K, Jerrett M, Lurmann F, Gilliland F, et al. Childhood incident asthma and traffic-related air pollution at home and school. Environ Health Perspect. 2010;118:1021–6. doi: 10.1289/ehp.0901232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sunyer J, Esnaola M, Alvarez-Pedrerol M, Forns J, Rivas I, Lopez-Vicente M, et al. Association between traffic-related air pollution in schools and cognitive development in primary school children: a prospective cohort study. PLoS Med. 2015;12:e1001792. doi: 10.1371/journal.pmed.1001792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gaffin JM, Petty CR, Hauptman M, Kang CM, Wolfson JM, Abu Awad Y, et al. Modeling indoor particulate exposures in inner-city school classrooms. J Expo Sci Environ Epidemiol. 2016 doi: 10.1038/jes.2016.52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zwozdziak A, Sowka I, Willak-Janc E, Zwozdziak J, Kwiecinska K, Balinska-Miskiewicz W. Influence of PM1 and PM2.5 on lung function parameters in healthy schoolchildren-a panel study. Environ Sci Pollut Res Int. 2016;23:23892–901. doi: 10.1007/s11356-016-7605-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Phipatanakul W, Bailey A, Hoffman EB, Sheehan WJ, Lane JP, Baxi S, et al. The school inner-city asthma study: design, methods, and lessons learned. J Asthma. 2011;48:1007–14. doi: 10.3109/02770903.2011.624235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–38. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- 27.Ogawa & Co. U, Inc. NO, NO2, NOx and SO2 Sampling Protocol Using The Ogawa Sampler. Ogawa & Co., USA, Inc; 2006. [Google Scholar]
- 28.Strunk RC, Weiss ST, Yates KP, Tonascia J, Zeiger RS, Szefler SJ, et al. Mild to moderate asthma affects lung growth in children and adolescents. J Allergy Clin Immunol. 2006;118:1040–7. doi: 10.1016/j.jaci.2006.07.053. [DOI] [PubMed] [Google Scholar]
- 29.Bacharier LB, Strunk RC, Mauger D, White D, Lemanske RF, Jr, Sorkness CA. Classifying asthma severity in children: mismatch between symptoms, medication use, and lung function. Am J Respir Crit Care Med. 2004;170:426–32. doi: 10.1164/rccm.200308-1178OC. [DOI] [PubMed] [Google Scholar]
- 30.Beydon N, Davis SD, Lombardi E, Allen JL, Arets HG, Aurora P, et al. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med. 2007;175:1304–45. doi: 10.1164/rccm.200605-642ST. [DOI] [PubMed] [Google Scholar]
- 31.Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159:179–87. doi: 10.1164/ajrccm.159.1.9712108. [DOI] [PubMed] [Google Scholar]
- 32.Busse WW, Morgan WJ, Gergen PJ, Mitchell HE, Gern JE, Liu AH, et al. Randomized trial of omalizumab (anti-IgE) for asthma in inner-city children. N Engl J Med. 2011;364:1005–15. doi: 10.1056/NEJMoa1009705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Morgan WJ, Crain EF, Gruchalla RS, O’Connor GT, Kattan M, Evans R, 3rd, et al. Results of a home-based environmental intervention among urban children with asthma. N Engl J Med. 2004;351:1068–80. doi: 10.1056/NEJMoa032097. [DOI] [PubMed] [Google Scholar]
- 34.Lai PS, Sheehan WJ, Gaffin JM, Petty CR, Coull BA, Gold DR, et al. School Endotoxin Exposure and Asthma Morbidity in Inner-city Children. Chest. 2015;148:1251–8. doi: 10.1378/chest.15-0098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Sheehan WJPP, Petty CR, Coull BA, Baxi SN, Gaffin JM, Lai PS, Gold DR, Phipatanakul W. Association Between Allergen Exposure in Inner-City Schools and Asthma Morbidity Among Students. JAMA Pediatrics. 2016 doi: 10.1001/jamapediatrics.2016.2543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.EPR3 NN. Guidelines for the Diagnosis and Management of Asthma. NIH; 2007. [Google Scholar]
- 37.Fact Sheets and Additional Information Regarding the 2010 Revision to the Primary National Ambient Air Quality Standards (NAAQS) for Nitrogen Dioxide (NO2) 2010 Available from https://www.epa.gov/no2-pollution/fact-sheets-and-additional-information-regarding-2010-revision-primary-national.
- 38.Ezratty V, Guillossou G, Neukirch C, Dehoux M, Koscielny S, Bonay M, et al. Repeated nitrogen dioxide exposures and eosinophilic airway inflammation in asthmatics: a randomized crossover study. Environ Health Perspect. 2014;122:850–5. doi: 10.1289/ehp.1307240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Gillespie-Bennett J, Pierse N, Wickens K, Crane J, Howden-Chapman P. The respiratory health effects of nitrogen dioxide in children with asthma. Eur Respir J. 2011;38:303–9. doi: 10.1183/09031936.00115409. [DOI] [PubMed] [Google Scholar]
- 40.Barck C, Sandstrom T, Lundahl J, Hallden G, Svartengren M, Strand V, et al. Ambient level of NO2 augments the inflammatory response to inhaled allergen in asthmatics. Respir Med. 2002;96:907–17. doi: 10.1053/rmed.2002.1374. [DOI] [PubMed] [Google Scholar]
- 41.Nitschke M, Pilotto LS, Attewell RG, Smith BJ, Pisaniello D, Martin J, et al. A cohort study of indoor nitrogen dioxide and house dust mite exposure in asthmatic children. J Occup Environ Med. 2006;48:462–9. doi: 10.1097/01.jom.0000215802.43229.62. [DOI] [PubMed] [Google Scholar]
- 42.Strand V, Rak S, Svartengren M, Bylin G. Nitrogen dioxide exposure enhances asthmatic reaction to inhaled allergen in subjects with asthma. Am J Respir Crit Care Med. 1997;155:881–7. doi: 10.1164/ajrccm.155.3.9117021. [DOI] [PubMed] [Google Scholar]
- 43.Viera L, Chen K, Nel A, Lloret MG. The impact of air pollutants as an adjuvant for allergic sensitization and asthma. Curr Allergy Asthma Rep. 2009;9:327–33. doi: 10.1007/s11882-009-0046-x. [DOI] [PubMed] [Google Scholar]
- 44.Mirowsky JE, Dailey LA, Devlin RB. Differential expression of pro-inflammatory and oxidative stress mediators induced by nitrogen dioxide and ozone in primary human bronchial epithelial cells. Inhal Toxicol. 2016;28:374–82. doi: 10.1080/08958378.2016.1185199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Devlin RB, Horstman DP, Gerrity TR, Becker S, Madden MC, Biscardi F, et al. Inflammatory response in humans exposed to 2.0 ppm nitrogen dioxide. Inhal Toxicol. 1999;11:89–109. doi: 10.1080/089583799197195. [DOI] [PubMed] [Google Scholar]
- 46.Ayyagari VN, Januszkiewicz A, Nath J. Effects of nitrogen dioxide on the expression of intercellular adhesion molecule-1, neutrophil adhesion, and cytotoxicity: studies in human bronchial epithelial cells. Inhal Toxicol. 2007;19:181–94. doi: 10.1080/08958370601052121. [DOI] [PubMed] [Google Scholar]
- 47.Gehring U, Wijga AH, Hoek G, Bellander T, Berdel D, Bruske I, et al. Exposure to air pollution and development of asthma and rhinoconjunctivitis throughout childhood and adolescence: a population-based birth cohort study. Lancet Respir Med. 2015;3:933–42. doi: 10.1016/S2213-2600(15)00426-9. [DOI] [PubMed] [Google Scholar]
- 48.Zheng XY, Ding H, Jiang LN, Chen SW, Zheng JP, Qiu M, et al. Association between Air Pollutants and Asthma Emergency Room Visits and Hospital Admissions in Time Series Studies: A Systematic Review and Meta-Analysis. PLoS One. 2015;10:e0138146. doi: 10.1371/journal.pone.0138146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ierodiakonou D, Zanobetti A, Coull BA, Melly S, Postma DS, Boezen HM, et al. Ambient air pollution, lung function, and airway responsiveness in asthmatic children. J Allergy Clin Immunol. 2016;137:390–9. doi: 10.1016/j.jaci.2015.05.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Guerriero C, Chatzidiakou L, Cairns J, Mumovic D. The economic benefits of reducing the levels of nitrogen dioxide (NO2) near primary schools: The case of London. J Environ Manage. 2016;181:615–22. doi: 10.1016/j.jenvman.2016.06.039. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.