

Introduction
Cut throat injuries are uncommon mode of committing suicides in Indian subcontinent. These injuries are usually superficial with multiple hesitation marks [1]. We hereby present a case of suicidal cut throat injury in a psychiatric patient with right internal jugular, tracheal and esophageal transection. Patient was successfully managed with primary vascular, tracheal and esophageal repairs following emergency room resuscitation. Such presentation of suicidal injuries is rare in terms of its mode and successful outcome and hence reported.
Case report
A 20 years old male was admitted to our emergency room in a state of shock and respiratory distress with a deep stab wound in his neck after attempting suicide. Patient had a history of being treated for major depression with poor follow up and drug compliance. As per the patient's sister who was the eye witness for the incident, suicide was committed using a sharp pointed kitchen knife which was stabbed by the patient in front and mid part of the neck. His vitals at the time of presentation were: pulse not palpable, blood pressure of 60/40 mm Hg, heart rate 150/min and undetectable saturation in extremities. A large hematoma was present over anterior aspect of neck. Tracheal end with air gushing was evident in between hematoma.
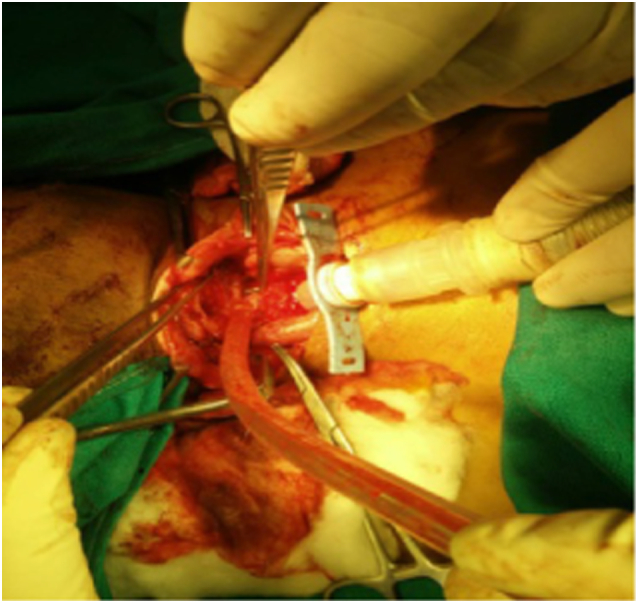
Emergency room resuscitation was started. Cervical spine was stabilized. Airway was secured using 7 Fr uncuffed tracheostomy tube which was inserted in the distal tracheal end by emergency trauma team (Fig. 1). Bilateral saphenous cut downs were done and intravenous crystalloids were started. Laceration in the neck was packed and patient was shifted to emergency operation theatre.
Fig. 1.

Showing airway management by 7 Fr tracheostomy tube inserted in the distal trachea and neck packed and pressurized to achieve hemostasis while the patient was shifted to operation theatre.
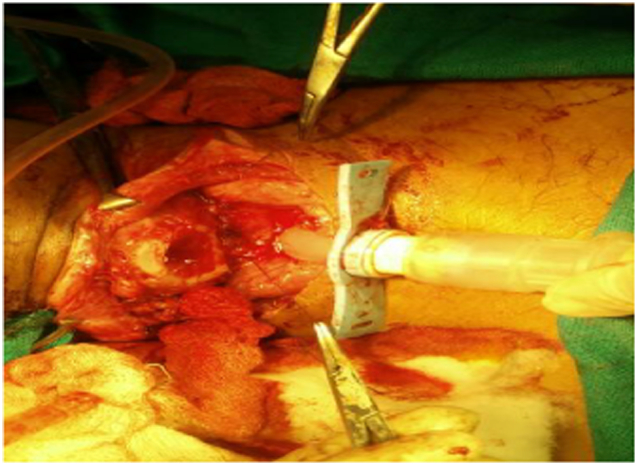
Emergency neck exploration was started by a team of surgeons under general anesthesia. Exploration of the neck revealed partial transection of the right internal jugular vein which was clamped and repaired using lateral prolene 6-O sutures. Hemostasis was achieved and tracheostomy tube was changed to 7.5 Fr cuffed tube for better ventilation. Vitals of the patient were stabilized by this time with intra-arterial pressures of 110/70 and heart rate of 98/min. Wound was thereafter carefully examined to reveal complete transection of trachea at the level of first tracheal ring and complete transection of cervical esophagus (Fig. 2). Platysma was found to be incised by the sharp stab but bilateral sternocleidomastoids were found to be intact.
Fig. 2.

Showing deep anterior neck wound, repaired right internal jugular vein, transected trachea (tracheostomy tube temporarily removed) and completely transected cervical esophagus.
Esophagus was repaired by absorbable 3-0 polygalactin round body sutures using interrupted sutures over a nasogastric tube in an end to end fashion (Fig. 3, Fig. 4). Following esophageal reconstruction tracheal transection was repaired. Posterior layer of transected trachea was repaired using interrupted 3-0 polypropylene sutures while keeping tracheostomy in situ (Fig. 5). Surgical knots were carefully kept outside the lumen. After completion of posterior layer tracheostomy tube was withdrawn and a 7.5 Fr endotracheal tube was carefully inserted per orally into the distal tracheal rent. Rest of the tracheal anastomosis was completed over the endotracheal tube (Fig. 6). Keeping in view of healthy tracheal and esophageal ends no muscle flap was kept in between esophageal and tracheal anastomosis.
Fig. 3.
Showing end to end anastomosis of transected esophagus anterior layer, posterior layer completed.
Fig. 4.
Showing completed anterior layer of esophageal anastomosis.
Fig. 5.

Showing tracheal anastomosis over endotracheal tube (posterior layer completed).
Fig. 6.

Showing complete anterior tracheal anastomosis with soft tissue strengthening around tracheal anastomosis.
Following completion of tracheal reconstruction over endotracheal tube, distal trachesostomy was done using cuffed 7.5 Fr tracheostomy tube and endotracheal tube was gently removed. Platysma was repaired; subcutaneous and skin closure was done in layers. A 12 Fr suction drain was placed in sub platysmal plane. Ryles tube was fixed and was kept in situ for 15 days. At 15 days contrast enhanced CT scan of neck was done which revealed healed tracheal and esophageal anastomosis with no evidence of contrast leak. Following which Ryles tube was removed and patient was allowed liquid and semisolid diet. Down gradation of tracheostomy was gradually done which was removed on 20th day. Patient was treated for major depression using injectable and later on oral olanzapine and psychotherapy. He was discharged on 25th postoperative day under stable physical and mental status.
Discussion
Suicidal injuries are one of the important causes of mortality among the persons in the age group of 15–30 years worldwide. In the Indian scenario studies have quoted there incidence to be around 38/1,00,000 in this vulnerable age group. Common modes of suicides in Indian subcontinent are consumption of poisonous substance (33.6%), hanging (31.5%), self-immolation (9.2%), and drowning (6.1%) [1].
Cut throat injuries are usually homicidal. Suicidal cut throat injuries with penetrating airway injuries in the neck are relatively uncommon [2]. In our case patient was a known case of major depression with poor follow-up to the concerned psychiatric clinic. As per the relatives he had committed suicide by slitting his throat with a kitchen knife which is a very uncommon mode because of it being extremely painful. Absence of any hesitation mark over the neck and body is also an unusual feature of the case and highlights that suicidal cuts may sometimes mimic homicidal cut throats.
Cut throat injuries are usually grievous injuries and carry a high risk of mortality and morbidity due to presence of vital structure in this small part of the body [3]. Even externally small appearing injuries to neck may harbor underlying serious trauma to blood vessels, nerves or visceral tubes (both airway and esophagus) [4]. Patient can rapidly exsanguinate even before reaching the hospital if neck vessels are injured. In a study conducted at Egypt following was the incidence of involvement of different structures in 74 cases of homicidal cut throats [5].
Skin, platysma and external jugular veins all cases
Cervical vertebrae 8.12% (n = 06) of cases.
Larynx, trachea, carotid and internal jugular vessels 91.89% (n = 68) of cases.
Sternocleidomastoid in 56.76% (n = 42).
Oesophagus and thyroid cartilage 18.92% (n = 14) and 10.81% (n = 08) of cases.
These injuries are also peculiar in an aspect of their requirement of a team which can manage the airway, control the hemorrhage and repair the viscera in an urgent and efficient manner [6]. In our case maintenance of airway using tracheostomy tube in the transected trachea, control of hemorrhage using packing and intravenous fluid resuscitation by the trauma team helped shifting the patient to operation theatre in a salvageable state.
Application of vascular clamps over the bleeding improves visibility in case of cut throat injuries and prevents further blood loss and we also utilized it in our case. In case of carotid vessels one has to be careful since many times significant cerebral hypoxia can occur even after temporary discontinuation of cerebral blood flow in setting of already existing hypovolemic shock [7]. Injuries to internal jugular veins are peculiar in the sense that they not only are the cause of hemorrhagic shock but carry the risk of air embolism and aspiration if accompanied by airway injuries as was in our case. Rents and sharp transection in the internal jugular vein without segmental loss can often be repaired primarily using a running, nonabsorbable fine suture as was in our case. In case there are large through-and through wounds or there is segmental loss of vein ligation is preferred which is well tolerated [8].
Concomitant transection of airway and esophagus in patient with cut throat injury is rare. Search of the published data reveals few cases of blunt trauma neck with airway and esophageal transections. None of them has been the outcome of suicidal cut throat injury [9].
Esophagus being posterior to trachea is rarely injured in homicidal or suicidal cut throats. Authors could not trace any case with suicidal esophageal transection in their search of medical literature. In case of blunt trauma neck with esophageal injuries esophagostomy as well as primary repair are surgical options depending upon duration of injury, site and size of esophageal rent and availability of expertise [10]. In our case due to high up esophageal transection with healthy margins and early presentation we decided to repair the esophagus primarily. Esophagus was repaired using absorbable 3-0 polygalactin sutures in interrupted single layer. We did not observe any postoperative leak from our esophageal anastomosis following removal of nasogastric tube.
Patients with completely transected trachea can survive and sustain systemic saturation for several hours and are salvageable. These patients can even instantly desaturate and exsanguinate if distal trachea retracts in to mediastinum [11]. In such conditions controlling the airway by cannulation becomes almost impossible. We employed following steps to deal with tracheal transection.
-
1.
Urgent control of airway by cannulation of distal trachea in the emergency room
-
2.
Tagging the cut ends of the airway on OT table
-
3.
Repair of esophagus and posterior tracheal wall
-
4.
Removal of tracheostomy tube and insertion of endotracheal tube
-
5.
Completion of remaining tracheal anastomosis
-
6.
Removal of endotracheal tube and creation of distal tracheostomy.
Each of these steps helped us in dealing with emergency situation of airway management and ultimately healthy anastomotic healing.
Distal tracheostomy in the patients with tracheal repair is a disputed topic [12]. We did it in our case for safe guarding the proximal tracheal anastomosis and expected prolonged invasive ventilation because of the presentation of severe haemmorhagic shock and multiple blood transfusions.
Postoperative contrast enhanced CT scan of the neck in case of our patient was done on 15th day which revealed healed tracheal and esophageal anastomosis area. Presence of subcutaneous emphysema in the neck is one of the features of leak from tracheal anastomosis in cases of cervical tracheal repairs. In our case we removed the tracheostomy tube on 20th day. Following which we didn't noticed any subcutaneous emphysema or breathing difficulty.
Cut throat injuries to neck are challenging in terms of being surgical emergencies, varied presentations and requirement of an efficient team work among anesthetists and various specialties of surgeons. However, if dealt with an urgent an efficient way results are often successful.
Declaration
Authors hereby declare no conflict of interest. No funding agency involved.
References
- 1.Radhakrishnan R., Andrade C. Suicides an Indian perspective. Indian J. Psychiatry. 2012;54(4):304–319. doi: 10.4103/0019-5545.104793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Symbas P.N., Hatcher C.R., Boehm G.A. Acute penetrating tracheal trauma. Ann. Thorac. Surg. 1976;22:473–477. doi: 10.1016/s0003-4975(10)64456-6. [DOI] [PubMed] [Google Scholar]
- 3.Demetriades D., Asensio J.A., Velmahos G., Thal E. Complex problems in penetrating neck trauma. Surg. Clin. North Am. 1996;76:661–683. doi: 10.1016/s0039-6109(05)70475-8. [DOI] [PubMed] [Google Scholar]
- 4.Waseem M., Gernsheimer J. A penetrating neck injury: trivial trauma with serious consequences. Pediatr. Emerg. Care. 2010;26:126–128. doi: 10.1097/PEC.0b013e3181ce3009. [DOI] [PubMed] [Google Scholar]
- 5.Rao Dinesh. An autopsy study of 74 cases of cut throat injuries. Egypt. J. Foren. Sci. 2015;5(4):144–149. [Google Scholar]
- 6.Sayyed Ehtesham H.N., Ali Eram, Beg M.H., Varshney Saurav. Successful resuscitation of a cardiac arrest following slit neck and carotid artery injury: a case report. J. Clin. Diagn. Res. 2016 Jun;10(6):25–27. doi: 10.7860/JCDR/2016/18641.8030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Brywczynski J.J. Management of penetrating neck injury in the emergency department: a structured literature review (meta-analysis of 20 studies) Emerg. Med. J. 2008;25:711–715. doi: 10.1136/emj.2008.058792. [DOI] [PubMed] [Google Scholar]
- 8.Simmons J.D., Ahmed N., Donnellan K.A., Schmieg R.E., Jr., Porter J.M., Mitchell M.E. Management of traumatic vascular injuries to the neck: a 7-year experience at a Level I trauma center. Am. Surg. 2012 Mar;78(3):335–338. [PubMed] [Google Scholar]
- 9.O'Connor A.E., Cooper J. Case of the month: complete transection of the trachea and oesophagus in a 10 year old child: a difficult airway problem. Emerg. Med. J. 2006 Feb;23(2):156–159. doi: 10.1136/emj.2004.022368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Asensio J.A., Berne J., Demetriades D. Penetrating esophageal injuries: time interval of safety for preoperative evaluation — how long is safe? J. Trauma. 1997;43:319–324. doi: 10.1097/00005373-199708000-00018. [DOI] [PubMed] [Google Scholar]
- 11.Cicala R.S., Kudsk K.A., Butts A. Initial evaluation and management of upper airway injuries in trauma patients. J. Clin. Anesth. 1991:391–398. doi: 10.1016/0952-8180(91)90003-6. [DOI] [PubMed] [Google Scholar]
- 12.Grillo Hermes C. Reconstruction of the trachea. Experience in 100 consecutive cases. Thorax. 1973;28:667. doi: 10.1136/thx.28.6.667. [DOI] [PMC free article] [PubMed] [Google Scholar]