

Abstract
In an era where noninvasive and minimally invasive techniques are heralding medical innovations and health science technology, necrological analysis is not bereft of this wave. Virtopsy is virtual autopsy. It is a new-age complimentary documentation approach to identify and analyze the details of demise. Utilizing virtual autopsy for orofacial forensic examination is an emerging specialty which holds a plethora of potential for future trends in forensic science. Being a noninvasive technique, it is a rapid method which facilitates the medicolegal process and aids in the delivery of justice. The present article is an overview of this emerging methodology.
Key words: Autopsy, forensic sciences, virtopsy
Introduction
Forensic science is a multidisciplinary science integrating criminalistics, engineering science, general jurisprudence, odontology, pathology/biology, psychiatry and behavioral science, questioned documents, toxicology, and physical anthropology.[1] An autopsy is a procedure which surveys the mortal remains of a person to identify the cause of death.[2] Forensic medicine deals with the examination and identification of relevant medical data in both the living and deceased and presentation of the same with exhaustive scientific matter for judicial proceedings.[3] Autopsy is also referred to as necropsy or postmortem examination and is revered as the cardinal expertise in forensic science. It is thus fondly called “the expertise of expertises.”[4]
The conventional procedure in postmortem examination is dissection, interpretation, and cataloguing.[5] The data obtained from this examination is then compiled, and the forensic experts arrive at a conclusion. The dead body is then handed over for the last rites to be performed. However, if the forensic expert wants to reconsider his/her decision over the previously gathered data, it may be difficult and not feasible.[3] The possible mutilation involved in the conventional autopsy often leaves the grieving family disturbed. Thus, the family of the deceased declares a negative consent for autopsy procedure on a sentimental basis.[6] Certain religious groups such as the Jews, Muslims, Jehovah's witness' do not completely accept conventional autopsy procedures.[7] These pitfalls of a conventional autopsy led to the genesis of virtopsy.
Virtopsy is a minimally invasive, observer-independent new-age technique in postmortem examination.
Virtopsy is “Virtual Autopsy.” Its etymology is derived from ancient Latin and Greek languages. The word “virtual” is derived from the Latin word virtus, meaning “useful, efficient, and good.” “Autopsy” is a marriage of the classical Greek terms “autos” (“self”) and “opsomei” (“I will see”), meaning “to see with one's own eyes.” Thus, the terms “virtual” and “autopsy” merge to form “virtopsy”.[1]
Virtopsy, like autopsy, is a multidisciplinary approach that unifies forensic medicine, pathology, radiology, image processing, physics, and biomechanics.[8]
History
In the late 1990s, a high-profile homicide case in Switzerland demanded an accurate forensic opinion. The impressions of the skull of the victim had to be matched with a most likely murder tool. The extensive work followed in this arena focusing on an objective method of forensic analysis which would minimally disturb the skull of the victim. Radiographic methods were used to forensically analyze the victim's remains which aided the legal judgment. This instance is commonly heralded as the birth of virtopsy.[3]
Virtopsy has four cornerstones, namely, (a) Three-dimensional (3D) surface scanning 3D/computer-aided design photogrammetry, (b) multi-slice computed tomography (MSCT), and (c) magnetic resonance imaging (MRI) (d) MRI spectroscopy.[8]
Three-dimensional surface scanning three-dimensional/computer-aided design photogrammetry
It is the science of making measurements using photographs. A number of different photographs are taken from different angles and are analyzed by TRITOP/ATOS II system (GOM, Braunschweig, Germany) software.[3] This software uses high-speed imaging and remote sensing to construct a 3D comprehensive image of the surface features of the deceased.
Multislice computed tomography
It features the hard tissue architecture in multiple sections. It aids in the identification of any changes in the same.
Magnetic resonance imaging
It features the condition of the soft tissue. It aids in the identification of any changes in the same.
MSCT and MRI together help in the differentiation of the adjacent structures.
Magnetic resonance imaging spectroscopy
It provides the biochemical picture of the deceased. It uses metabolites in the brain emerging from postmortem decomposition to give an accurate time of death.
Micro-computed tomography
Special cases require modifications of the above-mentioned techniques. The Institute of Medical Physics in Erlangen, Germany, developed a scanner to image a 3D volume with an isotropic resolution ranging from 10 to 100 μm.[9] This scanner is sensitive to examine samples of diameters ranging from 4 to 40 mm.
Magnetic resonance microscopy
In vitro studies on eyeballs were anatomically imaged. After this, eyeballs were paraffin embedded, and sections of 6 μm were cut and stained with hematoxylin and eosin.[10] Figure 1 Schematic representation of the procedure of virtopsy.
Figure 1.
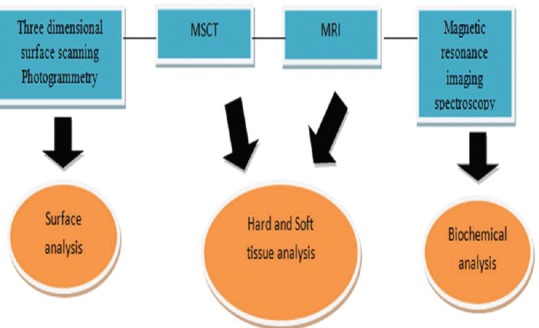
Schematic representation of the procedure of virtopsy
Practice of Virtopsy
Virtobots
In this era of robotics, virtopsy is not to be left behind. It uses an all-in-one machine called “Virtobot” which integrates the four imaging modalities mentioned above to practice virtopsy. This machine will allow combined surface and body volume data acquisition within a single 3D space, making present-day data fusion techniques dispensable.
Virtomobile
Virtobot is a gigantic machine making its utility in the sites of mass disaster futile. This leads to the requirement of a more compact device for the practice of virtopsy. Thus, virtomobile was conceived. It is a version of Virtobot mounted on a trailer which can be easily transported to the site of disaster.[2]
Merits of Virtopsy
It is a scalpel-free, noninvasive imaging technology. As it is a digitally mastered technique, transferring images over the web, archiving over years or decade are real possibilities. It is an ethical evolution which serves better acceptance for the relatives of the deceased and also by certain religious customs where incisions are not recommended after death. Since there is no mutilation of the body, it poses no hazard of infections from the blood or other tissue fluids to the health-care workers. It is less time consuming, and the body can be released immediately after the scanning. It is extremely efficient in studying wounds and helps matching of the probable weapon. This can be studied without disturbing the body architecture.[11]
Demerits of Virtopsy
The initial investment for the equipment required may not be feasible in developing countries. The insufficient database for comparative study of virtopsy and conventional autopsy has limited the diverse applications. It is not possible to distinguish all the pathological conditions with this technique. It cannot give a definitive the infection status. It is difficult to differentiate between ante- and post-mortem wounds. Postmortem artifacts are unclear. Organic changes in color, odor are not clear. Small tissue injuries may be missed.[11]
Effectiveness of Virtopsy
The present-day literature supports the accuracy of virtopsy. Virtopsy has about 80% concordance between cause of death identified with conventional autopsy and virtopsy. It not only has a high potential of accuracy but also scores over conventional autopsy in the identification of fracture lines. The base of the skull pathologies are better visualized by virtopsy. Explicit details about primary and secondary trauma, depth of injury, microbone injuries are better visualized by virtopsy.[12] Figure 2 Virtopsy in a nut-shell.
Figure 2.
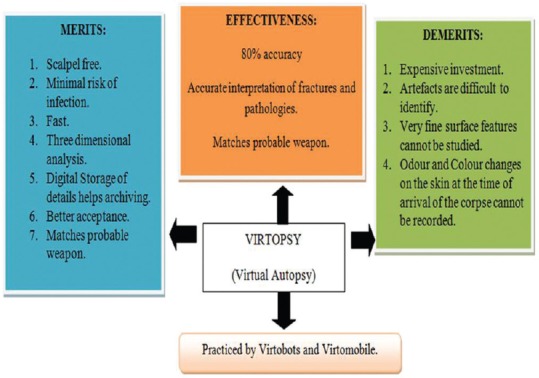
Virtopsy in a nut-shell
Applications in Forensic Odontology
Virtopsy has been used in various judicial cases to arrive at a fast, accurate legal judgment. Accurate analysis of depth of obstruction in a case of demise due to obstruction/asphyxiation.[13] Accurate analysis of ante- and post-mortem CT panoramic records.[3] Accurate comparison of ante- and post-mortem records of restorative materials and their variations under extreme condition of temperature simulating mass disaster environment.[14] If a body part is found, radiographic examination can be used to identify the pathologic lesions or implants placed in the victim. This can aid in personnel identification by comparing with antemortem records. Simulation and analysis of bite marks, lip prints, and rugae pattern can be performed by photogrammetry.[15]
Conclusion
In a world which is becoming more and more tolerant to incorporating various minorities into the mainstream, virtopsy along with its scientific rationale and practical merits salutes and respects the religious and emotional sentiments of various ethnic groups. Virtopsy is a simple, noninvasive procedure to record the surface and internal features of the deceased. This is immensely helpful for future correlations as it involves preserving the records for a longer duration. Because of these virtues, virtopsy is quickly gaining importance and holds great promise for the future of forensic science.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Jeelani S, Baliah J. Virtopsy – A moral boon in forensics. J Sci Dent. 2013;3:54–8. [Google Scholar]
- 2.Rajendran R, Sivapathasundharam B. Shafer's Textbook of Oral Pathology. 7th ed. India: Elsevier; 2012. Forensic Odontology; pp. 879–907. [Google Scholar]
- 3.Dirnhofer R, Jackowski C, Vock P, Potter K, Thali MJ. VIRTOPSY: Minimally invasive, imaging-guided virtual autopsy. Radiographics. 2006;26:1305–33. doi: 10.1148/rg.265065001. [DOI] [PubMed] [Google Scholar]
- 4.Zacharias M, Zacharias E. Dictionary of legal medicine. 2nd ed. Curitiba: University Publishing House Champagnat; 1991. [Google Scholar]
- 5.Lundberg GD. Low-tech autopsies in the era of high-tech medicine: Continued value for quality assurance and patient safety. JAMA. 1998;280:1273–4. doi: 10.1001/jama.280.14.1273. [DOI] [PubMed] [Google Scholar]
- 6.França GV. Legal Medicine. 5th ed. Rio de Janeiro: Guanabara Koogan; 1998. [Google Scholar]
- 7.Pomara C, Fineschi V, Scalzo G, Guglielmi G. Virtopsy versus digital autopsy: Virtual autopsy. Radiol Med. 2009;114:1367–82. doi: 10.1007/s11547-009-0435-1. [DOI] [PubMed] [Google Scholar]
- 8.Bolliger SA, Thali MJ, Ross S, Buck U, Naether S, Vock P. Virtual autopsy using imaging: Bridging radiologic and forensic sciences. A review of the Virtopsy and similar projects. Eur Radiol. 2008;18:273–82. doi: 10.1007/s00330-007-0737-4. [DOI] [PubMed] [Google Scholar]
- 9.Engelke K, Karolczak M, Lutz A, Seibert U, Schaller S, Kalender W. Micro-CT. Technology and application for assessing bone structure. Radiologe. 1999;39:203–12. doi: 10.1007/s001170050497. [DOI] [PubMed] [Google Scholar]
- 10.Vogel H. Violence Ro¨ntgenbild: Findings in war, torture and crimes. Echomed. 1997;41:13–42. [Google Scholar]
- 11.Patowary AJ. Virtopsy: One step forward in the field of forensic medicine – A review. J Indian Acad Forensic Med. 2008;30:32–6. [Google Scholar]
- 12.Junior R, Souza PH, Coudyzer W, Thevissen P, Willems G, Jacobs R. Virtual autopsy in forensic sciences and its applications in the forensic odontology. Revista Odonto Ciência. 2012;27:5–9. [Google Scholar]
- 13.Oesterhelweg L, Bolliger SA, Thali MJ, Ross S. Virtopsy: Postmortem imaging of laryngeal foreign bodies. Arch Pathol Lab Med. 2009;133:806–10. doi: 10.5858/133.5.806. [DOI] [PubMed] [Google Scholar]
- 14.Jackowski C, Wyss M, Persson A, Classens M, Thali MJ, Lussi A. Ultra-high-resolution dual-source CT for forensic dental visualization-discrimination of ceramic and composite fillings. Int J Legal Med. 2008;122:301–7. doi: 10.1007/s00414-008-0224-8. [DOI] [PubMed] [Google Scholar]
- 15.Brüschweiler W, Braun M, Dirnhofer R, Thali MJ. Analysis of patterned injuries and injury-causing instruments with forensic 3D/CAD supported photogrammetry (FPHG): An instruction manual for the documentation process. Forensic Sci Int. 2003;132:130–8. doi: 10.1016/s0379-0738(03)00006-9. [DOI] [PubMed] [Google Scholar]