

Abstract
Context:
In exhibiting gender dimorphism, the bony pelvis and skull give the most reliable results from morphometric analysis. Palatal dimensions were reported to exhibit racial difference and sexual dimorphism in several studies.
Aim:
The aim of the present study was to measure the maxillary arch depth and palatal depth in Indian population to assess their use as a tool for sexual dimorphism.
Materials and Methods:
Two hundred and fifty males and 250 females in the age group of 17–25 years were enrolled in the study, and impressions of maxillary arch were made. Measurement of palatal depth and maxillary arch depth was carried out at specific reference points using Korkhaus compass and digital caliper, respectively. The comparison of maxillary arch depth and palatal depth values was done using independent t-test. P < 0.05 was considered statistically significant. Diagnostic performance of significantly different variable was quantified by plotting “receiver operating characteristic” (ROC) curve.
Results:
Arch depth mean values were significantly higher in males than females. However, palatal depth mean values, though higher in males, were not significant. Area under the curve in ROC curve for maxillary arch depth was found to be 0.76, indicating sufficiency of discriminatory power of this variable.
Conclusion:
The present study showed that maxillary arch depth can be used as a tool for sex determination along with other morphometric methods. Mean value of both maxillary arch depth and palatal depth can be used as the baseline value for given population to be used as a reference for further studies.
Key words: Dental arch, forensic dentistry, palate, sex dimorphism
Introduction
Human identification is one of the most challenging tasks one has been confronted with whenever a catastrophe strikes. Forensic identification in such cases involves comparative identification and establishment of biologic profile. Biologic profile includes sex, ancestry, skeletal and dental age, stature, and physique.[1] Determination of sex is of immense importance in person identification. One of the older and widely used methods of gender identification is the morphological analysis of skeletal and dental remains.[1] Bone and dental structures of the palate are often preserved even in the face of serious bad damage at or following death. The sexual dimorphism of the palate has been affirmed by Krogman and Iscan, Woo and Larnach and Macintosh.[2,3,4] Johnson et al. selected palatal length as one of the best variables for sex determination of caucasoid skulls.[5] Sex determination using metric observation of the palate has been affirmed by Burris and Harris (1998).[6] Rogers (2005) has ranked palate size/shape as sixth among the 17 morphological features of the skulls used for sexing unknown skeletal remains.[7] Bigoni et al. noted significant sex differences in the region of the palate.[8] Significantly, higher arch depth values and palatal depth values were reported in males.[9,10,11,12] In the Indian context, very few studies focused on palatal dimensions such as arch depth and palatal depth which were reported to exhibit racial difference and sexual dimorphism.[2,6,13,14,15] Hence, the present study was undertaken to measure maxillary arch depth and palatal depth values in young adults of Marathwada region, India, and to evaluate its potential as sex determination tool.
Materials and Methods
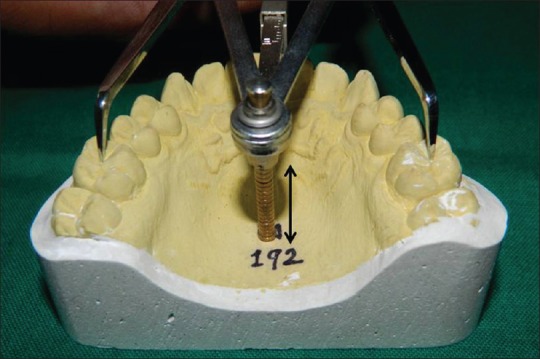
This study was approved by the Institutional Ethical Committee. Sample size was calculated using standard deviation from previous studies, with 95% confidence level and 5% margin of error. It comprised 500 dentulous individuals with 250 males and 250 females in the age group of 17–25 years having class I normal occlusion and healthy state of the periodontium. Exclusion criteria included participants with carious maxillary incisors, canine, first premolar or first molar, or crowding, spacing, missing teeth; participants with habits such as thumb sucking and mouth breathing; participants with previous orthodontic treatment; or participants with any localized or systemic hard or soft tissue pathology related to teeth or jaws. Informed consent was sought from the patients after a complete explanation of the purpose of the study. Impressions of maxillary arch were made in irreversible hydrocolloid material. Maxillary arch depth was measured from most labial midpoint between central incisors to a line connecting the mesial surfaces of two posterior corresponding teeth usually first permanent molars, along with a midsagittal plane [Figure 1].[16,17] Palatal depth was measured from a level coinciding with central fossa of first permanent molar to the deepest point of palate in the midline [Figure 2].[18] These measurements were carried out using Korkhaus compass and digital caliper. All values were taken in millimeters. Comparison of maxillary arch depth and palatal depth values were done using independent t-test. Difference was considered statistically significant when P < 0.05. Diagnostic performance of significantly different variable was quantified by plotting “receiver operating characteristic” (ROC) curve. All statistical analyses were performed using GraphPad Prism v. 5.0 software (GraphPad Software, Inc. CA, USA.).
Figure 1.

Maxillary arch depth measurement using digital caliper
Figure 2.
Palatal depth measurement with Korkhaus compass
Results
Mean maxillary arch depth and palatal depth values in male participants were 27.19 ± 1.79 mm (range 23.85–32.43 mm) and 18.17 ± 1.85 mm (range 13.2–22.0 mm), respectively. Mean maxillary arch depth and palatal depth values in female participants were 25.57 ± 1.42 mm (range 21.5–28.5 mm) and 17.99 ± 1.58 mm (range 14.0–22.5 mm), respectively. On comparison of these mean values among males and females by independent t-test, only mean maxillary arch depth values were found to be statistically significantly different (P < 0.0001, t = 11.99, df = 498, 95% confidence interval [CI]: −2.240 to − 1.609) [Figure 3]. Mean palatal depth values failed to show any statistically significant difference among males and females (P = 0.2525, t = 1.146, df = 498, 95% CI: −0.1253–0.4757) although males had slightly higher palatal depth values than females [Figure 4]. Area under the curve (AUC) for maxillary arch depth was found to be 0.7621 (SE 0.02069, 95% CI: 0.7215–0.8026) [Figure 5]. Optimal cutoff point was decided for maxillary arch depth as 26.05 mm (sensitivity - 72% and specificity - 65.2%) to use it as a probable reference for Indian population to differentiate between males and females.
Figure 3.
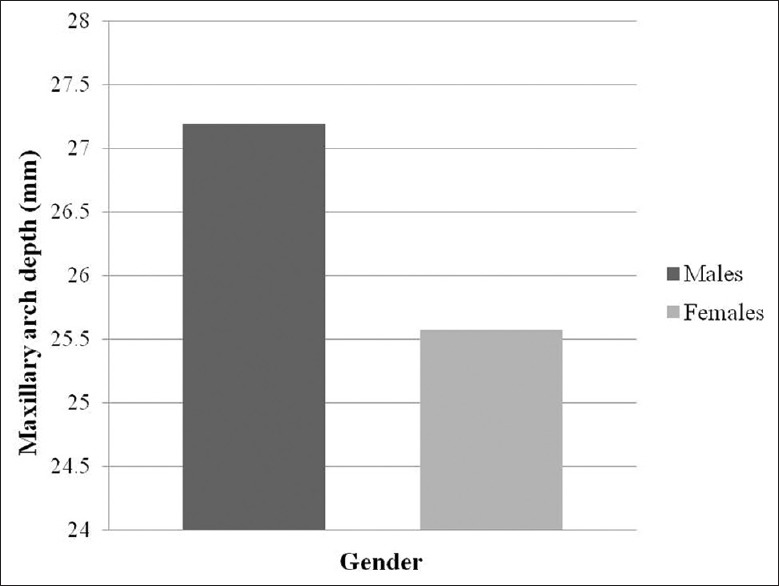
Comparison of mean values of maxillary arch depth in males and females
Figure 4.
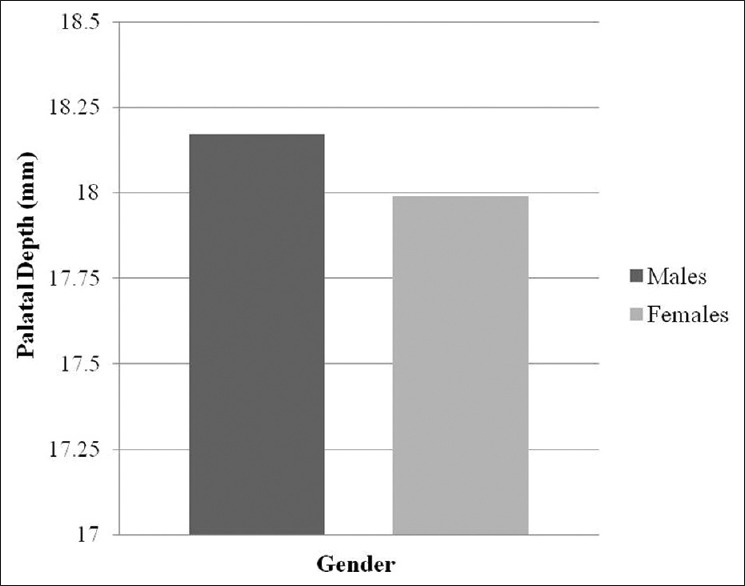
Comparison of mean values of palatal depth in males and females
Figure 5.
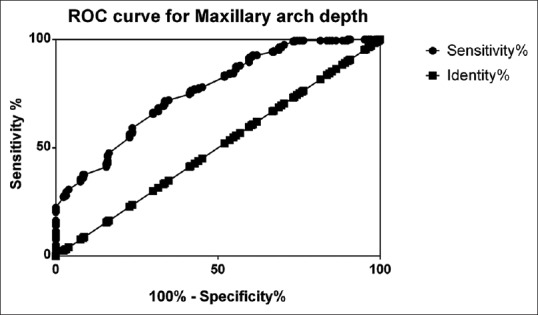
Area under the curve for arch depth values in study population
Discussion
In forensic human identification, sex determination is an important step because not only it does effectively cut the number of possible matches to half but also subsequent methods for age and stature estimation are often gender dependent.[19,20] The hormonal and visual differences that make living males and females distinct also create physiological differences between their skeletons. This “sexual dimorphism” is most obvious in the pelvic bones and the skull.[7,19] In general, males have more robust characters or larger dimensions.[21] Several sites on crania are reported to be suitable for sex determination.[22,23] Linear skeletal dimensions were found to be significantly greater in males than females.[24] Palatal dimensions were reported to exhibit racial difference and sexual dimorphism.[2,6,13,14,15] In general, in males, the palate is usually more in length and breadth with a closed U-shape compared to narrow and short palate with a parabolic shape in females.[21]
In the present study, mean values of arch depth were significantly higher in males than females, a finding in accord with previous studies.[9,10,11] Few of the studies found higher but insignificant mean values of arch depth.[6,25,26] Significant sex difference in palatal depth values demonstrated in some studies.[10,12] However, mean values of palatal depth, though higher in males, were not significant in the present study. The AUC is most commonly used method to summarize the discriminatory capacity of the ROC curve. The area measures discrimination, that is, the ability of the classifier (arch depth in the present case) to correctly differentiate study population into alternate states (male and female sex). In general, discrimination is deemed accurate where AUC exceeds 0.7–0.8.[27] AUC for maxillary arch depth was found to be 0.7621, indicating sufficiency of discriminatory power of this variable.
Often the corroboration of identification by utilization of data gained from several of the less specific methods may elevate the probability of correct identification beyond that which could be obtained by either of the methods alone. Thus, maxillary arch depth may be used as a supplementary method along with the other methods to increase the accuracy of sex identification in unknown body remains. Resilience of palatal structures to traumatic and natural forces makes this method practical in several forensic situations. However, while extrapolating results of such studies in field, it is important to note that a significant number, approximately 5% of individuals in most populations, will be androgynous, i.e., will possess an equal number of male and female skeletal traits and also the fact that palatal dimensions will be affected by the dental and skeletal malocclusion.[1] Most of the morphometric studies face a problem during measurement of metric traits, or observation of nonmetric traits is that these traits are affected by age, trauma or any discrepancy during growth (malocclusion, retention of deciduous tooth, clefting, and habits), etc., Hence, participants procured during the study would be based on criteria that will prevent sampling bias and are not affected by these factors. However, in the forensic examination, such ideal participants are rare to find. This preliminary study was carried out keeping in mind these limitations. It has provided baseline data for the determination of sex of young adults from Marathwada region of Maharashtra (Western India) from a fragment of the skull, that is, hard palate. Further research is necessary to standardize the procedure for measurement of these morphologic characters to increase their reproducibility, comparability, and credibility.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Gill-King H. Forensic anthropology. In: Senn DR, Stimson PG, editors. Forensic Dentistry. 2nd ed. Boca Raton: CRC Press Taylor & Francis Group;; 2010. pp. 137–58. [Google Scholar]
- 2.Suazo GI, Zavando MD, Smith RL. Accuracy of palate shape as sex indicator in human skull with maxillary teeth loss. Int J Morphol. 2008;26:989–93. [Google Scholar]
- 3.Brothwell DR. Dental Anthropology. London: Pergamon Press; 1963. [Google Scholar]
- 4.Krogman WM, Iscan MY. Forensic Medicine. Springfield, Illinois: Charles C. Thomas Publishers; 1986. The human skeleton. [Google Scholar]
- 5.Sumati, Patnaik VV, Phatak A. Determination of sex from hard palate by discriminant function analysis. Int J Basic Appl Med Sci. 2012;2:243–51. [Google Scholar]
- 6.Burris BG, Harris EF. Identification of race and sex from palate dimensions. J Forensic Sci. 1998;43:959–63. [PubMed] [Google Scholar]
- 7.Rogers TL. Determining the sex of human remains through cranial morphology. J Forensic Sci. 2005;50:493–500. [PubMed] [Google Scholar]
- 8.Bigoni L, Velemínská J, Bruzek J. Three-dimensional geometric morphometric analysis of cranio-facial sexual dimorphism in a Central European sample of known sex. Homo. 2010;61:16–32. doi: 10.1016/j.jchb.2009.09.004. [DOI] [PubMed] [Google Scholar]
- 9.Barrett MJ, Brown T, Macdonald MR. Size of dental arches in a tribe of Central Australian aborigines. J Dent Res. 1965;44:912–20. doi: 10.1177/00220345650440052701. [DOI] [PubMed] [Google Scholar]
- 10.Bottyan OL. Variations of the palatum with respect to sexual dimorphism. Ann Hist Nat Mus Nationalis Hung. 1970;62:393–404. [Google Scholar]
- 11.Abd-el Samad Younes S. Maxillary arch dimensions in Saudi and Egyptian population sample. Am J Orthod. 1984;85:83–8. doi: 10.1016/0002-9416(84)90126-x. [DOI] [PubMed] [Google Scholar]
- 12.Younes S, el Angbawi MF, al Dosari AM. A comparative study of palatal height in a Saudi and Egyptian population. J Oral Rehabil. 1995;22:391–5. doi: 10.1111/j.1365-2842.1995.tb00790.x. [DOI] [PubMed] [Google Scholar]
- 13.Wood JK. Direction and type of the transverse palatine suture and its relation to the form of the hard palate. Am J Phys Anthropol. 1949;7:385–99. doi: 10.1002/ajpa.1330070306. [DOI] [PubMed] [Google Scholar]
- 14.Jacobson A. The Dentition of the South African Negro. Birmingham: UAB School of Dentistry Publishers; 1982. [Google Scholar]
- 15.Byers SN, Churchill SE, Curran B. Identification of Euro-Americans, Afro-Americans, and Amerindians from palatal dimensions. J Forensic Sci. 1997;42:3–9. [PubMed] [Google Scholar]
- 16.Burris BG, Harris EF. Maxillary arch size and shape in American blacks and whites. Angle Orthod. 2000;70:297–302. doi: 10.1043/0003-3219(2000)070<0297:MASASI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Lindsten R, Ogaard B, Larsson E, Bjerklin K. Transverse dental and dental arch depth dimensions in the mixed dentition in a skeletal sample from the 14th to the 19th century and Norwegian children and Norwegian Sami children of today. Angle Orthod. 2002;72:439–48. doi: 10.1043/0003-3219(2002)072<0439:TDADAD>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 18.Louly F, Nouer PR, Janson G, Pinzan A. Dental arch dimensions in the mixed dentition: A study of Brazilian children from 9 to 12 years of age. J Appl Oral Sci. 2011;19:169–74. doi: 10.1590/S1678-77572011000200014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Macaluso PJ., Jr Sex discrimination potential of permanent maxillary molar cusp diameters. J Forensic Odontostomatol. 2010;28:22–31. [PubMed] [Google Scholar]
- 20.Scheuer L. Application of osteology to forensic medicine. Clin Anat. 2002;15:297–312. doi: 10.1002/ca.10028. [DOI] [PubMed] [Google Scholar]
- 21.Gentry Steele D, Bramblett CA. The Anatomy and Biology of the Human Skeleton. Texas: A & M University Press; 1988. The skull; pp. 53–4. [Google Scholar]
- 22.Bibby RE. A cephalometric study of sexual dimorphism. Am J Orthod. 1979;76:256–9. doi: 10.1016/0002-9416(79)90022-8. [DOI] [PubMed] [Google Scholar]
- 23.Vasudeva N, Choudhry R. Precondylar tubercles on the basiocciput of adult human skulls. J Anat. 1996;188:207–10. [PMC free article] [PubMed] [Google Scholar]
- 24.Wei SH. Craniofacial width dimensions. Angle Orthod. 1970;40:141–7. doi: 10.1043/0003-3219(1970)040<0141:CWD>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 25.Al-Khateeb SN, Abu Alhaija ES. Tooth size discrepancies and arch parameters among different malocclusions in a Jordanian sample. Angle Orthod. 2006;76:459–65. doi: 10.1043/0003-3219(2006)076[0459:TSDAAP]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 26.Hassanali J, Odhiambo JW. Analysis of dental casts of 6-8- and 12-year-old Kenyan children. Eur J Orthod. 2000;22:135–42. doi: 10.1093/ejo/22.2.135. [DOI] [PubMed] [Google Scholar]
- 27.Lustres-Perez V, Rodrıguez-Alvarez MX, Fernandez-Pulpeiro1 MP, Cadarso-Suarez C. Application of receiver operating characteristic (ROC) methodology in biological studies on marine resources: Sex determination of Paracentrotus lividus (Lamarck, 1816) Stat Oper Res Trans. 2010;34:239–48. [Google Scholar]