

Abstract
Metastasis from distant primary tumors is extremely rare in the paranasal sinuses with few hundred cases in the literature. Metastatic carcinoma of the prostate is even rarer, despite being one of the most common tumors, with only 24 cases published. In this article, we report a case of a 58-year-old male presenting with epistaxis and nasal obstruction as initial symptoms of a metastatic prostate carcinoma in the ethmoid cells and maxillary sinus.
1. Introduction
Paranasal sinus cancer represents a small portion of the head and neck cancer, approximately 5% of all head and neck tumors [1]. These tumors may arise from multiple tissues present in the nose and paranasal sinuses [2] or more rarely be a metastasis from a distant primary cancer.
Prostate adenocarcinoma is the most prevalent malignant cancer in the male population. In Europe, the incidence rate is 214 cases per 1000 men [3]. Metastases from prostate tumors are a major determinant of survival rates, and prostate-specific antigen tests decrease the incidence of metastatic disease at diagnosis [4].
In this article, we presented the rare case of a patient with a distant metastasis in the right ethmoid cells from a prostate adenocarcinoma.
2. Case Report
A 58-year-old male patient was referred to the Otolaryngology Emergency Service because of important unilateral epistaxis, the third episode in the previous month. He also presented with ipsilateral nasal obstruction and diplopia with a three-month evolution. In his medical report, there was a record of penile squamous cell carcinoma treated with surgery and radiotherapy in 2014 and stage IV prostate adenocarcinoma (iliac, lumbar, and encephalic metastasis) refractory to hormone therapy and chemotherapy, submitted to palliative radiotherapy one month earlier.
During endoscopy, a polypoid, papilloma-like mass originated from the middle meatus was visible, occupying the entire right nasal fossa. No other abnormality was seen in the left nasal fossa. The epistaxis was controlled; the patient was stabilized and referred to biopsy.
The computed tomography (CT) and magnetic resonance imaging (MRI) showed soft tissue density lesion in the right nasal fossa, ethmoid cells, and maxillary sinus with extension into the inferior portion of the orbit through the lamina papyracea and posteriorly to the pterygomaxillary fissure (Figures 1 and 2).
Figure 1.
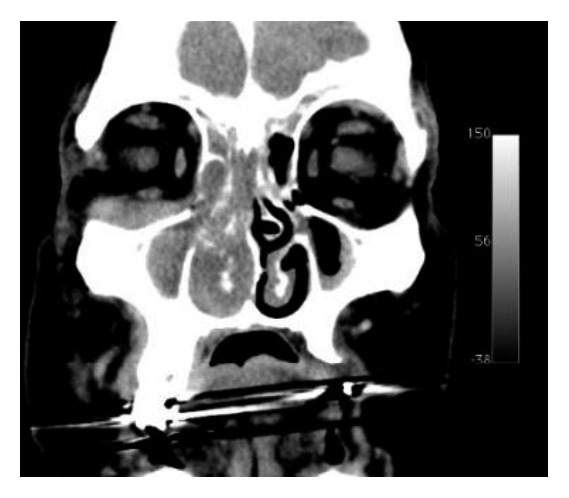
CT demonstrates lesion occupying ethmoid cells, nasal cavity, and maxillary sinus and extending through the lamina papyracea.
Figure 2.
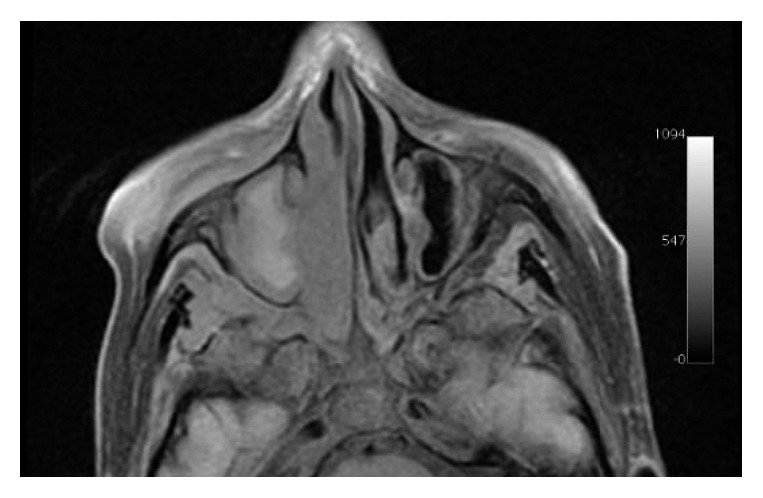
T1-weighted MRI with fat suppression demonstrates the lesion extending to the pterigomaxillary fissure.
The biopsy resulted in adenocarcinoma (Figures 3(a) and 3(b)). Since the patient had a medical report of prostate adenocarcinoma, the sample was submitted to an immunohistochemical panel. The prostate-specific antigen (PSA) was highly positive, and the diagnosis was confirmed as metastatic prostate adenocarcinoma (Figures 4(a) and 4(b)).
Figure 3.
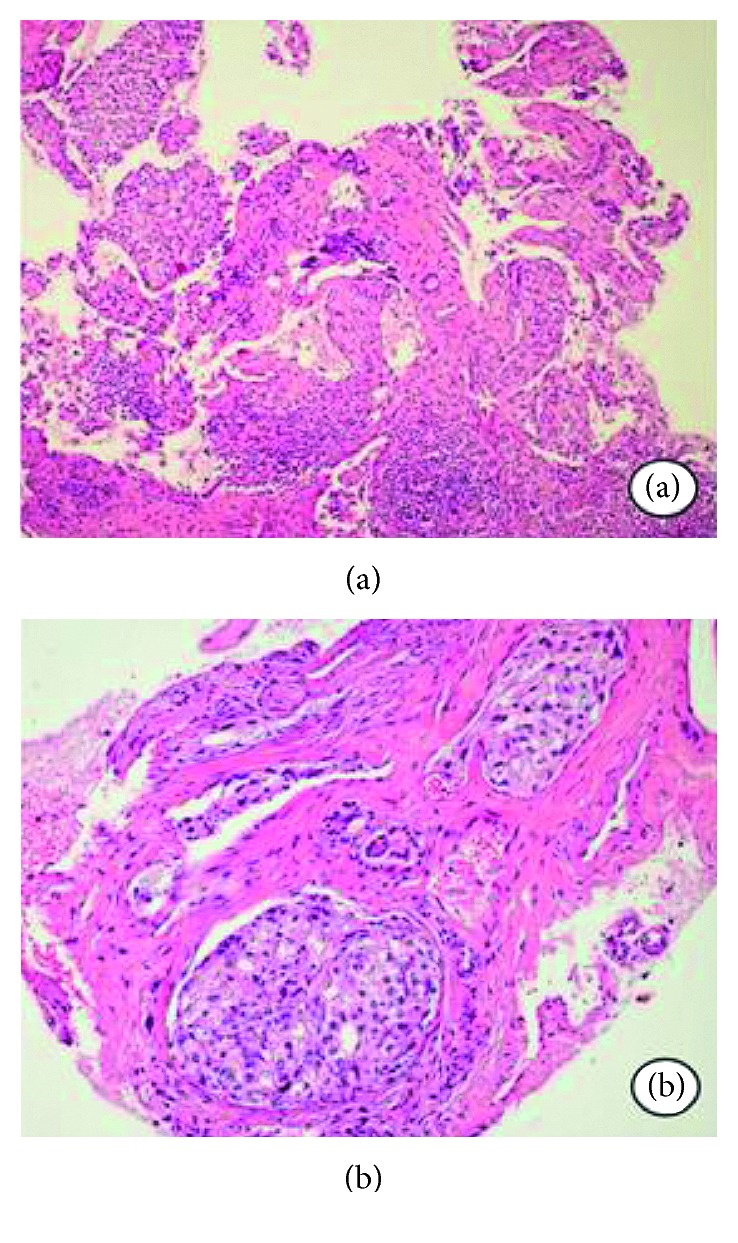
(a) Neoplasia infiltrating surrounding tissue with irregular margins (H&E stain). (b) Atypical epithelial islands with ductal characteristics resembling adenocarcinoma (H&E stain).
Figure 4.
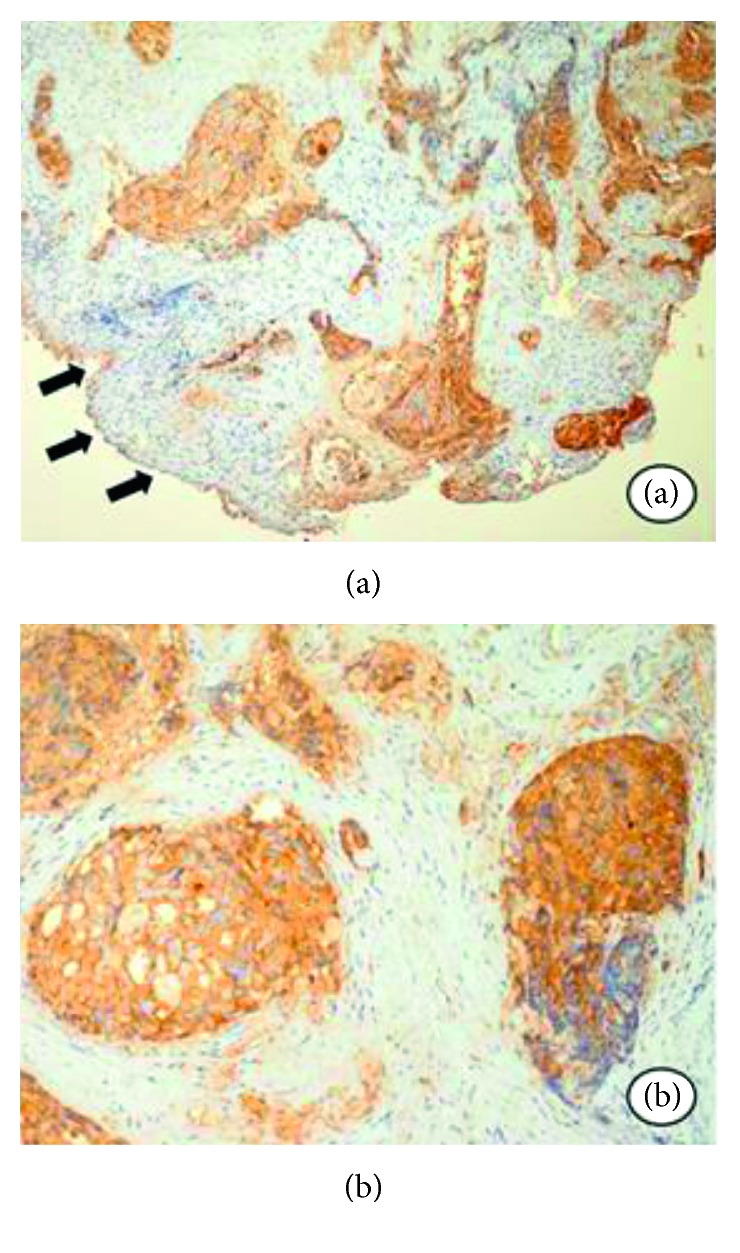
(a) Positive reaction to the PSA antigen in the epithelial islands, and there is no reaction in the superficial epithelium. (b) Strong expression of the PSA antigen in the ductal cells.
Because of the clinical status of the patient, a few symptoms presented, and the fact that he was already submitted to radiotherapy at the same field, it was opted for a clinical follow-up. After two months of the diagnosis, the patient deceased.
3. Discussion
Paranasal sinuses are a complex anatomic area, surrounding important structures such as the orbit and skull base. The most incident tumors are the squamous cell carcinoma, followed by adenocarcinoma and adenoid cystic carcinoma [5].
In a review, Prescher and Brors reported 169 cases of metastatic tumor to the paranasal sinuses [6]. Most cases originated from the kidney, followed by the lung, breast, thyroid, and prostate. Prescher and Brors also reported that the maxillary sinus was the most affected, followed by the sphenoid, ethmoid, and frontal sinuses [6]. These data are similar to those published by Bernstein [7]. In 77% of the cases, just one paranasal sinus was affected [6].
The nonspecific symptoms are similar to those of primary tumors. The nasal symptoms are usually nasal mass, nasal obstruction, facial deformity, and epistaxis. Orbital symptoms may also occur, such as proptosis, ptosis, decreased vision, and diplopia. Occasionally, these symptoms may be the first presentation of an occult primary tumor [8, 9].
The most frequent sites involved in prostate metastasis are the bone (90%), lung (46%), and liver (25%) [10]. The head and neck are rare locations for metastasis, and it occurs more frequently in the brain, dura, and lymph nodes [11]. The treatment may be hormone therapy, chemotherapy, radioisotopes, and radiotherapy [12].
Metastasis may reach the paranasal sinuses by hematogenous, lymphogenous, or vertebral venous plexus pathways. First postulated by Batson [13], this low-pressure valveless system is a connection between deep pelvic veins, intercostal veins, vena cava, and the azygos system. A rise in the abdominal pressure might redirect the blood flux from the vena cava system to the vertebral venous plexus. This flux alteration can allow the tumor to reach the paranasal sinuses [14].
This is the twenty-fifth reported case of metastatic prostate adenocarcinoma in the paranasal sinuses. The majority of cases involved patients with known prostate cancer, with a mean age of 63.15 years, and the most affected sinus was the sphenoid (44.5%). Radiotherapy was the preferred treatment option (40.7%). In Table 1, we describe the cases reported in full text, available online so far.
Table 1.
Prostate metastasis to the paranasal sinuses.
| Author | Age | Sinus | Symptoms | Treatment | Survival |
|---|---|---|---|---|---|
| Barrs et al. [15] | 61 | Sphenoid | Diplopia | Unknown | Died 2 years after presentation |
| Barrs et al. [15] | 57 | Sphenoid | Diplopia, decreased visual acuity, ptosis, and numbness of the left face | Unknown | Died 2 years after presentation |
| McClatchey et al. [16] | 54 | Sphenoid | Frontal headache and blurring of the right eye | Radiotherapy | Alive 1 year after presentation |
| Leduc et al. [17] | 75 | Sphenoid | Diplopia and ptosis of the right eye | Pulpectomy | Alive 19 months after presentation |
| Matsumoto et al. [18] | 79 | Sphenoid | Headache and diplopia | Orchiectomy | Unknown |
| Har-el et al. [19] | 77 | Maxillary | Exophthalmos of the right eye | Orchiectomy and hormonal block | Unknown |
| Mickel and Zimmerman [20] | 67 | Sphenoid | Diplopia and numbness on the right side of the nose | Radiotherapy | Died 2 and a half months after presentation |
| Saleh et al. [21] | 71 | Sphenoid | Bilateral exophthalmos and hemoptysis | None | Died 1 month after biopsy |
| Fortson et al. [22] | 50 | Ethmoid | Nasal obstruction, diplopia, proptosis, and blurred vision | Chemotherapy and radiotherapy | Died 7 months after presentation |
| Telera et al. [23] | 61 | Sphenoid | Ptosis and diplopia of the right eye | Radiotherapy | Died 13 months after presentation |
| Oliver et al. [8] | 72 | Maxillary, frontal, and ethmoid | Frontal headache and retro-orbital pain | Hormonal block | Alive three months after presentation |
| Hunt et al. [11] | 76 | Sphenoid | Unknown | Radiotherapy and hormonal block | Alive 14 months after presentation |
| Lavasani et al. [24] | 67 | Sphenoid | Decreased visual acuity | Radiotherapy | Alive 6 months after presentation |
| Başeskioglu et al. [25] | 69 | Maxillary | Sinus fullness | Radiotherapy | Died 32 months after diagnosis |
| Ibarguren et al. [26] | 64 | Maxillary and frontal | Ptosis, proptosis, and facial numbness | Hormonal block and chemotherapy | Alive 8 months after presentation |
| El Khatib et al. [27] | 57 | Maxillary | Facial swelling | Pulpectomy and hormonal block | Died 9 months after presentation |
| Viswanatha [28] | 68 | Ethmoid and frontal | Facial swelling and epistaxis | Radiotherapy | Lost to follow-up after 3 months of presentation |
| Tunio et al. [29] | 65 | Ethmoid | Nasal obstruction, diplopia, and proptosis | Radiotherapy and hormonal block | Alive until article publication |
| Azarpira et al. [30] | 74 | Maxillary | Nasal obstruction | Chemotherapy and radiotherapy | Died 11 months after presentation |
| Petersson et al. [31] | 55 | Sphenoid | Headache, diplopia, and blurred vision | Hormonal block | Unknown |
| Puche-Sanz et al. [32] | 56 | Sphenoid | Decreased visual acuity and facial numbness | Radiotherapy and hormonal block | Alive 5 years after presentation |
| Akdemir et al. [33] | 73 | Frontal and ethmoid | Headache and exophthalmos | Hormonal block | Unknown |
| Evarts et al. [34] | 59 | Maxillary and ethmoid | Cheek numbness, headache, decreased visual acuity, nasal obstruction, and drainage | Chemotherapy | Died 2 months after biopsy |
| Lechien et al. [35] | 67 | Frontal | Diplopia, facial pain, and headache | Hormonal block | Died a few months after presentation |
| Present case | 58 | Ethmoid and maxillary | Epistaxis, nasal obstruction, and diplopia | None | Died 2 months after diagnosis |
Imaging is not able to differentiate a local tumor from a metastasis; however, it is essential to determine location and extension and for surgical planning. CT may show enhancement, bone erosion, remodeling, and invasion. Magnetic resonance imaging (MRI) has an important role to help, defining leptomeningeal and orbital invasion [13]. Positron emission tomography (PET-CT) might be useful in the primary occult tumor.
Histopathology has an essential role in the diagnosis. When metastasizing to the paranasal sinuses, normally prostate carcinoma is not well differentiated. Immunohistochemical panel is also important, with positivity of prostate-specific antigen, prostate acid phosphatase, EpCam, NKX3.1, and prostein [36].
Usually, the diagnosis of a metastasis to the paranasal sinuses means a poor prognosis. An important factor that can be crucial is whether the metastasis is isolated or part of a widespread disease.
Normally, the treatment involving the metastasis to the paranasal sinuses is palliative, with the exception of an isolated metastasis, for which the radical surgery may be a viable option. The patient's quality of life should be a priority. The main goal is pain relief and bleeding prevention. Management has not changed greatly over the years, and therapy options include radiotherapy, chemotherapy, immunotherapy, and, more recently, endoscopic surgery [37].
Endoscopic surgery may provide symptom relief faster, with lower systemic and local side effects [37]. Tabaee et al. suggested three criteria to help in the decision of the surgery: reasonable expectation of improvement, possible prolongation of life, and survivability after anesthesia [38].
4. Conclusion
Despite being a rare entity, metastatic prostatic tumor in the paranasal sinuses should always be part of the differential diagnosis in patients with known prostatic tumor and recently developed nasal or orbital symptoms.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- 1.Bossi P., Farina D., Gatta G., Lombardi D., Nicolai P., Orlandi E. Paranasal sinus cancer. Critical Reviews in Oncology/Hematology. 2016;98:45–61. doi: 10.1016/j.critrevonc.2015.09.009. [DOI] [PubMed] [Google Scholar]
- 2.Barnes L., Eveson J. W., Reichart P., Sidransky D. World Health Organization Classification of Tumours, Pathology and Genetics, Head and Neck Tumours. Lyon, France: IARC Press; 2005. [Google Scholar]
- 3.Jemal A., Siegel R., Ward E. Cancer statistics, 2008. CA: A Cancer Journal for Clinicians. 2008;58(2):71–96. doi: 10.3322/ca.2007.0010. [DOI] [PubMed] [Google Scholar]
- 4.Carlotta B., Auvinen A., Roobol M. J., et al. Metastatic prostate cancer incidence and prostate-specific antigen testing: new insights from the European randomized study of screening for prostate cancer. European Urology. 2015;68(5):885–890. doi: 10.1016/j.eururo.2015.02.042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lund V. J., Stammberger H., Nicolai P., et al. European position paper on endoscopic management of tumours of the nose, paranasal sinuses and skull base. Rhinology Supplement. 2010;22(1):1–143. [PubMed] [Google Scholar]
- 6.Prescher A., Brors D. Metastases to the paranasal sinuses: case report and review of the literature. Laryngorhinootologie. 2001;80(10):583–594. doi: 10.1055/s-2001-17835. in German. [DOI] [PubMed] [Google Scholar]
- 7.Bernstein J. M., Montgomery W. W., Balogh K., Jr. Metastatic tumors to the maxilla, nose, and paranasal sinuses. Laryngoscope. 1966;76(4):621–650. doi: 10.1288/00005537-196604000-00003. [DOI] [PubMed] [Google Scholar]
- 8.Oliver V. J., Valdés A. L., Morillo A. D., et al. Frontal ethmoid metastases of prostatic carcinoma. Report of one case and review of the literature. Acta Otorrinolaringológica Española. 2001;52(2):151–154. doi: 10.1016/s0001-6519(01)78191-5. [DOI] [PubMed] [Google Scholar]
- 9.Lee S. M., Kim Y. M., Kim B. M. Epistaxis as the first manifestation of silent renal cell carcinoma: a case report with relevant literature review. Iran Journal of Radiology. 2016;13(1):p. e31208. doi: 10.5812/iranjradiol.31208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bubendorf L., Schopfer A., Wagner U., et al. Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Human Pathology. 2000;31(5):568–583. doi: 10.1053/hp.2000.6698. [DOI] [PubMed] [Google Scholar]
- 11.Hunt J. L., Tomaszewski J. E., Montone K. T. Prostatic adenocarcinoma metastatic to the head and neck and the workup of an unknown epithelioid neoplasm. Head and Neck. 2004;26(2):171–178. doi: 10.1002/hed.10353. [DOI] [PubMed] [Google Scholar]
- 12.Gilson C., Manickavasagar T., Chowdhury S. Treatment of metastatic prostate cancer. Trends Urology & Men Health. 2015;6(4):7–12. doi: 10.1002/tre.466. [DOI] [Google Scholar]
- 13.Batson O. V. The function of the vertebral veins and their role in the spread of metastases. Annals of Surgery. 1940;112(1):138–149. doi: 10.1097/00000658-194007000-00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lopéz F., Devaney K. O., Hanna E. Y., Rinaldo A., Ferlito A. Metastases to nasal cavity and paranasal sinuses. Head and Neck. 2016;38(12):1847–1854. doi: 10.1002/hed.24502. [DOI] [PubMed] [Google Scholar]
- 15.Barrs D. M., McDonald T. J., Whisnant J. P. Metastatic tumors to the sphenoid sinus. Laryngoscope. 1979;89(8):1229–1243. doi: 10.1002/lary.1979.89.8.1239. [DOI] [PubMed] [Google Scholar]
- 16.McClatchey K. D., Lloyd R. V., Schaldenbrand J. D. Metastatic carcinoma to the sphenoid sinus. Case report and review of the literature. Archives Otorhinolaryngology. 1985;241(3):219–224. doi: 10.1007/bf00453691. [DOI] [PubMed] [Google Scholar]
- 17.Leduc D., Massot C., Crouzet G., et al. Metastase sphenocaverneuse d’un cancer prostatique. La Revue de Medécine Interne. 1986;7(1):70–73. doi: 10.1016/s0248-8663(86)80086-8. in French. [DOI] [PubMed] [Google Scholar]
- 18.Matsumoto I., Furusato M., Inomaia L., Wada T., Aizawa S. Prostatic cancer presenting as metastatic adenocarcinoma of sphenoid sinus. Acta Pathologica Japonica. 1986;36(11):1753–1756. doi: 10.1111/j.1440-1827.1986.tb02239.x. [DOI] [PubMed] [Google Scholar]
- 19.Har-el G., Avidor I., Weisbord A., Sidi J. Carcinoma of the prostate metastatic to the maxillary antrum. Head and Neck. 1987;10(1):55–58. doi: 10.1002/hed.2890100109. [DOI] [PubMed] [Google Scholar]
- 20.Mickel R. A., Zimmerman M. C. The sphenoid sinus—a site for metastasis. Otolaryngology-Head and Neck Surgery. 1990;102(6):709–716. doi: 10.1177/019459989010200614. [DOI] [PubMed] [Google Scholar]
- 21.Saleh H. A., O’Flynn P., Jones N. S. Prostatic metastases in the nose and paranasal sinuses. Journal of Laryngology Otology. 1993;107(7):629–632. doi: 10.1017/s0022215100123928. [DOI] [PubMed] [Google Scholar]
- 22.Fortson J. K., Bezmalinovic Z. L., Moseley D. L. Bilateral ethmoid sinusitis with unilateral proptosis as an initial manifestation of metastatic prostate carcinoma. Journal of the National Medical Association. 1994;86(12):945–948. [PMC free article] [PubMed] [Google Scholar]
- 23.Telera S., Carloia S., Cavallotti D., Bosco S., Manni M., Cecconi L. Sphenoidal metastasis from prostate carcinoma. Case report and review of literature. Neurochirurgie. 2001;47(1):61–65. [PubMed] [Google Scholar]
- 24.Lavasani L., Zapanta P. E., Tanna N., Sadeghi N. Metastasis of prostatic adenocarcinoma to the sphenoid sinus. Annals of Otology, Rhinology & Laryngology. 2006;115(9):690–693. doi: 10.1177/000348940611500907. [DOI] [PubMed] [Google Scholar]
- 25.Başeskioglu B., Esklçorapçi S., Ekici S., Baydar D. E., Kendi S., Özen H. Maxillary sinus metastasis of prostate cancer: a case report. Turkish Journal of Cancer. 2006;36(2):79–81. [Google Scholar]
- 26.Ibarguren R. L., Rodríguez J. G., Mateos A. V., Arin I. A., Grasa I. O., Peña C. P. Metástasis en senos paranasales secundaria a adenocarcinoma prostático. Archivos Españoles de Urología. 2007;60(9):1137–1140. doi: 10.4321/s0004-06142007000900017. in Spanish. [DOI] [PubMed] [Google Scholar]
- 27.El Khatib K., Moufid K., Abouchadi A., Nassih M., Rzin A. Maxillary metastasis revealing a prostate cancer. Revue Stomatologie Chirurgie Maxillo-Faciale. 2007;108(5):468–469. doi: 10.1016/j.stomax.2007.06.025. in French. [DOI] [PubMed] [Google Scholar]
- 28.Viswanatha B. Prostatic carcinoma metastatic to the paranasal sinuses: a case report. Ear Nose Throat Journal. 2008;87(9):519–520. [PubMed] [Google Scholar]
- 29.Tunio M. A., Rafi M., Mohsin R., Hashmi A., Raza S., Mubarak M. Ipsilateral ethmoid sinuses metastasis and proptosis: rare presentation of metastatic prostate cancer. Pakistan Journal of Medical Sciences. 2011;27(1):212–213. [Google Scholar]
- 30.Azarpira N., Ashraf M. J., Khademi B., Asadi N. Distant metastases to nasal cavities and paranasal sinuses case series. Indian Journal of Otolaryngology Head Neck Surgery. 2011;64(4):349–352. doi: 10.1007/s12070-011-0269-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Petersson F., Hui T. S., Loke D., Putti T. C. Metastasis of occult prostatic carcinoma to the sphenoid sinus: report of a rare case and a review of the literature. Head and Neck Pathology. 2012;6(2):258–263. doi: 10.1007/s12105-011-0307-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Puche-Sanz I., Vázquez-Alonso F., Flores-Martín J. F., Almonte-Fernández H., Cózar-Olmo J. M. Sphenoid sinus metastasis as the presenting manifestation of a prostatic adenocarcinoma: case report and overview of the literature. Case Reports in Oncological Medicine. 2012;2012:4. doi: 10.1155/2012/819809.819809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Akdemir F., Aldemir M., Çakar H., Güler G. Metastasis of prostate adenocarcinoma to the frontal and ethmoid sinus. Turkish Journal of Urology. 2016;42(4):299–302. doi: 10.5152/tud.2016.21957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Evarts M., Schuster R. A., Steehler M., Steehler K. Metastasis of prostate carcinoma to the paranasal sinuses: a case study. Journal of Case Reports in Medicine. 2016;5:1–3. doi: 10.4303/jcrm/235947. [DOI] [Google Scholar]
- 35.Lechien J. R., Doyen J., Khalife M., Saussez S. Prostatic carcinoma metastatic to frontal and cavernous sinuses: a case report. Brazilian Journal of Otorhinolaryngology. 2016 doi: 10.1016/j.bjorl.2016.05.005. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Amin M. B., Epstein J. I., Ulbright T. M., et al. Best practices recommendations in the application of immunohistochemistry in the prostate: report from the International Society of Urologic Pathology consensus conference. American Journal of Surgical Pathology. 2014;38(8):1017–1022. doi: 10.1097/pas.0000000000000254. [DOI] [PubMed] [Google Scholar]
- 37.Roberts J. M., Brook C., Parnes S. Palliative endoscopic surgery for sinonasal metastases: a case report and literature review. Ear Nose Throat Journal. 2015;94(2):24–26. doi: 10.1177/014556131509400215. [DOI] [PubMed] [Google Scholar]
- 38.Tabaee A., Nyquist G., Anand V. K., Singh A., Kacker A., Schwartz T. H. Palliative endoscopic surgery in advanced sinonasal and anterior skull base neoplasms. Otolaryngology-Head and Neck Surgery. 2010;142(1):126–128. doi: 10.1016/j.otohns.2009.09.021. [DOI] [PubMed] [Google Scholar]