

Abstract
Aim:
The aim and objective of this study was to evaluate and compare the sealing ability of EndoSequence BC RRM-fast set putty, Proroot mineral trioxide aggregate (MTA), and Zirconomer in the repair of furcal perforation by measuring dye leakage under stereomicroscope.
Methodology:
A standard access cavity was made on forty-eight extracted mandibular and maxillary first molars followed by creating a furcal perforation in the center of the pulp chamber by using No. 4 round bur (creating a perforation of 2 mm diameter). Teeth were categorized into 4 groups containing 12 samples in each group based on material used for furcation repair. Group 1 – Endosequence BC RRM-fast set putty; Group 2 – Zirconomer; Group 3-MTA (positive control); Group 4 – negative control. All groups were covered with two layers of clear varnish except for 2 mm around the perforation region. All the teeth were immersed in 2% methylene blue dye for 48 h for dye penetration. Teeth were sectioned buccolingually using a diamond disk. The sectioned teeth were examined under stereomicroscope with ×10 magnification for dye penetration.
Results:
Endosequence showed less microleakage than MTA but not statistically significant. Zirconomer showed statistically significant higher microleakage.
Conclusion:
Endosequence and MTA showed less microleakage hence can be used as furcation repair materials. Due to higher microleakage, Zirconomer should be avoided as furcation repair material. Due to its favorable cost, ready availability, and almost similar outcome as bioceramics, MTA is considered as an alternative to Endosequence and is the gold standard in furcation repair.
Keywords: Bioceramic, mineral trioxide aggregate, root repair material, Zirconomer (glass ionomer cement)
INTRODUCTION
Perforations can be defined as mechanical or pathologic communications between the root canal system and the external tooth surface.[1] Perforations of the pulp chamber and the root canal adversely affect the prognosis of the treatment. Ingle has found root perforations to be the second most common reason for endodontic failures accounting for 9.6% of all unsuccessful cases.[2]
Perforations occur mainly due to large carious lesions, pathological resorption, and iatrogenic. Iatrogenic causes include during root canal therapy, i.e., zip, strip, and furcation perforations or its aftermath, for example, postpreparation perforation. Types of perforations include strip perforations, mid rood perforations, and apical perforations.[3]
In general, perforations occur most commonly in mesila roots of mandibular molars and distal roots of maxillary molar. Perforation in any region, i.e., either furcation perforation or root perforation leads to leakage of bacteria and their toxic products into periodontal and periapical tissues from the tooth and vice versa leading to pain, swelling, and failure of the endodontic treatment. Untreated perforation may lead to periodontal infection and resorption of surrounding bone.[3]
The furcal area of the coronal third has been described as a “danger zone.” There is less tooth structure in this area compared with the outer canal wall. Perforations in the furcation regions are one of the leading causes of endodontic failure.[3] Furcation perforation is an artificial communication between pulp chamber and the supporting structures of the tooth through the floor of the pulp chamber. These furcal perforations cause periradicular break down with an eventual loss of gingival attachment followed by loss of tooth.[4]
The ideal material for treating endodontic perforations should induce osteogenesis and cementogenesis, biocompatible, nonabsorbable, radiopaque, bacteriostatic or bactericidal and easy to apply. The material should tightly seal the perforation against microleakage.[5]
Several materials have been recommended for perforation repair including zinc oxide eugenol cements (IRM and Super-EBA), glass ionomer cement (GIC), composite resins, resin modified glass ionomer, amalgam, gutta-percha, calcium hydroxide, cavit and recently mineral trioxide aggregate (MTA), biodentine, Endosequence root repair material.[6] None of these materials fulfill the ideal requirements of repair material.
More recently, MTA is being used as furcation repair material. MTA has shown to have good biocompatibility, lesser bacterial leakage, and improved adaptation to the cavity walls. It is considered as the gold standard for furcation repair.[7]
Zirconomer (Zirconia + GIC) is a recently launched glass ionomer formulation to overcome the disadvantages of traditional GIC formulations. It has the strength of amalgam along with the beneficial effects of GIC's and eliminates the hazardous effect of mercury; hence, it is also termed as white amalgam.[8]
Bioceramic materials are bioinert, highly biocompatible, antibacterial, osteogenic, highly resistant to wash out, nonstaining and have a short setting time.[9]
Recently, Endosequence bioceramic root repair material fast set putty has been developed by Brassler USA. The material is available as premixed putty consistency to improve the handling characteristics and has short setting time. It is recommended for use in root repair, retrograde filling material, and pulp capping.[9]
The aim of the study was to evaluate and compare bioceramics and zirconia-reinforced GIC in sealing the furcal perforations using dye penetration method observed under stereomicroscope.
Objectives
This study serves the following purposes:
To analyze the sealing ability of bioceramics and zirconia-reinforced GIC in repair of furcation perforations in molars by using dye penetration technique under a stereomicroscope
To compare the sealing ability of bioceramics, zirconia-reinforced GIC, and MTA as furcal perforation repair materials.
METHODOLOGY
Tooth selection and preparation
The study was conducted on 48 extracted human molars collected from the Department of Oral and Maxillofacial surgery.
Inclusion criteria
Noncarious or minimal carious molars with two or more roots.
Teeth with Intact furcation.
Exclusion criteria
Teeth with extensive caries
Teeth with cracks
Teeth with fused roots
Teeth with dilacerations.
Sample collection
Forty-eight freshly extracted human mandibular and maxillary first molar teeth were collected, stored, and disinfected according to OSHA regulations.
Sample preparation
Access cavity preparation was done on forty-eight molars with Endo access and Endo-Z bur [Dentsply, Maillefer, Tulsa Dental, Tulsa, USA]. The roots were cut 3 mm below the furcation by using diamond disc [Mani Inc., Utsunomiya, Japan] on a straight handpiece. A temporary filling material zinc oxide eugenol cement was placed over the root canal orifice. In the center of furcation region, a perforation was done with the help of long shank round bur no #4 (2 mm in diameter).
The teeth samples were randomly categorized into 4 groups containing 12 samples each:
Experimental groups
Group 1 – Furcal perforation repair was done using Endosequence BC RRM
Group 2 –Furcal perforation repair was done using Zirconomer.
Control groups
Group 3 – Furcal perforation repair was done with MTA which served as positive control
Group 4 – Furcal perforations left unsealed acted as negative control.
All teeth in Groups 1, 2, and 3 were sealed with repair materials in the furcation perforation till the level of pulpal floor. A moist cotton pellet was introduced at the furcation region to imitate oral conditions. No attempt was made to prevent the overextension of the repair material [Figure 1]. After furcal repair, access restoration of all the samples was done with light cure composite resin.
Figure 1.
Materials used in the study
Sample evaluation
Clear varnish was applied on all the samples except for 2 mm around the perforation region. All the teeth were immersed in 2% methylene blue dye for 48 h for retrograde dye penetration. After 48 h, all the samples were cleaned under running water to clear the methylene blue dye. Teeth were dried, and all the teeth were sectioned in center buccolingually using a diamond disc. The sectioned teeth were examined under stereomicroscope with ×10 magnification for dye penetration. The images were captured using a Motic M210 camera. The microscopic images of perforation site were observed in a computer screen with 640 × 480 resolution, and the length of dye penetration was measured with Motic image plus software. The extent of dye leakage was measured as the most coronal linear extent of dye penetration from the most apical extent of perforation. For each tooth, the length of the perforation wall and the linear leakage of dye penetration were measured in millimeters (mm).
Statistical methods
All the data were subjected to statistical analysis. The length of the perforation of all the samples was statistically analyzed using one-way ANOVA test. The difference in dye penetration depth and percentage of dye penetration by the groups were statistically analyzed using Kruskal–Wallis test, and Mann–Whitney U-test was used for pairwise comparison between groups because of significant results of Kruskal–Wallis test.
RESULTS
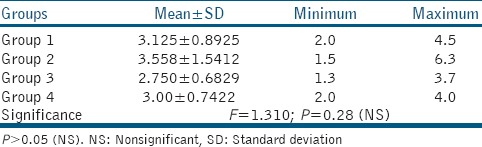
The mean length of perforation in Group 1 (Endosequence) is 3.12 ± 0.8, Group 2 (Zirconomer) is 3.55 ± 1.5, Group 3 (MTA) is 2.75 ± 0.6, and Group 4 (negative control) is 3.0 ± 0.7. The results are not statistically significant (P = 0.28) [Table 1].
Table 1.
Comparison of perforation length between groups in mm
The mean dye leakage of Group 1 is 0.08 ± 0.1, Group 2 is 0.55 ± 0.8, Group 3 is 0.15 ± 0.1, and Group 4 is 3 ± 0.7. Hence, all the experimental materials showed dye leakage [Table 2 and Figure 2].
Table 2.
Comparison of dye penetration between groups in mm
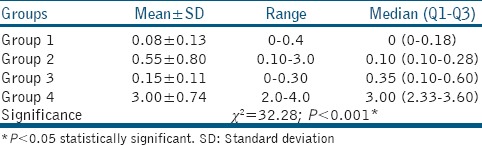
Figure 2.
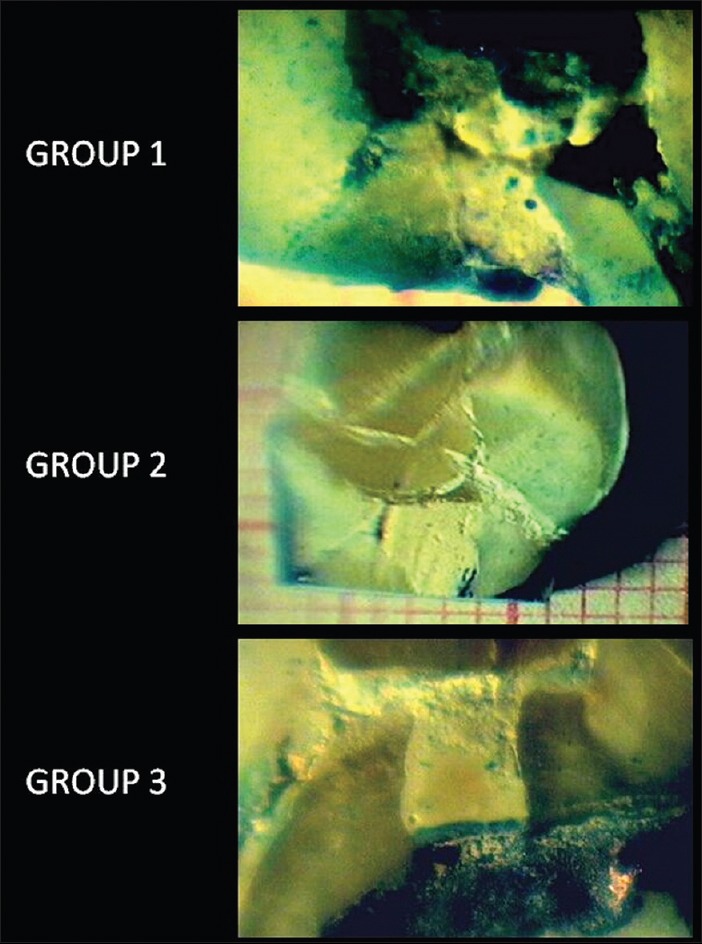
Dye penetration in different groups
Results showed that Group 4 (negative control) showed maximum mean dye penetration compared to other 3 groups. Endosequence group showed least dye penetration followed by MTA group and Zirconomer group which are statistically significant. The Kruskal–Wallis test depicted overall significant difference between the groups in dye penetration, so Mann–Whitney U-test for pairwise comparison between the means of the groups was performed.
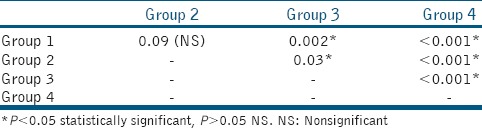
Endosequence group and MTA group showed statistically significant less dye penetration compared to Zirconomer group. All groups showed statistically significant less dye penetration compared to negative control group. There is no statistically significant difference in dye penetration between Endosequence group and MTA group (P = 0.09) [Table 3].
Table 3.
Pairwise comparison of dye penetration (mm) between groups
DISCUSSION
The prognosis of furcation perforation depends on time, size, and cause. Good prognosis is seen with small sized perforations and immediate treatment of perforation site, as it reduces the destructive inflammatory response of periodontium.[10]
Favorable prognosis of perforation is seen when it is sealed immediately either iatrogenic or pathologic. Any delay results in infection of perforation wound and delayed healing. Prognosis also depends on perforation and its relationship to gingival sulcus. Furcation perforations have doubtful prognosis because of close relation to gingival sulcus.[3]
Pathologic root perforations occur due to root resorption or dental caries. Root resorption is due to continued action of osteoclastic cells on cementum and dentine. Internal root resorption occurs within the root canal system, whereas external root resorption occurs due to damage to cementum or periodontal ligament on the root surface. Treatment of pathologic resorption may include pulp space therapy, crown lengthening or either surgical repair or root resection. However, perforations in these cases cause tooth unrestorable.[11]
In the present study, sealing ability of Endosequence bioceramic root repair material-fast set putty, zirconia-reinforced GIC, and MTA were evaluated and compared when used in furcation repair using dye penetration method.
Microleakage studies are always a challenging task because of lack of appropriate test methods. There is no standardized leakage test to evaluate the sealing ability of endodontic materials.[12]
Despite the vilification, dye penetration studies still remain best method for evaluating the sealing ability of the materials. The use of dyes is one of the most common and oldest methods of studying microleakage. Hence, the present study was conducted based on dye penetration methodology using methylene blue.[12]
The main advantages of aqueous methylene blue dye are the following:[6]
Easily penetrates water compartment of the tooth
Does not react with hard tissues of tooth
Particle size is comparable to size of microorganisms
It is readily detectable under visible light.
The limitations of a dye penetration study are the following:[13]
Destruction of specimens is necessary
Results are subjectively evaluated; hence, operator expertise is needed
It is considered as semiquantitative method of measuring microleakage.
The length of the perforation is not standardized because the length of furcation region is not constant in any tooth. Statistical analysis showed no significant difference between groups in the length of the furcation.
The results showed least mean dye leakage with Endosequence BC RRM-fast set putty (0.08 ± 0.13 mm) followed by MTA (0.15 ± 0.11 mm) and highest dye leakage with Zirconomer (0.55 ± 0.80 mm). However, there is no statistically significant difference in the mean dye penetration of Endosequence group and MTA group.
This was in accordance with previous studies on Endosequence BC RRM and MTA by Antunes et al.[14] and Jeevani et al.;[15] contrary to this, Hirschberg et al.[16] in their study showed the highest leakage in Endosequence BC RRM than MTA. This may be due to the different study designs used in that study and the material used. The present study used Endosequence BC RRM fast-set putty. The least dye penetration may be attributed to the following reasons:
Due to its nanoparticle size of the material which results in deeper penetration of the material into dentinal tubules, thus rendering a fluid-tight seal[17]
Premixed form of material which reduces the air entrapment in the mix, putty consistency gives better adaptability to dentinal walls and gives excellent handling of the material.[17]
The microleakage of MTA is in close relation to Endosequence BC RRM-fast set putty and better than Zirconomer.
MTA is water-based cement which sets in the presence of water; hence, it results in better flow and wettability thereby good adaptation to the dentinal walls[18]
The ability of MTA to expand while setting which more effectively adapts to the dentinal walls.[19]
The probable causes for slightly more microleakage of MTA compared to Endosequence BC RRM fast-set putty could be due to the following:[20]
Long setting time
Difficult handling of the material
Presence of voids.
The main advantages of Zirconomer include the following:
Increased strength
Chemical bonding to the tooth structure
Fluoride release.
GIC has been used as furcation repair material. Studies showed better sealing ability than conventional materials due to its adhesive properties.[5] Alhadainy did two subsequent studies showed light cured GIC had better sealing ability compared to amalgam and cavit and better sealing than chemically cured GIC.[21,22] Till date, Zirconomer has not been used as furcation repair material. However, previous studies on Zirconomer as a coronal restoration by Patel et al.[23] also showed increase dye leakage which is in accordance to our study.
The highest microleakage was seen with Zirconomer compared to Endosequence and MTA. The probable causes could be:
In the present study, the material might be slightly viscous which prevented the material to flow and might have inadequately filled or sealed the perforation
GIC is moisture sensitive. Presence of moisture in the furcation perforation (here in the study wet cotton was placed at the furcation site to simulate oral environment) might have adversely affected the sealing ability of the material.
CONCLUSION
Within the limitations of this study, the following conclusions can be made:
The results of the present study showed Endosequence BC RRM-fast set putty, and MTA has better sealing ability compared to Zirconomer
MTA showed more dye leakage than Endosequence BC RRM-fast set putty though the results were statistically not significant
Zirconomer showed statistically significant more dye leakage compared to Endosequence BC RRM-fast set putty and MTA
All the experimental materials in the present study showed microleakage.
The outcome of the present in vitro study is the use of Endosequence BC RRM is encouraging compared to Zirconomer usage as furcation repair material. Even though MTA showed more microleakage compared to Endosequence BC RRM, due to its favorable cost, ready availability, and almost similar outcome as Endosequence, MTA is considered as the gold standard in furcation repair.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.American Association of Endodontists. Glossary of Endodontic Terms. 7th ed. Chicago, IL: American Association of Endodontics; 2003. [Google Scholar]
- 2.Ingle JI. A standard endodontic technique utilizing newly designed instruments and filling materials. Oral Surg Med Oral Pathol. 1961;14:83–91. doi: 10.1016/0030-4220(61)90477-7. [DOI] [PubMed] [Google Scholar]
- 3.Alhadainy HA. Root perforations. A review of literature. Oral Surg Oral Med Oral Pathol. 1994;78:368–74. doi: 10.1016/0030-4220(94)90070-1. [DOI] [PubMed] [Google Scholar]
- 4.Lemon RR. Nonsurgical repair of perforation defects. Internal matrix concept. Dent Clin North Am. 1992;36:439–57. [PubMed] [Google Scholar]
- 5.Kakani AK, Veeramachaneni C, Majeti C, Tummala M, Khiyani L. A review on perforation repair materials. J Clin Diagn Res. 2015;9:ZE09–13. doi: 10.7860/JCDR/2015/13854.6501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wu MK, Wesselink PR. Endodontic leakage studies reconsidered. Part I. Methodology, application and relevance. Int Endod J. 1993;26:37–43. doi: 10.1111/j.1365-2591.1993.tb00540.x. [DOI] [PubMed] [Google Scholar]
- 7.Roberts HW, Toth JM, Berzins DW, Charlton DG. Mineral trioxide aggregate material use in endodontic treatment: A review of the literature. Dent Mater. 2008;24:149–64. doi: 10.1016/j.dental.2007.04.007. [DOI] [PubMed] [Google Scholar]
- 8.Walia R, Jasuja P, Verma KG, Juneja S, Mathur A, Ahuja L, et al. A comparative evaluation of microleakage and compressive strength of Ketac Molar, Giomer, Zirconomer, and Ceram-x: An in vitro study. J Indian Soc Pedod Prev Dent. 2016;34:280–4. doi: 10.4103/0970-4388.186746. [DOI] [PubMed] [Google Scholar]
- 9.Wang Z. Bioceramic materials in endodontics. Endod Topics. 2015;32:3–30. [Google Scholar]
- 10.Seltzer S, Sinai I, August D. Periodontal effects of root perforations before and during endodontic procedures. J Dent Res. 1970;49:332–9. doi: 10.1177/00220345700490022301. [DOI] [PubMed] [Google Scholar]
- 11.Saed SM, Ashley MP, Darcey J. Root perforations: Aetiology, management strategies and outcomes. The hole truth. Br Dent J. 2016;220:171–80. doi: 10.1038/sj.bdj.2016.132. [DOI] [PubMed] [Google Scholar]
- 12.Pashley DH, Thompson SM, Stewart FP. Dentin permeability: Effects of temperature on hydraulic conductance. J Dent Res. 1983;62:956–9. doi: 10.1177/00220345830620090801. [DOI] [PubMed] [Google Scholar]
- 13.Camps J, Pashley D. Reliability of the dye penetration studies. J Endod. 2003;29:592–4. doi: 10.1097/00004770-200309000-00012. [DOI] [PubMed] [Google Scholar]
- 14.Antunes HS, Gominho LF, Andrade-Junior CV, Dessaune-Neto N, Alves FR, Rôças IN, et al. Sealing ability of two root-end filling materials in a bacterial nutrient leakage model. Int Endod J. 2016;49:960–5. doi: 10.1111/iej.12543. [DOI] [PubMed] [Google Scholar]
- 15.Jeevani E, Jayaprakash T, Bolla N, Vemuri S, Sunil CR, Kalluru RS, et al. “Evaluation of sealing ability of MM-MTA, endosequence, and biodentine as furcation repair materials: UV spectrophotometric analysis”. J Conserv Dent. 2014;17:340–3. doi: 10.4103/0972-0707.136449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hirschberg CS, Patel NS, Patel LM, Kadouri DE, Hartwell GR. Comparison of sealing ability of MTA and EndoSequence Bioceramic Root Repair Material: A bacterial leakage study. Quintessence Int. 2013;44:e157–62. [PubMed] [Google Scholar]
- 17.Moinzadeh AT, Aznar Portoles C, Schembri Wismayer P, Camilleri J. Bioactivity potential of EndoSequence BC RRM putty. J Endod. 2016;42:615–21. doi: 10.1016/j.joen.2015.12.004. [DOI] [PubMed] [Google Scholar]
- 18.Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling material. J Endod. 1993;19:591–5. doi: 10.1016/S0099-2399(06)80271-2. [DOI] [PubMed] [Google Scholar]
- 19.Torabinejad M, Smith PW, Kettering JD, Pitt Ford TR. Comparative investigation of marginal adaptation of mineral trioxide aggregate and other commonly used root-end filling materials. J Endod. 1995;21:295–9. doi: 10.1016/S0099-2399(06)81004-6. [DOI] [PubMed] [Google Scholar]
- 20.Parirokh M, Torabinejad M. Mineral trioxide aggregate: A comprehensive literature review – Part III: Clinical applications, drawbacks, and mechanism of action. J Endod. 2010;36:400–13. doi: 10.1016/j.joen.2009.09.009. [DOI] [PubMed] [Google Scholar]
- 21.Alhadainy HA, Himel VT. Evaluation of the sealing ability of amalgam, Cavit, and glass ionomer cement in the repair of furcation perforations. Oral Surg Oral Med Oral Pathol. 1993;75:362–6. doi: 10.1016/0030-4220(93)90152-t. [DOI] [PubMed] [Google Scholar]
- 22.Alhadainy HA, Himel VT. Comparative study of the sealing ability of light-cured versus chemically cured materials placed into furcation perforations. Oral Surg Oral Med Oral Pathol. 1993;76:338–42. doi: 10.1016/0030-4220(93)90264-5. [DOI] [PubMed] [Google Scholar]
- 23.Patel MU, Punia SK, Bhat S, Singh G, Bhargava R, Goyal P, et al. An in vitro evaluation of microleakage of posterior teeth restored with amalgam, composite and zirconomer – A stereomicroscopic study. J Clin Diagn Res. 2015;9:ZC65–7. doi: 10.7860/JCDR/2015/13024.6225. [DOI] [PMC free article] [PubMed] [Google Scholar]