

Abstract
Introduction
Research on the shift in children's Body Mass Index (BMI) distribution is limited and conditional mean models used in the previous research have limitations in capturing cross-distribution variations in effects. The objectives are to analyze the shift in Chinese children’s BMI distribution and to test the associations between BMI distribution and other factors.
Methods
We analyzed data collected from children 7–17 years old from the China Health and Nutrition Survey (CHNS) conducted in 1997, 2000, 2004, 2006, 2009 and 2011, from 2,814 participants with 6,799 observations. Longitudinal quantile regression (QR) was used to explore the effect of several factors on BMI trends in 2015.
Results
The BMI curves shift to the right in boys and girls, with the distributions becoming wider, indicating a higher proportion of children have become overweight. The 5th, 15th, 50th, 85th and 95th BMI percentile curves all shifted upward from 1997 to 2011, and the higher percentiles had greater increases. The prevalence of overweight and obesity increased in boys and girls between 1997–2011, from 6.5% to 15.5% in boys and from 4.6% to 10.4% in girls. Energy intake and parents’ BMI levels had a positive association with children’s BMI. Per capita income was positively associated with changes in BMI only at the upper percentiles of the BMI distributions in boys. Increased physical activity was associated with decreased BMI in girls.
Conclusions
Children in China are becoming increasingly overweight. Energy intake, parental BMI, physical activity and early menarche age in girls are associated with elevated BMI in children.
Keywords: body mass index, obesity, overweight, adolescent, quantile regression
Introduction
In Chinese children and adolescents, it is common to see problems of underweight, stunting and micronutrient deficiencies in parallel with an increasing prevalence of overweight and obesity (1, 2). Childhood obesity has become an increasingly serious public health problem because of the risk for both short-term health consequences and long-term carry-over of obesity into adulthood (3, 4).
The increasing prevalence of childhood overweight and obesity in China has been well documented by national data. National surveys on Chinese school-aged children and adolescents show that in 2010, 15.0% of school-aged children were overweight or obese in China (9.9% overweight; 5.1% obese), after having been < 3.0% in 1985. Nationwide, 19.0% of boys and 10.9% of girls were overweight or obese in 2010 (5).
Overweight and obesity are often defined based on Body Mass Index (BMI). A rightward shift in BMI distribution has been observed among Chinese adults (6) and children(5). But related research in children is still limited. The effect of an obesity covariate may reasonably be hypothesized to vary across the BMI distribution (7, 8). Therefore, this study examined the shifts over time in child and adolescent BMI distributions and assessed the relationships between BMI and key covariates using data collected from a longitudinal survey.
Methods and Materials
Study Design and Study Population
We used data from the China Health and Nutrition Survey (CHNS), a prospective household-based study, across nine rounds of surveys between 1989 and 2011 covering nine provinces. Within each province, a multistage, stratified, random cluster sampling design was used to ensure a suitable representation of the population (9, 10). Data were collected on health, nutrition and socioeconomic variables at community, household and individual levels by questionnaire, dietary survey and physical measurements methods. We have obtained Institutional Review Board (IRB) clearance from UNC-Chapel Hill and from National Institute for Nutrition and Health. Further information on survey procedures and the rationale can be found in the cohort profile (10).
Our sample included children aged 7–17 years from nine provinces who were included in the six rounds of survey data collected in 1997, 2000, 2004, 2006, 2009 and 2011, participants with at least two measurements (N = 2,814) to assess temporal trends for these individuals. Data from the 1989, 1991 and 1993 surveys were not included because some of the covariates, such as physical activity and time of sedentary behaviors, were not collected. Observations were excluded from the analysis if a participant was missing weight or height. The final analysis sample included 2,814 participants with 6,799 observations, for an average of approximately 2.5 observations per subject.
Outcome variables
The key outcome of interest was BMI (kg/m2). Height was measured without shoes to the nearest 0.2 cm using portable SECA206 wall-mounted metal tapes, weight was measured without shoes and in light clothing to the nearest 0.1 kg on a calibrated beam SECA 880 scales. Identical anthropometric measurement techniques were used in all surveys.
Covariates
Physical activity (PA) and sedentary behaviors
Using the CHNS survey data, the average of metabolic equivalents of task (MET) hours per day in a week was estimated to indicate the PA level, including four domains of PA: Occupational, Domestic, Active Leisure and Travel. This measurement accounts for both the average intensity of each activity and the time spent in each activity. Sedentary behavior was calculated as average of hours per day in a week with low MET values due to sedentary activity.
Per capita family annual Income
Per capita income was based on reported gross annual per capita household income, which was inflated to 2011 values using the Consumer Price Index. (11)
Energy intake
Detailed dietary consumption data at both the household and individual levels were collected over three consecutive days to determine the average daily energy intake for each individual. (12, 13)
Parents’ education level
The parents’ education level was based on their formal education years.
Urbanicity index
This index was calculated at the community level using a multicomponent continuous scale. Communities could receive a maximum of 10 points for each of 12 components including population density, economic activity, traditional markets, modern markets, transportation infrastructure, sanitation, communications, housing, education, diversity, health infrastructure, and social services.(14)
Survey time
Time was included as a continuous measure, defined as years since 1997.
First menstruate age
The girls were classified as earlier age at menarche, if their first menstruate age were less than 13 years old.
Statistical analysis
First, we conducted descriptive analysis stratified by gender. As the distributions were not normal distributions, we used the Kruskal-Wallis test and the chi-squared test to examine the difference in means (or percentages) of these variables over time. These analyses were done in 2015.
Overweight and Obesity were classified using the IOTF age- and sex-specific BMI ≥ 25kg/m2 and BMI ≥ 30kg/m2 respectively. Chi-squared tests were used to test the statistically significant differences in prevalence of overweight and obesity. Descriptive analysis was done using SAS 9.3.
The BMI distribution and percentile curves were constructed for 1997 and 2011, by gender, using the LMS (lambda, mu, and sigma) method. (15, 16) VGAM package in R version 2.15.1 was used in the LMS methods.
Longitudinal quantile regression was used to investigate changes in the BMI distribution over time. Compared to traditional linear regression based on the conditional mean, this method is more suitable in cases where the effect of covariates differs at different levels of the response variable. Moreover, the technique allowed us to make better use of the information provided by the repeated measurements collected on the same individual over time and to handle the skewed distribution of the outcome variable to describe the full distribution (17). We were interested in testing whether the noted changes in BMI distribution over time were due to secular trends or other individual-level factors such as age, physical activity, sedentary behavior, or household-level factors such as parents’ education level, parents’ BMI level, per capita family annual income level or the degree of urbanicity of their community. For comparison, we also ran the least squared model to estimate the mean regression to look at predictors of the mean BMI.
We fitted three models: Model 1 controlled for time only where the “time” serves as a surrogate for time-dependent variables; so the coefficients tell us what change in BMI was associated with each additional year at a particular percentile of the BMI distribution; Model 2 controlled for time, individual and household factors (i.e., age, PA, sedentary hours, parents’ education level, parents’ BMI and per capita family annual income); and Model 3 controlled for time, individual and household characteristics, as well as the community urbanization index. Longitudinal quantile regressions were conducted using R version 2.15.1.
Results
Individual, household, and community factors changes
We also examined changes in individual, household, and community factors associated with children’s and adolescents’ weight status. Summary statistics for all the variables examined are presented in Table 1. From 2004 to 2011, the boy's PA levels decreased from 9.1 METs/d to 7.1 METs/d, from 6.7 METs/d to 5.6 METs/d in girls, while the sedentary time out of school, including watching TV and doing homework, remained relatively stable at 2 – 2.5 hours per day. The average of parents’ BMI, parents’ education years and per capita income increased for both genders.
Table 1.
Changes over time in characteristics of children and their families in China, 1997–2011
| 1997 Mean (SD) |
2000 Mean (SD) |
2004 Mean (SD) |
2006 Mean (SD) |
2009 Mean (SD) |
2011 Mean (SD) |
Time trend, P valuea |
|
|---|---|---|---|---|---|---|---|
| Boys | |||||||
| N | 723 | 946 | 678 | 516 | 456 | 309 | |
| Age (years) | 10.0 (2.1) | 11.9 (2.7) | 12.4 (3.1) | 11.8 (3.2) | 11.8 (2.8) | 12.6 (2.3) | <0.0001 |
| Height (cm) | 134.5 (13.2) | 146.0 (16.2) | 150.0 (17.7) | 147.2 (18.9) | 148.8 (16.7) | 153.9 (14.8) | <0.0001 |
| Weight (kg) | 30.4 (8.6) | 38.6 (12.3) | 42.2 (14.1) | 40.1 (14.5) | 41.0 (13.9) | 45.5 (14.6) | <0.0001 |
| BMI (kg/cm2) | 16.5 (2.4) | 17.6 (2.7) | 18.1 (2.9) | 17.9 (3.1) | 18.0 (3.3) | 18.7 (3.7) | <0.0001 |
| Overweight and obesity (%) | 6.5 | 7.5 | 9.3 | 11.0 | 14.3 | 15.5 | <0.0001b |
| PA (METs/d) | 3.7 (4.9) | 5.9 (5.7) | 9.1 (10.8) | 7.5 (8.9) | 7.6 (8.6) | 7.1 (7.1) | <0.0001 |
| Sedentary (hrs/d) | 1.8 (1.1) | 1.5 (1.0) | 2.3 (1.4) | 2.5 (1.4) | 2.4 (1.5) | 2.1 (1.3) | <0.0001 |
| Energy (kcal) | 2033 (674.0) | 2121 (700.6) | 2150 (749.7) | 2044 (711.9) | 1958 (701.6) | 1953 (690.6) | <0.0001 |
| Family characteristics | |||||||
| Father BMI (kg/cm2) | 22.3 (2.7) | 22.7 (2.9) | 22.9 (3.1) | 23.0 (3.1) | 23.4 (3.3) | 23.9 (3.3) | <0.0001 |
| Mother BMI (kg/cm2) | 22.2 (2.6) | 22.6 (2.8) | 22.8 (3.0) | 23.0 (5.8) | 23.0 (3.2) | 23.1 (3.4) | <0.0001 |
| Father Education (years) | 8.2 (3.1) | 8.4 (2.9) | 8.7 (2.8) | 9.1 (3.0) | 8.8 (3.1) | 9.2 (3.0) | <0.0001 |
| Mother Education (years) | 6.7 (3.8) | 7.0 (3.7) | 7.7 (3.3) | 8.2 (3.3) | 8.0 (3.2) | 8.4 (3.2) | <0.0001 |
| Per capital family income (1000Yuan/Y) | 3.8 (3.0) | 4.6 (4.4) | 5.7 (5.5) | 6.7 (6.7) | 9.9 (10.5) | 11.7 (14.6) | <0.0001 |
| Urbanization index | 49.0 (16.9) | 53.9 (17.0) | 58.6 (19.4) | 60.8 (20.2) | 63.1 (19.6) | 67.1 (19.1) | <0.0001 |
| Girls | |||||||
| N | 606 | 836 | 603 | 463 | 384 | 279 | |
| Age (years) | 10.1 (2.1) | 11.9 (2.8) | 12.1 (3.0) | 11.9 (2.9) | 11.5 (2.8) | 12.6 (2.4) | <0.0001 |
| Height (cm) | 134.8 (13.4) | 144.2 (13.6) | 145.5 (15.1) | 145.2 (15.1) | 144.9 (14.6) | 149.5 (11.6) | <0.0001 |
| Weight (kg) | 30.3 (8.8) | 37.1 (10.8) | 38.6 (11.8) | 37.9 (11.4) | 37.8 (12.2) | 41.6 (11.7) | <0.0001 |
| BMI (kg/cm2) | 16.3 (2.2) | 17.4 (2.7) | 17.7 (2.9) | 17.6 (3.0) | 17.5(3.2) | 18.2(3.4) | 0.0149 |
| Overweight and obesity (%) | 4.6 | 4.8 | 7.0 | 7.3 | 9.2 | 10.4 | <0.0001b |
| PA (METs/d) | 3.4 (4.9) | 4.5 (5.1) | 6.7 (8.5) | 6.3 (8.2) | 4.5 (4.8) | 5.6 (4.7) | <0.0001 |
| Sedentary (METs/d) | 1.8 (1.2) | 1.6 (1.1) | 2.2 (1.3) | 2.3 (1.2) | 2.5 (1.5) | 2.2 (1.1) | <0.0001 |
| Energy (kcal) | 1872 (593.4) | 1887 (589.5) | 1810 (610.3) | 1861 (607.6) | 1669 (515.1) | 1696 (682.2) | <0.0001 |
| Family characteristics | |||||||
| Father BMI (kg/cm2) | 22.3 (2.8) | 22.8 (2.9) | 23.0 (3.0) | 22.9 (3.1) | 23.2 (3.6) | 23.8 (3.3) | <0.0001 |
| Mother BMI (kg/cm2) | 22.6 (2.9) | 22.6 (2.8) | 22.8 (3.2) | 23.0 (3.1) | 22.9 (3.4) | 22.8 (3.2) | <0.0001 |
| Father Education (years) | 8.1 (3.1) | 8.4 (2.9) | 9.0 (2.8) | 9.2 (3.1) | 8.6 (3.0) | 8.5 (3.2) | <0.0001 |
| Mother Education (years) | 6.4 (3.9) | 7.0 (3.7) | 7.7 (3.4) | 8.0 (3.7) | 8.0 (3.2) | 8.2 (3.2) | <0.0001 |
| Per capital family income (1000Yuan/Y) | 3.5 (2.7) | 4.6 (4.4) | 5.7 (5.5) | 6.5 (6.4) | 9.2 (10.4) | 10.6 (15.0) | <0.0001 |
| Urbanization index | 50.0 (17.3) | 54.8 (17.2) | 58.9 (19.4) | 61.2 (19.2) | 64.6 (18.7) | 68.6 (18.0) | <0.0001 |
Kruskal-Wallis Test
Chi-squared Test
Trends of BMI distribution in boys and girls, 1997 to 2011
Figure 1 shows the smoothed distribution curves (using the LMS method) of BMI shifted over time among boys and girls age 7–17 years, for select years. For both genders, the main characteristics of the changes were the shift in the curves to the right, with the distributions becoming wider and with a higher proportion of the samples having a higher BMI. From 2006 to 2011, the distribution curve remained stable in boys and moved a little to left in girls. The dispersion of the BMI distributions increased from 1997 to 2006 and from 1997 to 2011, but it was stable from 2006 to 2011. The standard deviation increased from 2.4 to 3.7 for boys and from 2.2 to 3.4 for girls.
Figure 1.
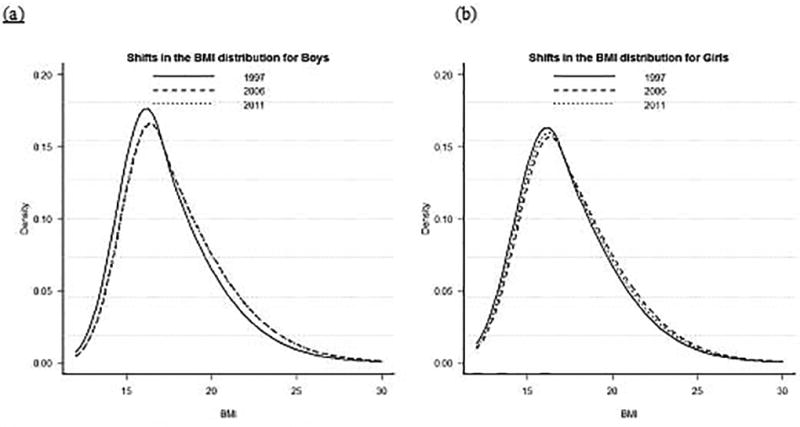
Shift in BMI Distribution in Chinese Boys and Girls aged 7–17 years, 1997 to 2011
Over-time shifts in the 5th, 15th, 50th, 85th, and 95th percentile BMI curves
Figure 2 shows the BMI percentile curves constructed using the LMS method for the years 1997 and 2011, by gender and age. All the percentile curves showed increasing trends from 1997 to 2011, with greater increases in the higher percentiles for all gender and age groups. For each percentile curve, the increases for girls were less than for boys.
Figure 2.
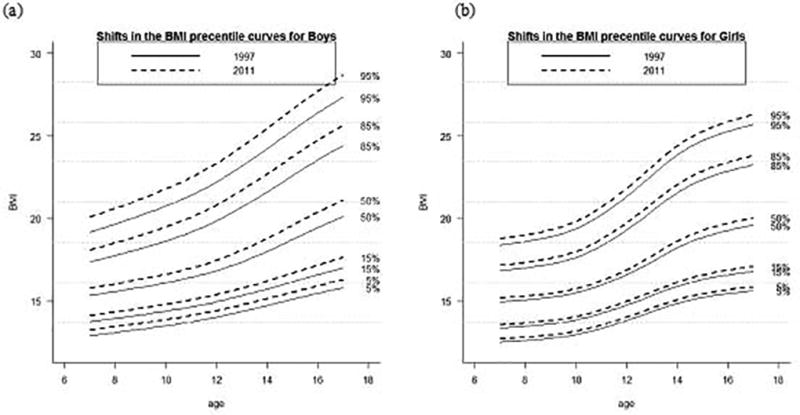
Shift in the BMI Percentile Curves in Chinese Boys and Girls Aged 7–17 years old, 1997 to 2011
Yearly change in percentile BMI based on longitudinal quantile regression
Table 2 shows the yearly change in percentile BMI among boys and girls based on longitudinal quantile regression. The results from Model 1 appear to suggest a significant increase from the 5th percentile to the 95th percentiles for both boys and girls. The increases were greater at the upper percentiles versus at the lower percentiles. For example, at the 85th percentile BMI increased 0.54 kg/m2 (95% CI: 0.50, 0.58) and 0.62 kg/m2 (95% CI: 0.58, 0.66) in boys and girls, respectively. At the 15th percentile, the increases were 0.41 kg/m2 (95% CI: 0.39, 0.43) and 0.48 kg/m2 (95% CI: 0.44, 0.52) in boys and girls, respectively. After controlling for individual- and household-level factors in Model 2 and for urbanicity in Model 3, the time effect became insignificant at both the lower tail and the upper tail of the BMI distribution.
Table 2.
Quantile regression results for 5th, 15th, 50th, 85th and 95th percentiles year coefficients in children in China, by sex
| Year effects | 5th | 15th | 50th | 85th | 95th | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
| Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | ||
| Boys | |||||||||||
| BMI (kg/cm2) in 1997 | 13.79 | 14.79 | 16.87 | 20.20 | 22.22 | ||||||
| Model 1a | 0.41*** | 0.01 | 0.41*** | 0.01 | 0.50*** | 0.01 | 0.54*** | 0.01 | 0.63*** | 0.04 | |
| Model 2b | 0.24 | 0.21 | 0.24 | 0.22 | 0.25 | 0.22 | 0.26 | 0.22 | 0.30 | 0.22 | |
| Model 3c | 0.25 | 0.21 | 0.25 | 0.21 | 0.26 | 0.21 | 0.25 | 0.21 | 0.30 | 0.21 | |
| Girls | |||||||||||
| BMI (kg/cm2) in 1997 | 13.54 | 14.58 | 16.86 | 20.12 | 22.25 | ||||||
| Model 1a | 0.47*** | 0.02 | 0.48*** | 0.02 | 0.55*** | 0.02 | 0.62*** | 0.22 | 0.68*** | 0.03 | |
| Model 2b | −0.26 | 0.26 | −0.25 | 0.26 | −0.24 | 0.26 | −0.23 | 0.25 | −0.20 | 0.26 | |
| Model 3c | −0.25 | 0.26 | −0.25 | 0.26 | −0.24 | 0.26 | −0.23 | 0.26 | −0.21 | 0.26 | |
Model 1: controlled for time only
Model 2: controlled for time, individual, and household factors
Model 3: controlled for time, individual, and household characteristics, as well as the community urbanization index
P<0.001
The association between individual-, household-, and community-level factors and the 5th, 15th, 50th, 85th, and 95th BMI percentiles based on longitudinal quantile regression
Table 3 presents the estimated coefficients and standard errors for the quantile regression in Model 3 and the least squared estimates of the mean regression for boys’ and girls’ BMI. Among individual-level factors, energy intake was associated with increased BMI in boys, with an additional 100kcal per day associated with a 0.02 kg/m2 (95% CI: 0.01, 0.03) increase in BMI per year at mean level. Among household-level factors, higher parents’ BMI levels and per capita income levels were associated with higher BMI in boys. At the 95th BMI percentile, an additional 1 unit increase of the father’s or mother’s BMI was associated with a 0.28 kg/m2 (95% CI: 0.23, 0.32) or a 0.22 kg/m2 (95% CI: 0.28, 0.26) in boys’ BMI. Although similar findings were observed at all BMI percentiles, the associations became progressively weaker toward the lower BMI percentiles. The upper quantiles show a positive effect larger than the least squared estimates, i.e., the mean estimates. At the 95th BMI percentile, every 1000 RMB increase of per capita income was associated with a 0.03 kg/m2 (95% CI: 0.01, 0.05) increase. Although similar findings were observed at BMI percentiles higher than the 50th, per capita income was not associated with changes in BMI at lower percentiles.
Table 3.
Quantile regression and mean regression Model 3 results for 5th, 15th, 50th, 85th and 95th percentiles
| Variable | Units | 5th | 15th | 50th | 85th | 95th | Mean Regression | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||||
| Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | Coefficient | SE | ||
| Boys | |||||||||||||
| Intercept | (none) | −0.01 | 3.51 | −0.004 | 3.51 | −0.004 | 3.51 | −0.006 | 3.51 | −0.003 | 3.51 | −0.004 | 3.49 |
| Year | Years | 0.24 | 0.23 | 0.25 | 0.23 | 0.25 | 0.23 | 0.25 | 0.23 | 0.30 | 0.23 | 0.26 | 0.21 |
| Age | Year | −0.02 | 0.21 | −0.01 | 0.21 | −0.01 | 0.21 | −0.02 | 0.21 | −0.01 | 0.21 | −0.01 | 0.15 |
| Age*Age | Year2 | 0.01 | 0.005 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.006 | 0.01 | 0.006 | 0.01 | 0.006 |
| Energy intake | 100 kcal/day | 0.02* | 0.01 | 0.02* | 0.01 | 0.02* | 0.01 | 0.02* | 0.01 | 0.03* | 0.01 | 0.02*** | 0.01 |
| Physical activity | Mets/d | −0.02 | 0.05 | −0.03 | 0.05 | −0.03 | 0.05 | −0.03 | 0.05 | −0.03 | 0.05 | −0.03 | 0.05 |
| Sedentary | Hrs/d | 0.11 | 0.06 | 0.12 | 0.07 | 0.12 | 0.07 | 0.13 | 0.07 | 0.12 | 0.07 | 0.12 | 0.07 |
| Father BMI | Kg/m2 | 0.18*** | 0.02 | 0.19*** | 0.02 | 0.21*** | 0.02 | 0.26*** | 0.02 | 0.27*** | 0.02 | 0.22*** | 0.02 |
| Mother BMI | Kg/m2 | 0.14*** | 0.02 | 0.15*** | 0.02 | 0.17*** | 0.02 | 0.19*** | 0.02 | 0.21*** | 0.02 | 0.17*** | 0.02 |
| Father education | Years | 0.03 | 0.02 | 0.03 | 0.02 | 0.03 | 0.02 | 0.04* | 0.02 | 0.04 | 0.02 | 0.03 | 0.02 |
| Mother education | Years | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 0.03 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 |
| HH per capital income | 1000 Yuan/year | 0.01 | 0.01 | 0.01 | 0.01 | 0.02** | 0.01 | 0.02* | 0.01 | 0.03** | 0.01 | 0.02*** | 0.01 |
| Urbanicity index | None | −0.002 | 0.004 | 0.001 | 0.003 | 0.004 | 0.003 | 0.01 | 0.004 | 0.01 | 0.01 | 0.004 | 0.003 |
| Age in 2011 | Years | 0.24 | 0.23 | 0.25 | 0.21 | 0.25 | 0.21 | 0.22 | 0.23 | 0.23 | 0.21 | 0.24 | 0.21 |
| Girls | |||||||||||||
| Intercept | (none) | 10.65* | 4.12 | 10.65* | 4.12 | 10.65* | 4.12 | 10.65* | 4.12 | 10.65* | 4.16 | 10.65* | 3.67 |
| Year | Years | −0.26 | 0.24 | −0.25 | 0.26 | −0.25 | 0.24 | −0.24 | 0.24 | −0.22 | 0.25 | −0.25 | 0.22 |
| Age | Year | 0.17 | 0.14 | 0.17 | 0.14 | 0.17 | 0.14 | 0.18 | 0.14 | 0.19 | 0.14 | 0.18 | 0.16 |
| Age*Age | Year2 | 0.02** | 0.01 | 0.02** | 0.01 | 0.02** | 0.01 | 0.02** | 0.01 | 0.02*** | 0.01 | 0.02*** | 0.01 |
| Energy intake | Kcal/day | 0.007 | 0.008 | 0.01 | 0.01 | 0.02 | 0.01 | 0.03* | 0.01 | 0.03* | 0.01 | 0.02* | 0.01 |
| Physical activity | Mets/d | −0.12* | 0.06 | −0.12 | 0.06 | −0.12* | 0.06 | −0.12* | 0.06 | −0.12* | 0.06 | −0.13* | 0.06 |
| Sedentary | Hrs/d | −0.003 | 0.06 | −0.003 | 0.06 | −0.002 | 0.06 | <0.01 | 0.06 | <0.01 | 0.06 | <0.01 | 0.06 |
| Menarche age | Dummy | 1.12*** | 0.16 | 1.12*** | 0.16 | 1.12*** | 0.16 | 1.13*** | 0.17 | 1.13*** | 0.16 | 1.13*** | 0.15 |
| Father BMI | Kg/m2 | 0.15*** | 0.02 | 0.15*** | 0.02 | 0.17*** | 0.02 | 0.19*** | 0.02 | 0.21*** | 0.02 | 0.17*** | 0.02 |
| Mother BMI | Kg/m2 | 0.12*** | 0.02 | 0.13*** | 0.02 | 0.14*** | 0.02 | 0.17*** | 0.02 | 0.18*** | 0.02 | 0.14*** | 0.02 |
| Father education | Years | <0.01 | 0.02 | <0.01 | 0.02 | 0.01 | 0.02 | 0.01 | 0.02 | 0.01 | 0.02 | 0.01 | 0.02 |
| Mother education | Years | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 0.02 | 0.03 | 0.02 | 0.03 | 0.02 | 0.02 | 0.02 |
| HH per capital income | 1000 Yuan/year | <0.01 | 0.008 | <0.01 | 0.008 | <0.01 | 0.008 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 |
| Urbanicity index | None | −0.01* | 0.004 | <0.01 | 0.003 | <0.01 | 0.004 | <0.01 | 0.004 | 0.01 | 0.01 | <0.01 | 0.003 |
| Age in 2011 | Years | −0.27 | 0.24 | −0.25 | 0.24 | −0.26 | 0.24 | −0.26 | 0.24 | −0.26 | 0.24 | −0.26 | 0.22 |
P<0.001,
P<0.01,
p<0.05
Among girls, individual-level factors including age, energy intake, and early menarche were associated with girls’ BMI changes. An additional 100 kcal per day was associated with a 0.03 kg/m2 (95% CI: 0.01, 0.05) increase above the 85th percentiles of BMI distribution. Energy intake was not significantly associated with changes in BMI at percentiles lower than the 85th percentile. Earlier age at menarche was associated with higher BMI. Physical activity was associated with decreased BMI in girls. An additional 1 MET hour per day was associated with a 0.12 kg/m2 (95% CI: −0.24, −0.006) BMI decrease; similar findings were observed at all BMI percentiles. Among household-level factors, higher parents’ BMI levels were associated with higher BMI in girls. At the 95th BMI percentile, every one-unit increase of the father’s or mother’s BMI was associated with a 0.21 kg/m2 (95% CI: 0.16, 0.27) or a 0.18 kg/m2 (95% CI: 0.13, 0.24) BMI increase in girls.
Discussion
CHNS longitudinal data shows that Chinese children’s BMI has increased between 1997 and 2006 based on BMI distribution shifts, with the increases being greater at the higher percentiles for all gender and age groups. The prevalence of overweight and obesity has also increased. In line with the result of the national students’ constitution and health survey in China that was conducted between 1985 and 2010, our results not only demonstrate a BMI increase in Chinese children and adolescents, but also indicate that the increase occurred mainly at the upper BMI percentiles. (5) This indicates that the BMI changes in China may be similar to those in other countries. (18–20) In contrast with the BMI distribution shifts in China, the distribution of BMI among US children and adolescents showed more changes in terms of the shape of the BMI distributions, becoming more skewed to the left. The negative effects of these secular changes for Chinese children and adolescents may be reflected in years to come in major health problems, such as shifts in the prevalence of nutrition-related non-communicable diseases (NR-NCDs) and increased medical care costs. (21–23)
Different definitions of overweight and obesity in children and adolescents have been used in China and other countries, which add complexities to making comparisons across studies.(24–26) However, the shifts of childhood BMI distribution in our study suggest that the prevalence of childhood overweight and obesity has been increasing over time no matter which classification is used for the analysis. Although the combined prevalence of childhood overweight and obesity in China was lower than that in developed countries such as the US (18, 27), the rates of increase were greater in China. According to the WGOC Chinese classifications, from 1997 to 2011, the prevalence of overweight and obesity increased 9.2 and 5.6 percentage points, respectively, and the average annual increase rates were 0.66 and 0.40 percent in boys and girls, respectively. Our estimates of the prevalence of overweight and obesity are lower than those based on the Chinese National Survey on Students Constitution and Health (CNSSCH). Geographic variation may be the main reason, because the CHNS covered only 9 provinces, while the CNSSCH surveyed 26 mainland provincial capital cities and 4 municipalities. In China, in general the prevalence of overweight and obesity is higher in urban areas than in rural areas. Due to China’s large population and unequal regional development, it is intuitive that studies will observe differences at different aggregate levels.
Compared with traditional linear regression analysis, the quantile regression method applied in this study provides more useful information. In this study we found a significant time effect on BMI, with a greater increase over time at the upper percentiles. The time variable included in the model captures the effects of time-varying variables such as policy, environment, and other structural changes that are either unobservable or hard to disentangle. Children with high BMI have proven themselves to be quite vulnerable to these changes that are occurring with China’s rapid economic growth and social changes. Policies and interventions should thus target these groups of children to improve their health and ensure more cost-effective long-term outcomes.
Previously studies indicated that both genetic traits and household environments shared by parents and children influence the intergenerational transmission of health capital (28). Our study showed a positive association between parental and child BMI. The associations became progressively weaker toward the lower BMI percentiles. The association with the father’s BMI was stronger than with mother’s; the association was stronger for boys than for girls. We do not foresee that genetic differences will be found to account for such differential effects. Instead, behaviors, and the interactions between behaviors and environments, may play more influential roles, i.e., parents and children with different BMIs may have responded differently to rapid environmental changes. For example, children with high BMI are usually from high SES families in China. Their parents are more likely to be exposed to obesogenic environments such as more opportunities to eat out in restaurants, more access to animal sources of food, and access to other high-energy-design foods. The shared environment of the high SES and high BMI families, which is more self-selected, could have led to a greater resemblance between parents’ and children’s BMI. This finding is in line with findings based on the US national survey data for US children and parents’ BMI (29). Due to traditional norms in China, boys are more likely share “good food” (i.e., food that is high in energy and protein context) with their parents than are girls. Another important factor is that girls are under stronger pressure from people around them to be thinner than boys, especially in urban areas. Our findings indicate that changing parenting practices and parents’ food behaviors, especially for wealthy families, could be an option to help reduce childhood obesity.
A positive energy balance underlies the positive shift of BMI distribution. (30, 31) More sedentary hours, (32–34) less physical activity (35) or increasing energy intake could contribute to a positive energy balance. Although the average energy intake in these samples decreased 160 kcal – 200 kcal per day, longer sedentary hours and less physical activity still made for a positive energy balance. An additional 100 kcal per day was associated with a 0.02–0.03 kg/m2 increase in BMI in boys and girls. The effect was about the same across the BMI distribution. This finding suggests that promoting PA could be effective for all children. This study has some limitations. First, using questionnaires can influence the results, For example, PA and sedentary hours were collected using questionnaires, it may lead to biased answer when compared to more objective measures. Second, the sample size in 2009 and 2011 were small, this may affect the stable of the BMI curves.
In conclusion, the CHNS longitudinal survey suggests right-shifting trends in BMI distributions between 1997 and 2006 in China, with greater increases at higher percentiles, for all gender and age groups. BMI distributions remained stable between 2006 and 2011. The prevalence of childhood overweight and obesity has been increasing in the past 15 years. Children with high BMI, their parents and their schools, which play important roles in children’s lives, should be target groups for interventions to curb childhood obesity in China.
Acknowledgments
The research was supported in part by a research grant from the US National Institutes of Health (NIH, Grant No.1U54hd070725), the Eunice Kennedy Shriver National Institute of Child Health & Human Development, and Office of Behavioral and Social Sciences Research. It is part of the collaboration project between the National Institute of Nutrition and Food Safety at the Chinese Center for Disease Control and Prevention and the University at Buffalo, State University of New York. The content of the paper is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
This research uses data from the China Health and Nutrition Survey (CHNS). We thank the National Institute for Nutrition and Food Safety at the Chinese Center for Disease Control and Prevention, the Carolina Population Center at the University of North Carolina at Chapel Hill, and the US NIH (R01-HD30880, DK056350, R24 HD050924, and R01-HD38700) for financial support for the CHNS data collection and management.
Footnotes
Conflict of Interest: The authors have no conflict of interest.
Financial disclosure: No financial disclosures were reported by the authors of this paper.
Author Contributions: Huijun Wang and Bing Zhang contributed to the initial design of the analysis. Huijun Wang and Ji Zhang contributed to the analysis. All authors contributed to the interpretation of data analysis results. Huijun Wang wrote the first draft of the manuscript. Hong Xue, Shufa Du and Youfa Wang revised the manuscript. Youfa Wang led the effort receiving the NIH grant (1U54hd070725) that funded the international collaboration project and has provided some administrative support for developing the manuscript.
References
- 1.Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70(1):3–21. doi: 10.1111/j.1753-4887.2011.00456.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wang Y, Mi J, Shan XY, Wang QJ, Ge KY. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int J Obes (Lond) 2007;31(1):177–88. doi: 10.1038/sj.ijo.0803354. [DOI] [PubMed] [Google Scholar]
- 3.Singh AS, Mulder C, Twisk JW, van Mechelen W, Chinapaw MJ. Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Rev. 2008;9(5):474–88. doi: 10.1111/j.1467-789X.2008.00475.x. [DOI] [PubMed] [Google Scholar]
- 4.Li Y, Yang X, Zhai F, Piao J, Zhao W, Zhang J, et al. Childhood obesity and its health consequence in China. Obes Rev. 2008;9(Suppl 1):82–6. doi: 10.1111/j.1467-789X.2007.00444.x. [DOI] [PubMed] [Google Scholar]
- 5.Ji CY, Chen TJ, Sun X. Secular changes on the distribution of body mass index among Chinese children and adolescents, 1985–2010. Biomed Environ Sci. 2013;26(7):520–30. doi: 10.3967/0895-3988.2013.07.002. [DOI] [PubMed] [Google Scholar]
- 6.Wang H, Du S, Zhai F, Popkin BM. Trends in the distribution of body mass index among Chinese adults, aged 20–45 years (1989–2000) Int J Obes (Lond) 2007;31(2):272–8. doi: 10.1038/sj.ijo.0803416. [DOI] [PubMed] [Google Scholar]
- 7.Yin G, Cai J. Quantile regression models with multivariate failure time data. Biometrics. 2005;61(1):151–61. doi: 10.1111/j.0006-341X.2005.030815.x. [DOI] [PubMed] [Google Scholar]
- 8.Geraci M, Bottai M. Quantile regression for longitudinal data using the asymmetric Laplace distribution. Biostatistics. 2007;8(1):140–54. doi: 10.1093/biostatistics/kxj039. [DOI] [PubMed] [Google Scholar]
- 9.Popkin BM, Du S, Zhai F, Zhang B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989–2011. Int J Epidemiol. 2010;39(6):1435–40. doi: 10.1093/ije/dyp322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhang B, Wang HJ, Du WW. [Progress of cohort study and its inspiration to China Health and Nutrition Survey] Zhonghua Yu Fang Yi Xue Za Zhi. 2011;45(4):295–8. [PubMed] [Google Scholar]
- 11.Du S, Mroz TA, Zhai F, Popkin BM. Rapid income growth adversely affects diet quality in China--particularly for the poor! Soc Sci Med. 2004;59(7):1505–15. doi: 10.1016/j.socscimed.2004.01.021. [DOI] [PubMed] [Google Scholar]
- 12.Popkin BM. The nutrition transition: an overview of world patterns of change. Nutr Rev. 2004;62(7 Pt 2):S140–3. doi: 10.1111/j.1753-4887.2004.tb00084.x. [DOI] [PubMed] [Google Scholar]
- 13.Cui Z, Dibley MJ. Trends in dietary energy, fat, carbohydrate and protein intake in Chinese children and adolescents from 1991 to 2009. Br J Nutr. 2012;108(7):1292–9. doi: 10.1017/S0007114511006891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Monda KL, Gordon-Larsen P, Stevens J, Popkin BM. China's transition: the effect of rapid urbanization on adult occupational physical activity. Soc Sci Med. 2007;64(4):858–70. doi: 10.1016/j.socscimed.2006.10.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. 1992;11(10):1305–19. doi: 10.1002/sim.4780111005. [DOI] [PubMed] [Google Scholar]
- 16.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320(7244):1240–3. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Geraci M, Bottai M. Quantile regression for longitudinal data using the asymmetric Laplace distribution. Biostatistics. 2007;8(1):140–54. doi: 10.1093/biostatistics/kxj039. [DOI] [PubMed] [Google Scholar]
- 18.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA. 2012;307(5):483–90. doi: 10.1001/jama.2012.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kromeyer-Hauschild K, Zellner K. Trends in overweight and obesity and changes in the distribution of body mass index in schoolchildren of Jena, East Germany. Eur J Clin Nutr. 2007;61(3):404–11. doi: 10.1038/sj.ejcn.1602533. [DOI] [PubMed] [Google Scholar]
- 20.Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1(1):11–25. doi: 10.1080/17477160600586747. [DOI] [PubMed] [Google Scholar]
- 21.Wang Y, Lim H, Wu Y. Growing global burden of chronic noncommunicable diseases and an alarming situation in China. Beijing Da Xue Xue Bao. 2012;44(5):688–93. [PubMed] [Google Scholar]
- 22.Cao ZQ, Zhu L, Zhang T, Wu L, Wang Y. Blood pressure and obesity among adolescents: a school-based population study in China. Am J Hypertens. 2012;25(5):576–82. doi: 10.1038/ajh.2012.5. [DOI] [PubMed] [Google Scholar]
- 23.Lu X, Shi P, Luo CY, Zhou YF, Yu HT, Guo CY, et al. Prevalence of hypertension in overweight and obese children from a large school-based population in Shanghai, China. BMC Public Health. 2013;13:24. doi: 10.1186/1471-2458-13-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chen S, Binns CW, Zhang Y. The importance of definition in diagnosing obesity: a review of studies of children in China. Asia Pac J Public Health. 2012;24(2):248–62. doi: 10.1177/1010539512441617. [DOI] [PubMed] [Google Scholar]
- 25.Li YP, Hu XQ, Jing Z, Yang XG, Ma GS. Application of the WHO growth reference (2007) to assess the nutritional status of children in China. Biomed Environ Sci. 2009;22(2):130–5. doi: 10.1016/S0895-3988(09)60035-0. [DOI] [PubMed] [Google Scholar]
- 26.Xu YQ, Ji CY. Report on childhood obesity in China (7). Comparison of NCHS and WGOC. Biomed Environ Sci. 2008;21(4):271–9. doi: 10.1016/S0895-3988(08)60041-0. [DOI] [PubMed] [Google Scholar]
- 27.Ogden CL, Carroll MD, Flegal KM. High body mass index for age among US children and adolescents, 2003–2006. JAMA. 2008;299(20):2401–5. doi: 10.1001/jama.299.20.2401. [DOI] [PubMed] [Google Scholar]
- 28.Classen TJ. Measures of the intergenerational transmission of body mass index between mothers and their children in the United States, 1981–2004. Econ Hum Biol. 2010;8(1):30–43. doi: 10.1016/j.ehb.2009.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Zhang QLR, Chen HJ, Xue H, Wang Y. Does child-parent resemblance in body weight status vary by socio-demographic factors in the United States? Journal of Epidemiology and Community Health. 2014 doi: 10.1136/jech-2013-203476. [DOI] [PubMed] [Google Scholar]
- 30.te Velde SJ, van Nassau F, Uijtdewilligen L, van Stralen MM, Cardon G, De Craemer M, et al. Energy balance-related behaviours associated with overweight and obesity in preschool children: a systematic review of prospective studies. Obes Rev. 2012;13(Suppl 1):56–74. doi: 10.1111/j.1467-789X.2011.00960.x. [DOI] [PubMed] [Google Scholar]
- 31.Hodgkin E, Hamlin MJ, Ross JJ, Peters F. Obesity, energy intake and physical activity in rural and urban New Zealand children. Rural Remote Health. 2010;10(2):1336. [PubMed] [Google Scholar]
- 32.Mitchell JA, Rodriguez D, Schmitz KH, Audrain-McGovern J. Greater screen time is associated with adolescent obesity: a longitudinal study of the BMI distribution from Ages 14 to 18. Obesity (Silver Spring) 2013;21(3):572–5. doi: 10.1002/oby.20157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Yang TC, Matthews SA, Chen VY. Stochastic Variability in Stress, Sleep Duration, and Sleep Quality Across the Distribution of Body Mass Index: Insights from Quantile Regression. Int J Behav Med. 2013 doi: 10.1007/s12529-013-9293-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Chen CM, Chang CK, Yeh CY. A quantile regression approach to re-investigate the relationship between sleep duration and body mass index in Taiwan. Int J Public Health. 2012;57(3):485–93. doi: 10.1007/s00038-011-0239-7. [DOI] [PubMed] [Google Scholar]
- 35.Li YP, Hu XQ, Schouten EG, Liu AL, Du SM, Li LZ, et al. Report on childhood obesity in China (8): effects and sustainability of physical activity intervention on body composition of Chinese youth. Biomed Environ Sci. 2010;23(3):180–7. doi: 10.1016/S0895-3988(10)60050-5. [DOI] [PubMed] [Google Scholar]