

Abstract
Globozoospermia, characterized by round-headed acrosomeless sperm, is a rare and severe form of teratozoospermia. We report a successful pregnancy in two cases of total globozoospermia after intracytoplasmic sperm injection (ICSI) with oocyte activation with calcium ionophore. In thefirst case, globozoospermia was diagnosed on the day of oocyte retrieval. Among 11 retrieved oocytes, only one fertilized after ICSI. The pregnancy test 2 weeks after embryo transfer was negative. Two months later, the patient underwent ovarian stimulation again. The 12 retrieved oocytes were exposed to calcium ionophore medium following ICSI. Four oocytes were fertilized and two blastocysts were transferred resulting in a clinical pregnancy. In the second case, among seven retrieved oocytes, three fertilized after ICSI and assisted oocyte activation, and two 8-cell embryos were transferred, resulting in a positive pregnancy. The successful outcome here justifies the use of ICSI with oocyte activation to improve the pregnancy rate significantly when dealing with globozoospermia.
KEYWORDS: Acrosome, assisted oocyte activation, failed fertilization, globozoospermia, intracytoplasmic sperm injection, male infertility
INTRODUCTION
One in every six couples worldwide is affected by infertility, nearly 30% of which are attributed to male infertility. A rare and severe form of male infertility is caused by globozoospermia (a form of teratozoospermia) with an incidence of <0.1% in infertile men.[1] The round-headed acrosomeless spermatozoa cannot bind to and penetrate the zona pellucida of an oocyte, thereby causing complete fertilization failure.
Due to this failure of fertilization, globozoospermia was previously considered as a sterilizing pathology. With the advent of intracytoplasmic sperm injection (ICSI), few successful pregnancies have been reported.[2] However, the fertilization rates were poor due to inability of the round-headed spermatozoa to activate an oocyte to complete second meiotic division because of premature chromatin condensation.[3] The use of oocyte activation medium reportedly improves fertilization rates.[4] In this report, we present two successful cases of pregnancies in couples with globozoospermia using ICSI with calcium ionophore medium.
CASE REPORTS
Case 1
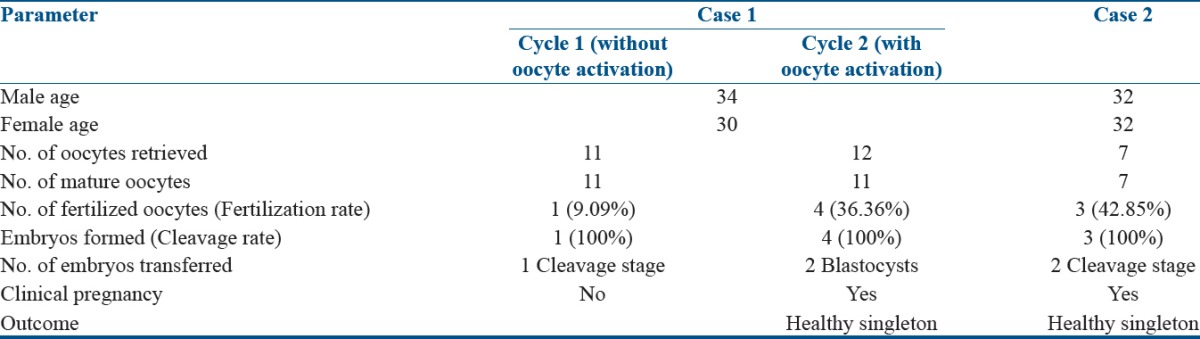
The couple was referred with primary unexplained infertility of 8-year duration. The 30-year-oldfemale had regular ovulatory cycles, normal hormonal profile, and normal uterus with bilateral patent fallopian tubes on hysterosalpingography. Her husband, aged 34 years, had no significant history and had several semen analysis reports from another laboratory showing a sperm count of 60–80 million/ml, with 50%–60% progressive motility, and >30% normal morphology. The couple had undergone five intrauterine insemination cycles. Since the last semen analysis report was very recent, the couple declined a repeat test at our center. The couple was advised in vitro fertilization treatment (IVF). Controlled ovarian stimulation was started using 225 units of recombinant follicle stimulating hormone (rFSH) (Folisurge, Intas Pharmaceuticals, India) along with an antagonist protocol using 0.25 mg cetrorelix (Cetrolix, Intas Pharmaceuticals, India). Final oocyte maturation was provided by 250 IU of recombinant human chorionic gonadotropin (Ovitrelle®, Merck Serono, Switzerland). Thirty-five h later, 11 oocytes were retrieved by transvaginal ultrasound-guided follicle aspiration. However, an analysis of the semen sample produced on oocyte retrieval day under high magnification using an inverted microscope revealed total globozoospermia, later confirmed by morphology staining. The couple was informed of the diagnosis, and informed consent was obtained for ICSI. ICSI was performed after sperm immobilization in 7% polyvinylpyrrolidone (PVP, SAGE Media™, Trumbull, CT, USA) using Olympus IX73 Inverted Research Microscope (Olympus Corporation, Shibuya-ku, Tokyo, Japan) equipped with Narishige ON-3 Microinjector (Narishige CO. LTD, Setagaya-ku, Tokyo, Japan), leading to only one fertilized oocyte. The resulting embryo was transferred on day 2 at 4-cell stage. However, the pregnancy test 2 weeks later was negative. Two months later, the same patient underwent another stimulation cycle with the same protocol. Following ICSI, the oocytes were placed into oocyte activation media (GM508, Cult-Active, GYNEMED) for 15 min at 37° 5% O2 and 6% CO2. The oocytes were then washed free of calcium ionophore and were cultured overnight in G-IVF PLUS (Vitrolife, Göteborg, Sweden) in the incubator (K-MINC-1000, Cook Medical Inc., Bloomington, USA). Eighteen h postinjection, four oocytes showed signs of fertilization. Two blastocysts were transferred on day 5 resulting in a clinical pregnancy. An elective cesarean section was done at 38 weeks resulting in the birth of a healthy male child weighing 2.9 kg.
The embryological details are summarized in Table 1.
Table 1.
Embryology details of patients
Case 2
The couple was referred with a history of primary infertility of 6 years. A 32-year-oldfemale had regular ovulatory cycles, normal hormonal profile, and normal hysterosalpingography findings. Her husband, aged 32 years, had no significant history and one previous normal semen analysis report. A repeat semen analysis done at our clinic revealed a count of 46 million/ml, with 38% progressive motility and 100% globozoospermia. The woman underwent controlled ovarian stimulation with 225 units of rFSH (Gonal-f®, Merck Serono, Switzerland) using an antagonist protocol with 0.25 mg cetrorelix (Cetrotide®, Merck Serono, Switzerland). Seven mature oocytes were retrieved. Considering the high risk of complete fertilization failure, oocyte activation media was used in the first ICSI cycle. Three oocytes fertilized and two 8-cell Grade I embryos were transferred on day 3, resulting in a positive pregnancy test. A singleton clinical pregnancy was obtained with an uncomplicated clinical course.
DISCUSSION
Although the etiology of globozoospermia remains unknown, some reports mention a familial occurrence and possible genetic origin. However, no responsible genes have been identified. An increased aneuploidy rate has been reported mostly in the acrocentric (13, 14, 15, 18, and 21) and sex chromosomes.[5] Recently, a mutation in SPATA16 gene was also found to be associated with certain types of globozoospermia.[6]
Globozoospermia has been categorized into two types. Type I involves a complete lack of acrosome and acrosomal enzymes leading to total (100%) round-headed spermatozoa, whereas Type II has some acrosomal covering with a conical nucleus, which may be surrounded by large droplets of cytoplasmic material indicating degenerative changes (leading to partial globozoospermia).[7,8] The main morphological defect in globozoospermia is an absence or severe malformation of acrosomal structures. Despite other sperm parameters such as count, density, and motility being normal, globozoospermia is an important etiology of male infertility with very low assisted reproductive technology success rates. Before the advent of ICSI, these men were considered sterile as conventional IVF failed in these patients due to lack of acrosome reaction and failure to penetrate zona pellucida. Although ICSI overcomes this, severe sperm morphological abnormalities result in very low fertilization rates and poor embryo quality.[3,9] We also observed a very low fertilization rate.
The main cause of fertilization failure following conventional ICSI is failure of oocyte activation. Oocyte activation is a series of events that converts a metaphase-II-arrested oocyte into a fertilized egg. In mammalian oocytes, an intracellular rise in calcium that starts shortly following spermatozoon–oocyte fusion is responsible for the resumption of meiosis and beginning of embryo development.[10] The spermatozoa of some men suffering from fertilization failure (e.g., globozoospermic men) are either totally unable to trigger robust calcium oscillations upon injection into oocytes or induce calcium oscillations of reduced frequency and amplitude compared with those from fertile men.
Calcium ionophores help to activate the oocyte by increasing the calcium permeability of the cell membrane, thereby allowing extracellular calcium to flow into the cell, thereby mimicking physiological cell signaling mechanisms that result in oocyte activation.[10] In 1997, improved fertilization with assisted oocyte activation was first reported by applying calcium ionophore in such cases.[4] Quality embryos were obtained in the oocyte activation group while no fertilized oocytes, oocyte cleavage, or quality embryos were found in the conventional treatment group. Some studies have shown that mechanical oocyte activation yielded a better fertilization rate.[7]
Our report concludes that a careful semen examination by appropriately trained personnel would save such couples from unnecessary investigations and treatment as seen in these cases. In both our cases, globozoospermia was missed by the previous laboratories where semen analysis was done. Thus, due to lack of proper morphology assessment, male factor infertility was not diagnosed. Although ICSI is the ideal treatment modality for globozoospermia, fertilization rates remain low. Oocyte activation following ICSI results in better fertilization rates. The present report suggests that oocyte activation (with calcium ionophore) could improve the pregnancy rate significantly in cases with globozoospermia.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ghasemzadeh J, Talebi AR, Khalili MA, Fesahat F, Halvaei I, Nabi A, et al. Sperm parameters, protamine deficiency, and apoptosis in total globozoospermia. Iran J Reprod Med. 2015;13:495–502. [PMC free article] [PubMed] [Google Scholar]
- 2.Kilani Z, Ismail R, Ghunaim S, Mohamed H, Hughes D, Brewis I, et al. Evaluation and treatment of familial globozoospermia in five brothers. Fertil Steril. 2004;82:1436–9. doi: 10.1016/j.fertnstert.2004.03.064. [DOI] [PubMed] [Google Scholar]
- 3.Battaglia DE, Koehler JK, Klein NA, Tucker MJ. Failure of oocyte activation after intracytoplasmic sperm injection using round-headed sperm. Fertil Steril. 1997;68:118–22. doi: 10.1016/s0015-0282(97)81486-0. [DOI] [PubMed] [Google Scholar]
- 4.Rybouchkin AV, Van der Straeten F, Quatacker J, De Sutter P, Dhont M. Fertilization and pregnancy after assisted oocyte activation and intracytoplasmic sperm injection in a case of round-headed sperm associated with deficient oocyte activation capacity. Fertil Steril. 1997;68:1144–7. doi: 10.1016/s0015-0282(97)00378-6. [DOI] [PubMed] [Google Scholar]
- 5.Machev N, Gosset P, Viville S. Chromosome abnormalities in sperm from infertile men with normal somatic karyotypes: Teratozoospermia. Cytogenet Genome Res. 2005;111:352–7. doi: 10.1159/000086910. [DOI] [PubMed] [Google Scholar]
- 6.ElInati E, Fossard C, Okutman O, Ghédir H, Ibala-Romdhane S, Ray PF, et al. A new mutation identified in SPATA16 in two globozoospermic patients. J Assist Reprod Genet. 2016;33:815–20. doi: 10.1007/s10815-016-0715-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dirican EK, Isik A, Vicdan K, Sozen E, Suludere Z. Clinical pregnancies and livebirths achieved by intracytoplasmic injection of round headed acrosomeless spermatozoa with and without oocyte activation in familial globozoospermia: Case report. Asian J Androl. 2008;10:332–6. doi: 10.1111/j.1745-7262.2008.00248.x. [DOI] [PubMed] [Google Scholar]
- 8.Dam AH, Ramos L, Dijkman HB, Woestenenk R, Robben H, van den Hoven L, et al. Morphology of partial globozoospermia. J Androl. 2011;32:199–206. doi: 10.2164/jandrol.109.009530. [DOI] [PubMed] [Google Scholar]
- 9.Kahraman S, Akarsu C, Cengiz G, Dirican K, Sözen E, Can B, et al. Fertility of ejaculated and testicular megalohead spermatozoa with intracytoplasmic sperm injection. Hum Reprod. 1999;14:726–30. doi: 10.1093/humrep/14.3.726. [DOI] [PubMed] [Google Scholar]
- 10.Vanden Meerschaut F, Nikiforaki D, Heindryckx B, De Sutter P. Assisted oocyte activation following ICSI fertilization failure. Reprod Biomed Online. 2014;28:560–71. doi: 10.1016/j.rbmo.2014.01.008. [DOI] [PubMed] [Google Scholar]