

Abstract
Objectives:
To evaluate the use of hysteroscopy in the assessment of uterine pathologies in infertile women with repeated implantation failure (RIF) after in vitro fertilization (IVF) and determine whether removal of such pathologies increased pregnancy rates in women with RIF.
Methods:
This prospective study was conducted at King Fahd Hospital of the University, Al-Khobar, Kingdom of Saudi Arabia, between January 2010 and December 2015. The inclusion criteria were women who underwent IVF treatment cycles and ended in more than 2 RIF, and women who underwent hysterosalpingography (HSG). Hysteroscopies were performed, findings were recorded, and the clinical pregnancy rates were compared and assessed in patients with and without uterine cavity abnormality. All hysteroscopic procedures were performed by a single consultant.
Results:
Hysteroscopies were performed on 266 women who had at least 2 RIF. The average duration of infertility was 7.2±3.1 years. In 162 patients (60.9%), a hysteroscopy did not find any abnormality of the uterine cavity. In 104 patients (39.1%) there were one or more abnormal hysteroscopic findings. Hysterosalpingography was able to detect only 54 abnormalities (51.9%). The pregnancy rate was significantly higher in patients who were treated by a hysteroscopy for a detected uterine abnormality (39.4%).
Conclusion:
A hysteroscopy was able to detect intrauterine pathologies which were missed by other investigative modalities. We believe patients with a history of RIF should undergo hysteroscopic examination before any further cycles are considered.
Recurrent implantation failure is defined as a failure to achieve a clinical pregnancy after transfer of 4 or more good-quality embryos in a minimum of 2 in vitro fertilization (IVF) cycles in a woman under the age of 40.1 The failure of implantation may be a consequence of embryo or uterine factors. Repeated implantation failure (RIF) in IVF failures have long baffled many experts in the field of IVF and have been attributed not only to the embryos but also to decrease in endometrial receptivity. Specific issues with the uterine cavity were suggested to be due to inadequacy of the endometrial thickness, adhesions, and anatomical abnormalities. Uterine pathologies, like endometrial hyperplasia, polyps, and leiomyomata have been shown in 18% to 50% of women with repeated IVF failure.2-4 To diagnose the status of a uterine cavity, noninvasive techniques are available that offer reasonable accuracy. Vaginal ultrasonography, sonohysterography, and hysterosalpingography (HSG) are regular tools in the investigation of patients with RIF. If all of the above tests return normal results, patients end up in RIF, which frustrates both the patient and the IVF consultants as some pathologies are missed in routine radiological assessments.5,6 In the recent past, hysteroscopy was added to the armamentarium in the investigation of RIF as many physicians began focusing on the uterine cavity and correcting any intrauterine pathologies that may have been missed. It is reported that the accuracy of a hysteroscopy is superior to the other modalities in use for diagnosis of intrauterine pathologies.7-9 The objective of this study was to evaluate hysteroscopy in the assessment of uterine pathologies in infertile women with RIF after IVF, and explore whether removal of such pathologies increased rate of pregnancy in women with RIF.
Methods
This prospective study was conducted between January 2010 and December 2015 using patients at King Fahd Hospital of the University, Al-Khobar, Kingdom of Saudi Arabia. Patients with at least 2 previous IVF embryo transfer failures were eligible for participation in this study. After approval of the institution’s ethical committee, informed consent was received from all participants, and the study began. The study was carried out according to principles of the Declaration of Helsinki. The inclusion criteria were women who underwent IVF treatment cycles and ended in more than 2 RIF and women who underwent HSG. The exclusion criteria were patients with no history of RIF, women who have a male factor as a cause of infertility, and those who have had no previous HSG. A transvaginal ultrasonography was performed before the patients were scheduled for a hysteroscopy. A hysteroscopy was performed after 2 months of HSG using a hysteroscope (Karl Storz SE & Company, Tuttlingen, Germany), which has a 30-degree view with 2.9 mm Bettocchi continuous-flow sheath. The uterine distention was performed using normal saline with an electronic pump (Hysteromat; Karl Storz). Surgical video assisted the hysteroscopy and was performed using a bipolar electric resectoscope (Karl Storz) and intrauterine bigatti shaver. Endometrial pathology was removed and, before the scope was removed, the endometrium was scratched at 4 sites: the fundus, lateral, anterior, and posterior walls of the uterus. On day 2 of the cycle, antagonist stimulation protocol was used. During follow-up, transvaginal ultrasonography was performed to assess the size of the follicles. As soon as 3 follicles reached a size of at least 17 mm, oocytes were retrieved. On average, 2 embryos were transferred to the uterine cavity. Patients who had no uterine pathology were in Group I, and those who underwent hysteroscopic surgery were in Group II. Patients were followed in the clinic, and data were recorded and entered into the database and analyzed using the Statistical Package for the Social Science version 21 (IBM Corp., Armonk, NY, USA). When appropriate, statistical comparisons between groups were performed using a Chi-squared test. A p-value of <0.05 was considered statistically significant.
Results
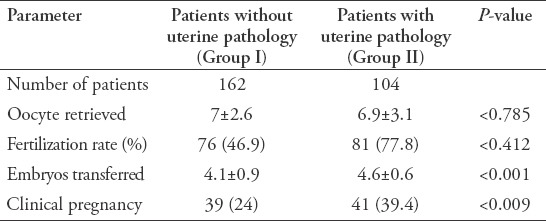
Hysteroscopies were performed on 266 women who had at least 2 RIF. The average age was 32.9 ± 4.2 years with the mean duration of infertility of 7.2 ± 3.1 years. Patients’ demographic data are given in Table 1. In 162 patients (60.9%), a hysteroscopy did not find any abnormality of the uterine cavity. Table 2 gives the abnormal hysteroscopic findings in 104 patients in which the majority were due to endometrial adhesions and scarring. Hysterosalpingography was able to detect only 54 abnormalities (51.9%). Table 3 gives the outcomes of the subsequent IVF cycles in women with a detected and treated uterine abnormality and those who did not have any abnormality. The fertilization rates in both groups were not significant (p<0.4), embryo transfer was higher in Group II (p<0.001), and the clinical pregnancy was statistically significant in Group II (p<0.009). There were 7 (2.63%) complications related to the hysteroscopy: 2 during diagnostic and 5 during operative procedures. They were diagnosed at the time of surgery and dealt accordingly without any further complications.
Table 1.
Demographic data of 266 patients
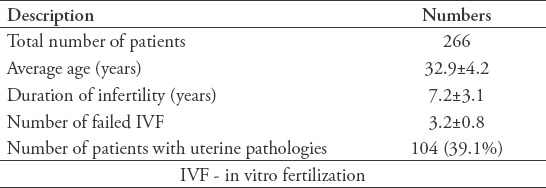
Table 2.
Uterine pathologies as diagnosed on hysteroscopy.
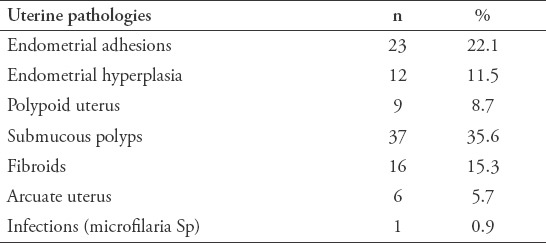
Table 3.
A comparison of assessment of fertilization with and without hysteroscopic surgery.
Discussion
The results of this study indicate that patients with RIF have uterine abnormalities which could not be diagnosed by other available methodologies. Out of 266 patients, 104 (39.1%) had abnormal hysteroscopic findings. Reports in the literature suggest such abnormalities range between 30-60%.10-13 Uterine masses like polyps and fibroids are known to affect the implantation in various ways, including increased uterine contractions, abnormal vascularization, and, especially, chronic inflammation.14-16 In our study we found over 50% of the patients had polyps and fibroids after surgical removal.
Hysteroscopy is a valuable tool in the management of infertility. Apart from direct visualizing of the endometrium by naked eye, pathologies missed by other modalities of investigation can be picked up and managed appropriately. Hysteroscopy has proved its value and has now become a gold-standard technique carried out as an outpatient procedure.17 Unfortunately, the procedure itself is not free from complications. In this study, complications were under 2.5%, and the majority of them occurred during operative procedures. This is within the reported incidence of complications of 1% to 3%.10 It has been reported that hysteroscopic surgery of the missed uterine pathologies in patients with RIF increases the chances of future IVF pregnancies, and there is evidence to support this view.3 Miona et al3 also reported an increase of clinical pregnancy by 20%.
In our study, after the correction of the intrauterine pathologies, there was an increase in pregnancy rates. Patients who had a second look and those who had removal of submucous fibroids and anti-adhesives were used, and they waited for at least 2 cycles before an IVF-embryo transfer cycle was instituted. Pereira et al19 reported that there was no difference of pregnancy rate and delay in the IVF cycle after hysteroscopic surgery. Our study supports the view that there is no difference in pregnancy rates when IVF cycles are instituted immediately or delayed after hysterscopic surgery.
Study limitations and strengths
The limitations are the number of patients and similarities to previous studies conducted elsewhere. The primary strength of this study is that it is a prospective cohort study, which gives results of higher accuracy and without bias. Additionally, all of the patients were operated on by the author, and different levels of expertise of hysteroscopy techniques did not arise.
In conclusion, as per our results and in alignment with current literature, a hysteroscopy can detect intrauterine pathologies that are missed by other investigative modalities. Also, we believe patients with a history of RIF should undergo a hysteroscopic examination before any further cycles are considered.
Acknowledgment
The author acknowledges the help of Dr. Kamylia Al-Obaid in data collection.
Footnotes
References
- 1.Coughlan C, Ledger W, Wang Q, Liu F, Demirol A, Gurgan T, et al. Recurrent implantation failure: definition and management. Reprod Biomed Online. 2014;28:14–38. doi: 10.1016/j.rbmo.2013.08.011. [DOI] [PubMed] [Google Scholar]
- 2.Kogan L, Dior U, Chill HH, Karavani G, Revel A, Shushan A, et al. Operative hysteroscopy for treatment of intrauterine pathologies does not interfere with later endometrial development in patients undergoing in vitro fertilization. Arch Gynecol Obstet. 2016;293:1097–1100. doi: 10.1007/s00404-015-3988-3. [DOI] [PubMed] [Google Scholar]
- 3.Moini A, Kiani K, Ghaffari F, Hosseini F. Hysteroscopic findings in patients with a history of two implantation failures following in vitro fertilization. Int J Fertil Steril. 2012;6:27–30. [PMC free article] [PubMed] [Google Scholar]
- 4.Al-Turki HA, Gullenpet AH, Syed A, Al-Saif HS, Aldhafery BF. Uterine and tubal abnormalities in infertile Saudi Arabian women: A teaching hospital experience. Saudi J Med Med Sci. 2016;4:89–92. doi: 10.4103/1658-631X.178293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vitner D, Filmer S, Goldstein I, Khatib N, Weiner Z. A comparison between ultrasonography and hysteroscopy in the diagnosis of uterine pathology. Eur J Obstet Gynecol Reprod Biol. 2013;171:143–145. doi: 10.1016/j.ejogrb.2013.08.024. [DOI] [PubMed] [Google Scholar]
- 6.Chawla I, Tripathi S, Vohra P, Singh P. To evaluate the accuracy of saline infusion sonohysterography (SIS) for evaluation of uterine cavity abnormalities in patients with abnormal uterine bleeding. J Obstet Gynaecol India. 2014;64:197–201. doi: 10.1007/s13224-013-0501-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khan F, Jamaat S, Al-Jaroudi D. Saline infusion sonohysterography versus hysteroscopy for uterine cavity evaluation. Ann Saudi Med. 2011;31:387–392. doi: 10.4103/0256-4947.83213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zinna M, Gentile M, Torcia F, Bianchi P, Cozza G, Marziani R, et al. Diagnostic accuracy of sonohysterography vs hysteroscopy in benign uterine endocavitary findings. Eur Rev Med Pharmacol Sci. 2015;19:365–371. [PubMed] [Google Scholar]
- 9.Vitner D, Filmer S, Goldstein I, Khatib N, Weiner Z. A comparison between ultrasonography and hysteroscopy in the diagnosis of uterine pathology. Eur J Obstet Gynecol Reprod Biol. 2013;171:143–145. doi: 10.1016/j.ejogrb.2013.08.024. [DOI] [PubMed] [Google Scholar]
- 10.Sahu L, Tempe A, Gupta S. Hysteroscopic evaluation in infertile patients: a prospective study. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2012;1:1–5. [Google Scholar]
- 11.Jain N, Manchanda R, Lekhi A, Chitra S. Role of hysteroscopy in evaluation of infertility: A retrospective study of 100 cases. Journal of Gynecology. 2016;1:000117. [Google Scholar]
- 12.Calles-Sastre L, Engels-Calvo V, Ríos-Vallejo M, Serrano-González L, García-Espantaleón M, Royuela A, et al. Prospective study of concordance between hysterosalpingo-contrast sonography and hysteroscopy for evaluation of the uterine cavity in patients undergoing infertility studies. J Ultrasound Med. 2017:16. doi: 10.1002/jum.14483. doi:10.1002/jum.14483. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 13.Promberger R, Simek IM, Nouri K, Obermaier K, Kurz C, Ott J. Accuracy of tubal patency assessment in diagnostic hysteroscopy compared to laparoscopy in infertile women: A retrospective cohort study. J Minim Invasive Gynecol. 2017:6. doi: 10.1016/j.jmig.2017.11.020. pii: S1553-4650(17)31327-4. [DOI] [PubMed] [Google Scholar]
- 14.Al Chami A, Saridogan E. Endometrial polyps and subfertility. J Obstet Gynaecol India. 2017;67:9–14. doi: 10.1007/s13224-016-0929-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zepiridis LI, Grimbizis GF, Tarlatzis BC. Infertility and uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2016;34:66–73. doi: 10.1016/j.bpobgyn.2015.12.001. [DOI] [PubMed] [Google Scholar]
- 16.Samejima T, Koga K, Nakae H, Wada-Hiraike O, Fujimoto A, Fujii T, et al. Identifying patients who can improve fertility with myomectomy. Eur J Obstet Gynecol Reprod Biol. 2015;185:28–32. doi: 10.1016/j.ejogrb.2014.11.033. [DOI] [PubMed] [Google Scholar]
- 17.Ma T, Readman E, Hicks L, Porter J, Cameron M, Ellett L, et al. Is outpatient hysteroscopy the new gold standard?Results from an 11 year prospective observational study. Aust N Z J Obstet Gynaecol. 2017;57:74–80. doi: 10.1111/ajo.12560. [DOI] [PubMed] [Google Scholar]
- 18.Di Spiezio Sardo A, Di Carlo C, Minozzi S, Spinelli M, Pistotti V, Alviggi C, et al. Efficacy of hysteroscopy in improving reproductive outcomes of infertile couples: a systematic review and meta-analysis. Hum Reprod Update. 2016;22:479–496. doi: 10.1093/humupd/dmw008. [DOI] [PubMed] [Google Scholar]
- 19.Pereira N, Amrane S, Estes JL, Lekovich JP, Elias RT, Chung PH, et al. Does the time interval between hysteroscopic polypectomy and start of in vitro fertilization affect outcomes? Fertil Steril. 2016;105:539–544. doi: 10.1016/j.fertnstert.2015.10.028. [DOI] [PubMed] [Google Scholar]