

Abstract
Background
In response to growing pressures on primary care, leaders have introduced a wide range of workforce and practice innovations, including team redesigns that delegate some physician tasks to nonphysicians. One important question is how such innovations affect care team members, particularly in view of growing dissatisfaction and burnout among healthcare professionals. We examine the work experiences of primary care physicians and staff after implementing Lean-based workflow redesigns. This included co-locating physician and medical assistant dyads, delegating significant responsibilities to nonphysician staff, and mandating greater coordination and communication among all care team members.
Methods
The redesigns were implemented and scaled in three phases across 46 primary care departments in a large ambulatory care delivery system. We fielded 1164 baseline and 1333 follow-up surveys to physicians and other nonphysician staff (average 73% response rate) to assess workforce engagement (e.g., job satisfaction, motivation), perceptions of the work environment, and job-related burnout. We conducted multivariate regressions to detect changes in experiences after the redesign, adjusting for respondent characteristics and clustering of within-clinic responses.
Results
We found that both physicians and nonphysician staff reported higher levels of engagement and teamwork after implementing redesigns. However, they also experienced higher levels of burnout and perceptions of the workplace as stressful. Trends were the same for both occupational groups, but the increased reports of stress were greater among physicians. Additionally, members of all clinics, except for the pilot site that developed the new workflows, reported higher burnout, while perceptions of workplace stress increased in all clinics after the redesign.
Conclusions
Our findings partially align with expectations of work redesign as a route to improving physician and staff experiences in delivering care. Although teamwork and engagement increased, the redesigns in our study were not enough to moderate long-standing challenges facing primary care. Yet higher levels of empowerment and engagement, as observed in the pilot clinic, may be particularly effective in facilitating improvements while combating fatigue. To help practices cope with increasing burdens, interventions must directly benefit healthcare professionals without overtaxing an already overstretched workforce.
Electronic supplementary material
The online version of this article (10.1186/s12913-018-3062-5) contains supplementary material, which is available to authorized users.
Keywords: Primary care redesign; Patient care team; Work environment, Professional burnout; Organizational innovation
Background
Primary care faces growing pressure to deliver higher quality care at lower cost, a trend accelerated in the United States by recent expansion of insurance coverage and embodied in the growth of value-based payment [1, 2]. Demand for primary care change in the U.S and other industrial countries reflects budgetary constraints, population ageing, growing chronic illness, and reliance on primary care to reduce use of more costly services [3]. In response, leaders have advocated and introduced a wide range of primary care workforce innovations, including some that redesign the entire practice. These redesigns create teams in which more time is allocated for managing chronic and preventive care, and where allied health practitioners relieve physicians of routine tasks [4–6].
One important question is how such care redesigns affect physicians and other members of primary care teams. This issue is particularly important in view of growing evidence on physician dissatisfaction and burnout, and concern over shortages of primary care physicians and nurses [3, 7]. Some analysts anticipate that if physicians’ tasks are shared by other team members, physicians will experience greater work satisfaction and less burnout [1, 8]. Observations of high-functioning primary care practices support this expectation [9], as do some studies on implementing the patient-centered medical home (PCMH) [10, 11]. There is evidence that a diverse range of changes in primary care, including work redesigns, can reduce burnout and enhance satisfaction [12–14], but limited information on how these changes affect particular types of physicians and also nonphysician staff.
Further research is clearly needed to illuminate how physicians and other staff experience care redesign and how diverse settings impact these experiences. To help address these questions, we report here on a study of a primary care redesign that grew out of an application of Lean management principles, which were derived from the manufacturing industry. Lean’s basic premise is to improve efficiency by removing waste and streamlining flow [15, 16]. This is accomplished through the mapping of start-to-end processes, called “value stream mapping,” to identify non-value-added activities. More broadly Lean aims to empower and engage the workforce in continuous quality improvement [16–18]. This type of approach has been shown to improve healthcare delivery [16, 19–24] and a wide range of operational metrics such as efficiency, productivity, and satisfaction among patients, providers and staff, without detriments to clinical quality [25]. But less is known about Lean’s influence on teamwork, staff engagement, and participation in quality improvement, all of which are also targeted by Lean management principles.
To contribute to the broader study of care redesign and add to knowledge of Lean in primary care, we examine physician and staff experiences after implementing a series of workflow changes. Based on the goals of Lean methodology and previous findings from inpatient settings [24, 26], we expect work redesigns to increase staff empowerment, engagement, and satisfaction among primary care physicians and other care team members. We also expect that Lean redesigns can reduce burnout and workplace stress among staff. However, we recognize some analysts expect that Lean applications could lead to a speed-up of care and reductions in autonomy [27, 28], which may ultimately result in higher burnout and work dissatisfaction. These issues are considered within our broader study of work experiences among primary care physicians and nonphysician staff.
Methods
Study setting and data source
This study was conducted in a not-for-profit, ambulatory care system in the U.S serving over one million patients across six counties. In efforts to improve performance, the delivery system implemented Lean-based redesigns beginning in the area of primary care. The redesigns were implemented in all primary care departments using the same sequence of activities: (1) “5S” standardization of medical equipment, supplies, and health education materials in patient exam rooms; (2) call management and redesign of call center functions; (3) co-location of existing care teams composed of a physician and a medical assistant (MA); and (4) redesign of care team roles and workflows, including daily huddles between physician-MA dyadic care teams, agenda setting by MAs at the start of patient visits, and designation of all MAs as care team “Flow Managers” responsible for managing or triaging incoming patient care items (e.g., test results, referrals, patient messages). Over an implementation period of 2 years, daily workflows for all physicians and staff were redesigned in 46 primary care departments located within 17 geographically distinct clinics across the system. Each clinic location housed 1 to 3 primary care departments, i.e., Family Medicine, Internal Medicine, and/or Pediatrics. The implementation occurred in three phases, starting with primary care departments in one pilot clinic (phase 1), followed by three “beta” test clinics (phase 2), and completed in all 13 remaining clinics (phase 3). During the pilot phase, physicians and other staff were deeply engaged in the design of new work roles and workflows. These changes were implemented in the beta clinics with some further modifications, and then spread to the remaining clinics by organizational leaders with the support of external Lean consultants.
Prior to implementation, a team of independent researchers embedded within the delivery system fielded a baseline survey to 1333 primary care physicians and non-physician staff (e.g., MAs, licensed vocational nurses, patient service representatives) across the system. The organization’s Institutional Review Board (IRB) approved all data collection activities, which included voluntary completion of work experience surveys. The average response rate for the baseline survey was 73%, with a range of 63%–86% by clinic location. A follow-up survey was administered in the same clinics to 1164 physicians and staff upon completion of redesigns. Based on the sequential phases of implementation, this follow-up survey was administered 2.5 to 3 years after completion of redesigns in the pilot clinic, 1.5 to 2 years after completing redesigns in phase 2 clinics, and 8 to 5 months after redesigns were completed in phase 3 clinics. The follow-up had an average response rate of 74%, ranging from 67%–77% by clinic location. Both surveys assessed current experiences of work, including levels of employee engagement and job-related burnout; and perceptions of work environments such as degree of teamwork, participation in decision making, and levels of stress in the workplace.
Work experience measures
Physician and staff engagement
We assessed employee engagement among physicians and staff using an adapted version of a work experience survey [29]. As this instrument lacked specification of a priori domains, we conducted exploratory factor analysis with varimax rotation that yielded three separate factors (3 items per domain, eigenvalues > 1) with Cronbach’s alpha coefficients of 0.89, 0.84 and 0.81, respectively. We labeled these factors as: (1) Personal motivation, perceptions among staff that work contributions are valued and that professional development is encouraged (e.g., “My ideas and suggestions for improvement are valued by my department,” “My manager provides me with sufficient opportunities to improve myself”); (2) Work satisfaction, degree to which individuals are satisfied in the workplace (e.g., “Overall, I think this is a great place to work”); and (3) Ownership, degree to which individuals contribute to and understand how their efforts affect the organization’s goals (e.g., “I am willing to put in a great deal of effort to help my department succeed,” “I understand how my daily work contributes to my department’s mission”).
Work environment
We assessed perceptions of the work environment using a validated instrument developed to measure organizational attributes in primary care practices [30]. This instrument has three subscales of 3–5 items each, all demonstrating high internal consistency and reliability with Cronbach’s alpha coefficients of 0.76, 0.74, and 0.71. The following attributes were assessed in each department: (1) Teamwork, the extent to which members from different organizational levels and job functions work together as a team (e.g., “Staff and clinicians in this department operate as a real team”); (2) Participation in Decision Making or collective problem solving (e.g., “All staff members participate in important decisions about clinical operations”); and (3) Workplace Stress, reflecting negative feelings about workload and operating conditions (e.g., “This department is experienced as ‘stressful’,” “It’s hard to make any changes in this department because we’re so busy seeing patients”).
All measures of engagement and work environment used 5-point Likert scales ranging from 1 = “strongly disagree” to 5 = “strongly agree.” Scores for each domain were averaged for each respondent.
Job-related burnout
The well-validated Maslach Burnout Inventory (MBI—Human Services Version) [31] was used to assess levels of burnout and how health professionals view their daily work activities. We used the MBI to measure three domains each with 5–7 items and Cronbach’s alpha coefficients of 0.91, 0.70, and 0.76, respectively: (1) Emotional exhaustion or fatigue from delivering patient care (e.g., “I feel emotionally drained from my work”); (2) Depersonalization, a hardening of the attitudes of care providers toward patients (e.g., “I feel I treat some patients as if they were impersonal objects”); and (3) Personal accomplishment, a positive self-assessment of care provision (e.g., “I feel I’m positively influencing other people’s lives through my work”). All statements were assessed on 7-point scales ranging from 1 = “never” to 7 = “every day,” and averaged for each respondent.
Respondent characteristics
Demographic and other respondent characteristics included: gender, age, ethnicity, race, education, departmental tenure, professional role, and clinic phase for implementing Lean redesigns. The variables were categorized with reference groups: female, over 60, non-Hispanic, white, more than 4-year college degree, less than 1-year tenure, physician, and pilot clinic (phase 1 implementation). Based on two sample independent t-tests, the two statistically significant differences in respondent characteristics between baseline and follow-up cohorts were respondent race and departmental tenure.
Statistical analysis
We first conducted multivariate regression analyses to detect changes in work experiences between baseline and follow-up surveys, adjusting for respondent characteristics and response clustering within departments in each clinic-location. To assess need for hierarchical modeling, intercept-only models were first used to calculate intra-class correlations (ICC) for each outcome variable. All ICC values were above 0.10 suggesting the appropriateness of the hierarchical approach [32]. All regression analyses thus leveraged random intercept models to account for the hierarchical (i.e., nested) structure of individuals located within departments. The main covariate of interest in each regression model was a binary variable indicating follow-up, as compared with baseline, experiences as reported on physician and staff surveys. Robust standard errors were estimated in all models to avoid violating the assumption of independence due to correlated observations within departments. All models were fitted excluding null values or outliers identified in diagnostic plots of residuals. Statistical analyses were conducted using R version 2.11.1 and SAS Enterprise Guide 5.1.
Results
Table 1 presents univariate results for both baseline and follow-up survey respondents. There were no structural differences between cohorts except for tenure in the department and distribution of respondent race/ethnicity.
Table 1.
Characteristics of Survey Respondents
| Baseline (N = 970) |
Follow-up (N = 860) |
|||
|---|---|---|---|---|
| N | % | N | % | |
| Gender | ||||
| Female | 770 | 79% | 599 | 70% |
| Male | 169 | 17% | 122 | 14% |
| Age | ||||
| Under 30 | 145 | 15% | 113 | 13% |
| 30–39 | 313 | 32% | 212 | 25% |
| 40–49 | 255 | 26% | 213 | 25% |
| 50–59 | 181 | 19% | 143 | 17% |
| 60 or over | 49 | 5% | 43 | 5% |
| Ethnicity | ||||
| Non-Hispanic | 689 | 71% | 400 | 47% |
| Hispanic | 205 | 21% | 122 | 14% |
| Race* | ||||
| Black or African American | 22 | 2% | 7 | 1% |
| American Indian or Alaska Native | 3 | 0.3% | 5 | 1% |
| Native Hawaiian or Pacific Islander | 18 | 2% | 20 | 3% |
| Asian | 221 | 23% | 129 | 16% |
| White (European, Middle Eastern) | 437 | 45% | 284 | 34% |
| Other | 207 | 21% | 40 | 5% |
| Education | ||||
| Some high school, High school graduate/GED | 71 | 7% | 53 | 6% |
| Some college or 2-year degree | 394 | 41% | 274 | 32% |
| 4-year college degree | 99 | 10% | 74 | 9% |
| More than 4-year college degree | 392 | 40% | 330 | 38% |
| Tenure in Department* | ||||
| Less than 1 year | 105 | 11% | 78 | 9% |
| 1–2 years | 99 | 10% | 113 | 13% |
| 2–5 years | 278 | 29% | 140 | 16% |
| More than 5 years | 478 | 49% | 414 | 48% |
| Specialty | ||||
| Family Medicine | 290 | 30% | 328 | 38% |
| Internal Medicine | 261 | 27% | 280 | 33% |
| Pediatrics | 235 | 24% | 252 | 29% |
| Professional Role | ||||
| Physician | 350 | 36% | 330 | 38% |
| Non-Physician | 518 | 53% | 521 | 61% |
| Phase of Lean Implementation | ||||
| Pilot (phase 1) | 133 | 14% | 99 | 12% |
| Beta (phase 2) | 328 | 34% | 270 | 31% |
| Gamma (phase 3) | 509 | 52% | 491 | 57% |
Note: Cells may not add to 100% due to missing data
*p < 0.05
As shown in Fig. 1, there were improvements in reported measures of engagement, teamwork, and participation in decision-making among physicians and staff after implementing Lean changes. However, reports of workplace stress (a measure of work environment) and emotional exhaustion (a measure of burnout) also dramatically increased. Since there were some differences between the experiences of physicians and nonphysician staff, we present these results separately in Tables 2 and 3.
Fig. 1.
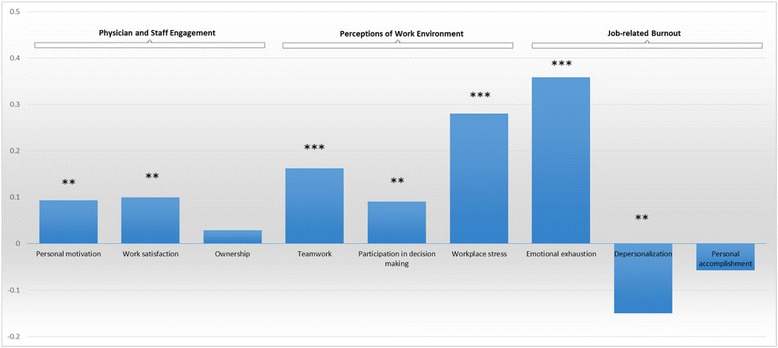
Changes in Physician and Staff Experiences After Lean Workflow Redesigns. Reference group: Baseline survey. Note: All models are adjusted for respondent characteristics, including gender, age, race/ ethnicity, education, department tenure, and clinic phase of implementation. **p < 0.05, ***p < 0.01
Table 2.
Changes in Physician Experiences After Workflow Redesigns (N = 680)
| Experience Domains | Parameter Estimatea | Standard Deviation |
|---|---|---|
| Physician Engagement | ||
| Personal motivation | 0.065 | 0.076 |
| Work satisfaction | 0.122* | 0.089 |
| Ownership | 0.091* | 0.064 |
| Perceptions of Work Environment | ||
| Teamwork | 0.200*** | 0.060 |
| Participation in decision making | 0.100* | 0.077 |
| Workplace stress | 0.406*** | 0.068 |
| Job-related Burnout | ||
| Emotional exhaustion | 0.390*** | 0.135 |
| Depersonalization | −0.018 | 0.112 |
| Personal accomplishment | −0.154** | 0.069 |
Note: All models are adjusted for respondent characteristics, including gender, age, race/ ethnicity, education, department tenure, and clinic phase of implementation
aReference group: Baseline survey
*p < 0.10, **p < 0.05, ***p < 0.01
Table 3.
Changes in Nonphysician Staff Experiences After Workflow Redesigns (N = 1039)
| Experience Domains | Parameter Estimatea | Standard Deviation |
|---|---|---|
| Staff Engagement | ||
| Personal motivation | 0.115** | 0.070 |
| Work satisfaction | 0.076 | 0.066 |
| Ownership | −0.005 | 0.052 |
| Perceptions of Work Environment | ||
| Teamwork | 0.146** | 0.059 |
| Participation in decision making | 0.096* | 0.069 |
| Workplace stress | 0.177*** | 0.067 |
| Job-related Burnout | ||
| Emotional exhaustion | 0.365** | 0.120 |
| Depersonalization | −0.244*** | 0.077 |
| Personal accomplishment | 0.034 | 0.097 |
Note: All models are adjusted for respondent characteristics, including gender, age, race/ ethnicity, education, department tenure, and clinic phase of implementation
aReference group: Baseline survey
*p < 0.10, **p < 0.05, ***p < 0.01
Physicians reported increases in two of the three engagement measures: work satisfaction and ownership. There were no improvements at follow-up for nonphysician staff in these dimensions, but there was growth in personal motivation, another measure of engagement. Positive trends in perceptions of the work environment, including teamwork and participation in decisions to improve care, were the same for both groups. Nonphysician staff reported greater work stress, as did physicians, but the increase from baseline was much greater among physicians. Both occupational groupings also experienced higher levels of emotional exhaustion after the redesigns, but only physicians reported lower feelings of personal accomplishment. In contrast, after the redesigns, staff other than physicians reported less depersonalization of relations to patients than had originally been the case.
All work experience results shown in Tables 2 and 3 were adjusted for respondent characteristics. Briefly, respondents of younger age (less than 60) and with longer tenure in the department (over 2 years in most cases) reported less engagement, teamwork and motivation, along with more stress and burnout compared to the reference groups (i.e., those over 60 and those with less than 1 year tenure). Non-physicians with less education reported less emotional exhaustion and workplace stress, along with more personal accomplishment and work satisfaction compared to those with more than a four-year degree. Race was significant with African American physicians reporting less work satisfaction, while Asian and Native Hawaiian/Pacific Islander physicians and non-physician staff reported more motivation and less burnout, than white physicians. Among physicians, males reported more personal motivation, teamwork, and work satisfaction than females. These results can be found in the Additional files 1 and 2.
To further explore the growth in workplace stress and burnout observed in Tables 2 and 3, we examined relationships between changes in work experiences and specific phase in which clinics implemented the redesigns. Implementation phase provided a rough indicator of how long respondents were exposed to the new workflows. There were no significant differences in stress or burnout levels between either phase 2 or phase 3 clinics and the pilot site. Hence, changes in work stress and burnout do not appear to reflect length of exposure to the redesigns. To explore these changes further, we conducted three separate sets of regression analyses for each distinct cohort of clinics according to implementation phase. As shown in Table 4, in all three phases perceptions of workplace stress were higher after the redesign than beforehand. Members of all clinics except for the pilot also reported higher burnout at follow-up compared to baseline. In contrast, members of the pilot clinic reported a higher sense of personal accomplishment from work and no changes on the other two measures of burnout after implementing Lean redesigns.
Table 4.
Changes in Workplace Stress and Burnout After Redesigns in Each Phase (Separate Analyses, by Implementation Phase)
| Pilot (Phase 1) (N = 232) |
Betas (Phase 2) (N = 558) |
All Other Clinics (Phase 3) (N = 1000) |
||||
|---|---|---|---|---|---|---|
| Experience Domains | Parameter Estimatea | (SD) | Parameter Estimatea | (SD) | Parameter Estimatea | (SD) |
| Perceptions of Work Environment | ||||||
| Workplace stress | 0.419*** | (0.144) | 0.332*** | (0.090) | 0.231*** | (0.063) |
| Job-related Burnout | ||||||
| Emotional exhaustion | −0.016 | (0.248) | 0.476*** | (0.164) | 0.383*** | (0.120) |
| Depersonalization | −0.016 | (0.207) | −0.230* | (0.118) | −0.117 | (0.087) |
| Personal accomplishment | 0.417* | (0.222) | −0.308*** | (0.095) | −0.001 | (0.086) |
Note: All models adjusted for respondent characteristics, including gender, age, race/ethnicity, education, department tenure, and clinic implementation phase
SD, Standard Deviation
aReference group: Baseline survey
*p < 0.05, **p < 0.01, ***p < 0.001
Discussion
We examined differences in work experiences reported by physicians and staff after a system-wide redesign in primary care clinics. The redesign, which was based on Lean workflow principles, co-located MA-physician dyads, delegated significant responsibilities to MAs, and mandated greater coordination and communication among care team members. After implementation of Lean redesigns, physicians and staff reported higher levels of teamwork and more participation in decisions to improve care. Physicians also reported higher levels of engagement, including increased work satisfaction and ownership, while nonphysician staff reported becoming more personally motivated at work. However, both physicians and other staff experienced increased burnout at follow-up, and reported higher workplace stress than at baseline.
These mixed findings partially align with the expectations of researchers who view work redesign as a route to improving the experience of primary care providers. In our study, teamwork, participation, and work engagement rose among physicians and staff, as might have been anticipated from other studies of primary care redesign and from research on Lean in hospital settings [9, 33–36]. These findings may have reflected specific benefits of co-locating each dyadic care team in a shared workspace. Besides improving workflow efficiency, this feature of the redesign served to enhance communication and partnership between physicians and MAs. Additionally, formal re-designation of MAs as Lean “Flow Managers” may have yet furthered a sense of teamwork and participation in decisions; in this new role, MAs became responsible for managing daily team workflows and incoming patient care items.
These findings are aligned with past observations of primary care redesigns that found benefits in proximity of workstations, and that “shared-care models” improved satisfaction among physicians and staff [9, 33, 34]. However, although these activities likely increased experiences of teamwork and participation in the work process, these improvements did not significantly enhance nonphysicians’ sense of ownership or overall work satisfaction as observed among physicians. Similarly, other researchers who studied a number of primary care practices found the transition to team-based care “does not come naturally” and, in fact, may be particularly challenging among certain health professionals [37]. It may be that other aspects of physician–staff interactions remain unaffected by redesigns and continue to reinforce certain experiences among nonphysicians with the care delivery process.
Unlike our research, prior studies have not typically explored whether new team functions may lead to unintended consequences like burnout. We found that despite their positive effects, Lean redesigns did not relieve work burdens reported by both physicians and non-physician staff. On the contrary, after the redesigns both groups reported significantly higher levels of workplace stress and some forms of burnout than they did beforehand. Lean efficiencies have been found in other care settings to “give the gift of time” [38], but this was not apparent in our study of primary care clinics. Although reported work experiences may reflect demands imposed by this organization as it sought to increase efficiency, it is also entirely possible that they reflect secular trends such as the growing burden on primary care providers. This was likely aggravated during our study period as pressure grew to manage complex patients and as insurance coverage expanded under the Affordable Care Act, which passed and was implemented contemporaneously with the Lean initiative at this study organization. Hence, our study may serve to highlight unique differences between primary care and other healthcare settings that have adopted Lean, potentially reflecting distinctive challenges facing primary care. Consistent with this, other studies indicate that primary care may be especially vulnerable to increasing workloads and decreased satisfaction after initiation of new designs [39].
Our study may also reflect features of primary care change that make it difficult, but not impossible, to obtain benefits of teamwork and task delegation as reported in some studies. One possibility is suggested by the contrast between our findings and those of Linzer and colleagues [13]. In their research, physicians whose practices were randomly selected for an intervention group were encouraged to choose among a variety of possible workflow designs targeting known predictors of burnout, and then to develop quality improvement teams to implement them based on their own practice data. In our study, members of the pilot team also were deeply engaged in developing new workflows; however, members of the phase 2 beta sites and all remaining phase 3 sites had less discretion, since they were charged mainly with either adopting or adapting designs to fit their local environments. The difference in empowerment between the majority of clinics in our study and those in the experiment by Linzer and colleagues [13] may help explain the divergence in burnout outcomes. In like manner, greater empowerment of the pilot clinic members in our study may explain why they did not experience more burnout after implementing changes. It may be that staff engagement is particularly effective in facilitating improvements while also combating fatigue.
Finally, some limitations of our study include the lack of a comparison group as the organization implemented Lean redesigns in all clinic sites. Thus, we cannot determine with certainty whether observed changes were due to secular trends or to the Lean redesign itself. Nor was our study based on a panel design, though we do provide a comparison of respondent characteristics from the baseline and follow-up surveys. Based on these results and adjusted regression models, it is unlikely that self-selection or workforce composition skewed the differences observed in pre- and post-Lean work experiences. Finally, closed-ended questions on the MBI were not detailed enough for us to identify specific causes of reported burnout. Despite this limitation, we attempted to distinguish between Lean-caused fatigue versus secular trends in primary care by exploring patterns between pilot clinic, phase 2 and phase 3 implementation sites.
Conclusions
Leveraging operational activities and survey data in a large ambulatory care delivery system, we sought to understand work experiences of primary care physicians and staff after implementing workflow redesigns that held promise for fostering teamwork, communication, and workflow efficiency for all clinic staff. The redesigns were also intended to reduce workload and burnout among physicians by delegating some tasks to other staff members. Following implementation of changes, we indeed observed higher levels of teamwork, participation and engagement, but we also found higher levels of workplace stress and burnout. Taken together, our results provide a complex picture of the impact of Lean on primary care physicians and staff. Despite the largely favorable responses among survey respondents, our study suggests that Lean-based redesigns have not yet reduced growing challenges in primary care, where a shortage of physicians and growing patient population create dual burdens on care delivery. To help primary care practices cope with existing challenges, changes must create efficiencies that directly benefit care providers without overtaxing an already overstretched workforce.
Additional files
Respondent Characteristics When Assessing Changes in Physician Experiences After Workflow Redesigns. This file details all the respondent characteristics that were adjusted for in the analysis of physician work experiences shown in Table 2. (DOCX 601 kb)
Respondent Characteristics When Assessing Changes in Non-physician Staff Experiences After Workflow Redesigns. This file details all the respondent characteristics that were adjusted for in the analysis of non-physician staff work experiences shown in Table 3. (DOCX 562 kb)
Acknowledgements
Not applicable
Funding
The research reported in this paper was funded by the Agency for Healthcare Research and Quality under its ACTION II contract HHSA2902010000221, Task Order 2. The views expressed in this paper are solely those of the authors and do not represent any US government agency or any institutions with which the authors are affiliated.
Availability of data and materials
The datasets used for this study are available from the corresponding author upon request.
Abbreviations
- HMO
Health maintenance organization
- ICC
Intra-class correlations
- MA
Medical assistant
- MBI
Maslach Burnout Inventory
- PCMH
Patient-centered medical home
Authors’ contributions
DYH oversaw and coordinated all aspects of the study. DYH, XD, and QT were involved in data extraction, analysis, and illustration of findings. DYH, MIH, QT, and XD were actively engaged in interpretation of results, writing of the manuscript, and commenting on the development and refinement of intellectual content. All authors read and approved the completed manuscript.
Ethics approval and consent to participate
Study activities were conducted with approval from the Institutional Review Board (protocol #12–06-143). Physicians and staff completed the surveys as part of their regular duties, and consent was implied with completion of the survey.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (10.1186/s12913-018-3062-5) contains supplementary material, which is available to authorized users.
Contributor Information
Dorothy Y. Hung, Phone: (650) 853-4807, Email: hungd@pamfri.org
Michael I. Harrison, Phone: (301) 427-1434, Email: michael.harrison@ahrq.hhs.gov
Quan Truong, Phone: (650) 330-4528, Email: truongq@pamfri.org.
Xue Du, Phone: (650) 625-3874, Email: dux@pamfri.org.
References
- 1.Bodenheimer TS, Smith MD. Primary care: proposed solutions to the physician shortage without training more physicians. Health Aff (Millwood) 2013;32(11):1881–1886. doi: 10.1377/hlthaff.2013.0234. [DOI] [PubMed] [Google Scholar]
- 2.VanLare JM, Conway PH. Value-based purchasing--national programs to move from volume to value. N Engl J Med. 2012;367(4):292–295. doi: 10.1056/NEJMp1204939. [DOI] [PubMed] [Google Scholar]
- 3.Five Year Forward View [www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf].
- 4.Friedman A, Hahn KA, Etz R, Rehwinkel-Morfe AM, Miller WL, Nutting PA, Jaén CR, Shaw EK, Crabtree BF. A typology of primary care workforce innovations in the United States since 2000. Med Care. 2014;52(2):101–111. doi: 10.1097/MLR.0000000000000043. [DOI] [PubMed] [Google Scholar]
- 5.Margolius D, Bodenheimer T. Transforming primary care: from past practice to the practice of the future. Health Aff (Millwood) 2010;29(5):779–784. doi: 10.1377/hlthaff.2010.0045. [DOI] [PubMed] [Google Scholar]
- 6.National Health Service PCWCfHEE . The future of primary care, creating teams for tomorrow. 2015. [Google Scholar]
- 7.Ariely D, Lanier WL. Disturbing trends in physician burnout and satisfaction with work-life balance: dealing with malady among the Nation's healers. Mayo Clin Proc. 2015;90(12):1593–1596. doi: 10.1016/j.mayocp.2015.10.004. [DOI] [PubMed] [Google Scholar]
- 8.Rabatin J, Williams E, Baier Manwell L, Schwartz M, Brown R, Linzer M. Predictors and outcomes of burnout in primary care physicians. J Prim Care Community Health. 2016;7(1):41–43. doi: 10.1177/2150131915607799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sinsky CA, Willard-Grace R, Schutzbank AM, Sinsky TA, Margolius D, Bodenheimer T. In search of joy in practice: a report of 23 high-functioning primary care practices. Ann Fam Med. 2013;11(3):272–278. doi: 10.1370/afm.1531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Reid RJ, Coleman K, Johnson EA, Fishman PA, Hsu C, Soman MP, Trescott CE, Erikson M, Larson EB. The group health medical home at year two: cost savings, higher patient satisfaction, and less burnout for providers. Health Aff (Millwood) 2010;29(5):835–843. doi: 10.1377/hlthaff.2010.0158. [DOI] [PubMed] [Google Scholar]
- 11.Day J, DL S, Kim J, Sheets-Mervis A, Day R, Tomoaia-Cotisel A, Waitzman NJ, MK M. Quality, satisfaction, and financial efficiency associated with elements of primary care practice transformation: preliminary findings. Ann Fam Med. 2013;11(Suppl 1):550–559. doi: 10.1370/afm.1475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.West C, Dyrbye L, Erwin P, Shanafelt T. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;388(10057):2272–2281. doi: 10.1016/S0140-6736(16)31279-X. [DOI] [PubMed] [Google Scholar]
- 13.Linzer M, Sinsky C, Poplau S, Brown R, Williams E. Healthy work place investigators: joy in medical practice: clinician satisfaction in the healthy work place trial. Health Aff (Millwood) 2017;36(10):1808–1814. doi: 10.1377/hlthaff.2017.0790. [DOI] [PubMed] [Google Scholar]
- 14.Shanafelt TD, Noseworthy J. Executive leadership and physician well-being: nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92(1):129–146. doi: 10.1016/j.mayocp.2016.10.004. [DOI] [PubMed] [Google Scholar]
- 15.Andersen H, Rovik KA, Ingebrigtsen T. Lean thinking in hospitals: is there a cure for the absence of evidence? A systematic review of reviews. BMJ Open. 2014;4(1):e003873. doi: 10.1136/bmjopen-2013-003873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Womack JP, Byrne AP, Flume OJ, Kaplan GS, Toussaint J. IHI innovation series white paper. Cambridge, MA: Institute for Healthcare Improvement; 2005. Going lean in health care. [Google Scholar]
- 17.Shah R, Ward PT. Defining and developing measures of lean production. J Oper Manag. 2007;25(4):785–805. doi: 10.1016/j.jom.2007.01.019. [DOI] [Google Scholar]
- 18.Spear S, Bowen HK. Decoding the DNA of the Toyota production system. Harv Bus Rev. 1999;77:96–108. [Google Scholar]
- 19.Wojtys EM, Schley L, Overgaard KA, Agbabian J. Applying lean techniques to improve the patient scheduling process. J Healthc Qual. 2009;31(3):10–16. doi: 10.1111/j.1945-1474.2009.00025.x. [DOI] [PubMed] [Google Scholar]
- 20.Braaten JS, Bellhouse DE. Improving patient care by making small sustainable changes: a cardiac telemetry unit's experience. Nurs Econ. 2007;25(3):162–166. [PubMed] [Google Scholar]
- 21.Kim CS, Spahlinger DA, Billi JE. Creating value in health care: the case for lean thinking. JCOM. 2009;16(12):557–562. [Google Scholar]
- 22.Mazzocato P, Savage C, Brommels M, Aronsson H, Thor J. Lean thinking in healthcare: a realist review of the literature. Qual Saf Health Care. 2010;19(5):376–382. doi: 10.1136/qshc.2009.037986. [DOI] [PubMed] [Google Scholar]
- 23.Garcia, M. Using Lean Management principles to improve patient satisfaction and reduce wait times at UNM GI/Endoscopy. UNM CIR Journal of Quality Improvement in Healthcare. 2017;2(1).
- 24.Jimmerson C, Weber D, Sobek DK. Reducing waste and errors: piloting lean principles at Intermountain Healthcare. Jt Comm J Qual Patient Saf. 2005;31(5):249–257. doi: 10.1016/S1553-7250(05)31032-4. [DOI] [PubMed] [Google Scholar]
- 25.Hung DY, Harrison MI, Martinez MC, Luft HS. Scaling lean in primary care: impacts on system performance. Am J Manag Care. 2017;23(3):161–168. [PubMed] [Google Scholar]
- 26.Kaplan GS, Patterson SH. Seeking perfection in healthcare. A case study in adopting Toyota production system methods. Healthc Exec. 2008;23(3):16–18. [PubMed] [Google Scholar]
- 27.Hartzband P, Groopman J. Medical Taylorism. N Engl J Med. 2016;374(2):106–108. doi: 10.1056/NEJMp1512402. [DOI] [PubMed] [Google Scholar]
- 28.Rees GH, Gauld R. Can lean contribute to work intensification in healthcare? J Health Organ Manag. 2017;31(3):369–384. doi: 10.1108/JHOM-11-2016-0219. [DOI] [PubMed] [Google Scholar]
- 29.Helping you build a high-performance culture [http://www.advisory.com/talent-development/employee-engagement-initiative]. [PubMed]
- 30.Ohman-Strickland PA, John Orzano A, Nutting PA, Perry Dickinson W, Scott-Cawiezell J, Hahn K, Gibel M, Crabtree BF. Measuring organizational attributes of primary care practices: development of a new instrument. Health Serv Res. 2007;42(3 Pt 1):1257–1273. doi: 10.1111/j.1475-6773.2006.00644.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Maslach C, Jackson SE, Leiter MP, Schaufeli WB, Schwab RL. Maslach burnout inventory (human services) 1986. [Google Scholar]
- 32.Snijders T, Bosker R. Multilevel analysis: an introduction to basic and advanced multilevel modeling. Thousand Oaks, CA: Sage Publications; 1999. [Google Scholar]
- 33.O'Malley AS, Gourevitch R, Draper K, Bond A, Tirodkar MA. Overcoming challenges to teamwork in patient-centered medical homes: a qualitative study. J Gen Intern Med. 2015;30(2):183–192. doi: 10.1007/s11606-014-3065-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ghorob A, Bodenheimer T. Building teams in primary care: a practical guide. Fam Syst Health. 2015;33(3):182–192. doi: 10.1037/fsh0000120. [DOI] [PubMed] [Google Scholar]
- 35.Drotz E, Poksinska B. Lean in healthcare from employees’ perspectives. J Health Organ Manag. 2014;28(2):177–195. doi: 10.1108/JHOM-03-2013-0066. [DOI] [PubMed] [Google Scholar]
- 36.Ulhassan W, Westerlund H, Thor J, Sandahl C, Schwarz U. Does lean implementation interact with group functioning? J Health Organ Manag. 2014;28(2):196–213. doi: 10.1108/JHOM-03-2013-0065. [DOI] [PubMed] [Google Scholar]
- 37.Ladden MD, Bodenheimer T, Fishman NW, Flinter M, Hsu C, Parchman M, Wagner EH. The emerging primary care workforce: preliminary observations from the primary care team: learning from effective ambulatory practices project. Acad Med. 2013;88(12):1830–1834. doi: 10.1097/ACM.0000000000000027. [DOI] [PubMed] [Google Scholar]
- 38.Nelson-Peterson DL, Leppa CJ. Creating an environment for caring using lean principles of the Virginia Mason production system. J Nurs Adm. 2007;37(6):287–294. doi: 10.1097/01.NNA.0000277717.34134.a9. [DOI] [PubMed] [Google Scholar]
- 39.Tufano JT, Ralston JD, Martin DP. Providers’ experience with an organizational redesign initiative to promote patient-centered access: a qualitative study. J Gen Intern Med. 2008;23(11):1778–1783. doi: 10.1007/s11606-008-0761-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Respondent Characteristics When Assessing Changes in Physician Experiences After Workflow Redesigns. This file details all the respondent characteristics that were adjusted for in the analysis of physician work experiences shown in Table 2. (DOCX 601 kb)
Respondent Characteristics When Assessing Changes in Non-physician Staff Experiences After Workflow Redesigns. This file details all the respondent characteristics that were adjusted for in the analysis of non-physician staff work experiences shown in Table 3. (DOCX 562 kb)
Data Availability Statement
The datasets used for this study are available from the corresponding author upon request.