

Key Points
The administration of third-party FMT capsules early after allogeneic HCT is feasible and appears safe.
FMT is associated with early expansion of microbiome diversity in transplant recipients.
Abstract
We hypothesized that third-party fecal microbiota transplantation (FMT) may restore intestinal microbiome diversity after allogeneic hematopoietic cell transplantation (allo-HCT). In this open-label single-group pilot study, 18 subjects were enrolled before allo-HCT and planned to receive third-party FMT capsules. FMT capsules were administered no later than 4 weeks after neutrophil engraftment, and antibiotics were not allowed within 48 hours before FMT. Five patients did not receive FMT because of the development of early acute gastrointestinal (GI) graft-versus-host disease (GVHD) before FMT (n = 3), persistent HCT-associated GI toxicity (n = 1), or patient decision (n = 1). Thirteen patients received FMT at a median of 27 days (range, 19-45 days) after HCT. Participants were able to swallow and tolerate all FMT capsules, meeting the primary study endpoint of feasibility. FMT was tolerated well, with 1 treatment-related significant adverse event (abdominal pain). Two patients subsequently developed acute GI GVHD, with 1 patient also having concurrent bacteremia. No additional cases of bacteremia occurred. Median follow-up for survivors is 15 months (range, 13-20 months). The Kaplan-Meier estimates for 12-month overall survival and progression-free survival after FMT were 85% (95% confidence interval, 51%-96%) and 85% (95% confidence interval, 51%-96%), respectively. There was 1 nonrelapse death resulting from acute GI GVHD (12-month nonrelapse mortality, 8%; 95% confidence interval, 0%-30%). Analysis of stool composition and urine 3-indoxyl sulfate concentration indicated improvement in intestinal microbiome diversity after FMT that was associated with expansion of stool-donor taxa. These results indicate that empiric third-party FMT after allo-HCT appears to be feasible, safe, and associated with expansion of recipient microbiome diversity. This trial was registered at www.clinicaltrials.gov as #NCT02733744.
Visual Abstract
Introduction
The role of the intestinal microbiota and its potential influence on clinical outcomes for patients undergoing allogeneic hematopoietic cell transplantation (allo-HCT) has been investigated in recent years.1-3 Multiple factors contribute to significantly reduced microbiota diversity in patients undergoing allo-HCT, including previous and peri-HCT use of antibiotics, administration of chemotherapy and/or radiation, and altered nutritional patterns. Analyses of fecal specimens taken from recipients of allo-HCT around the time of engraftment have shown that reduced intestinal microbiome diversity is associated with significantly worse survival outcomes, and that changes in microbiota composition may influence important clinical outcomes such as acute graft-versus-host disease (GVHD) and disease relapse.4-6 Although these associations between microbiome diversity and clinically important outcomes after allo-HCT do not demonstrate causality, they provide data to support clinical evaluation as to whether these relationships can be modified to influence outcomes for patients.
We hypothesize that approaches to restore a patient’s microbiome diversity after HCT may improve outcomes after HCT. Although such approaches to restoring microbiome diversity are still investigational, fecal microbiota transplantation (FMT) from a healthy individual carries promise, as initial studies have shown this approach to be a remarkably effective therapy for recurrent Clostridium difficile infection, for which loss of microbiome diversity is an important predisposing factor.7 Early approaches to FMT for C difficile colitis administered liquid fecal inocula by invasive methods such as nasogastric intubation or endoscopy.8,9 A novel approach to FMT administration is through third-party frozen, encapsulated inoculum, which can be delivered by the oral route.10,11 In this pilot study, we investigated whether empiric third-party frozen FMT capsules would be safe and feasible after allo-HCT, and would be able to restore recipient microbiome diversity.
Methods
Patients
This study was approved by the Institutional Review Board at the Dana-Farber Harvard Cancer Center and conducted under IND 16857 (Holder: E. Hohmann). The study was conducted at the Massachusetts General Hospital Cancer Center. Written informed consent was obtained from all subjects. This trial was registered at ClinicalTrials.gov (NCT02733744). Patients were between the ages of 18 and 75 years and undergoing a first allo-HCT. Eligible conditioning regimens were myeloablative or the combination of fludarabine with melphalan (100-140 mg/m2). Any GVHD prophylaxis regimen was allowed at the discretion of the treating physician. Donors were 8/8 HLA-matched related or unrelated, or haploidentical. Stem cell sources were peripheral blood precursor cells or bone marrow grafts. Patients with a history of inflammatory bowel disease, delayed gastric emptying syndrome, or active gastrointestinal infection were excluded from the trial. In addition, patients who developed acute GI GVHD after HCT and before FMT administration were withdrawn from the trial out of concerns for safety. The decision to use prophylactic antibiotics during the peri-HCT period was at the discretion of the treating physician.
FMT capsule preparation
FMT donors were healthy, nonpregnant adults between the ages of 18 and 50 years. Donors had a normal body mass index (19-25 kg/m2) and did not take any medications on a regular basis; oral contraceptives were allowed. Volunteers were excluded for any significant medical history, employment as a healthcare worker, travel outside the United States, or use of antibiotics in the preceding 6 months. Candidates passed the American Association of Blood Banks donor questionnaire, physical examination, and general laboratory screening tests. Screening tests performed on donor blood and stool are listed in supplemental Table 1. All tests were within normal ranges or negative for all infectious screening tests (including cytomegalovirus), and the specified virologic screens were repeated after donation before samples were used. A fecal suspension was prepared in normal saline without preservatives, using a commercial blender in ambient air, and sequentially sieved to remove particulates. The final slurry was concentrated by centrifugation and resuspended in saline at one-tenth the volume of the initial sample, with 20% glycerol added as a bacterial cryoprotectant. The final fecal microbial solution was pipetted into size 0 capsules (650 μL) that were closed and then secondarily sealed in size 00 capsules (DR Capsules; Capsugel, Greenwood, SC). Capsules were stored frozen at −80°C (−112°F). Capsules were transported to the clinic or bedside on dry ice. Thirty capsules contained the microbial content of a median 38.6 g of feces (range, 24-56.7 g). In this study, FMT capsules were generated from 2 individual FMT donors, with patients receiving capsules from a single donor.
FMT capsule administration and specimen collection
The study schema is shown in Figure 1. FMT was administered no later than 4 weeks after neutrophil engraftment, and antibiotics were not allowed in the 48 hours before FMT. Patients were given a single standard dose of oral FMT, based on our published work for treatment of recurrent C difficile colitis, which is 15 capsules per day for 2 consecutive days, for a total of 30 capsules.9-11 The capsules were administered each day at an outpatient clinic visit. Participants fasted for 4 hours before and 1 hour after capsule intake. Patients had up to 4 hours to swallow the capsules. Capsules could not be crushed, chewed, or dissolved. Stool and urine samples were collected before HCT, 1 week post-HCT, and at 5 points after the FMT administration (1 week, 1 month, 2 months, 6 months, and 12 months). Urine specimens were aliquoted in cryogenic vials and stored at −80°C until time of sample analysis. For bacterial analysis of stool specimens, 95% ethanol solution was added to stool samples in a 1:1 wt/vol ratio and mixed and stored at −80°C until sequencing analysis.
Figure 1.

Study schema.
Analysis of urinary 3-IS
Analysis of the tryptophan metabolite 3-indoxyl sulfate (3-IS) was performed by reverse-phase liquid chromatography-electrospray ionization-tandem mass spectrometry in negative ion multiple reaction monitoring mode, as previously described.12,13 Obtained concentration values were corrected to urinary creatinine.
Analysis of stool specimens
Genomic 16S ribosomal sequencing was performed on stool specimens, as previously described.5,14 Briefly, genomic bacterial DNA was extracted from fecal specimens, and the 16S ribosomal-RNA V4-V5 variable region was amplified and sequenced on the Illumina MiSeq platform.4,5 VSEARCH was used for analyzing nucleotide sequences.15 Paired-end reads were merged, de-replicated, and sorted by length and size. For analyses of bacterial origin, sequences were error-corrected and chimera-filtered, using the UNOISE algorithm (http://www.biorxiv.org/content/early/2016/10/15/081257) to generate a preliminary list of operational taxonomic units (OTUs). For analyses of Clostridiales abundance and diversity as measured by inverse Simpson diversity index, an internally developed closed-reference OTU reference was used to classify sequences, and taxonomy was assigned in QIIME,16 using the Mothur method17 and the August 2013 release of the Greengenes reference taxonomy.18 An OTU table was generated using VSEARCH, and UniFrac19 distances between samples were determined with QIIME. For assessment of the inverse Simpson diversity score, sample sequences were first rarefied at a number below the sample, with the least number of sequences (n = 1152) using QIIME. All sequencing files and our internal OTU reference will be made available in the European Nucleotide Archive.
Data collection and management
Study data were collected and managed using REDCap electronic data capture tools hosted by Partners HealthCare Research Computing, Enterprise Research Infrastructure & Services group. REDCap is a secure, web-based application designed to support data capture for research studies.20
Subset analysis and comparison cohort with patients not receiving FMT
An exploratory subset analysis was performed to identify a group of patients that may benefit most from FMT after HCT based on exposure to broad-spectrum antibiotics. As this was a pilot study primarily aimed at establishing feasibility and safety of FMT in allogeneic HCT recipients, no control group was incorporated into the study design. In an exploratory analysis of the association of FMT with changes in microbiome diversity in this subgroup compared with what occurs in the absence of FMT, a comparison cohort of patients who did not receive FMT was retrospectively assembled. The patients in this comparison cohort were treated at Memorial Sloan Kettering Cancer Center or Duke University Medical Center and had stool specimens collected after allo-HCT as part of observational studies. The selection of patients for this cohort was based on broad-spectrum antibiotic exposure during HCT hospitalization, as well as availability of stool samples for sequencing analysis. Stool specimens from patients in the comparison cohort were analyzed according to the same methods listed here.
Statistical methods
This was an open-label, single-arm, pilot study evaluating FMT administered after allogeneic HCT to 13 adult patients. The primary endpoint of the study was feasibility, which was evaluated by the proportion of patients who were eligible for FMT administration and who were able to swallow 15 or more capsules (of 30). FMT was considered feasible if this proportion was 80% or higher and not feasible if it was 50% or lower. Secondary endpoints included cumulative incidence of bloodstream infections, C difficile colitis, and acute GVHD, as well as estimates for nonrelapse mortality, progression-free survival, and overall survival (OS). Progression-free survival and OS were estimated using the Kaplan-Meier method. Progression-free survival was calculated from the date of FMT administration to disease progression or death from any cause. Patients who were alive without relapse or progression were censored at the time of last clinical evaluation. OS was calculated from the date of FMT administration to death or censored at last clinical evaluation. The cumulative incidence of nonrelapse mortality was estimated with relapse as a competing risk. Comparisons of microbiome parameters (urinary 3-IS, Clostridiales abundance, inverse Simpson diversity index, UniFrac distance) were performed using the Mann-Whitney U test.
Results
Patient characteristics
Eighteen patients were enrolled on the study before admission for HCT. Five patients did not receive FMT because of the development of early acute GI GVHD before FMT (n = 3), patient withdrawal of consent before HCT (n = 1), and prolonged chemotherapy-associated gastrointestinal toxicity (n = 1; Figure 2). Baseline patient and transplant characteristics of the 13 patients who received FMT are shown in Table 1. The median age was 63 years (range, 26-71 years). Of those given FMT, 7 were female and 6 were male. The most common underlying diagnoses were acute myeloid leukemia (n = 4), myelodysplastic syndrome (n = 3), and non-Hodgkin lymphoma (n = 3). Donors included matched unrelated (n = 9), matched related (n = 2), and haploidentical (n = 2). Twelve patients received peripheral blood precursor cells, and 1 patient received a bone marrow graft. Ten patients received reduced-toxicity conditioning with fludarabine and melphalan, and 3 received conventional myeloablative regimens. GVHD prophylaxis regimens included tacrolimus/sirolimus (n = 9), tacrolimus/methotrexate (n = 2), and posttransplant cyclophosphamide with tacrolimus/mycophenolate mofetil for the 2 haploidentical transplants. Antibiotic exposures beginning at the time of HCT hospitalization through day +60 are summarized in supplemental Table 2.
Figure 2.

Study flow diagram. IBD, inflammatory bowel disease.
Table 1.
Baseline characteristics
| Characteristic | Value |
|---|---|
| Median age (range), y | 63 (26-71) |
| Sex, female/male, n | 7/6 |
| Diagnosis, n | |
| Acute myeloid leukemia | 4 |
| Myelodysplastic syndrome | 3 |
| Non-Hodgkin lymphoma | 3 |
| Myeloproliferative disorder | 1 |
| Chronic lymphocytic leukemia | 1 |
| Myelofibrosis | 1 |
| Graft source, n | |
| Peripheral blood stem cells | 12 |
| Bone marrow | 1 |
| Donor, n | |
| Matched unrelated | 9 |
| Matched related | 2 |
| Haploidentical | 2 |
| Conditioning, n | |
| Reduced intensity | 10 |
| Myeloablative | 3 |
| GVHD prophylaxis, n | |
| Tacrolimus/sirolimus | 9 |
| Tacrolimus/methotrexate | 2 |
| Posttransplant cyclophosphamide plus tacrolimus/mycophenolate mofetil | 2 |
Safety and toxicity
Fourteen patients were deemed eligible for evaluation of the feasibility endpoint: the 13 patients who received FMT and the single patient with prolonged chemotherapy-related gastrointestinal toxicity. All thirteen patients who received FMT capsules were able to swallow all 30 capsules (15 capsules/day for 2 consecutive days). Patients swallowed the daily allotment of capsules within 30 minutes. Thus, the primary endpoint of the study was met, as 13 (93%) of 14 patients eligible to receive FMT were able to take 15 or more of 30 capsules. There was only 1 serious treatment-related adverse event (grade 3 abdominal pain), and this resolved within 24 hours of capsule administration. There was no treatment-related nausea, vomiting, or diarrhea reported.
Clinical outcomes
Clinical outcomes are summarized in Table 2. FMT capsules were administered at a median of 27 days (range, 19-45 days) after HCT. Median follow-up for survivors is 15 months (range, 13-20 months). Two patients developed grade 3-4 acute GI GVHD subsequent to FMT. One case of severe GI GVHD occurred 20 days after FMT in a patient who had to prematurely discontinue tacrolimus after developing posterior reversible encephalopathy syndrome. The patient also developed Klebsiella pneumoniae bacteremia and sepsis, with subsequent multiorgan failure. In the second, skin manifestations of GVHD were noted 7 days after FMT, with the onset of GI involvement weeks later. There were no additional cases of bacteremia after FMT. There was 1 case of C difficile colitis observed after FMT. Six patients have developed moderate-severe chronic GVHD. The Kaplan-Meier estimates for 12-month OS and progression-free survival after FMT were 85% (95% confidence interval, 51%-96%) and 85% (95% confidence interval, 51%-96%), respectively. There was 1 nonrelapse death, which was a result of acute GI GVHD (12-month nonrelapse mortality, 8%; 95% confidence interval, 0%-30%).
Table 2.
Clinical outcomes
| Outcome | Value |
|---|---|
| Patients receiving FMT, n | 13 |
| Median time from allo-HCT to FMT (range), d | 27 (19-45) |
| Median follow-up (range), mo | 15 (13-20) |
| C difficile colitis, n | 1 |
| Bacteremia, n | 1 |
| Grade 3-4 acute GVHD, n | 2 |
| Deaths, n | 2 |
Correlative analysis of serial stool and urine specimens
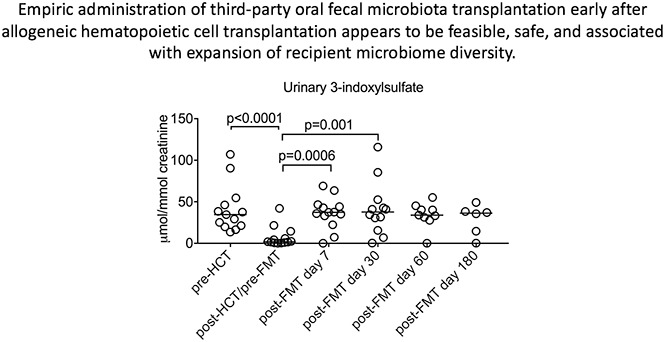
Low urinary concentrations of 3-IS after HCT are indicative of significant and clinically relevant intestinal microbiota disruption.13 A significant decrease in the median urinary 3-IS level was noted when comparing the pre-HCT with the post-HCT/pre-FMT specimen (34.59 umol/mmol creatinine vs 4.36; P ≤ .0001; Figure 3). Furthermore, there were significant increases in 3-IS in the urinary specimens collected 1 week (4.36 vs 36.57; P = .0006) and 1 month (4.36 vs 40.89; P = .001) after FMT when compared with the post-HCT/pre-FMT specimen.
Figure 3.

Longitudinal changes in urinary 3-IS levels before allo-HCT and after FMT administration in the early posttransplant period.
There was no statistically significant change in the intestinal microbiome α-diversity between the pre-HCT specimens and the post-HCT/pre-FMT or post-FMT specimens, as measured by the inverse Simpson index (Figure 4A). A significant decrease in Clostridiales abundance was observed when comparing the pre-HCT with the post-HCT/pre-FMT stool specimen, which corrected after FMT (Figure 4B). UniFrac distance analysis showed a more similar microbiome in patients when compared with their FMT donor after the administration of FMT than before FMT (Figure 4C). To assess engraftment of the FMT product, OTU origins were classified as being initially identified in the FMT donor sample only, in the patient pre-FMT samples only, both, or neither. Expansion of FMT donor-only OTUs was clearly observed in recipients after administration of FMT (Figure 4D).
Figure 4.

Evaluation of the microbiome prior to and following administration of FMT. Longitudinal changes in (A) inverse Simpson index, (B) Clostridiales abundance, and (C) UniFrac distance before allo-HCT and after FMT administration in the early posttransplant period, as determined from 16S rRNA sequencing of stool specimens. (D) Longitudinal changes in the origin of operational taxonomic units. Four selected patients shown.
Subset analysis and comparison cohort with patients not receiving FMT
According to the known association between antibiotic exposure and reduced microbiome diversity,21 we identified 8 patients who both received broad-spectrum antibiotics (not including ciprofloxacin prophylaxis) during HCT hospitalization before FMT and, thus, likely experienced an initial microbiota injury, and did not receive broad-spectrum antibiotics after FMT, which we hypothesized would increase the likelihood of durable engraftment of the FMT. This subset of patients experienced more significant increases in microbiome diversity, as measured by urinary 3-IS, inverse Simpson index, Clostridiales abundance, and shorter UniFrac distance from the FMT donor (Figure 5). For a comparison cohort, we identified 32 patients from 2 other institutions who received broad-spectrum antibiotic exposure during their HCT hospitalization and had available 16S-sequenced stool samples, but who did not receive an FMT. As the median time of FMT administration was 27 days after HCT (range, 19-45 days), we chose stool samples collected at points days 25-40 and days 50-70 after HCT for the control cohort to compare with the 1-week and 1-month post-FMT samples. In this unplanned post hoc analysis, patients who received FMT on this study had significantly improved intestinal microbiome diversity, as measured by the inverse Simpson index (Figure 6).
Figure 5.

Microbiome assessment under conditions that highlight the potential benefit of FMT as part of an exploratory analysis in a subset of 8 patients. Eligibility criteria for inclusion in this subset analysis received microbiome-disrupting antibiotics (ceftazidime, cefepime, piperacillin-tazobactam, meropenem, oral vancomycin, or metronidazole) before FMT, and did not receive microbiome-disrupting antibiotics in the 60 days after FMT.
Figure 6.

Microbiome diversity after FMT compared with a post hoc comparison cohort of patients with allo-HCT who did not receive FMT. The inverse Simpson scores of 8 FMT recipients from Figure 5 are compared with those of patients who underwent allo-HCT at 2 other institutions and had stool specimens collected and 16S sequenced in a manner identical to those from FMT recipients.
Discussion
This pilot study is the first to explore the empiric administration of frozen third-party oral FMT capsules to patients early after allo-HCT to reconstitute microbiome diversity. We found that third-party FMT was safe and feasible when given in the period immediately after neutrophil engraftment. The primary endpoint of the study, feasibility of oral FMT early after allo-HCT, was met. We also found the approach to be safe, as patients experienced minimal toxicity and a low incidence of infectious complications. We did not observe transmission of infectious organisms from FMT capsules. There was a single case of bacteremia after administration of FMT, which occurred in the setting of active GI GVHD. We are encouraged by the safety and feasibility demonstrated, as there are multiple advantages to oral third-party FMT capsules, including noninvasive administration, centralized screening of donors and preparation of an FMT product, and the ability to treat many patients from a few healthy donors. This formulation and route of administration are perhaps more readily scaled up to multicenter studies than a liquid FMT preparation collected freshly and delivered via nasogastric intubation, enema, or endoscopically.
Our results also represent the first outside validation of urinary 3-IS, a tryptophan-derived metabolite produced by commensal bacteria, as a biomarker for microbiome diversity in allo-HCT patients. The patients in this study exhibited an expected decrease in microbial diversity while undergoing HCT, as predicted by the biomarker urinary 3-IS concentration, although this change was not statistically significant when assessed directly by 16S sequencing and the inverse Simpson index. The reason for this may be that urinary 3-IS concentration and stool 16S-based diversity measurements each detect different, and perhaps overlapping, patterns of microbiota injury. The administration of FMT in this study was associated with maintenance or recovery of intestinal microbiome diversity, as indicated by urinary 3-IS levels and 16S ribosomal sequencing of stool specimens, which could be observed as early as 1 week after FMT. Furthermore, there was clear expansion of donor-specific OTUs, suggesting that the recovery of microbiome diversity was directly attributable to the FMT. Previous studies have identified Clostridiales as a commensal anaerobe with an important role in intestinal homeostasis, and its loss during allo-HCT has been associated with increased transplant-related mortality.4,22 The increase in Clostridiales abundance after FMT is consistent with the other measures of microbiome health. We also retrospectively identified a subset of patients in this study who received broad-spectrum antibiotics during HCT hospitalization who appear to have attained the largest gains in terms of microbiome diversity after FMT. When compared with a post hoc cohort of allo-HCT patients from other institutions with similar antibiotic exposures but who did receive FMT, patients who received FMT had significantly improved intestinal microbiome diversity. Clearly, these comparisons must be interpreted with caution, given the differences between institutional clinical practices and the limitations of retrospective analyses. Nevertheless, taken together with the expansion of donor-specific taxa we observed, these results are consistent with the notion that the improvements in microbiome diversity in this study can be, in part, attributed to the FMT.
The loss of intestinal microbial diversity has recently been associated with adverse outcomes in recipients after allo-HCT. Reduced diversity of the intestinal microbiome within the first 7 days after neutrophil engraftment, as measured by 16S rRNA sequencing and defined by the inverse Simpson index, has been correlated with significantly worse survival outcomes (OS at 3 years was 36%, 60%, and 67% for low-, intermediate-, and high-diversity groups, respectively (P = .019).4 Similarly, low levels of urinary 3-IS in the first 10 days after allo-HCT have been associated with higher transplant-related mortality (P = .017) and worse OS (P = .05), with the majority of TRM being related to acute GI GVHD (86.4%; P < .001).13 Subsequent studies have explored associations between the intestinal microbiome with acute GVHD and disease relapse. One analysis showed that increased bacterial diversity after allo-HCT was associated with reduced acute GVHD-related mortality, and that increased amounts of bacteria specifically belonging to the genus Blautia were associated with reduced acute GVHD mortality.5 In a second study, acute GVHD was associated with lower α diversity of stool microbiota, with the presence of oral Actinobacteria and oral Firmicutes in stool at neutrophil recovery after allo-HCT being positively correlated with subsequent acute GVHD.23 Finally, a link between disease relapse after allo-HCT and the changes in the amount of specific bacteria in the intestinal flora has been demonstrated, notably with higher Eubacterium limosum abundance being associated with a decreased risk for relapse.6
It remains unknown whether interventions designed to modify the microbiome can affect clinical HCT outcomes, but numerous initial investigations are underway. Early administration of broad-spectrum antibiotic therapy is associated with significantly altered microbiota (reflected by suppression of urinary 3-IS levels), higher TRM, and worse OS when compared with patients with late or no antibiotic exposure.13,21 It has been hypothesized that commensal anaerobic organisms, such as Clostridiales, help maintain and restore microbiota diversity, and that the use of anaerobe-sparing antibiotics may benefit patients.21,24 Indeed, multiple prospective clinical trials are evaluating the effect of choice of antibiotic prophylaxis or empiric therapy for neutropenic fever on the intestinal microbiome during allo-HCT (NCT02641236, NCT03078010). In addition, the use of certain prebiotics and probiotics are being explored as possible approaches to prevent microbiota dysbiosis.25 Murine models have identified microbiome-derived metabolites, which may mitigate GI toxicity and GVHD, although clinical investigations in humans have not yet been reported.26,27 An ongoing pilot study is investigating the administration of fructooligosaccharides, a prebiotic with known ability to alter butyrate-producing bacteria,28 to patients undergoing allo-HCT (NCT02805075). In addition, there is a planned randomized clinical trial to study the role of Lactobacillus in preventing acute GI GVHD in pediatric recipients of HCT (NCT03057054). Exposure to the hospital environment may also have an effect on the intestinal microbiome, and it has been recently shown that patients who received care after transplant at home had similar outcomes to matched hospital controls, with a noted lower incidence of grade 2-4 acute GVHD.29 An ongoing study will evaluate changes in the intestinal microbiota for patients who receive HCT at home, as compared with those treated in the clinic or hospital (NCT01725022).
Previous investigations of FMT in HCT recipients have focused mainly on the treatment of antibiotic-resistant bacteria and C difficile infection.30-33 A prospective single-center study in patients with blood disorders, which included HCT recipients, suggested that FMT can eradicate antibiotic-resistant bacteria from the GI tract of recipients.34 A randomized trial of empiric autologous FMT to prevent C difficile infection in allo-HCT recipients is now ongoing (NCT02269150). Interestingly, 2 recent preliminary reports have suggested a possible role for FMT as treatment of steroid-refractory acute GI GVHD.35,36 These interventional studies, as well as the associations of low intestinal microbial diversity with the risk for infectious complications, acute GVHD, and TRM, suggest that microbiome restoration early after allo-HCT may be of benefit. Here, we show that frozen third-party FMT capsules allow for an easily accessible, noninvasive approach that is well tolerated in the early post-HCT period and can potentially hasten the recovery of microbiome diversity.
Limitations of this study include primarily the small sample size. A pilot safety and feasibility study was necessary, given that participants were receiving donor live bacteria in the immediate post-HCT period. This design inherently limits our ability to draw any conclusions about whether microbial manipulation by FMT directly influenced patient outcomes, as that requires a larger study with incorporation of a proper control group. In addition, given safety concerns about the risk for FMT-related bacteremia, we excluded patients with acute GI GVHD, as active inflammation compromises the integrity of the intestinal barrier. Given our data associating FMT with restoration of microbial diversity, and preliminary reports of the therapeutic effect of FMT in patients with steroid-resistant aGVHD,35,36 additional studies should be designed to investigate the effect of FMT on clinical outcomes after allo-HCT, including acute GVHD and infectious complications.
Further prospective evaluations into the use of FMT in patients undergoing allogeneic HCT are needed to better understand its effects on the recipient microbiome and to better characterize its influence on clinical outcomes. Given the limited size of current clinical studies, microbiome diversity-associated correlative endpoints seem most appropriate. However, a larger prospective trial with a clinical primary endpoint will eventually be required to ultimately determine whether microbiome diversity manipulation can truly have an effect on patient outcomes after allo-HCT.
Supplementary Material
The full-text version of this article contains a data supplement.
Acknowledgments
The authors thank the patient and donor volunteers.
This work was supported by the National Institutes of Health, National Institute of Allergy and Infectious Diseases (5K08AI110655) (M.K.M.), National Center for Advancing Translational Sciences (5KL2TR001115-03) (A.D.S.), National Heart, Lung, and Blood Institute (R01 HL124112 [R.R.J.] and 1R01HL123340-01A1), and National Cancer Institute (P01-CA023766 [M.R.M.v.d.B.] and P30 CA008748). This work also was supported by the Jose Carreras Leukaemia Foundation (E. Holler and G.L.), the Cancer Prevention and Research Institute of Texas Recruitment of Rising Stars (R.R.J.), The Lymphoma Foundation, The Susan and Peter Solomon Divisional Genomics Program, and the Parker Institute for Cancer Immunotherapy at Memorial Sloan Kettering Cancer Center.
Authorship
Contribution: S.L., M.K.M., E. Hohmann, and Y.-B.C. designed the study; Z. DeFilipp, C.D.R., B.V., M.E.K., M.S., J.B., B.R.D., A.E.-J., S.L.M., T.R.S., K.K.B., and Y.-B.C. recruited patients to the study and collected clinical data; J.M. and E. Hohmann prepared the FMT capsules; J.U.P., Z. Dagher, A.E.S., K.D., G.L., P.O., E. Holler, M.K.M., M.R.M.v.d.B., and R.R.J., contributed to the analysis of stool and urine specimens; J.U.P., A.D.S., T.E.D., J.A.M., Y.T., E.G.P., M.R.M.v.d.B., and R.R.J. contributed to the formation of the control cohort; Z. DeFilipp, S.L., E. Holler, M.K.M., E. Hohmann, R.R.J., and Y.-B.C. analyzed the data; Z. DeFilipp and Y.-B.C. wrote the manuscript; and all authors approved the final of the manuscript and submission of the manuscript.
Conflict-of-interest disclosure: E. Hohmann receives research support from Seres Therapeutics, Inc. J.U.P. holds patents with or receives royalties from Seres Therapeutics, Inc. R.R.J. is on the board of directors or an advisory committee for Seres Therapeutics, Inc., has consulted for Ziopharm Oncology, and holds patents with or receives royalties from Seres Therapeutics, Inc. M.R.M.v.d.B. is on the board of directors or an advisory committee for Seres Therapeutics, Inc. and holds patents with or receives royalties from Seres Therapeutics, Inc. E.G.P. is on the board of directors or an advisory committee for Seres Therapeutics, Inc. and holds patents with or receives royalties from Seres Therapeutics, Inc. The remaining authors declare no competing financial interests.
Correspondence: Yi-Bin Chen, Blood and Marrow Transplant Program Massachusetts General Hospital, 55 Fruit St, Yawkey 9E-9052, Boston, MA 02114; e-mail: ychen6@partners.org.
References
- 1.Peled JU, Hanash AM, Jenq RR. Role of the intestinal mucosa in acute gastrointestinal GVHD. Blood. 2016;128(20):2395-2402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Staffas A, Burgos da Silva M, van den Brink MR. The intestinal microbiota in allogeneic hematopoietic cell transplant and graft-versus-host disease. Blood. 2017;129(8):927-933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mathewson ND, Reddy P. The microbiome and graft versus host disease. Curr Stem Cell Rep. 2015;1(1):39-47 [Google Scholar]
- 4.Taur Y, Jenq RR, Perales MA, et al. The effects of intestinal tract bacterial diversity on mortality following allogeneic hematopoietic stem cell transplantation. Blood. 2014;124(7):1174-1182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jenq RR, Taur Y, Devlin SM, et al. Intestinal blautia is associated with reduced death from graft-versus-host disease. Biol Blood Marrow Transplant. 2015;21(8):1373-1383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Peled JU, Devlin SM, Staffas A, et al. Intestinal microbiota and relapse after hematopoietic-cell transplantation. J Clin Oncol. 2017;35(15):1650-1659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kassam Z, Lee CH, Yuan Y, Hunt RH. Fecal microbiota transplantation for Clostridium difficile infection: systematic review and meta-analysis. Am J Gastroenterol. 2013;108(4):500-508. [DOI] [PubMed] [Google Scholar]
- 8.van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med. 2013;368(5):407-415. [DOI] [PubMed] [Google Scholar]
- 9.Youngster I, Sauk J, Pindar C, et al. Fecal microbiota transplant for relapsing Clostridium difficile infection using a frozen inoculum from unrelated donors: a randomized, open-label, controlled pilot study. Clin Infect Dis. 2014;58(11):1515-1522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Youngster I, Russell GH, Pindar C, Ziv-Baran T, Sauk J, Hohmann EL. Oral, capsulized, frozen fecal microbiota transplantation for relapsing Clostridium difficile infection. JAMA. 2014;312(17):1772-1778. [DOI] [PubMed] [Google Scholar]
- 11.Youngster I, Mahabamunuge J, Systrom HK, et al. Oral, frozen fecal microbiota transplant (FMT) capsules for recurrent Clostridium difficile infection. BMC Med. 2016;14(1):134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhu W, Stevens AP, Dettmer K, et al. Quantitative profiling of tryptophan metabolites in serum, urine, and cell culture supernatants by liquid chromatography-tandem mass spectrometry. Anal Bioanal Chem. 2011;401(10):3249-3261. [DOI] [PubMed] [Google Scholar]
- 13.Weber D, Oefner PJ, Hiergeist A, et al. Low urinary indoxyl sulfate levels early after transplantation reflect a disrupted microbiome and are associated with poor outcome. Blood. 2015;126(14):1723-1728. [DOI] [PubMed] [Google Scholar]
- 14.Taur Y, Xavier JB, Lipuma L, et al. Intestinal domination and the risk of bacteremia in patients undergoing allogeneic hematopoietic stem cell transplantation. Clin Infect Dis. 2012;55(7):905-914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rognes T, Flouri T, Nichols B, Quince C, Mahé F. VSEARCH: a versatile open source tool for metagenomics. PeerJ. 2016;4:e2584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Caporaso JG, Kuczynski J, Stombaugh J, et al. QIIME allows analysis of high-throughput community sequencing data. Nat Methods. 2010;7(5):335-336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Schloss PD, Westcott SL, Ryabin T, et al. Introducing mothur: open-source, platform-independent, community-supported software for describing and comparing microbial communities. Appl Environ Microbiol. 2009;75(23):7537-7541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Werner JJ, Koren O, Hugenholtz P, et al. Impact of training sets on classification of high-throughput bacterial 16s rRNA gene surveys. ISME J. 2012;6(1):94-103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wong RG, Wu JR, Gloor GB. Expanding the UniFrac Toolbox. PLoS One. 2016;11(9):e0161196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Weber D, Jenq RR, Peled JU, et al. Microbiota disruption induced by early use of broad-spectrum antibiotics is an independent risk factor of outcome after allogeneic stem cell transplantation. Biol Blood Marrow Transplant. 2017;23(5):845-852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jenq RR, Ubeda C, Taur Y, et al. Regulation of intestinal inflammation by microbiota following allogeneic bone marrow transplantation. J Exp Med. 2012;209(5):903-911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Golob JL, Pergam SA, Srinivasan S, et al. Stool microbiota at neutrophil recovery is predictive for severe acute graft vs host disease after hematopoietic cell transplantation. Clin Infect Dis. 2017;65(12):1984-1991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Shono Y, van den Brink M. Empiric antibiotic use in allogeneic hematopoietic cell transplantation: should we avoid anaerobe coverage? Blood Adv. 2017;1(25):2325-2328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Andermann TM, Rezvani A, Bhatt AS. Microbiota manipulation with prebiotics and probiotics in patients undergoing stem cell transplantation. Curr Hematol Malig Rep. 2016;11(1):19-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mathewson ND, Jenq R, Mathew AV, et al. Gut microbiome-derived metabolites modulate intestinal epithelial cell damage and mitigate graft-versus-host disease. Nat Immunol. 2016;17(5):505-513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Waller EK, Giver CR, Rangaraju S, et al. Administation of a tryptophane metabolite, indole-3-carboxaldehyde, reduces graft versus host disease morbidity and mortality and enhances gastrointestinal barrier function in a murine model of allogeneic bone marrow transplantation. Blood. 2014;124:2420. [Google Scholar]
- 28.Liu F, Li P, Chen M, et al. Fructooligosaccharide (FOS) and galactooligosaccharide (GOS) increase bifidobacterium but reduce butyrate producing bacteria with adverse glycemic metabolism in healthy young population. Sci Rep. 2017;7(1):11789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ringdén O, Remberger M, Holmberg K, et al. Many days at home during neutropenia after allogeneic hematopoietic stem cell transplantation correlates with low incidence of acute graft-versus-host disease. Biol Blood Marrow Transplant. 2013;19(2):314-320. [DOI] [PubMed] [Google Scholar]
- 30.Neemann K, Eichele DD, Smith PW, Bociek R, Akhtari M, Freifeld A. Fecal microbiota transplantation for fulminant Clostridium difficile infection in an allogeneic stem cell transplant patient. Transpl Infect Dis. 2012;14(6):E161-E165. [DOI] [PubMed] [Google Scholar]
- 31.de Castro CG Jr, Ganc AJ, Ganc RL, Petrolli MS, Hamerschlack N. Fecal microbiota transplant after hematopoietic SCT: report of a successful case. Bone Marrow Transplant. 2015;50(1):145. [DOI] [PubMed] [Google Scholar]
- 32.Mittal C, Miller N, Meighani A, Hart BR, John A, Ramesh M. Fecal microbiota transplant for recurrent Clostridium difficile infection after peripheral autologous stem cell transplant for diffuse large B-cell lymphoma. Bone Marrow Transplant. 2015;50(7):1010. [DOI] [PubMed] [Google Scholar]
- 33.Falconer S, Moss E, Andermann T, et al. Fecal microbiota transplant is a potentially safe and effective treatment for Clostridium difficile infection in hematopoietic stem cell recipients. Biol Blood Marrow Transplant. 2016;22(3):S53-S54. [Google Scholar]
- 34.Bilinski J, Grzesiowski P, Sorensen N, et al. Fecal microbiota transplantation in patients with blood disorders inhibits gut colonization with antibiotic-resistant bacteria: results of a prospective, single-center study. Clin Infect Dis. 2017;65(3):364-370. [DOI] [PubMed] [Google Scholar]
- 35.Kakihana K, Fujioka Y, Suda W, et al. Fecal microbiota transplantation for patients with steroid-resistant acute graft-versus-host disease of the gut. Blood. 2016;128(16):2083-2088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Spindelboeck W, Schulz E, Uhl B, et al. Repeated fecal microbiota transplantations attenuate diarrhea and lead to sustained changes in the fecal microbiota in acute, refractory gastrointestinal graft-versus-host-disease. Haematologica. 2017;102(5):e210-e213. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.