

Abstract
Robot-assistance is increasingly used in surgical practice. We performed a nonsystematic literature review using PubMed/MEDLINE and Google for robotic surgical systems and compiled information on their current status. We also used this information to predict future about the direction of robotic systems based on various robotic systems currently being developed. Currently, various modifications are being made in the consoles, robotic arms, cameras, handles and instruments, and other specific functions (haptic feedback and eye tracking) that make up the robotic surgery system. In addition, research for automated surgery is actively being carried out. The development of future robots will be directed to decrease the number of incisions and improve precision. With the advent of artificial intelligence, a more practical form of robotic surgery system can be introduced and will ultimately lead to the development of automated robotic surgery system.
INTRODUCTION
Since the introduction of the da Vinci™ surgical system (Intuitive Surgical Inc., Mountain View, CA, USA), more sophisticated surgery has been achieved with improved three-dimensional (3D) visual acuity, 7 degrees of freedom, breakthrough accuracy, and accessibility to surgery. Robot-assisted laparoscopic radical prostatectomy was pioneered in 2001.[1] After the approval of the US Food and Drug Administration (FDA), four generations of the da Vinci system have been introduced over the past 17 years.[2,3,4,5] In 2016, da Vinci installations increased by more than 25%, mainly in urology and gynecology.[6] Several manufacturers are developing alternate robotic systems [Figure 1]. However, due to issues related to patents, clinical deployments are limited[7,8,9] Nevertheless, the era of robotic surgery is expected to rapidly evolve as new technologies become available soon. The aim of the present study is to provide a comprehensive overview of the current state of robotic surgery and to predict the future of the surgical robot system based on the current status.
Figure 1.

Revo-i: It consists of a surgeon control console, a four-arm robotic operation cart, a high-definition vision cart, and reusable endoscopic instruments
METHODOLOGY
A comprehensive literature review was performed using the PubMed electronic search engine. The following search terms were used: “da Vinci” (n = 4308), “robotic surgical system” (n = 2051), and “new robotic surgical device” (n = 760). The references of related papers were used, and the articles and information were searched by Google search engine (www.google.com).
da Vinci surgical system
According to ISRG's stock report,[10] Intuitive Surgical has maintained its market leader position for over 17 years. Historically, an updated model is launched approximately every 6 years [Figure 2]. Of the 3919 da Vinci systems installed worldwide at the end of 2016, 63% were in the US, 15% in Europe, 18% were in Asia, and 4% were in the rest of the world [Figure 3].
Figure 2.
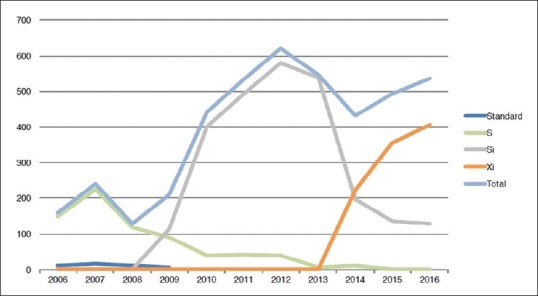
Installed systems by model of da Vinci series
Figure 3.
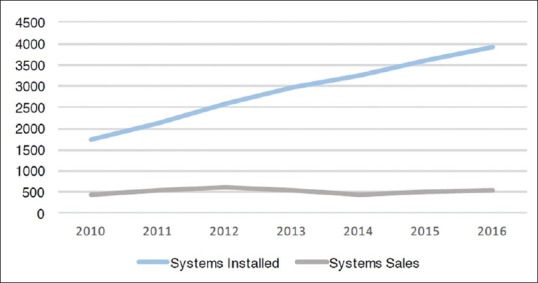
System growth of da Vinci series
Future of da Vinci
According to the Intuitive Surgical Investor Presentation in 2017,[11] they have focused on three aims for technical advances; first, “enhanced imaging” which can help surgeons and staff overcome the limitations of the human eye [Figure 4a]; second, “intelligent systems” which can provide to surgeons a real-time feedback [Figure 4b]; and third, “less invasive approaches to the body” [Figure 4c and d]. They are expected to launch da Vinci X surgical system which is optimized for focused-quadrant surgery for procedures and can incorporate da Vinci Xi endoscope technology, instruments, and accessories in 2017 [Figure 5]. The expected launch of the da Vinci SP will also ignite a new product update cycle [Figure 4d].
Figure 4.

(a) Enhanced imaging which can help surgeons and staff overcome the limitations of the human eye. (b) Intelligent systems which can provide to surgeons a real-time feedback. (c) Less invasive approaches to the body: da Vinci SP surgical system. (d) Less invasive approaches to the body: Flexible catheter-based system
Figure 5.

Da Vinci X surgical system: This system is optimized for focused-quadrant surgery for procedures
New surgical system on the Horizon
Revo-i
The Revo-i (Meere Company Inc., Yongin, Republic of Korea) consists of a surgeon control console, a four-arm robotic operation cart, a high-definition vision cart, and reusable endoscopic instruments [Figure 1]. The basic configuration and development of this model is designed to be similar to da Vinci systems. A preclinical study with porcine model was completed in 2016.[9] Moreover, the clinical trial in treating patients with radical cholecystectomy or prostatectomy was performed using this surgical system in 2017. The manufacturers obtained a commercialized approval of Korean FDA in August 2017 and new model of Revo-i® surgical system is expected to be launched.
Telelap ALF-X
The multiport surgical robotic ALF-X system (SORAR SpA, Milan, Italy) was initially introduced for gynecological surgery and was recently assessed in a preclinical animal study of robot-assisted partial nephrectomy[12,13] Fanfani et al. reported that they performed 80 cases of hysterectomy with ALF-X system for benign and malignant disease, from October 2013 to May 2014.[14] They also reported that they performed partial nephrectomy with ALF-X system on pig models.[12] Unlike the da Vinci system, each arm of this device can be positioned independently from the others on the surgical field. The system's unique features also include haptic feedback and an eye-tracking system. Haptic feedback is achieved by counter movements of the laparoscopic handle at the console according to force and direction applied at the tip of the instrument.[15] The eye-tracking system controls camera movements; for example, the image is zoomed in when the surgeon's head approaches the screen.[16]
Micro Hand S
This device consists of a surgeon console and a slave cart which is similar to the da Vinci surgical robot. The first clinical trials were reported in 2014 including one patient with gastric perforation and two patients with acute appendicitis.[17]
Upcoming robotic systems: ongoing projects
The Medrobotics® (Raynham, MA, USA) received the US FDA clearance for the Flex robotic system in July 2015. The Flex robotic system provides surgeons with single-site access visualization of hard-to-reach anatomical locations. Remacle et al.[18] reported the first surgical application of the Medrobotics Flex system on humans, by performing three procedures of transoral robotic surgery. Titan Medical (Toronto, ON, Canada), a public company, has developed the Single Port Orifice Robotic Technology (SPORT™ Surgical system). The system utilizes a 25 mm single-access port that contains two articulating instruments and a 3D high-definition camera. The Versius system (Cambridge Medical Robotics) has arms that are small and light enough to be moved around an operating table as a surgeon pleases. The arm, built like a human arm, has three joints, corresponding to the shoulder, the elbow and the wrist.
DISCUSSION
The da Vinci robotic surgical system developed by Intuitive Surgery for the past 17 years has dominated the robotic surgery market. The surgeons saw the image through the lens of the camera, and the operation was carried out according to the control performed at the console. The competing robot that has been developed does not seem to deviate much from the concept of the basic da Vinci robotic surgical system. However, they are continuing their efforts to evolve into a better surgical robot system than existing ones. For example, the da Vinci system provides excellent 3D visualization of the surgical site and improved dexterity, but it lacks haptic force feedback and subsurface tissue visualization. Laparoscopic or robotic surgery has the disadvantage of not having haptic sense, but this is overcome by the surgeon's experience, by looking at the tissue, whether it is hard or soft. Engineers are trying to introduce haptic technology into robot systems, but the technology is limited at this time. These limitations make the introduction more difficult.[19,20] There are also many reports of image guidance using navigation technologies and applying to neurosurgery or spinal surgery.[21,22] However, it is not yet applied to clinical urologic robot surgery.[23] In the closed console of da Vinci system, surgeon's situational awareness can be compromised. To overcome this disadvantage, there are some trials for using 3D glasses or 3D high-definition monitor[3,9,15] Rassweiler et al.[24] in the “Future of robotic surgery in urology” presented their prediction of the specific development and evolution of technology based on the current technology advances and patent status. For example, the first automobile has vastly evolved to the high tech ones we drive now a day. Furthermore, autonomous cars have recently been advertised and there is promise of an intelligent automobile that drives itself. As such, the robotic surgery system is expected to ultimately follow the automobile model and will evolve onto the automated surgery system. Technically speaking, automated surgery is no more difficult than automatic driving. Because there are no sudden emergency situations such as protruding vehicle or person during driving, once artificial intelligence (AI) acquires the anatomical understanding and the surgical technique, technically automated surgery can be performed. In addition, in more recent years, attempts to learn internal organs through deep learning have been published in various studies,[25] and there are reports that it is possible to learn in the initial stage. Furthermore, if videos of surgical procedures are taught, surgical techniques can be taught to AI, and related studies are underway. An automated surgical robot known as the Smart Tissue Autonomous Robot has proven to be capable of performing some surgical procedures on pigs, such as sewing tissue.[26,27] The machine operates on its own but is currently being used under designer's supervision. It is designed to perform work within a predictable range, rather than full-scale operations on its own, and is nearing availability for human testing. This machine showed to cut three pig's tissues (skin, fat, and muscle) which are attached markers along the markers automatically in 2017. They showed accurate resection lenses and could suggest that this could be beneficial in tumor resection. Currently, studies are underway to analyze surgeons’ performance using a tool of “dVLogger” and to predict efficiency.[28,29] Based on this, robots can facilitate the performance of surgeons and potentially result in less inadvertent complications and improved outcomes. In addition, the robots that have learned the videos of surgery performed by expert surgeons can also play a role of navigator. It can be used as a guide to the novice surgeon during surgery. However, not only technical barriers but also other barriers such as ethical dilemmas will become issues. Even if AI is technically feasible for surgery, safety must be ensured should any unexpected or inadvertent problem arise. Since it is not possible to conduct experiments on humans without extra cautionary measures, priority will be given to application to animals. However, the question of whether the patient will accept it is another matter. We are on the verge of preparing a second-generation robotic surgery system. This will be the time when not only technical issues but also social issues need to be coordinated and addressed. Obviously, the robotic surgery system will continue to evolve and the surgeon will have to continue to adapt.
CONCLUSIONS
In the near future, robots will be developed in a way that the number of incisions is less with high precision. A more efficient system will be introduced with greater applicability with more diverse devices while ensuring patient safety. With the advent of AI between the robotic system and the surgeon, a more efficiently functional form of robotic surgery system could be introduced and ultimately the development type will go to an automated robot surgery system.
Footnotes
Financial support and sponsorship: Nil.
Conflicts of interest: There are no conflicts of interest.
REFERENCES
- 1.Abbou CC, Hoznek A, Salomon L, Olsson LE, Lobontiu A, Saint F, et al. Laparoscopic radical prostatectomy with a remote controlled robot. J Urol. 2001;165:1964–6. doi: 10.1097/00005392-200106000-00027. [DOI] [PubMed] [Google Scholar]
- 2.Rao R, Nayyar R, Panda S, Hemal AK. Surgical techniques: Robotic bladder diverticulectomy with the da Vinci-S surgical system. J Robot Surg. 2007;1:217–20. doi: 10.1007/s11701-007-0030-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kang SW, Lee SC, Lee SH, Lee KY, Jeong JJ, Lee YS, et al. Robotic thyroid surgery using a gasless, transaxillary approach and the da Vinci S system: The operative outcomes of 338 consecutive patients. Surgery. 2009;146:1048–55. doi: 10.1016/j.surg.2009.09.007. [DOI] [PubMed] [Google Scholar]
- 4.Tobis S, Knopf J, Silvers C, Yao J, Rashid H, Wu G, et al. Near infrared fluorescence imaging with robotic assisted laparoscopic partial nephrectomy: Initial clinical experience for renal cortical tumors. J Urol. 2011;186:47–52. doi: 10.1016/j.juro.2011.02.2701. [DOI] [PubMed] [Google Scholar]
- 5.Kaouk JH, Haber GP, Autorino R, Crouzet S, Ouzzane A, Flamand V, et al. A novel robotic system for single-port urologic surgery: First clinical investigation. Eur Urol. 2014;66:1033–43. doi: 10.1016/j.eururo.2014.06.039. [DOI] [PubMed] [Google Scholar]
- 6.Leal Ghezzi T, Campos Corleta O. 30 years of robotic surgery. World J Surg. 2016;40:2550–7. doi: 10.1007/s00268-016-3543-9. [DOI] [PubMed] [Google Scholar]
- 7.Falavolti C, Gidaro S, Ruiz E, Altobelli E, Stark M, Ravasio G, et al. Experimental nephrectomies using a novel telesurgical system: (The telelap ALF-X)-A pilot study. Surg Technol Int. 2014;25:37–41. [PubMed] [Google Scholar]
- 8.Kim DK, Park DW, Rha KH. Robot-assisted partial nephrectomy with the REVO-I robot platform in porcine models. Eur Urol. 2016;69:541–2. doi: 10.1016/j.eururo.2015.11.024. [DOI] [PubMed] [Google Scholar]
- 9.Abdel Raheem A, Troya IS, Kim DK, Kim SH, Won PD, Joon PS, et al. Robot-assisted fallopian tube transection and anastomosis using the new REVO-I robotic surgical system: Feasibility in a chronic porcine model. BJU Int. 2016;118:604–9. doi: 10.1111/bju.13517. [DOI] [PubMed] [Google Scholar]
- 10. [Last accessed on 2018 Mar 12]. Available from: http://www.usf.edu/business/documents/departments/finance/smif/analysis-intuitive-surgical.pdf .
- 11. [Last accessed on 2018 Mar 12]. Available from: http://phx.corporate.ir.net/phoenix.zhtml?c=122359&p=irol-irhome .
- 12.Bozzini G, Gidaro S, Taverna G. Robot-assisted laparoscopic partial nephrectomy with the ALF-X robot on pig models. Eur Urol. 2016;69:376–7. doi: 10.1016/j.eururo.2015.08.031. [DOI] [PubMed] [Google Scholar]
- 13.Fanfani F, Monterossi G, Fagotti A, Rossitto C, Gueli Alletti S, Costantini B, et al. The new robotic TELELAP ALF-X in gynecological surgery: Single-center experience. Surg Endosc. 2016;30:215–21. doi: 10.1007/s00464-015-4187-9. [DOI] [PubMed] [Google Scholar]
- 14.Fanfani F, Restaino S, Gueli Alletti S, Fagotti A, Monterossi G, Rossitto C, et al. TELELAP ALF-X robotic-assisted laparoscopic hysterectomy: Feasibility and perioperative outcomes. J Minim Invasive Gynecol. 2015;22:1011–7. doi: 10.1016/j.jmig.2015.05.004. [DOI] [PubMed] [Google Scholar]
- 15.Gidaro S, Buscarini M, Ruiz E, Stark M, Labruzzo A. Telelap alf-X: A novel telesurgical system for the 21st century. Surg Technol Int. 2012;22:20–5. [PubMed] [Google Scholar]
- 16.Gidaro S, Altobelli E, Falavolti C, Bove AM, Ruiz EM, Stark M, et al. Vesicourethral anastomosis using a novel telesurgical system with haptic sensation, the telelap alf-X: A pilot study. Surg Technol Int. 2014;24:35–40. [PubMed] [Google Scholar]
- 17.Yi B, Wang G, Li J, Jiang J, Son Z, Su H, et al. The first clinical use of domestically produced Chinese minimally invasive surgical robot system “Micro Hand S”. Surg Endosc. 2016;30:2649–55. doi: 10.1007/s00464-015-4506-1. [DOI] [PubMed] [Google Scholar]
- 18.Remacle M, Prasad V, Lawson G, Plisson L, Bachy V, Van der Vorst S, et al. Transoral robotic surgery (TORS) with the medrobotics flex™ system: First surgical application on humans. Eur Arch Otorhinolaryngol. 2015;272:1451–5. doi: 10.1007/s00405-015-3532-x. [DOI] [PubMed] [Google Scholar]
- 19.Enayati N, De Momi E, Ferrigno G. Haptics in robot-assisted surgery: Challenges and benefits. IEEE Rev Biomed Eng. 2016;9:49–65. doi: 10.1109/RBME.2016.2538080. [DOI] [PubMed] [Google Scholar]
- 20.Munawar A, Fischer G. A Surgical Robot Teleoperation Framework for Providing Haptic Feedback Incorporating Virtual Environment-Based Guidance. Frontiers in Robotics and AI. 2016:3. [Google Scholar]
- 21.Widmann G. Image-guided surgery and medical robotics in the cranial area. Biomed Imaging Interv J. 2007;3:e11. doi: 10.2349/biij.3.1.e11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Overley SC, Cho SK, Mehta AI, Arnold PM. Navigation and robotics in spinal surgery: Where are we now? Neurosurgery. 2017;80:S86–99. doi: 10.1093/neuros/nyw077. [DOI] [PubMed] [Google Scholar]
- 23.Herrell SD, Galloway RL, Miga MI. Image guidance in robotic-assisted renal surgery. In: Liao JC, Su LM, editors. Advances in Image-Guided Urologic Surgery. New York: Springer New York; 2015. pp. 221–41. [Google Scholar]
- 24.Rassweiler JJ, Autorino R, Klein J, Mottrie A, Goezen AS, Stolzenburg JU, et al. Future of robotic surgery in urology. BJU Int. 2017;120:822–41. doi: 10.1111/bju.13851. [DOI] [PubMed] [Google Scholar]
- 25.Petscharnig S, Schöffmann K. Deep learning for shot classification in gynecologic surgery videos. In: Amsaleg L, Guðmundsson GT, Gurrin C, Jonsson BT, Satoh Si, editors. MultiMedia Modeling: 23rd International Conference, MMM 2017, Reykjavik, Iceland, January 4-6, 2017, Proceedings, Part I. Cham: Springer International Publishing; 2017. pp. 702–13. [Google Scholar]
- 26.Shademan A, Decker RS, Opfermann JD, Leonard S, Krieger A, Kim PC, et al. Supervised autonomous robotic soft tissue surgery. Sci Transl Med. 2016;8:337ra64. doi: 10.1126/scitranslmed.aad9398. [DOI] [PubMed] [Google Scholar]
- 27.Leonard S, Wu KL, Kim Y, Krieger A, Kim PC. Smart tissue anastomosis robot (STAR): A vision-guided robotics system for laparoscopic suturing. IEEE Trans Biomed Eng. 2014;61:1305–17. doi: 10.1109/TBME.2014.2302385. [DOI] [PubMed] [Google Scholar]
- 28.Goldenberg MG, Goldenberg SL, Grantcharov TP. Surgeon performance predicts early continence after robotic-assisted radical prostatectomy. J Endourol. 2017 doi: 10.1089/end.2017.0284. [DOI] [PubMed] [Google Scholar]
- 29.Goh AC, Goldfarb DW, Sander JC, Miles BJ, Dunkin BJ. Global evaluative assessment of robotic skills: Validation of a clinical assessment tool to measure robotic surgical skills. J Urol. 2012;187:247–52. doi: 10.1016/j.juro.2011.09.032. [DOI] [PubMed] [Google Scholar]