

Abstract
Cervicothoracic thymic cysts are rare and difficult to diagnose preoperatively. We report a case of a cervicothoracic thymic cyst presenting as a lateral neck mass and mimicking a laryngocele in a 3-year-old boy and its definitive management.
Keywords: Thymic cyst, Laryngocele, Cervical, Thoracic
Case report
A 3-year-old boy presented with a gradually progressive swelling of 2 years’ duration in the middle of the left side of the neck with variation in size on crying/coughing and respiration (Fig. 1). There was no associated breathing difficulty, voice change, or dysphagia. He was initially assessed at the Department of Otorhinolaryngology, and the swelling was suspected to be a laryngocele. An ultrasound examination of the neck was suggestive of a hypoechoic cystic lesion in the left paratracheal/paraglottic space, extending from the hyoid level into the supraclavicular region. A direct laryngoscopy failed to reveal the internal opening of the laryngocele, which prompted a thoracic surgical consultation and further work-up. Computed tomography of the neck and thorax revealed a well-defined, hypodense cystic lesion of the neck, medial and anterior to the carotid artery and internal jugular vein, extending from the hyoid bone into the anterior mediastinum. Magnetic resonance imaging of the neck and thorax confirmed a well-defined cystic lesion measuring 9.4×2.7×4 cm in the left parapharyngeal space, extending into the thymus in the anterior mediastinum, that was suggestive of a thymic cyst (Fig. 2). There was associated deviation of the trachea to the right without luminal compromise. It was confirmed that a large cystic swelling on the left side of the neck in the anterior triangle communicated through the thoracic inlet into the anterior part of the superior mediastinum, with fluid entering the chest cavity during inspiration and returning to the neck compartment during expiration. Echocardiography revealed a structurally normal heart. The working diagnosis of a benign cervicothoracic cyst was made. After a multidisciplinary team meeting, surgical excision was planned.
Fig. 1.

Left lateral neck swelling.
Fig. 2.

(A–D) Magnetic resonance imaging of the neck and thorax showing well-defined, hyperintense cervical and thoracic components of the cyst.
The tumor was approached through a median sternotomy and a 4-cm left cervical incision along the anterior border of the left sternocleidomastoid. A large cystic mass occupying the upper two-thirds of the anterior mediastinum was identified. The mass was completely surrounded by thymic tissue and was anterior to the pericardium and the brachiocephalic vein. It extended into the left side of the neck behind the sternal notch. The cystic mass located in the upper two-thirds of the anterior mediastinum was dissected, along with the thymus tissue surrounding the cyst. All the fibro-fatty tissue with the thymus was dissected from the left to the right phrenic nerves. In the neck, the cyst was medial to the sternocleidomastoid, lateral to the trachea, and overlying the carotid artery and internal jugular vein. The cyst was thin-walled in this region, located just under the skin and platysma, and was dissected and mobilized on both sides, as well as posteriorly from the vascular plane. After complete dissection, the cyst was pulled down into the chest and removed. By gradual and meticulous dissection, we were able to remove it intact (Fig. 3). The 2 incisions were closed after securing hemostasis. The patient made an uneventful postoperative recovery. A histopathological examination confirmed the diagnosis of a benign multiloculated thymic cyst with thymic hyperplasia.
Fig. 3.
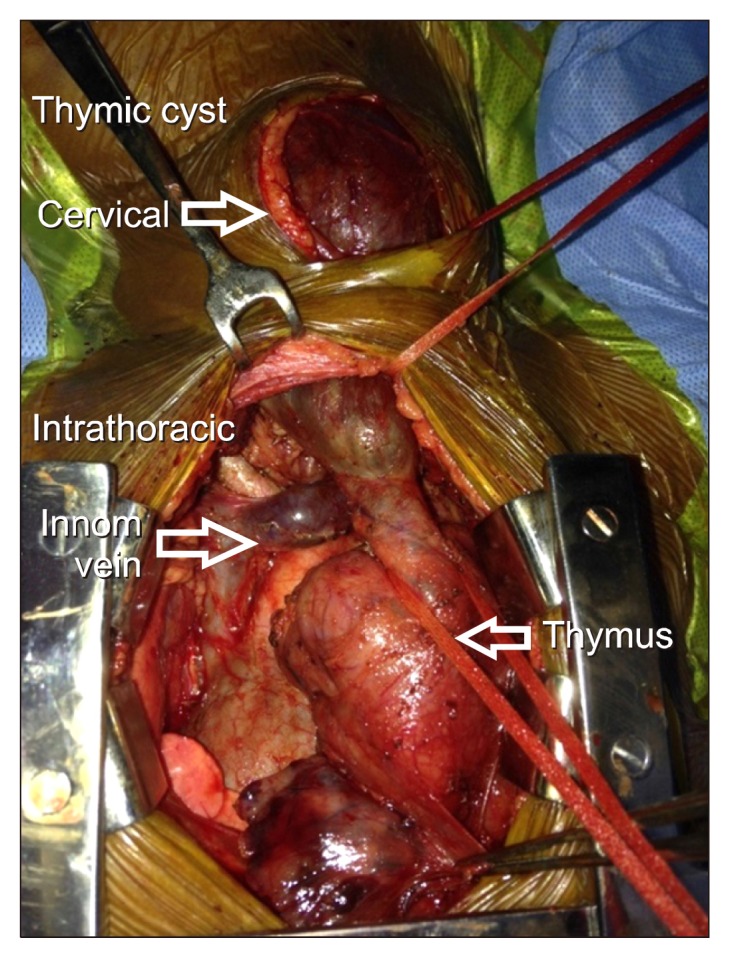
Intraoperative picture showing the cervical and thoracic components of the thymic cyst.
Discussion
The differential diagnosis of lateral neck masses in children includes cystic hygroma, branchial cleft cyst, epidermoid cyst, bronchogenic cyst, laryngocele, and thymic cyst. Thymic cysts are rare and represent fewer than 1% of cystic cervical masses [1]. However, thymic cysts occurring as cervicothoracic masses are a diagnostic challenge.
A painless, soft, compressible cystic swelling in the lateral aspect of the neck, increasing in size with the Valsalva maneuver and expiration, is usually indicative of an external laryngocele. In our case, this particular presentation was clinically diagnosed as an external laryngocele by an otorhinolaryngologist. Further imaging by computed tomography was also inconclusive. However, magnetic resonance imaging confirmed the diagnosis of a cervicothoracic thymic cyst with fluid shifts within the cervical and thoracic components. On magnetic resonance imaging, cervical thymic cysts are hyperintense on T1-weighted images. Mediastinal thymic cysts are usually hypointense on T1-weighted images and hyperintense on T2-weighted imaging. Hyperintensity on T1-weighted images may reflect hemorrhage, high cyst protein content, or cholesterol granulomas [2]. In this case, the hyperintensity on T1-weighted images, with a cervical and thoracic component but with no communication with the laryngotracheal tree, was key for making the diagnosis and helped to differentiate this cervicothoracic thymic cyst from a laryngocele.
Thymic cysts are usually asymptomatic and detected incidentally on imaging. Symptomatic thymic cysts resulting in chest pain, cough, hoarseness, dyspnea, and dysphagia have been reported. Other unusual presentations have included Horner syndrome, tracheomalacia, and cardiac tamponade. Miller et al. [3] reported a mediastinal thymic cyst causing intermittent obstruction of the left brachiocephalic vein, varying with posture.
Cervical thymic cysts represent fewer than 1% of cystic lateral neck masses and approximately 50% have a thoracic extension [1]. However, an increase in size with increasing intrathoracic pressure, mimicking an external laryngocele, is a very rare presentation of a thymic cyst, and should be considered among the rare causes of expansile cystic lateral neck masses. The few reports of this condition in the literature include Sameh et al. [4], who reported a case of a huge cervicothoracic thymic cyst with respiratory variation mimicking a cystic hygroma, and Ozturk et al. [5], who reported a similar presentation mimicking a laryngocele. The definitive treatment is excision.
We report a case of a cervicothoracic thymic cyst presenting as a lateral neck mass and mimicking a laryngocele in a 3-year-old boy and its definitive management.
Footnotes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
References
- 1.Shenoy V, Kamath MP, Hegde MC, Rao Aroor R, Maller VV. Cervical thymic cyst: a rare differential diagnosis in lateral neck swelling. Case Rep Otolaryngol. 2013;2013:350502. doi: 10.1155/2013/350502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cure JK, Tagge EP, Richardson MS, Mulvihill DM. MR of cystic aberrant cervical thymus. AJNR Am J Neuroradiol. 1995;16:1124–7. [PMC free article] [PubMed] [Google Scholar]
- 3.Miller JS, LeMaire SA, Reardon MJ, Coselli JS, Espada R. Intermittent brachiocephalic vein obstruction secondary to a thymic cyst. Ann Thorac Surg. 2000;70:662–3. doi: 10.1016/S0003-4975(00)01573-3. [DOI] [PubMed] [Google Scholar]
- 4.Sameh IS, Ismaeil MF, Nasser MA, Awadalla MM. Huge cervico-thoracic thymic cyst. Interact Cardiovasc Thorac Surg. 2003;2:339–40. doi: 10.1016/S1569-9293(03)00077-X. [DOI] [PubMed] [Google Scholar]
- 5.Ozturk K, Elsurer C, Bulut S, Duran M, Ugras S. Cervical thymic cyst mimicking laryngocele. Case Rep Otolaryngol. 2013;2013:839406. doi: 10.1155/2013/839406. [DOI] [PMC free article] [PubMed] [Google Scholar]