

Abstract
Background
Cancer patients often report increased stress during chemotherapy. Stress management training has been shown to reduce this adverse outcome, but few interventions exist for Spanish-speaking Hispanic and Latina women (Latinas).
Methods
Following community feedback (including focus groups/in-depth interviews), we transcreated the Spanish-Language Self-Administered Stress Management Training (SL-SAT) intervention based on our previously developed and implemented English-based intervention. Latinas about to begin chemotherapy were randomized to SL-SAT (n=121) or usual care (UC; n=119). A Spanish-speaking interventionist met with SL-SAT participants who received the SL-SAT toolkit containing instructions in three well-established stress management techniques (deep breathing, progressive muscle relaxation and guided imagery, and use of coping self-statements). UC participants received an educational booklet about coping with chemotherapy. All patients were instructed by nurses on their chemotherapy medications and given a resource listing of local support groups. Outcomes were obtained at baseline, and 7 and 13 weeks after starting chemotherapy. Primary outcomes included anxiety and depression, cancer-related distress, emotional well-being, and spiritual well-being. Secondary outcomes included functional well-being, social/family well-being, physical well-being, symptom severity, and self-efficacy for managing stress. Data were analyzed using mixed models.
Results
In both groups, improvements were observed in emotional well-being (p=.01), and declines were observed in functional well-being (p=.05), and physical well-being (p<.0001). Symptom severity increased across the follow-up period (p<.001).
Conclusions
To be effective, stress management interventions for Latinas receiving chemotherapy may necessitate more attention from an interventionist, delivery of the intervention over a longer interval, and/or a group-based format.
Cancer patients receiving chemotherapy typically experience multiple aversive symptoms accompanied by declines in quality of life. Stress management training interventions often involve cognitive and/or affective components, to alleviate nausea, fatigue, and emotional distress,1–5 and improve physical and mental quality of life.6 Interventions that provide patients with only audiotapes of relaxation exercises have generally yielded disappointing results.7, 8 Thus, many programs include multiple components such as progressive muscle relaxation training with guided imagery3, 4 and systematic desensitization.5
Although the benefits of stress management training interventions on quality of life are well documented, published studies examining the efficacy of these interventions among Spanish-speaking Hispanic women and Latinas (hereafter referred to as Latinas) receiving chemotherapy are limited. This is surprising given that Hispanics are the largest ethnic minority group in the United States, constituting 17% of the population, and are expected to double in size by 2050.9 Further, recent research has documented high rates of emotional distress in Spanish-speaking Latinas prior to receiving chemotherapy.10
Few randomized trials have investigated the efficacy of stress management programs among Spanish-speaking Latinos, and to our knowledge, only two included women. In the first randomized trial,11 Spanish-speaking Hispanic men with localized prostate cancer participated in either a 10-week stress management intervention or a half-day stress management seminar. Men randomized to the intervention demonstrated improved physical, emotional, and total well-being relative to men in the seminar. In another study,12 Latino men and women undergoing chemotherapy were randomized to receive either a self-administered stress management intervention or usual care. Delivered in community-based cancer settings, the intervention was not found to improve quality of life or reduce psychological distress. In the last study, Spanish-speaking Latinas with breast cancer participated in a stress management intervention emphasizing self-efficacy, outcome expectations, and self-regulation.13 Trained peer companions delivered the intervention in community settings over 8 sessions, and participants randomized to the intervention exhibited significantly improved quality of life and reduced depression relative to participants receiving usual care.
While potentially efficacious, the paucity of linguistically/culturally similar mental health professionals working in oncology settings and the potentially prohibitive costs of using mental health professionals as interventionists14 limit the likelihood of wide dissemination of training-intensive interventions. Thus, the goal of this study was to evaluate, relative to usual care, the efficacy of a Spanish-Language Self-Administered Stress Management Training (SL-SAT) intervention “transcreated” from a successful self-administered stress management training intervention developed for English-language patients.6 Primary outcomes were anxiety and depression (general distress), cancer-related distress, emotional well-being, and spiritual well-being. Secondary outcomes were functional well-being, social/family well-being, physical well-being, symptom severity, and self-efficacy for managing stress. We hypothesized that women randomized to receive SL-SAT would demonstrate better outcomes over the first 13 weeks of chemotherapy relative to those randomized to receive usual care (UC). We also hypothesized that the greatest benefits would be observed among patients who preferred to receive health information in Spanish.
Methods
Participants
Participants were recruited from the Moffitt Cancer Center in Tampa, FL (MCC) and the University of Miami Sylvester Comprehensive Cancer Center in Miami, FL (SCCC). Eligibility criteria included: 1) ≥18 years old; 2) female; 3) self-identified as Hispanic or Latina; 4) able to speak and read in Spanish; 5) diagnosed with cancer; 6) scheduled to start outpatient intravenous chemotherapy for reasons other than symptom palliation; 7) not receiving chemotherapy in the previous two months; 8) free of observable visual, auditory, psychiatric, or neurological disorders that would interfere with participation; and 9) able to provide written informed consent.
Procedure
Study procedures were approved by Institutional Review Boards at the University of South Florida (Pro00006699) and University of Miami (20111145). The study was registered on clinicaltrials.gov (NCT01599520). Eligibility criteria were determined via electronic medical record review identifying patients scheduled for initial consultations with medical oncologists prior to chemotherapy. After completing written informed consent, participants completed baseline self-report questionnaires. Participants were then randomized in equal numbers to SL-SAT or to UC using a computer-generated randomization schedule stratified by study site and chemotherapy cycle format (e.g., 7, 14, 21, or 28 day regimens). As is typical practice at MCC and SCCC, an oncology nurse provided participants standard education about the chemotherapy agents and anti-emetics that were to be administered, possible adverse reactions to these medications, and recommended precautions for avoiding illness during chemotherapy. All participants received information for local support groups and were informed that a social worker could meet with them, without charge, to discuss any concerns.
Usual Care
Participants randomized to UC met with a Spanish-speaking interventionist for approximately 10 minutes at the initial consultation and received a copy of the National Cancer Institute (NCI) publication “La quimioterapia y usted: Apoyo para las personas con cancer” (“Chemotherapy and You: Support for People with Cancer”),15 that the interventionist reviewed with each participant. A research assistant met with each participant at the infusion appointment 5 or 7 weeks after their initial infusion (depending on their regimen) and again at 13 weeks after their initial infusion to administer follow-up self-report questionnaires.
Intervention
The SL-SAT intervention was based on an English-language version that improved depression, anxiety, and mental health in cancer patients during chemotherapy in a randomized trial compared to UC.6 The English version is available as a ‘Research-Tested Intervention Program’ on the Cancer Control P.L.A.N.E.T. website. Guided by a community-based participatory research approach, we translated information from an existing evidence-based English-language stress management intervention using a process called transcreation, in which materials were translated and culturally adapted.16, 17 Similar to the English-language version, the SL-SAT intervention, called “Cómo tratar el estrés durante la quimioterapia” (“How to manage stress during chemotherapy”), provided instruction in three well-established stress management techniques (abdominal breathing, progressive muscle relaxation/guided imagery, and coping self-statements). Consistent with published recommendations for transcreation and materials development,17–20 and guided by an advisory group (patients and providers), the SL-SAT was based on formative work21 involving extensive pretesting and feedback that informed design and content elements such as cultural appropriateness and sensitivity, literacy, visual appeal, and learning stimulation/motivation. For example, concepts like “family” were operationalized beyond just presenting a picture of a Hispanic family. We moved beyond the surface structure to capture the centrality of obligation to family, emotional/physical closeness, and interpersonal communication, all of which were at the center of the stressors discussed during the focus groups. We also emphasized existing coping strategies such as prayer, reading the bible, and faith.21 Further, materials were reviewed with a sample (n=15) of women who comprised the following ethnic sub-groups of Latinas: Puerto Rican, Guatemalan, Cuban, Dominican, and Mexican to ensure understanding and acceptability in consideration of any regional language variations. For example, the original English toolkit used an example of a balloon to illustrate deep breathing. Depending on where participants were from, balloon could be translated as “vejiga,” “bomba,” “globo,” or “bocadillo”—thus, we settled on terms that were universally understood.
Intervention Content
Participants randomized to SL-SAT met with a Spanish-speaking interventionist for an extra 10 minutes on the first day to be introduced to the training materials. Participants were given an 18-minute DVD or video file on a USB drive, 16-page booklet, and a 28-minute CD, which described common sources and manifestations of stress during chemotherapy, and illustrated the three stress management techniques. The DVD also included segments in which Latinas described how they used and benefitted from the techniques. Participants were asked to view the DVD first, then review the booklet, and then listen to the CD, and were encouraged to practice daily and when they experienced chemotherapy-related symptoms (e.g., pain, nausea, fatigue). A Spanish-speaking interventionist called to follow-up one week after the initial visit, and at their infusion appointments approximately every three weeks. At these visits, the interventionist would answer questions about the intervention, and encourage participants to practice the techniques daily.
Intervention Fidelity
Interventionists received extensive training in the protocols to ensure consistency in intervention delivery. They were audio-recorded for their first several interventions, and then periodically thereafter. Approximately 20% of all audio files were reviewed by a bilingual member of the research team to ensure intervention fidelity using multi-item checklists and feedback was shared with interventionists to enhance fidelity.
Measures
Sociodemographic factors assessed at baseline via self-report included age, race, country of origin, number of years residing in the US, country lived in the longest, marital status, education, and income. Self-reported comorbidities were assessed using the Charlson Comorbidity Index.22 All questions were in Spanish. Clinical data were abstracted from the medical chart including date of cancer diagnosis, type of cancer, disease stage, and chemotherapy agents administered.
A Spanish version of the five-item Stress Reduction Checklist used in our previous research was developed for this study to indicate usage of any stress management techniques.
Psychological distress was measured using the validated Spanish version of the 14-item Hospital Anxiety and Depression Scale (HADS).23 This scale asks respondents to indicate the severity of anxiety and depression symptoms. Analyses focused on the total distress score.
Cancer-related distress was assessed using the validated 8-item Spanish version of the Intrusion Subscale of the Impact of Events Scale-Revised (IES-R).24 This scale asked respondents to rate the severity of intrusive thoughts (e.g., dreams, images, reminders of a stressful event) related to a specific event. The questions were keyed to “su cancer y a su diagnóstico” (your cancer and cancer diagnosis).
The 27-item validated Spanish version of the Functional Assessment of Cancer Therapy – General Version 4 (FACT-G) was used to measure quality of life.25 This scale yields subscales for physical, social/family, emotional, and functional well-being.
Spiritual well-being was measured using the validated 12-item Spanish version of the Functional Assessment of Chronic Illness Therapy – Spiritual Well-Being Scale (FACIT-SP).26
Symptom severity was evaluated using the Spanish version of the 24-item Memorial Symptom Assessment Scale – Short Form (MSAS-SF), which asks respondents to indicate whether they experienced various symptoms, and if they were distressing or bothersome.27 Subscales included measures of psychological symptoms (e.g., difficulty concentrating), physical symptoms (e.g., constipation), and a total symptoms score.
Self-efficacy in engaging in stress management strategies was assessed using the 17-item Spanish version of the Measure of Current Status (MOCS),28 which was developed for this study using a process adapted from the Brislin Model of Translation,29, 30 including forward- and back-translation as well as pilot-testing for comprehension and ease of administration.
Hispanic/Latino acculturation was estimated using the Marin Acculturation Scale,31 an eight item scale assessing acculturation related to language use and media preferences. An additional four items were developed and pilot-tested for this study to assess preference for receiving health information. The combined 12 items had high internal reliability (α=.94), and total acculturation was associated with years of U.S. residence (r=.59, p<.0001).
Statistical Analyses
Determination of sample sizes was guided by considerations of statistical power for cross-sectional comparisons, and for differences in rates of changes across the two groups. For between groups comparisons, 150 persons per group would be required to detect 30% differences in slope assuming power of .80, a two-tailed alpha of .05, and three measurement points.32
Chi-square analyses and independent samples t-tests were conducted to compare groups and study sites on baseline demographic and clinical characteristics. Factors different between groups at p<.10 were included as covariates in multivariate analyses. Changes across the follow-up period between groups were compared using PROC MIXED in SAS, version 9.4 (Cary, NC).33, 34 Group*time*acculturation interactions were conducted to examine the moderating effect of acculturation on group differences in change over time.
Results
Of the 324 patients approached for participation, 258 (80%) signed consent (Supplemental Appendix 1 – Consort Diagram). Of consented patients, 11 were deemed ineligible, three were lost to follow-up, and four withdrew from the study, resulting in 240 who were randomized to either the SL-SAT (n=121) or UC (n=119) group. One individual in the SL-SAT group was lost to follow-up prior to starting the baseline assessment and was not included in analyses. Participants who completed all three assessments were more likely than those who did not to have more advanced disease (e.g., 40% vs. 30% with stage III or IV cancer, p<.0001). There were no other significant demographic or clinical differences between those who completed all assessments and those who did not (p-values>.10).
Demographic and clinical characteristics are displayed in Table 1. Participants averaged 51 years of age (SD=10.6), were predominantly White (82.4%), married (52.7%), with 12 or fewer years of education (50%), and earned less than $20,000 in household income (55.8%). Most were diagnosed within the prior three and a half months (SD=10.2 months) with breast cancer (81%), ovarian cancer (6%), or lung cancer (3%), and had stage I or II cancer (62%).
Table 1.
Sociodemographic and Clinical Characteristics of Participants
| Variable | Stress Management (N = 120) |
Usual Care (N = 119) |
p-value |
|---|---|---|---|
| Age: M (SD) | 51.1 (10.6) | 51.71 (10.7) | 0.66 |
| Ethnicity, Hispanic: n (%) | 120 (100) | 119 (100) | |
| Race, White: n (%) | 100 (85) | 89 (79) | 0.18 |
| Marital Status, Married: n (%) | 56 (47) | 69 (58) | 0.09 |
| Education, 12 years or less: n (%) | 62 (52) | 57 (48) | 0.60 |
| Annual household income, $20,000 or more: n (%) | 35 (35) | 41 (51) | 0.04 |
| Employment, at least part-time: n (%) | 45 (39) | 43 (36%) | 0.71 |
| Years residing in the US: M (SD) | 24.50 (16.7) | 24.13 (16.8) | 0.87 |
| Country of Birth: n (%) | 0.42 | ||
| Cuba | 37 (43) | 39 (49) | |
| United States | 18 (21) | 12 (15) | |
| Mexico | 11 (13) | 9 (11) | |
| Colombia | 10 (12) | 5 (6) | |
| Puerto Rico | 10 (12) | 15 (19) | |
| Disease Type: n (%) | 0.91 | ||
| Breast Cancer | 100 (83) | 94 (79) | |
| Ovarian Cancer | 7 (6) | 8 (7) | |
| Other | 13 (11) | 17 (14) | |
| Disease Stage: n (%) | 0.07 | ||
| I | 27 (23%) | 18 (15%) | |
| II | 51 (43%) | 51 (44%) | |
| III | 30 (25%) | 43 (37%) | |
| IV | 12 (10%) | 5 (4%) | |
| Months since Initial Diagnosis: M (SD) | 3.02 (5.72) | 3.92 (13.25) | 0.50 |
Participants recruited from SCCC were significantly more likely to have breast cancer (98% vs. 69%, p<.0001) and early stage disease (75% vs. 56% with stage I or II cancer, p=.02) than participants recruited from MCC. Participants randomized to SL-SAT reported lower annual household income (p=.04, missing=28%), were marginally less likely to be married (p=.09), and had less advanced disease (p=.07) than participants in the UC group (Table 1). Because of these differences, recruitment site and marital status were entered as covariates in later analyses. The large percentage of participants declining to provide income data (28%) precluded us from including income as a covariate. No other comparisons by recruitment site or intervention assignment were significant (i.e., education, race, ethnicity, and age).
Results relating to the primary outcomes of anxiety and depression, cancer-related distress, emotional well-being, and spiritual well-being are in Table 2. Emotional well-being improved significantly over the follow-up period (p=.01), with the quadratic effect of time (p=.05) revealing that improvement plateaued from Time 2 to Time 3. No other outcomes exhibited statistically significant change across the follow-up period. No group differences were observed in change over time in these outcomes (p-values>.05; Cohen’s ds<.05). Post-hoc analyses with distress as a moderator did not reveal an effect of distress on intervention efficacy. Among women receiving SL-SAT, acculturation was not associated with change in primary outcomes (p-values>.05).
Table 2.
Unstandardized Parameter Estimates for Primary Outcomes
| Effect | General Distress | Cancer-related Distress | Emotional Well-Being | Spiritual Well-Being |
|---|---|---|---|---|
| Intercept | 13.87*** | 1.39*** | 15.72*** | 37.90*** |
| Intervention | −1.31 | −0.2 | 0.48 | 0.35 |
| Time | −1.95 | −0.19 | 2.40** | 1.09 |
| Time*Time | 1.16 | 0.03 | −0.95* | −0.76 |
| Time*Intervention | 2.01 | 0.08 | −0.79 | −0.87 |
| Time*Time*Intervention | −0.83 | <.01 | 0.35 | 0.52 |
Note: Covariates included married/not married, and recruitment site, and their linear and quadratic interactions with time.
p <.001
p < .01
p < .05
Table 3 displays the results of the analyses for the secondary outcomes of functional well-being, social/family well-being, physical well-being, total symptom severity, and self-efficacy for managing stress. Both functional well-being (p=.05) and physical well-being (p<.0001) declined significantly over time. Total symptom severity increased significantly over the follow-up period across groups (p<.0001). There were no group differences in change in these outcomes over time (p-values>.05; Cohen’s ds<.05). No differences in intervention effects over time by acculturation were observed (p-values>.05).
Table 3.
Unstandardized Parameter Estimates for Secondary Outcomes
| Effect | Functional Well-Being | Social/Family Well-Being | Physical Well-Being | Total Symptom Severity | Self-Efficacy |
|---|---|---|---|---|---|
| Intercept | 17.85*** | 21.75*** | 22.24*** | 0.61*** | 60.58** |
| Intervention | −0.08 | −0.38 | −0.10 | -0.03 | -0.99 |
| Time | −2.40* | −0.13 | −7.16** | 0.78*** | 1.45 |
| Time*Time | 0.59 | −0.24 | 2.09** | −0.21*** | −1.20 |
| Time*Intervention | −1.28 | 0.47 | 1.40 | 0.00 | −0.36 |
| Time*Time*Intervention | 0.68 | −0.09 | −0.71 | 0.00 | 0.64 |
Note: Covariates included married/not married, and recruitment site, and their linear and quadratic interactions with time.
p <.001
p < .01
p < .05
The results of our stress reduction manipulation check indicated significant group*time (p<.0001) and group*time*time (p<.0001) interactions, such that use of stress management techniques increased over time in the SL-SAT group but not the UC group (d=.42; see Figure 1). No group differences were observed at baseline (p=.58), but the SL-SAT group reported greater use of stress management techniques at T2 and T3 (p-values<.001).
Figure 1. Estimated Means for Stress Management Techniques.
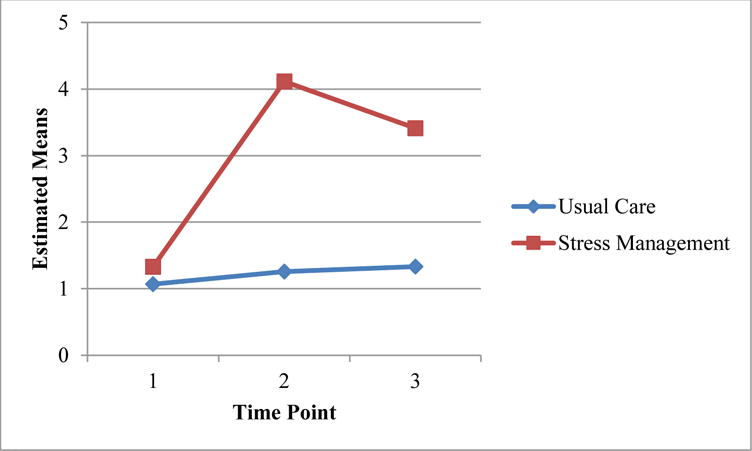
Note. Estimated means are adjusted for marital status (married/not married) and recruitment site.
Discussion
In this study, we evaluated the efficacy of a culturally-transcreated stress management intervention in a randomized controlled trial involving Spanish-speaking Latinas about to begin chemotherapy for cancer. It was hypothesized that patients who received the intervention would have better psychosocial outcomes compared to patients who received usual care. While improvements were observed in both groups in emotional well-being, group assignment did not impact study outcomes (all Cohen’s ds<.05). This is contrary to our previous research6 evaluating a patient self-administered stress management training among English-speaking cancer patients undergoing chemotherapy, in which we found that patients who received the intervention reported significantly better physical functioning, greater vitality, fewer role limitations because of emotional problems, and better mental health. In particular, the current findings are surprising since the SL-SAT intervention was transcreated based on extensive formative research.
There are a number of possible explanations for these findings. One may be a need for additional cultural adaptation or customization of certain elements in the intervention, particularly considering the sample represented 16 different nationalities. Our formative work showed that it was important to address family as a central aspect of care, acknowledge current coping strategies, and highlight staying connected with support persons/systems to desahogar (to vent and/or alleviate distress by telling one’s problems to someone). This may suggest that increasing contact and interpersonal communications may be especially helpful since many were far away from their family who lived in other countries.21 Further, while exposure to the techniques was provided in SL-SAT, continued reinforcement of these more ‘structured’ techniques (vs prayer) may be needed to fully integrate the practices into their everyday lives (similar to the adoption and integration of healthy eating or stop smoking behaviors). Future interventions may benefit from integrating more support enhancements. For example, a recent study with Latino men points out that a vital area for future work involves strengthening social networks and alleviating feelings of social isolation. It may be that incorporating coaches, peer booster sessions, group trainings delivered in-person or via the web, or additional therapist contact might complement existing support systems and bolster motivation.
In a study12 that evaluated a similar self-administered stress-management training intervention for Latino men and women in multiple community clinical settings, no significant treatment effects on quality of life were found among participants receiving stress management training. However, the intervention techniques were deemed useful by participants. Taken together with our findings, future interventions to reduce distress in Latina cancer patients might consider added interventionist contact or a wider variety of learning formats, such as group-based education, to bolster support. Other group-based stress management programs of varying durations,35, 36 some eight weeks or longer,13, 28, 37 have demonstrated positive psychosocial effects in individuals with cancer.
In the current study, we hypothesized that among women who received the intervention, those who were less acculturated and had a stronger preference for receiving health care information in Spanish would benefit more. This was not the case, consistent with prior research on self-administered stress management in Latinos.12 Latinas who were less acculturated may have experienced more stress related to immigration, communication with family members, or other interpersonal issues related to the cancer diagnosis and subsequent treatment that were not addressed by the SL-SAT techniques.
Study Strengths
The current study has several strengths, including being the largest stress management study to target Latinas undergoing chemotherapy with multiple follow-up assessments. We were able to successfully reach and provide Latinas who preferred Spanish language with information that could be helpful in their recovery. Further, among women in the intervention group, adherence to stress management techniques increased over time.
Study Limitations
Limitations include marginally lower baseline distress in the stress management group, potentially masking group differences in stress reduction over time. In addition, participants who did not complete all assessments were more likely than those who did to have more advanced disease, and to be in the intervention group, making it difficult to evaluate the effects of the intervention on participants most in need of stress management.
Clinical Implications
Future directions for stress management interventions with Spanish-speaking Latinas being treated for chemotherapy include examining the impact of additive individual and/or group social support features (e.g., peer support, additional therapist sessions) delivered over longer periods of time. Further, the supplementation of interventions with technologies (e.g., embodied conversational agents, smart phone apps) may further enrich supportive care in this population. For example, in a recent study, a technology-assisted psychosocial intervention was found to be feasible, acceptable, and efficacious among men with advanced prostate cancer, and significantly reduced depressive symptoms and improved relaxation self-efficacy at the 6-month follow-up.38 In conclusion, as Latinas are a growing segment of the population of cancer patients, there is a need for enhanced clinical and research efforts to detect unmet care needs and to develop efficacious and empowering psychosocial educational care interventions.
Supplementary Material
Acknowledgments
The study was funded by RSG-12-087-01-CPPB (Current PI: Meade; former PI: Jacobsen) from the American Cancer Society. The efforts of Dr. Hoogland were supported by R25 CA090314 (Current PI: Brandon; former PI: Jacobsen) from the National Cancer Institute. This work was also supported in part by the Biostatistics Core and the Survey Methods Core at the H. Lee Moffitt Cancer Center & Research Institute, an National Cancer Institute-designated Comprehensive Cancer Center (NIH/NCI Grant Number: P30-CA076292). A portion of the results for the current study were presented at the 2015 Society for Behavioral Medicine Annual Meeting.
Footnotes
Conflict of Interest
The authors declare no conflicts of interest. This work was performed while Dr. Jacobsen was at the Moffitt Cancer Institute and does not represent the views of the National Cancer Institute.
References
- 1.Lerman C, Rimer B, Blumberg B, Cristinzio S, Engstrom PF, MacElwee N, et al. Effects of coping style and relaxation on cancer chemotherapy side effects and emotional responses. Cancer Nurs. 1990 Oct;13(5):308–15. [PubMed] [Google Scholar]
- 2.Walker L, Walker M, Ogston K, Heys S, Ah-See A, Miller I, et al. Psychological, clinical and pathological effects of relaxation training and guided imagery during primary chemotherapy. Br J Cancer. 1999;80(1–2):262. doi: 10.1038/sj.bjc.6690349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Burish TG, Lyles JN. Effectiveness of relaxation training in reducing adverse reactions to cancer chemotherapy. J Behav Med. 1981 Mar;4(1):65–78. doi: 10.1007/BF00844848. [DOI] [PubMed] [Google Scholar]
- 4.Lyles JN, Burish TG, Krozely MG, Oldham RK. Efficacy of relaxation training and guided imagery in reducing the aversiveness of cancer chemotherapy. J Consult Clin Psychol. 1982 Aug;50(4):509–24. doi: 10.1037//0022-006x.50.4.509. [DOI] [PubMed] [Google Scholar]
- 5.Morrow GR. Effect of the cognitive hierarchy in the systematic desensitization treatment of anticipatory nausea in cancer patients: A component comparison with relaxation only, counseling, and no treatment. Cognit Ther Res. 1986;10(4):421–46. [Google Scholar]
- 6.Jacobsen PB, Meade CD, Stein KD, Chirikos TN, Small BJ, Ruckdeschel JC. Efficacy and costs of two forms of stress management training for cancer patients undergoing chemotherapy. J Clin Oncol. 2002 Jun 15;20(12):2851–62. doi: 10.1200/JCO.2002.08.301. [DOI] [PubMed] [Google Scholar]
- 7.Carey MP, Burish TG. Providing relaxation training to cancer chemotherapy patients: A comparison of three delivery techniques. J Consult Clin Psychol. 1987 Oct;55(5):732–7. doi: 10.1037//0022-006x.55.5.732. [DOI] [PubMed] [Google Scholar]
- 8.Morrow GR. Appropriateness of taped versus live relaxation in the systematic desensitization of anticipatory nausea and vomiting in cancer patients. J Consult Clin Psychol. 1984 Dec;52(6):1098–9. doi: 10.1037//0022-006x.52.6.1098. [DOI] [PubMed] [Google Scholar]
- 9.Siegel RL, Fedewa SA, Miller KD, Goding-Sauer A, Pinheiro PS, Martinez-Tyson D, et al. Cancer statistics for Hispanics/Latinos, 2015. CA Cancer J Clin. 2015;65(6):457–80. doi: 10.3322/caac.21314. [DOI] [PubMed] [Google Scholar]
- 10.Lee MS, Martinez D, Gonzales BD, Small BJ, Lechner SC, Antoni MH, et al. Anxiety and depression in Spanish-speaking Latina cancer patients prior to starting chemotherapy. Psychooncology. 2017 doi: 10.1002/pon.4462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Penedo FJ, Traeger L, Dahn J, Molton I, Gonzalez JS, Schneiderman N, et al. Cognitive behavioral stress management intervention improves quality of life in Spanish monolingual hispanic men treated for localized prostate cancer: Results of a randomized controlled trial. Int J Behav Med. 2007;14(3):164–72. doi: 10.1007/BF03000188. [DOI] [PubMed] [Google Scholar]
- 12.Aguado Loi CX, Taylor TR, McMillan S, Gross-King M, Xu P, Shoss MK, et al. Use and helpfulness of self-administered stress management therapy in patients undergoing cancer chemotherapy in community clinical settings. J Psychosoc Oncol. 2012;30(1):57–80. doi: 10.1080/07347332.2011.633981. [DOI] [PubMed] [Google Scholar]
- 13.Nápoles AM, Ortíz C, Santoyo-Olsson J, Stewart AL, Gregorich S, Lee HE, et al. Nuevo Amanecer: Results of a randomized controlled trial of a community-based, peer-delivered stress management intervention to improve quality of life in Latinas with breast cancer. Am J Public Health. 2015;105(S3) doi: 10.2105/AJPH.2015.302598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Services UDoHaH. A supplement to mental health: A report of the Surgeon General. Rockville, MD: 2001. Mental health: Culture, race, and ethnicity. [PubMed] [Google Scholar]
- 15.Institute NC. La quimioterapia y usted: Apoyo para las personas con cáncer (Chemotherapy and You: Support for People with Cancer). National Cancer Institute. Washington, DC: National Institutes of Health; 2007. [Google Scholar]
- 16.Castro FG, Barrera M, Jr, Holleran Steiker LK. Issues and challenges in the design of culturally adapted evidence-based interventions. Annu Rev Clin Psychol. 2010;6:213–39. doi: 10.1146/annurev-clinpsy-033109-132032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Solomon FM, Eberl-Lefko AC, Michaels M, Macario E, Tesauro G, Rowland JH. Development of a linguistically and culturally appropriate booklet for Latino cancer survivors: Lessons learned. Health Promot Pract. 2005 Oct;6(4):405–13. doi: 10.1177/1524839905278447. [DOI] [PubMed] [Google Scholar]
- 18.Macario E, Boyte RM. Translating health information effectively for Latino populations. Calif J Health Promot. 2008;6(1):128–37. [Google Scholar]
- 19.Cowan CF. Teaching patients with low literacy skills. 2004 [Google Scholar]
- 20.Buki LP, Salazar SI, Pitton VO. Design elements for the development of cancer education print materials for a Latina/o audience. Health Promot Pract. 2008 doi: 10.1177/1524839908320359. [DOI] [PubMed] [Google Scholar]
- 21.Tyson DM, Jacobsen P, Meade CD. Understanding the stress management needs and preferences of Latinas undergoing chemotherapy. J Cancer Educ. 2016;31(4):633–9. doi: 10.1007/s13187-015-0844-x. [DOI] [PubMed] [Google Scholar]
- 22.Katz JN, Chang LC, Sangha O, Fossel AH, Bates DW. Can comorbidity be measured by questionnaire rather than medical record review? Med Care. 1996;34(1):73–84. doi: 10.1097/00005650-199601000-00006. [DOI] [PubMed] [Google Scholar]
- 23.Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 24.Báguena MJ, Villarroya E, Beleña A, Díaz A, Roldán C, Reig R. Propiedades psicométricas de la versión española de la Escala Revisada de Impacto del Estresor (EIE-R) Análisis Modificación Conducta. 2001;27:581–604. [Google Scholar]
- 25.Dapueto JJ, Francolino C, Servente L, Chang C-H, Gotta I, Levin R, et al. Evaluation of the Functional Assessment of Cancer Therapy-General (FACT-G) Spanish Version 4 in South America: classic psychometric and item response theory analyses. Health Qual Life Outcomes. 2003;1(1):32. doi: 10.1186/1477-7525-1-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Peterman AH, Fitchett G, Brady MJ, Hernandez L, Cella D. Measuring spiritual well-being in people with cancer: the functional assessment of chronic illness therapy—Spiritual Well-being Scale (FACIT-Sp) Ann Behav Med. 2002;24(1):49–58. doi: 10.1207/S15324796ABM2401_06. [DOI] [PubMed] [Google Scholar]
- 27.Chang VT, Hwang SS, Feuerman M, Kasimis BS, Thaler HT. The memorial symptom assessment scale short form (MSAS-SF) Cancer. 2000 Sep 01;89(5):1162–71. doi: 10.1002/1097-0142(20000901)89:5<1162::aid-cncr26>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 28.Antoni MH, Lechner SC, Kazi A, Wimberly SR, Sifre T, Urcuyo KR, et al. How stress management improves quality of life after treatment for breast cancer. J Consult Clin Psychol. 2006;74(6):1143. doi: 10.1037/0022-006X.74.6.1152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1(3):185–216. [Google Scholar]
- 30.Jones PS, Lee JW, Phillips LR, Zhang XE, Jaceldo KB. An adaptation of Brislin’s translation model for cross-cultural research. Nurs Res. 2001;50(5):300–4. doi: 10.1097/00006199-200109000-00008. [DOI] [PubMed] [Google Scholar]
- 31.Marin G, Sabogal F, Marin BV, Otero-Sabogal R, Perez-Stable EJ. Development of a short acculturation scale for Hispanics. Hisp J Behav Sci. 1987;9(2):183–205. [Google Scholar]
- 32.Diggle PJ, Heagerty P, Liang K-Y, Zeger SL. Analysis of Longitudinal Data. New York, NY: Oxford University Press; 2002. [Google Scholar]
- 33.Singer JD. Using SAS PROC MIXED to fit multilevel models, hierarchical models, and individual growth models. J Educ Behav Stat. 1998;23(4):323–55. [Google Scholar]
- 34.Singer JD, Willett JB. Applied longitudinal data analysis: Modeling change and event occurrence. Oxford university press; 2003. [Google Scholar]
- 35.Antoni MH, Wimberly SR, Lechner SC, Kazi A, Sifre T, Urcuyo KR, et al. Reduction of cancer-specific thought intrusions and anxiety symptoms with a stress management intervention among women undergoing treatment for breast cancer. Am J Psychiatry. 2006;163(10):1791–7. doi: 10.1176/ajp.2006.163.10.1791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gudenkauf LM, Antoni MH, Stagl JM, Lechner SC, Jutagir DR, Bouchard LC, et al. Brief cognitive–behavioral and relaxation training interventions for breast cancer: A randomized controlled trial. J Consult Clin Psychol. 2015;83(4):677. doi: 10.1037/ccp0000020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Penedo FJ, Molton I, Dahn JR, Shen B-J, Kinsinger D, Traeger L, et al. A randomized clinical trial of group-based cognitive-behavioral stress management in localized prostate cancer: Development of stress management skills improves quality of life and benefit finding. Ann Behav Med. 2006;31(3):261–70. doi: 10.1207/s15324796abm3103_8. [DOI] [PubMed] [Google Scholar]
- 38.Yanez B, McGinty HL, Mohr DC, Begale MJ, Dahn JR, Flury SC, et al. Feasibility, acceptability, and preliminary efficacy of a technology-assisted psychosocial intervention for racially diverse men with advanced prostate cancer. Cancer. 2015;121(24):4407–15. doi: 10.1002/cncr.29658. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.