

Abstract
Surveillance for hepatocellular carcinoma (HCC) has been recommended in patients with cirrhosis. In this work, we examine the extent to which the competing risk of hepatic decompensation influences the benefit of HCC surveillance, by investigating the impact of availability of liver transplantation (LTx) and rate of progression of hepatic decompensation on survival gain from HCC surveillance. A multistate Markov model was constructed simulating a cohort of 50-year old patients with compensated cirrhosis. The primary outcome of interest was all-cause and HCC-specific mortality. The main input data included incidence of HCC, sensitivity of screening test, and mortality from hepatic decompensation. Treatment modalities modeled included LTx, resection, and radiofrequency ablation. In the base case scenario, LTx would be available to rescue a proportion of patient from deaths. In the absence of surveillance, 68.2% of the cohort members died by 15 years, which was from HCC in 25.1% and from hepatic decompensation in 43.6% of decedents. With surveillance, the median survival improved from 10.4 years to 11.2 years. The number needed to be under surveillance to reduce one all- cause and HCC-specific death over 15 years was 28 and 18, respectively. In sensitivity analyses, incidence of HCC and progression of cirrhosis had the strongest effect on the benefit of surveillance, whereas LTx availability had negligible impact.
Conclusions
HCC surveillance decreases all-cause and tumor-specific mortality in patients with compensated cirrhosis regardless of LTx availability. In addition, incidence of HCC and sensitivity of surveillance test also had a substantial impact on the benefits of surveillance.
Keywords: Liver cancer, screening, Markov model
Introduction
Despite recent advances in the treatment of hepatocellular carcinoma (HCC) that help patients in an early stage achieve better outcomes, an unacceptable proportion of patients present at an advanced, symptomatic stage of disease. In order to detect HCC at an early stage, surveillance for HCC has been recommended in patients at risk, principally in those with cirrhosis.1 A number of studies have shown that HCC surveillance leads to early detection of HCC, affords the patient a chance to receive curative treatment, and decreases mortality.2, 3 Based on these results, the American Association for the Study of Liver Disease (AASLD), European Association for the Study of the Liver (EASL), European Organization for Research and Treatment of Cancer (EORTC), and Asian Pacific Association for the Study of the Liver (APASL) practice guidelines have recommended HCC surveillance in selected, high risk patients.4-6
Surveillance for HCC, however, is not uniformly embraced. This may in part be related to lack of support from authorities such as the US National Cancer Institute, which believe that conclusive data for its benefits outweighing risks are lacking.7 A unique aspect of HCC is that the vast majority of affected patients have underlying chronic liver disease and cirrhosis. In addition to HCC, these patients are at risk of developing hepatic decompensation. Thus, death from hepatic decompensation, constituting a competing risk for HCC, diminishes the effectiveness of surveillance. Clearly, patients who succumb to hepatic decompensation derive no benefit.
In this work, we recognize that the impact of hepatic decompensation on the effectiveness of HCC surveillance may be mitigated by the availability of liver transplantation (LTx) or, as exemplified in the recent success in antiviral therapy against hepatitis B or C, by slowing the rate of progression to hepatic decompensation. Ideally, high quality randomized studies with adequate statistical power would provide robust answers to these questions.8 In the absence of such empirical data, however, simulation modeling provides a means to evaluate the extent to which HCC surveillance may affect survival in patients with liver cirrhosis. The aims of this work included 1) to determine the magnitude of the long-term survival benefit of HCC surveillance in patients with compensated cirrhosis and 2) to identify determinants of the benefits of surveillance, specifically focusing on the impact of LTx availability and progression of liver disease.
Methods
Markov Simulation Method
A multistate Markov microsimulation model was constructed simulating a cohort of 50-year old patients with compensated cirrhosis. The cycle length of the model was 1 month and the Markov cycle was repeated for 180 cycles or 15 years. HCC surveillance would be performed every 6 months. Figure 1 demonstrates the Markov state transition model used in this study. In the model, the benefits of surveillance would result from HCCs diagnosed at an early stage, which may be treated with a potentially curative modality, namely LTx, surgical resection, or radiofrequency ablation (RFA). A cohort of 100,000 individual subjects was modeled under two scenarios; no surveillance (N=50,000) and surveillance (N=50,000)
Figure 1.
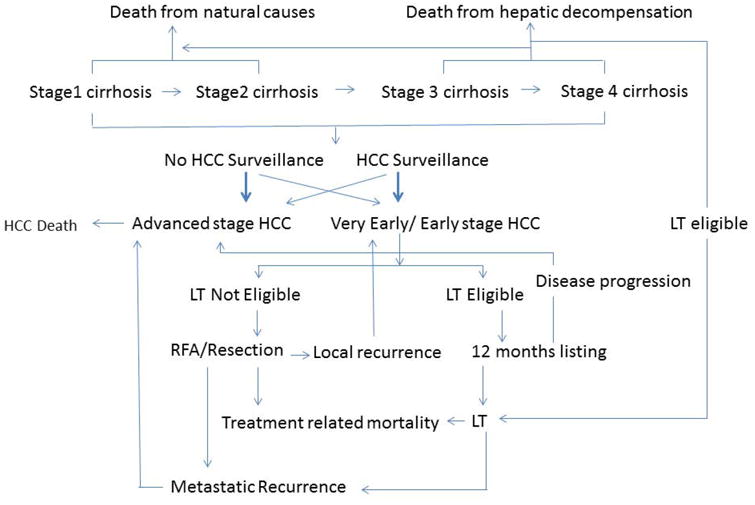
A simplified outline of the Markov state transition model.
Subjects in both groups remain at risk of death from hepatic decompensation, HCC, death from treatment complication or death of unrelated causes.
Subjects in all groups could over time experience hepatic decompensation and/or develop HCC. HCC would progress from early to advanced stages. Subjects under surveillance would be more likely diagnosed with an early stage HCC, whereas those not under surveillance would be diagnosed at an early stage less frequently. The extent to which subjects under surveillance are diagnosed in an early stage HCC would depend on the sensitivity of the surveillance test. Subjects with HCC may die because of treatment complications, progressive or recurrent HCC, decompensated liver disease, or unrelated causes.
The primary outcome of interest was mortality from all causes and from HCC. In addition to the number of deaths in each cohort, we calculated the number of subjects that need to undergo surveillance to save one life (number needed to be in surveillance, NNS) from all-cause and HCC-specific mortality. This was obtained following the standard method to compute the number needed to treat (inverse of the absolute risk reduction). In addition, relative risk reduction was calculated by the ratio of the difference between mortality without surveillance and mortality with surveillance divided by mortality without surveillance. TreeAge Pro (v20151120 Williamstown, MA) was used to generate the Markov model.
Input Variables
The main input data included in this analysis were extracted from published literature; however, since not all of the variables needed to execute the model could be populated in a robust, evidence-based fashion, expert opinion was used to supplement the available data. Sensitivity analyses were undertaken, as described in more detail below, to evaluate the degree to which the study conclusion would be affected by the uncertainty in the data.
Key transition probabilities in the model included annual incidence of HCC (3%, range: 1-5%)9, 10 and median annual mortality of incurable HCC (50%, range: 45-55%).11, 12 The mean interval of tumor progression between early, detectable lesions to advanced stage was set to be 1 year, based on the reported doubling time of HCC of approximately 6 months.13 Median time-to-event for annual HCC mortality and mean tumor progression were converted into transition probabilities using standard declining exponential functions (1-e-ht, where h is ln(2)/Median Time and r is 1/Mean Time). We modeled cirrhosis progression stochastically, as well. Transition probabilities for the four stages of cirrhosis were utilized based on data from a large meta-analysis and the probability of death from hepatic decompensation was based on cirrhosis stage.14
In patients undergoing LTx, postoperative mortality was set to be 9% in the first 12 months and then 2% annually thereafter.15 Procedure-related mortality was assigned to be 1% and 5% in the first 6 months post RFA 16, 17 and liver resection, 18-20 respectively. There would be no procedure-related mortality for RFA or liver resection beyond 6 months after the treatment. We modeled that 70% (combining metastatic recurrence at 4.4% annually over 5 years and de novo HCC or intrahepatic ‘early’ HCC recurrence at 17.8% annually) of patients receiving RFA or resection develop HCC recurrence over 5 years, while 13% of patients receiving LT develop metastatic recurrent disease over 5 years.21-23 Progression of cirrhosis stage and the risk of death from hepatic decompensation would persist except in patients undergoing LTx. In all cohorts, age-specific mortality from unrelated causes was taken from the life expectancy data of the US population. 24
Base case scenario and Sensitivity Analyses
We estimated that 30% in the non-surveillance cohort would be diagnosed at an early stage of HCC and eligible for curative treatment in the same fashion as early HCC patients of the surveillance cohort.25 We have modelled that 75% of individuals with early stage HCC would receive potentially curative treatment (LTx, RFA or resection).26, 27
In the base case scenario, LTx would be available for 17% of patients who would have died of hepatic decompensation.28 We estimated that 33% of early stage HCC patients to be eligible for LTx listing. The remaining two thirds would receive either RFA or resection, depending on their cirrhosis stage. Patients with stage 1 cirrhosis would receive resection while RFA would be available for patients in all other stages. The waiting time before receiving LTx for HCC would be 12 months at which time 80% would undergo LTx while the remaining 20% of HCC patients listed for LTx would drop out due to tumor progression, death from cirrhosis, death from natural causes, or for other reasons.29, 30
We assumed that 18% patients with early stage HCC had very early stage HCC (single tumor less than 2cm).31 As patients with BCLC 0 HCC don't qualify for MELD exception score in the current organ allocation system in the US, we have modelled that they receive resection or RFA. Alternatively, they can wait for 6 months without any HCC treatment to simulate the situation where patients wait until the tumor grows into UNOS T2 stage to be listed for LTx. LTx would be considered as a treatment option in 33% of patients for BCLC 0 patients only after waiting for 6 months. We have assumed that there is no metastatic recurrence after curative treatment for very early stage HCC but patients continue to have risk of developing de novo HCC after curative treatment.
One-way sensitivity analysis was undertaken to identify variables that have an important impact on the results of the analyses. These include (1) no progression of cirrhosis beyond stage 1, (2) annual incidence of HCC (range: 1%-5%), (3) sensitivity of HCC surveillance test (range: 50%-90%), (4) availability of LTx for hepatic decompensation (range: 0%-100%), (5) time to develop a late stage cancer from an early stage (range: 4-36 months), and (6) annual mortality due to late stage HCC (range: 40%-80%). Finally, we incorporated discounting for future years of life, recognizing the time preference in evaluation of life over time. Without making value judgment about the impact of hepatic decompensation and HCC on the utility of the patient, we used the standard discount rate of 3% uniformly in the model and assessed its impact on the results.
Probabilistic sensitivity analysis (PSA) was performed to address uncertainty beyond limited one-way sensitivity analyses. Uncertainty regarding the base case value of each variable (i.e. second-order uncertainty) and the impact of such uncertainty on base case results was examined in PSA by sampling all variables over their ranges (Table 1), using triangular or Beta distributions. The Markov analysis was performed for 100 iterations (100,000 subjects in each iteration, 50,000 per strategy), where each iteration represented a different sampling of variables from the assumed distributions.
Table 1. Main Variables used for the Markov Model.
| Variable | Input data | |
|---|---|---|
| Basecase scenario | Range | |
| Progression of cirrhosis stage per year14 | stage 1 to 2:7% stage 1 to 3: 4% stage 2 to 3: 7% stage 2 to 4: 4% stage 3 to 4: 8% |
stage 1 to 2: 4-10% stage 1 to 3: 2-6% stage 2 to 3: 4-10% stage 2 to 4: 2-6% stage 3 to 4: 6-10% |
| Annual hepatic decompensation mortality per cirrhosis stage14 | stage 1: 1% stage 2: 3% stage 3: 20% stage 4: 57% |
stage 1: 0.8-1.3% stage 2: 2.6-4.3% stage 3: 15-25% stage 4: 44-70% |
| Annual incidence of HCC9-10 | 3% | 1-5% |
| Sensitivity of screening test1 | 70% | 60-80% |
| Detection of early stage HCC without surveillance25 | 30% | 25-35% |
| Probability of transition from Early to Advanced HCC13 | 63% | 40-86% |
| Annual mortality of incurable HCC11,12 | 50% | 45-55% |
| Probability of receiving curative treatment for early stage HCC26-27 | 75 % | 70-80% |
| Treatment related mortality | ||
| LTx15 | 9% in the first 12 months and then 2% annually after the first year | 3-15% in the first 12 months and then 1.5-2.5% annually after the first year |
| Surgery19-20 | 5% in the first 6 months and 0% thereafter | 2.5-7.5% in the first 6 months and 0% thereafter |
| RFA16-17 | 1% in the first 6 months and 0% thereafter | 0.5-1.5% in the first 6 months and 0% thereafter |
| Probability of Liver transplant listing28 | Hepatic decompensation: 17%HCC: 33% | Hepaticdecompensation:11-23%HCC: 29-36% |
| Duration of Liver transplant waitlist15 | 12 months | 6-18 months |
| Risk of recurrence after treatment within 5 years | ||
| LTx22 | 13% over 5 years | 10-16% |
| Surgery23 | 70%over 5 years | 65-75% |
| RFA21 | 70%over 5 years | 65-75% |
HCC- hepatocellular carcinoma; LTx- liver transplant; MELD- model for end stage liver disease; RFA- radiofrequency ablation
Results
Base case scenario
Figure 2 summarizes the overall result indicating that HCC surveillance improves survival. The median survival in the surveillance cohort was 11.2 years compared to 10.4 years in the no-surveillance cohort. In Table 2, mortality from all causes at 15 years improved from 68.2% without surveillance to 64.7% with surveillance. Without surveillance, HCC was the cause of death in 25.1% and hepatic decompensation in 43.6%. In the surveillance cohort, the proportion of patients dying of HCC decreased to 17.8%, whereas that of hepatic decompensation increased to 47.1%.
Figure 2. All-cause and HCC-specific mortality.
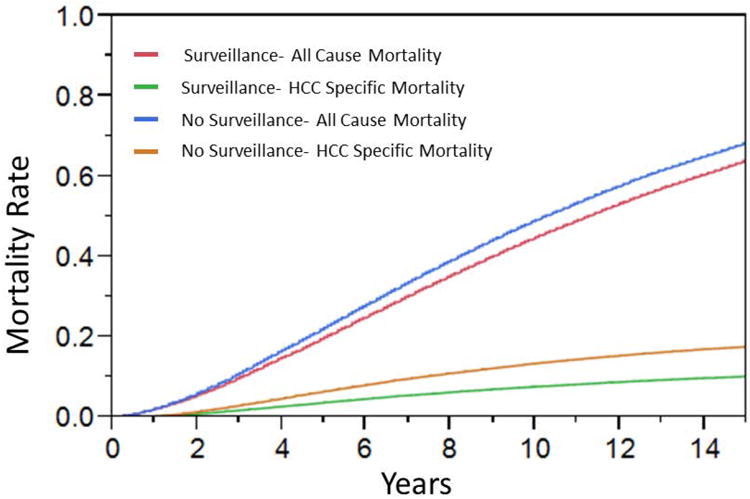
Table 2.
Effect of HCC Surveillance on Mortality, Number Needed to Treat and Absolute Risk Reduction in 3, 5,10 or 15 years.
| Mortality | NNS | Relative Risk Reduction | ||||
|---|---|---|---|---|---|---|
| Overall | HCC | Overall | HCC | Overall | HCC | |
| 3 years | 120 | 101 | 6.7% | 34.4% | ||
| No Surveillance | 12.3% | 2.9% | ||||
| Surveillance | 11.5% | 1.9% | ||||
| 5 years | 54 | 46 | 7.9% | 35.1% | ||
| No Surveillance | 23.5% | 6.2% | ||||
| Surveillance | 21.6% | 4.0% | ||||
| 10 years | 29 | 22 | 6.8% | 34.1% | ||
| No Surveillance | 50.2% | 13.1% | ||||
| Surveillance | 46.8% | 8.7% | ||||
| 15 years | 28 | 18 | 5.2% | 32.8% | ||
| No Surveillance | 68.2% | 17.1% | ||||
| Surveillance | 64.7% | 11.5% | ||||
HCC- hepatocellular carcinoma
NNS- number needed to be surveillance (in comparison to no surveillance)
Table 2 also reports NNS and relative risk reduction calculations. The NNS to reduce one death decreased progressively from three years to fifteen years. At 15 years, the NNS to avoid one HCC death was 18 and one death from all cases 28. Relative risk reduction was fairly constant regardless of the timeframe of assessment. Surveillance was associated with an approximate 30- 35% relative reduction in HCC mortality throughout. Relative reduction in overall mortality was 5.2% with surveillance at 15 years.
Model Validation
Using the model, we calculated expected survival of HCC patients according to the treatment received. Patients who received LTx had 71% of post LT survival at 5 years, whereas those who underwent resection or RFA had overall survival of 61% at 5 years, which are consistent with a general consensus of survival results reported in the literature.21-23 Patients with BCLC 0 who were treated with RFA had 5 year survival 78%, which calibrate to the result seen in the recent meta-analysis.32 Next, we evaluated the overall survival of HCC patients from the onset and diagnosis of HCC (Supplementary Figures 1 and 2, respectively). The median survival of HCC patients was longer in surveillance cohort than no surveillance cohort (3.1 years vs. 2.2 years from the time of HCC onset and 2.8 years vs. 1.4 years from the time of HCC diagnosis). The five year overall survival from HCC diagnosis was 34% with surveillance and 15% without surveillance, both of which fall well within the range of survival rates reported in the literatures.33
Competing Risks on the Effectiveness of HCC Surveillance
First, we tested a scenario where cirrhosis did not progress and thus deaths from hepatic decompensation occurred at a lower frequency than the base case scenario. In Table 3, cirrhosis remained at stage 1 throughout the follow-up, which resulted in a reduction in deaths from hepatic decompensation and an increase in HCC mortality, with a net effect of overall reduction in all-cause mortality. The NNS to prevent one death from all causes at 15 years decreased by 37% (from 28 to 18) and that from HCC by 24% (from 18 to 13).
Table 3. Sensitivity analysis: Effect of non-progression of cirrhosis stage.
| Mortality | NNS | Relative Risk Reduction | ||||
|---|---|---|---|---|---|---|
| Overall | HCC | Overall | HCC | Overall | HCC | |
| 3 years | 103 | 91 | 12.0% | 36.0% | ||
| No Surveillance | 8.1% | 3.0% | ||||
| Surveillance | 7.1% | 2.0% | ||||
| 5 years | 47 | 42 | 14.6% | 35.9% | ||
| No Surveillance | 14.6% | 6.7% | ||||
| Surveillance | 12.5% | 4.3% | ||||
| 10 years | 22 | 19 | 14.4% | 33.9% | ||
| No Surveillance | 30.9% | 15.8% | ||||
| Surveillance | 26.5% | 10.4% | ||||
| 15 years | 18 | 13 | 12.9% | 32.6% | ||
| No Surveillance | 43.9% | 22.7% | ||||
| Surveillance | 38.3% | 15.3% | ||||
HCC- hepatocellular carcinoma; LTx- liver transplant; NNT- number needed to treat; RFA- radiofrequency ablation
NNS- number needed to be surveillance (in comparison to no surveillance)
In addition, we considered a scenario where liver disease remained stable with concomitant reduction in the incidence of HCC, as would be expected in cirrhotic patients with viral hepatitis who have received effective antiviral therapy (Supplementary Table 1). As expected, all-causes and HCC specific mortality decreased compared to the base case scenario. The NNS for all-cause and HCC mortality increased – the NNS over 15 years for overall mortality increased by 57% from 28 to 44 and that for HCC mortality by 90% from 18 to 34.
Other sensitivity analyses
As expected, the annual incidence of HCC affected the effectiveness of HCC surveillance: higher annual incidence rates of HCC were associated with lower NNSs to prevent one all-cause or HCC mortality and larger relative risk reduction for all-cause mortality (Figures 3A and 4A, Supplementary Table 2 and Supplementary Figures 3A and 4A). Similarly, higher sensitivity of HCC surveillance test was associated with a larger impact of surveillance, although its magnitude was smaller than that from variability in HCC incidence. (Figures 3B and 4B, Supplementary Table 3, and Supplementary Figures 3B and 4B). It is noteworthy in Figures 3B and 4B, the impact of the sensitivity of surveillance test was very small when assessed for long term (e.g., 15 years).
Figure 3.
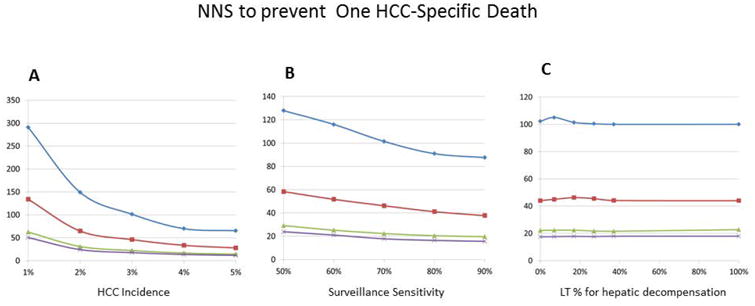
One way sensitivity analysis: Impact of HCC surveillance on NNS to avoid one death from HCC
Blue diamond- 3 year; Red square- 5 year; Green triangle-10 year ; Violet X -15 year
A: HCC incidence and NNS for HCC specific mortality (X axis- annual incidence of HCC, Y axis-NNS)
B: Surveillance test sensitivity and NNS for HCC specific mortality (X axis- surveillance sensitivity of HCC detection, Y axis-NNS)
C: Rate of rescue transplant for hepatic decompensation and NNS for HCC specific mortality (X axis- percent of rescue transplant for hepatic decompensation, Y axis-NNS)
Figure 4. One way sensitivity analysis: Impact of HCC surveillance on NNS to avoid one death from any cause.
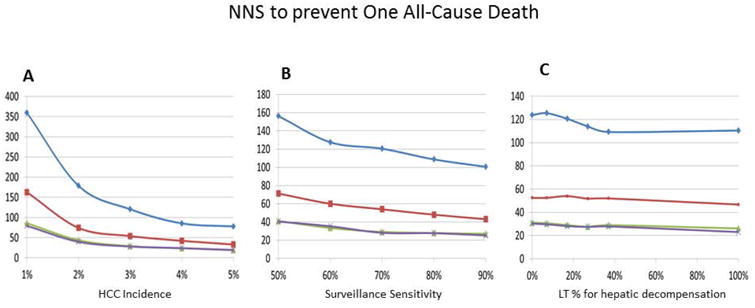
Blue diamond- 3 year; Red square- 5 year; Green triangle-10 year ; Violet X -15 year
A: HCC incidence and NNS for All-cause mortality (X axis- annual incidence of HCC, Y axis-NNS)
B: Surveillance test sensitivity and NNS for All-cause mortality (X axis- surveillance sensitivity of HCC detection, Y axis-NNS)
C: Rate of rescue transplant for hepatic decompensation and NNS for All-cause mortality (X axis- percent of rescue transplant for hepatic decompensation, Y axis-NNS)
Other variables tested had a much smaller effect on the survival benefits of HCC surveillance. For example, availability of LTx had little impact on the effectiveness of surveillance, as gauged both by NNS and relative risk reduction (Supplementary Table 4). Similarly, varying access to LTx for hepatic decompensation had little impact on the benefits of HCC surveillance (Figures 3C and 4C, Supplementary Table 5, and Supplementary Figures 3C and 4C). Lastly, other variables subjected to sensitivity analyses; namely, time to develop late stage cancer and mortality of late stage HCC had negligible impact on the overall results (data not shown).
The probabilistic sensitivity analysis (PSA) was performed to address the second order uncertainty (uncertainty around the parameters used in the base case analysis) along with first order uncertainty (patient level) (Figure 5, Supplementary Figure 5). All-cause and HCC-specific mortality reduction were above 0%, indicating there are no instances where there would be no risk reduction. For example, the median 5-year risk reduction in all-cause mortality was 7.8%. The 2.5th and 97.5th percentiles of the PSA were 3.3% and 11.4%, respectively. The median 5-year risk reduction in HCC-specific mortality 34.8%. The 2.5th and 97.5th percentiles of the PSA were 30.8% and 40.7%, respectively.
Figure 5. The probabilistic sensitivity analysis.
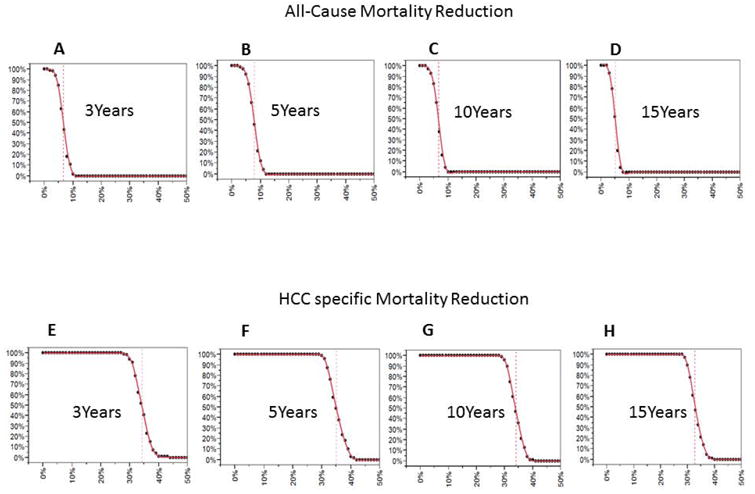
X axis-relative risk reduction of death
Y axis- Percent of the probabilistic sensitivity analysis result above the corresponding mortality reduction (X axis)
Dashed red line is base case outcome
A: All-cause death risk reduction over 3 years
B: All-cause death risk reduction over 5 years
C: All-cause death risk reduction over10 years
D: All-cause death risk reduction over 15 years
E: HCC- specific death risk reduction over 3 years
F: HCC- specific death risk reduction over 5 years
G: HCC- specific death risk reduction over 10 years
H: HCC- specific death risk reduction over 15 years
Lastly, a discounted life year analysis was performed with reducing the value of life by 3% per year. HCC surveillance offered, in the base case scenario, an increase of 0.24 life-years for a subject relative to no surveillance (discounted life years: 8.52 years vs 8.27 years). In general, it reduced the apparent benefits of surveillance in other scenarios without fundamentally altering the direction of effects (data not shown).
Discussion
In this study, we designed a multistate Markov model to investigate the survival benefit of HCC surveillance in patients with compensated cirrhosis and identify factors associated with the effectiveness of HCC surveillance in reducing mortality. In our simulated cohorts of 50-year old patients, 68% of the cohort members died after fifteen years of follow up without HCC surveillance, which decreased to 65% with surveillance. These resulted in NNS to reduce one death over 15 years of 28 for all causes and 18 for HCC. While the survival benefit in cirrhotic patients under surveillance may not be directly comparable to that in other cancer surveillance programs in otherwise healthy individuals, the NNS to avoid one cancer death has been reported to be 550 for prostate-specific antigen over 12 years of follow-up and between 233 and 746 for mammography over lifetime depending on the age of the subject.34, 35
The results of our sensitivity analyses strongly indicate that HCC surveillance remains highly effective irrespective of the factors that were taken into consideration. We did find that HCC surveillance is most effective when the risk of death from hepatic decompensation decreases, even when the incidence of HCC is also decreased. In addition, the incidence of HCC and the sensitivity of surveillance test also had a substantial impact on the benefits of surveillance. These considerations are particularly relevant today when there are increasing number of older patients with cirrhosis (e.g., HCV) in whom current and future therapies may halt or slow the progression of cirrhosis.
In order to assess the impact of HCC surveillance in cirrhotic patients, outcome should be measured from cirrhosis patients for whom surveillance is implemented, not just in a subset of cirrhotic patients who had already developed HCC. There were numerous observational studies comparing survival post-HCC diagnosis, but no observational or randomized controlled trial study specifically evaluated the impact of HCC surveillance on overall survival among cirrhotic patients from the beginning of HCC surveillance.25 A previous modeling study attempted to evaluate the impact of HCC surveillance in cirrhotic patients, but outcome was measured only in patients who had developed HCC from the time of HCC diagnosis, but not from the beginning of HCC surveillance.26 Cadier et al recently performed a cost-effectiveness analysis of HCC surveillance, but did not investigate the major determinant for effectiveness of HCC surveillance and failed to incorporate competing risk of death from hepatic decompensation.36 The contribution of our work is deeper insight of the medical effectiveness of HCC surveillance and its determinants, which would be a pre-requisite for cost-effectiveness. Similarly, we do not delve into the discussion of harms and costs associated with false-positive results. Data to date indicate that the harms associated with HCC surveillance is minimal, attributable to radiocontrast toxicity or biopsy complications. 37
The main purpose of HCC surveillance is to reduce mortality. Although a number of previous observational studies reported that HCC surveillance is associated with earlier diagnosis and increased survival, it is essentially impossible to exclude lead time (earlier detection of HCC without affecting the natural history of disease) or length (preferential detection of slowly growing HCC) biases from the data.1 So far, only two randomized controlled trials have evaluated the effect of HCC surveillance on mortality. These studies were performed in China in patients with HBV infection and showed inconsistent results. One study included 18,816 patients and showed a reduction of HCC mortality by more than a third.3 The other study, conducted in 5,581 men, failed to show statistically significant mortality reduction despite detection of HCC in an earlier stage.38
Death from hepatic decompensation is the leading causes of death and a major competing risk of HCC in cirrhotic patients. Our data suggest that if the underlying disease process can be controlled, surveillance becomes more beneficial, even in the absence of LTx. It is now well established that successful therapy of viral hepatitis in cirrhotic patients reduces the development of hepatic decompensation.39 Further, an increasing body of literature shows that effective therapy of underlying liver disease may reverse cirrhosis in the long run.40 Thus, our data suggest that HCC surveillance would be beneficial in those patients, whereas it remains unknown whether HCC surveillance should continue indefinitely in those patients. However, further data are needed to inform whether and when the risk of HCC in those patients is sufficiently lowered to warrant discontinuation of surveillance.
In our validation attempt, we were pleased to see that our multistate model seemed to replicate data reported in the literature well. In a study of 1,155 consecutive cirrhotic patients, the six-year survival rates of patients with compensated and decompensated cirrhosis without LTx were 54% and 21%, respectively.41 Most of the deaths were attributed to complications of advanced liver disease - hepatic failure in 49%, HCC in 22%, and bleeding complications in 13%. A systematic review summarizing 118 studies on the natural history of cirrhosis showed similar results - the 10-year survival of patients with compensated cirrhosis was 61%.14 In our previous cohort study, the 15-year survival of patients with Child Pugh A cirrhosis was approximately 30%.42 These data, in totality, indicate that our estimates calibrate well to real life data at the present time. Finally, previous studies consistently showed that 25-30% of deaths in cirrhotic patients were attributed to HCC, again similar to the estimates of our model.43
As with any studies based on simulation models, our data are an approximation of real life observations only to the degree that the structure and input data of the model are reflective of the best knowledge available. For example, the heterogeneity in the biological characteristics and tumor behavior of HCC are difficult to model precisely. At the same time, an important advantage of simulation analyses is that they allow sensitivity analyses assessing the impacts of various components of the model. Our results clearly show that the risk of hepatic decompensation is a major driver for the effectiveness of surveillance, whereas tumor specific variables may be much less so – which suggests that more elaborate models that take into account individual tumor biology are unlikely to change the main results. Further, simulation modeling makes it possible to analyze the long term outcomes associated with surveillance, whereas conducting a randomized trial of 15 years' duration is prohibitively costly and, to many investigators, unethical.
In conclusion, while routine implementation of HCC surveillance in cirrhotic patients remains controversial in the US, our study offers additional insights about the mortality benefits of surveillance of cirrhotic patients. HCC surveillance is most effective in preventing mortality in the setting where death from hepatic decompensation is lower, the incidence of HCC is higher and sensitivity of HCC surveillance test increases while availability of LTx had minimal impact. In all of the scenarios considered in this analysis, HCC surveillance decreases all-cause and tumor-specific mortality, which lead us to advocate that surveillance for HCC be conducted in patients with compensated cirrhosis, even if LTx is not available.
Supplementary Material
Acknowledgments
Grant support: This study was supported by the National Institutes of Diabetes and Digestive and Kidney Diseases (DK-34238, DK-92336) (to WRK) and T32 DK07198 (to JY).
Footnotes
Disclosure: There is no conflict of interest to report.
References
- 1.Yang JD, Kim WR. Surveillance for hepatocellular carcinoma in patients with cirrhosis. Clin Gastroenterol Hepatol. 2012;10:16–21. doi: 10.1016/j.cgh.2011.06.004. [DOI] [PubMed] [Google Scholar]
- 2.Yang JD, Harmsen WS, Slettedahl SW, et al. Factors that affect risk for hepatocellular carcinoma and effects of surveillance. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2011;9:617–23 e1. doi: 10.1016/j.cgh.2011.03.027. [DOI] [PubMed] [Google Scholar]
- 3.Zhang BH, Yang BH, Tang ZY. Randomized controlled trial of screening for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2004;130:417–22. doi: 10.1007/s00432-004-0552-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020–2. doi: 10.1002/hep.24199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. Journal of hepatology. 2012;56:908–43. doi: 10.1016/j.jhep.2011.12.001. [DOI] [PubMed] [Google Scholar]
- 6.Omata M, Lesmana LA, Tateishi R, et al. Asian Pacific Association for the Study of the Liver consensus recommendations on hepatocellular carcinoma. Hepatology international. 2010;4:439–74. doi: 10.1007/s12072-010-9165-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.NCI. https://www.cancer.gov/types/liver/hp/liver-screening-pdq#section/_1.
- 8.Poustchi H, Farrell GC, Strasser SI, et al. Feasibility of conducting a randomized control trial for liver cancer screening: is a randomized controlled trial for liver cancer screening feasible or still needed? Hepatology. 2011;54:1998–2004. doi: 10.1002/hep.24581. [DOI] [PubMed] [Google Scholar]
- 9.Ascha MS, Hanouneh IA, Lopez R, et al. The incidence and risk factors of hepatocellular carcinoma in patients with nonalcoholic steatohepatitis. Hepatology. 2010;51:1972–8. doi: 10.1002/hep.23527. [DOI] [PubMed] [Google Scholar]
- 10.Lin CW, Lin CC, Mo LR, et al. Heavy alcohol consumption increases the incidence of hepatocellular carcinoma in hepatitis B virus-related cirrhosis. J Hepatol. 2013;58:730–5. doi: 10.1016/j.jhep.2012.11.045. [DOI] [PubMed] [Google Scholar]
- 11.Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10:25–34. doi: 10.1016/S1470-2045(08)70285-7. [DOI] [PubMed] [Google Scholar]
- 12.Yang JD, Ahmed Mohammed H, Harmsen WS, et al. Recent Trends in the Epidemiology of Hepatocellular Carcinoma in Olmsted County, Minnesota: A US Population-based Study. J Clin Gastroenterol. 2017;51:742–748. doi: 10.1097/MCG.0000000000000810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.O'Malley ME, Takayama Y, Sherman M. Outcome of small (10-20 mm) arterial phase-enhancing nodules seen on triphasic liver CT in patients with cirrhosis or chronic liver disease. Am J Gastroenterol. 2005;100:1523–8. doi: 10.1111/j.1572-0241.2005.41814.x. [DOI] [PubMed] [Google Scholar]
- 14.D'Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. Journal of hepatology. 2006;44:217–31. doi: 10.1016/j.jhep.2005.10.013. [DOI] [PubMed] [Google Scholar]
- 15.Kim WR, Lake JR, Smith JM, et al. OPTN/SRTR 2015 Annual Data Report: Liver. Am J Transplant. 2017;17(Suppl 1):174–251. doi: 10.1111/ajt.14126. [DOI] [PubMed] [Google Scholar]
- 16.Mulier S, Mulier P, Ni Y, et al. Complications of radiofrequency coagulation of liver tumours. Br J Surg. 2002;89:1206–22. doi: 10.1046/j.1365-2168.2002.02168.x. [DOI] [PubMed] [Google Scholar]
- 17.Rhim H, Yoon KH, Lee JM, et al. Major complications after radio-frequency thermal ablation of hepatic tumors: spectrum of imaging findings. Radiographics. 2003;23:123–34. doi: 10.1148/rg.231025054. discussion 134-6. [DOI] [PubMed] [Google Scholar]
- 18.Ikai I, Arii S, Kojiro M, et al. Reevaluation of prognostic factors for survival after liver resection in patients with hepatocellular carcinoma in a Japanese nationwide survey. Cancer. 2004;101:796–802. doi: 10.1002/cncr.20426. [DOI] [PubMed] [Google Scholar]
- 19.Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology. 1999;30:1434–40. doi: 10.1002/hep.510300629. [DOI] [PubMed] [Google Scholar]
- 20.Zhou XD, Tang ZY, Yang BH, et al. Experience of 1000 patients who underwent hepatectomy for small hepatocellular carcinoma. Cancer. 2001;91:1479–86. doi: 10.1002/1097-0142(20010415)91:8<1479::aid-cncr1155>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 21.Kim YS, Lim HK, Rhim H, et al. Ten-year outcomes of percutaneous radiofrequency ablation as first-line therapy of early hepatocellular carcinoma: analysis of prognostic factors. J Hepatol. 2013;58:89–97. doi: 10.1016/j.jhep.2012.09.020. [DOI] [PubMed] [Google Scholar]
- 22.Mehta N, Heimbach J, Harnois DM, et al. Validation of a Risk Estimation of Tumor Recurrence After Transplant (RETREAT) Score for Hepatocellular Carcinoma Recurrence After Liver Transplant. JAMA Oncol. 2016 doi: 10.1001/jamaoncol.2016.5116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tabrizian P, Jibara G, Shrager B, et al. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann Surg. 2015;261:947–55. doi: 10.1097/SLA.0000000000000710. [DOI] [PubMed] [Google Scholar]
- 24.census. https://www.census.gov/compendia/statab/2012/tables/12s0107.pdf, 2012
- 25.Singal AG, Pillai A, Tiro J. Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta-analysis. PLoS Med. 2014;11:e1001624. doi: 10.1371/journal.pmed.1001624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mourad A, Deuffic-Burban S, Ganne-Carrie N, et al. Hepatocellular carcinoma screening in patients with compensated hepatitis C virus (HCV)-related cirrhosis aware of their HCV status improves survival: a modeling approach. Hepatology. 2014;59:1471–81. doi: 10.1002/hep.26944. [DOI] [PubMed] [Google Scholar]
- 27.Trinchet JC, Chaffaut C, Bourcier V, et al. Ultrasonographic surveillance of hepatocellular carcinoma in cirrhosis: a randomized trial comparing 3- and 6-month periodicities. Hepatology. 2011;54:1987–97. doi: 10.1002/hep.24545. [DOI] [PubMed] [Google Scholar]
- 28.Goldberg D, French B, Newcomb C, et al. Patients With Hepatocellular Carcinoma Have Highest Rates of Wait-listing for Liver Transplantation Among Patients With End-Stage Liver Disease. Clin Gastroenterol Hepatol. 2016;14:1638–1646.e2. doi: 10.1016/j.cgh.2016.06.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Maddala YK, Stadheim L, Andrews JC, et al. Drop-out rates of patients with hepatocellular cancer listed for liver transplantation: outcome with chemoembolization. Liver Transpl. 2004;10:449–55. doi: 10.1002/lt.20099. [DOI] [PubMed] [Google Scholar]
- 30.Salvalaggio PR, Felga GE, Guardia BD, et al. Time of Dropout From the Liver Transplant List in Patients With Hepatocellular Carcinoma: Clinical Behavior According to Tumor Characteristics and Severity of Liver Disease. Transplant Proc. 2016;48:2319–2322. doi: 10.1016/j.transproceed.2016.06.013. [DOI] [PubMed] [Google Scholar]
- 31.Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015;35:2155–66. doi: 10.1111/liv.12818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cucchetti A, Piscaglia F, Cescon M, et al. Cost-effectiveness of hepatic resection versus percutaneous radiofrequency ablation for early hepatocellular carcinoma. J Hepatol. 2013;59:300–7. doi: 10.1016/j.jhep.2013.04.009. [DOI] [PubMed] [Google Scholar]
- 33.Altekruse SF, McGlynn KA, Dickie LA, et al. Hepatocellular carcinoma confirmation, treatment, and survival in surveillance, epidemiology, and end results registries, 1992-2008. Hepatology. 2012;55:476–82. doi: 10.1002/hep.24710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hendrick RE, Helvie MA. Mammography screening: a new estimate of number needed to screen to prevent one breast cancer death. AJR Am J Roentgenol. 2012;198:723–8. doi: 10.2214/AJR.11.7146. [DOI] [PubMed] [Google Scholar]
- 35.Loeb S, Vonesh EF, Metter EJ, et al. What is the true number needed to screen and treat to save a life with prostate-specific antigen testing? J Clin Oncol. 2011;29:464–7. doi: 10.1200/JCO.2010.30.6373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cadier B, Bulsei J, Nahon P, et al. Early detection and curative treatment of hepatocellular carcinoma: A cost-effectiveness analysis in France and in the United States. Hepatology. 2017;65:1237–1248. doi: 10.1002/hep.28961. [DOI] [PubMed] [Google Scholar]
- 37.Atiq O, Tiro J, Yopp AC, et al. An assessment of benefits and harms of hepatocellular carcinoma surveillance in patients with cirrhosis. Hepatology. 2017;65:1196–1205. doi: 10.1002/hep.28895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Chen JG, Parkin DM, Chen QG, et al. Screening for liver cancer: results of a randomised controlled trial in Qidong, China. J Med Screen. 2003;10:204–9. doi: 10.1258/096914103771773320. [DOI] [PubMed] [Google Scholar]
- 39.van der Meer AJ, Veldt BJ, Feld JJ, et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. Jama. 2012;308:2584–93. doi: 10.1001/jama.2012.144878. [DOI] [PubMed] [Google Scholar]
- 40.Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet. 2013;381:468–75. doi: 10.1016/S0140-6736(12)61425-1. [DOI] [PubMed] [Google Scholar]
- 41.D'Amico G, Morabito A, Pagliaro L, et al. Survival and prognostic indicators in compensated and decompensated cirrhosis. Digestive diseases and sciences. 1986;31:468–75. doi: 10.1007/BF01320309. [DOI] [PubMed] [Google Scholar]
- 42.Zhang X, Harmsen WS, Mettler TA, et al. Continuation of metformin use after a diagnosis of cirrhosis significantly improves survival of patients with diabetes. Hepatology. 2014;60:2008–16. doi: 10.1002/hep.27199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.D'Amico G, Pasta L, Morabito A, et al. Competing risks and prognostic stages of cirrhosis: a 25-year inception cohort study of 494 patients. Aliment Pharmacol Ther. 2014;39:1180–93. doi: 10.1111/apt.12721. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.