

Abstract
Background:
Burr-hole irrigation surgery is now recognized as a widespread simple technique for the treatment of chronic subdural hematoma (CSDH). However, recurrence of CSDH is sometimes experienced after initial surgery. Recently, it has been reported that goreisan is effective in preventing CSDH recurrence.
Materials and Methods:
Methods: We studied patients with CSDH who received burr-hole irrigation at our hospital between January 2011 and December 2014. We divided these patients into three groups. The first group was given goreisan during the early phase after burr-hole irrigation. The second group was given goreisan when there was a visual tendency of recurrence, as observed in the course of computed tomography imaging for outpatients. The third group was not given any drug.
Results:
The recurrence rate was compared between each group. The recurrence rate was significantly lower in the early goreisan administration group (5% vs. 12%, P = 0.046). There was a decreased tendency of recurrence in the goreisan-administered group compared with the group that was not administered any drug, but this was not statistically different (6.1% vs. 12%, P = 0.082). The recurrence period in the goreisan-administered group was longer than that in the group that was not administered any drug (39.9 ± 12.1 vs. 27.45 ± 8.5, P = 0.017).
Conclusions:
Goreisan is effective in preventing recurrence of CSDH after burr-hole irrigation.
Keywords: Chronic subdural hematoma, goreisan, Kampo, recurrence
Introduction
Goreisan is a Japanese traditional herbal medicine that comprises five herbs (Alismatis rhizoma, Atractylodis rhizoma, Polyporus, Poria, and Cinnamomi cortex) and is used to treat nausea, dry mouth, edema, headache, and dizziness. It has been reported that one of the important effects of goreisan is its diuretic action, particularly if there is an excess of water in the body.
Burr-hole irrigation surgery is now a widespread simple technique for the treatment of chronic subdural hematoma (CSDH). However, CSDH recurrence is sometimes experienced after the initial surgery.
As the use of computed tomography (CT) and magnetic resonance imaging is widespread, the chances of detecting asymptomatic or preliminary CSDH are increasing. Moreover, 2.8%–21% of such mild cases are cured without any treatment.[1] Because the use of surgical treatment or hospitalization is hesitated in most mild cases in the elderly patients, it is very important to establish effective conservative treatment or treatment for preventing CSDH recurrence.[2] Furthermore, studies have suggested that the recurrence rate of CSDH is 9.2%–26.5% after surgery.[3]
Recently, it has been reported that goreisan is effective in preventing recurrence of CSDH.[1,2,4,5,6] However, these studies comprised only either a small number of cases or lacked statistical differences.[1,2,4,5]
In our hospital, burr-hole irrigation has been performed on symptomatic CSDH cases, and goreisan was administered after surgery when the risk of recurrence was considered to be high, as dictated by insufficient subdural space shrinkage after burr-hole irrigation. Moreover, in cases where goreisan was not initially used, it was administered when the tendency of recurrence was suddenly observed in a follow-up CT image.
We retrospectively evaluated the effects of goreisan in preventing recurrence of CSDH after burr-hole irrigation.
Materials and Methods
We retrospectively studied patients who underwent burr-hole surgery for CSDH between January 2011 and December 2014. We performed burr-hole irrigation for 306 cases in the total, including recurrent cases. We proved CSDH by head CT. Burr-hole irrigation was performed for symptomatic CSDH cases such as headache, vertigo, hemiparesis, mental decrease, and so on. About 4 cm scalp incision was made over the hematoma site, and the periosteal membrane was stripped off. Single burr hole, 1 cm diameter was made using a high-speed drill. Hematoma drainage was put in the subdural space after dural and hematoma membrane incisions. Aspirating hematoma and irrigating cavity by physiological saline were performed up to 1 L. CT was checked in postoperative day 1, 6, approximately 1 month, and every 1 month until subdural space was disappeared, or stable. Tendency of the recurrence was defined as the expansion of the subdural space or increase of the hematoma density compared to the last follow-up CT. Reoperation was performed when the symptoms and signs attribute to CSDH occurred. Patient data consisted of the following information: age, sex, anamnesis, prescription, recurrence, term from operation to recurrence, usage of goreisan, term from operation to administration of goreisan, and term of follow-up as an outpatient.
We divided this population into three groups [Figure 1]. The first group was given goreisan during the early phase after burr-hole irrigation (Group A). The second group was given goreisan when a tendency of recurrence was observed during CT imaging on follow-up (Group B). The third group was not given any drug (Group C). Goreisan was administered 7.5 g t.i.d. orally.
Figure 1.
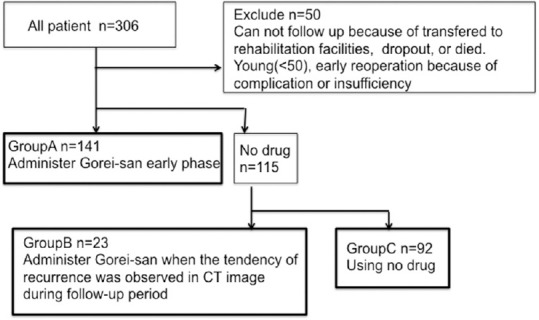
Flow chart showing stratification of patients into three groups and usage of goreisan
The recurrence rate and the term from operation to reoperation were compared for each group. Data were presented as means ± standard deviation or medians (interquartile range) for continuous variables and numbers (percentage) for categorical variables. Chi-square test (Fisher's exact test was used when the expected cell frequency was <5) and Student's t-test for continuous variables were used for statistical analysis. Statistical significance was considered as P < 0.05.
Results
Of 306 cases, fifty cases were excluded, and thus we evaluated 256 cases. Thirty-one cases could not be followed up because of transfer to rehabilitation facilities or had not returned as an outpatient. Five cases died during the early phase after surgery. Four cases were younger than 50 years old, and ten cases needed prompt repeat surgery because of operative complications such as acute subdural hematoma (SDH) or insufficient hematoma irrigation. A summary of the patients in this study is presented in Table 1 and of the recurrent cases is presented in Table 2. The mean age of individuals in this study was 75.2 ± 10.8, and 187 (3.4%) of them were male. The mean follow-up period was 71.8 ± 44.4 days, and the number of recurrent cases was 21 (8.2%). There were no statistically significant differences in patient characteristics between each group.
Table 1.
Summary of the patient characteristics
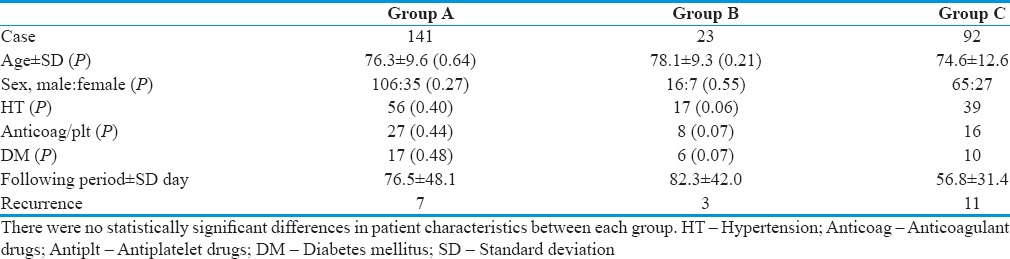
Table 2.
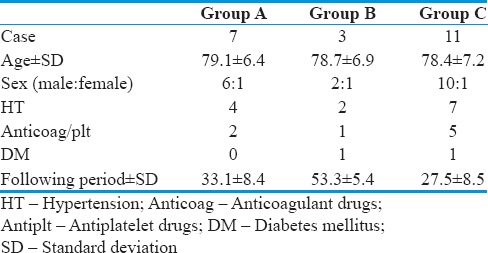
Summary of the recurrent case characteristic
The recurrence rate was significantly lower in the early goreisan administration group (Group A) (5% vs. 12%, P = 0.046) [Figure 2]. There was a decreased tendency for recurrence in the goreisan-administered group (A + B) compared with the group that was not administered any drug (C), but this was not statistically different (6.1% vs. 12%, P = 0.082) [Figure 2]. The recurrence period was significantly longer in the goreisan-administered group (A + B) than that in the group that was not administered any drug (C) (39.9 ± 12.1 vs. 27.45 ± 8.5, P = 0.017) [Figure 3].
Figure 2.
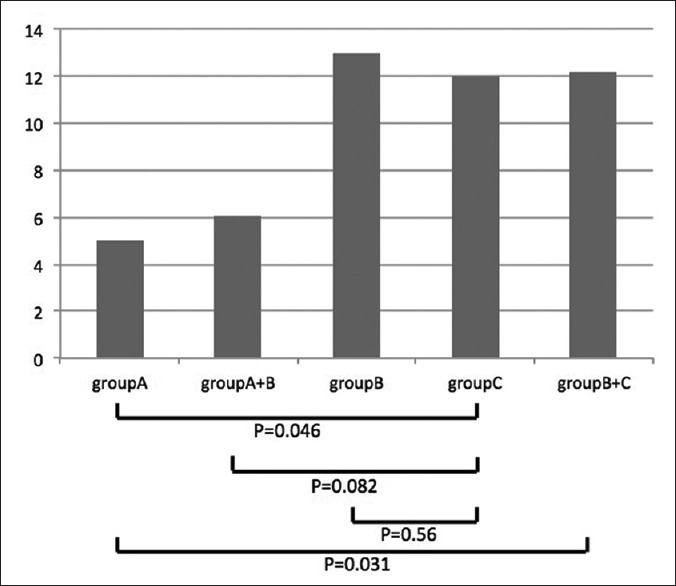
Comparison of recurrence rate of chronic subdural hematoma. Recurrence rate was significantly lower in the early goreisan administration group (Group A). There was a decreased tendency of recurrence in the goreisan-administered group (A + B) compared with the group that was not given any drug (C), but this was not statistically different
Figure 3.
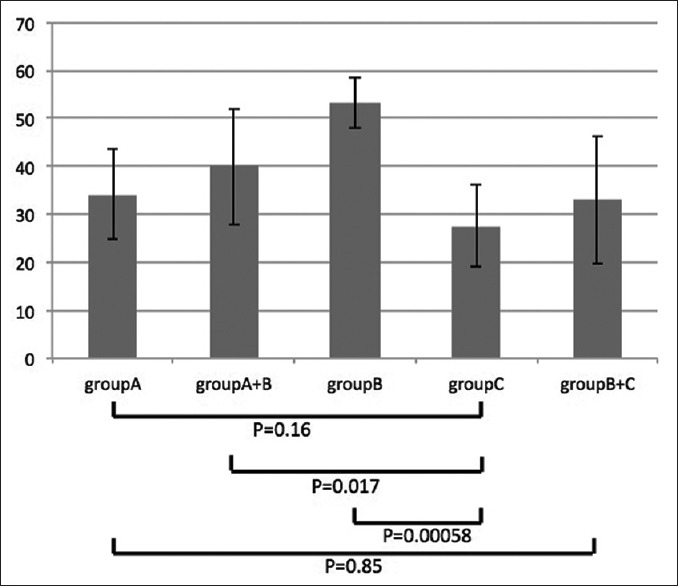
Comparison of the recurrence period of chronic subdural hematoma. Recurrence period was significantly longer in the goreisan-administered group (A + B) than that in the group that was not administered any drug (C)
No side effects of goreisan were reported.
Representative case presentation
Case 1
A 76-year-old female presented with right hemiparesis. Initial head CT showed left CSDH, and an emergency burr-hole irrigation was performed. The cerebral hemispheres were as expanded as we expected. On postoperative day 1, administration of goreisan was started in the early phase after surgery because we observed a tendency for recurrence. SDH gradually decreased, and her CT was normal on day 23 [Figure 4].
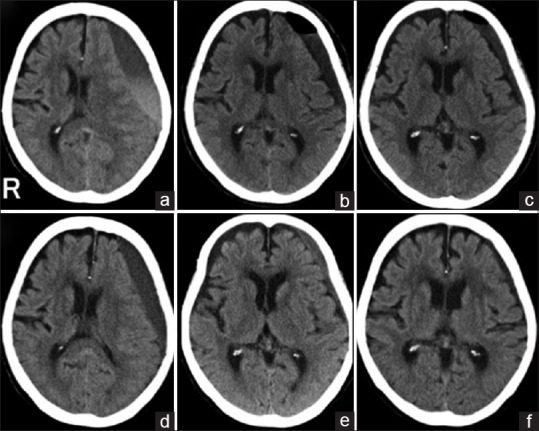
Figure 4.
Head computed tomography scan showing the therapeutic course of left subdural hematoma. (a) Initial computed tomography before burr-hole irrigation, (b) day 1 postoperation, cerebral hemispheres were not expanded as we expected; thus administration of goreisan was started, (c) day 7, subdural space gradually shrunk over time, (d) day 23, chronic subdural hematoma disappeared
Case 2
An 86-year-old female presented with right hemiparesis. Initial head CT showed left CSDH, and an emergency burr-hole irrigation was performed. The subdural space shrank to expected levels. However, a tendency for recurrence was quickly observed in a follow-up CT, and administration of goreisan was started on postoperative day 47. SDH gradually decreased and completely disappeared by day 152 [Figure 5].
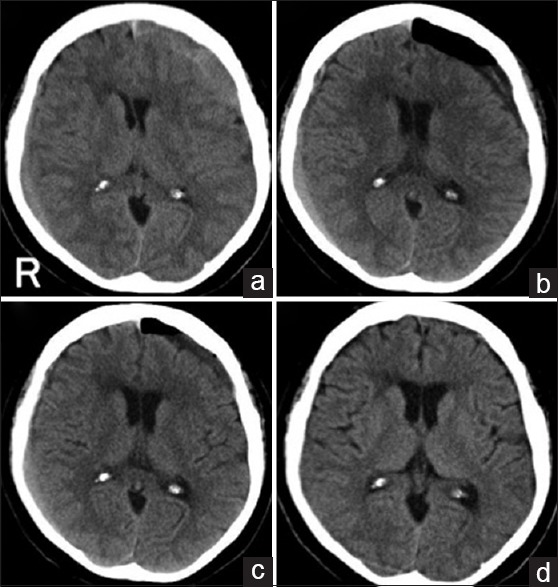
Figure 5.
Head computed tomography scan showing therapeutic course of left subdural hematoma. (a) Initial computed tomography before burr-hole irrigation, (b) computed tomography postoperative day 1, subdural space shrunk over time, (c) day 5, (d) day 47, the tendency of recurrence was rapidly shown by computed tomography, and goreisan was immediately started, (e) day 110, (f) day 152, computed tomography confirms final disappearance
Discussion
Several treatments have been shown to be useful in the treatment of CSDH such as etizolam, ibudilast, steroids, mannitol, and glycerol. These are reported to be infused as an adjunctive therapy to surgery or as conservative therapy in patients eligible for surgery.[7] However, they are far from well established, and there are currently no established conservative therapies. Some reports have referred to the effectiveness of goreisan for conservative therapy or preventing recurrence of CSDH.[1,2,4,5,6]
The mechanism by which goreisan prevents recurrence of CSDH may be explained by a mechanism of hydrostatic modulation through the aquaporin-4 (AQP4). AQP4 is the major water channel for fluid transport in the central nervous system and increases the water permeability of cell membranes.[4] AQP4 plays an integral role in the pathogenesis of brain edema.[8] A previous study showed that AQP4 was expressed on the outer membrane of CSDH.[9] Moreover, it caused excessive fluid leakage into the subdural space leading to hematoma development.
Goreisan inhibits AQP4, which is expressed on the outer membrane of CSDH.[1,10]
The etiology and development of CSDH are incompletely understood. Head injury causes arachnoid tearing and traumatic subdural effusion. It facilitates the formation of the outer membrane of CSDH. Consequently, outer membrane inflammation forms internal capillaries or sinusoids. These fenestrated blood vessels allow plasma fluid leakage into the resultant enlarged subdural space. Bleeding occurs repeatedly from capillaries with degenerating endothelium, which is one of the causes of developing CSDH.[11]
The same mechanisms are assumed to occur in recurrence of CSDH. Goreisan may inhibit effusion from the CSDH outer membrane during early phase after burr-hole irrigation and modulate the osmosity of the hematoma, thus resulting in prevention of recurrent CSDH.[5]
Most of the previous clinical studies assessing the use of goreisan to treat CSDH were small case series with no control group or no significant difference.[4] Moreover, most of these studies were published in Japanese language journals. A summary of the journal type is shown in Table 3. One report was a nationwide clinical setting, using a Japanese diagnosis procedure combination (DPC) inpatient database. This study suggested that goreisan was statistically effective in preventing recurrence of CSDH. However, DPC does not include detailed clinical data or a detailed procedure of the operation. Therefore, it is possible that many recurrent cases included the cases that were recurrent because irrigation was insufficient. Moreover, the usage and duration of goreisan treatment were not established.
Table 3.
Literature used to assess goreisan treatment for chronic subdural hematoma

In our study, the recurrence rate was significantly lower in the early goreisan administration group compared with the group that was not administered any drug. Our study shows that the inflammation during the early phase after burr-hole irrigation is responsible for recurrence of CSDH and that goreisan can inhibit this inflammation.
Recently, in a Japanese journal, it has been reported that goreisan is effective in preventing recurrence of CSDH. However, this study comprised only a small number of cases and lacked statistical difference. Therefore, this is the first study which demonstrates the effectiveness of goreisan statistically in preventing CSDH by retrospective comparison with a control group.
This study has several limitations. First, this study does not refer to the size of hematoma or the initial pressure of the hematoma. Second, there are no studies based on randomized controlled trials, which are necessary for truly establishing the effectiveness of goreisan in preventing recurrence of CSDH.
Conclusions
Early administration of goreisan after burr-hole irrigation is effective in preventing recurrence of CSDH.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Miyagami M, Kagawa Y. Effectiveness of Kampo medicine Gorei-san for chronic subdural hematoma. No Shinkei Geka. 2009;37:765–70. [PubMed] [Google Scholar]
- 2.Muramatsu M, Yoshikawa T, Hanabusa K. Effectiveness of Kampo medicine Gorei-san-ryo for chronic subdural hematoma in very elderly patients. No Shinkei Geka. 2005;33:965–9. [PubMed] [Google Scholar]
- 3.Abouzari M, Rashidi A, Rezaii J, Esfandiari K, Asadollahi M, Aleali H, et al. The role of postoperative patient posture in the recurrence of traumatic chronic subdural hematoma after burr-hole surgery. Neurosurgery. 2007;61:794–7. doi: 10.1227/01.NEU.0000298908.94129.67. [DOI] [PubMed] [Google Scholar]
- 4.Okamura A, Kawamoto Y, Sakoda E, Murakami T, Hara T. Evaluation of recurrence factors and Gorei-san administration for chronic subdural hematoma after percutaneous subdural tapping. Hiroshima J Med Sci. 2013;62:77–82. [PubMed] [Google Scholar]
- 5.Wakabayashi Y, Yamashita M, Asano T, Yamada A, Kenai H, Kondoh Y, et al. Effect of Gorei-san with tranexamic acid for preventing recurrence of chronic subdural hematoma. No Shinkei Geka. 2012;40:967–71. [PubMed] [Google Scholar]
- 6.Yasunaga H. Effect of Japanese herbal Kampo medicine goreisan on reoperation rates after burr-hole surgery for chronic subdural hematoma: Analysis of a national inpatient database. Evid Based Complement Alternat Med. 2015;2015:817616. doi: 10.1155/2015/817616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sakakibara F, Tsuzuki N, Uozumi Y, Nawashiro H, Shima K. Chronic subdural hematoma – Recurrence and prevention. Brain Nerve. 2011;63:69–74. [PubMed] [Google Scholar]
- 8.Taussky P, Fandino J, Landolt H. Number of burr holes as independent predictor of postoperative recurrence in chronic subdural haematoma. Br J Neurosurg. 2008;22:279–82. doi: 10.1080/02688690701818885. [DOI] [PubMed] [Google Scholar]
- 9.Markwalder TM, Steinsiepe KF, Rohner M, Reichenbach W, Markwalder H. The course of chronic subdural hematomas after burr-hole craniostomy and closed-system drainage. J Neurosurg. 1981;55:390–6. doi: 10.3171/jns.1981.55.3.0390. [DOI] [PubMed] [Google Scholar]
- 10.Sun TF, Boet R, Poon WS. Non-surgical primary treatment of chronic subdural haematoma: Preliminary results of using dexamethasone. Br J Neurosurg. 2005;19:327–33. doi: 10.1080/02688690500305332. [DOI] [PubMed] [Google Scholar]
- 11.Mori K, Maeda M. Surgical treatment of chronic subdural hematoma in 500 consecutive cases: Clinical characteristics, surgical outcome, complications, and recurrence rate. Neurol Med Chir (Tokyo) 2001;41:371–81. doi: 10.2176/nmc.41.371. [DOI] [PubMed] [Google Scholar]