

Abstract
Health lifestyles are important for health and social identity, yet little is known about their development in early life. We use data from the Early Childhood Longitudinal Study, Kindergarten Class of 1998-99 (ECLS-K; N=8786) to track children's health lifestyles and assess a theoretical model of health lifestyle development. Latent class analyses identify health lifestyles at four time points from first to eighth grade, and multivariate models investigate their interrelationships and social contextual influences. Health lifestyles are multidimensional and dynamic, and children demonstrate distinct combinations of risks and protections. Family factors such as resources and parenting shape earlier health lifestyles, which influence later lifestyles. Results show that development and contexts drive changes in health lifestyles, as family factors decrease in influence with age while some school and peer influences appear to emerge. Policymakers and researchers interested in shaping health behaviors should consider the multidimensional and dynamic nature of health lifestyles.
Keywords: health lifestyle, health behaviors, childhood, life course, ECLS-K
Research on health has often focused on individuals' health behaviors without explicitly acknowledging their embeddedness within social structures, groups, and identities (Cockerham 2005, Link and Phelan 1995). Because health behaviors often persist over time, those developed early in life are important for understanding population health in conjunction with other approaches emphasizing institutional and distal influences (Woolf and Aron 2013). A promising theoretical lens for contextualizing health behaviors in social influences is health lifestyles (Cockerham 2005, Cockerham 2013, Frohlich, Corin and Potvin 2001). Health lifestyles are sets of interrelated health behaviors, rooted in group-based identities and shaped by social structure and human agency. A health lifestyles perspective yields distinctive policy implications. Instead of targeting single health behaviors, acknowledging that behaviors are interrelated justifies a focus on underlying lifestyles and links to social identities. Although the promise of this approach is acknowledged (Cockerham 2005, Frohlich, Corin and Potvin 2001, Prochaska, Spring and Nigg 2008), there are substantial gaps in empirical understandings of health lifestyles. Very little is known about their formation and change in early life; we have found no longitudinal studies of health lifestyles among children and very little focus on middle childhood or early adolescence.
Childhood is important for studying health lifestyles because of its implications for later life. School readiness—cognition, behavior, and health (Crosnoe 2006, Entwisle, Alexander and Olson 2004)—is influenced by early childhood health lifestyles [author citation 2014]. In turn, children's early development predicts adolescent and adult educational and socioeconomic outcomes and health (Duncan and Magnuson 2011). Both early childhood and mid- to late adolescence are periods of change when new health behaviors emerge and become incorporated into health lifestyles. In contrast, kindergartners and middle schoolers typically engage in similar health behaviors, though their prevalence may change. This period of behavioral consistency may have life course implications as habits crystallize and lay a foundation for future behaviors.
Although health behavior types and domains remain fairly stable throughout middle childhood and early adolescence, social contexts do not. Family is the main sphere of influence for many preschoolers. With the advent of formal schooling and accompanying extensive exposure to a stable peer group, school and peers join families as major influences on development (Laible, Carlo and Raffaelli 2000, Steinberg and Silverberg 1986, Zimmer-Gembeck et al. 2003). Limited research has investigated family effects on preschoolers' health lifestyles [author citation 2014], but none has examined health lifestyles in middle childhood or early adolescence. Grounded in the life course perspective (Elder 1994), this study proposes a dynamic model that anticipates a blend of stability and change in a child's health lifestyles, likely yielding longer-term implications for individuals' developing health lifestyles.
This study has two primary aims: To describe the development of children's health lifestyles from first through eighth grade, and to understand how these lifestyles are shaped by families, peers, and schools. Using nationally representative data from the 1998-2007 Early Childhood Longitudinal Study-Kindergarten Cohort (ECLS-K), we conducted latent class analyses to model predominant health lifestyles of U.S. children. Findings preliminarily support our theoretical model of health lifestyle development, which incorporates multiple social contexts and developmental change.
Background
Health Lifestyles
Defined as “collective patterns of health-related behavior based on choices from options available to people according to their life chances” (Cockerham 2007:460), health lifestyles build on Weber's initial conceptualization of lifestyles as the interaction of life chances (structure) and life choices (agency), further developed by Sobel (1981), Abel (1991), Frohlich and colleagues (2001), Cockerham (2005), and others. Lifestyles are a manifestation of class and other social statuses, a characteristic of status groups rather than individuals, yet one's lifestyle is not fully determined by sociodemographics. By adopting a group's lifestyle, a person can communicate her/his group identity. Health lifestyles are the aspect of lifestyles that relates to health behaviors (Cockerham 2005), but as with other aspects, consumption and self-presentation are key. Beyond behaviors, health lifestyles reflect norms and understandings of the meaning of health (Krueger, Bhaloo and Rosenau 2009). Adults' health behaviors do indeed cluster in their level of healthfulness (Laaksonen, Prättälä and Lahelma 2003), and socioeconomic status (SES) and other statuses predict health lifestyles (Cockerham 2000, Mize 2017, Olson, Hummer and Harris 2017). Studying California adolescents, Mistry and colleagues (2009) found that clusters of health behaviors within individuals were sometimes consistently healthy or unhealthy and sometimes internally inconsistent (e.g., physically active teenagers with unhealthy dietary consumption).
Health Lifestyles in Middle Childhood and Early Adolescence
A health lifestyle is not just something an adult has. Informed by the life course perspective (Elder 1994) and ideas about cumulative advantage and disadvantage (Dannefer 2003, DiPrete and Eirich 2006), we emphasize two reasons why early health lifestyle development is important. First, because they are shaped by the previous generation yet influence future health lifestyle and socioeconomic attainment, early health lifestyles likely play a part in the intergenerational transmission of social disadvantage within families (author citation 2014, Wickrama et al. 1999). They may also be a pathway of intergenerational transmission within communities and social groups, as intergenerational continuity in health behaviors can result from parent socialization or exposure to the same social environments as one's parents (De Genna et al. 2006). Sociodemographic background and parent resources shape preschool health lifestyles, which subsequently influence children's kindergarten readiness [author citation 2014]. Thus, early childhood health lifestyles may be a pathway for intergenerational transmission of social (dis)advantage.
Second, early health lifestyles likely shape individuals' later lives. We expect people to transition gradually from the “received” health lifestyle of a young child—who has less agency to determine her own health behaviors—to the “achieved” health lifestyle of an adult—whose health lifestyle is still shaped by social structure but less often determined by others' agency [author citation 2014]. We focus here on the unknown processes through which this change happens. We call health lifestyles in middle childhood and early adolescence developing health lifestyles, which change over time as agency increases and different social contexts shape the child's circumstances.
Consistency within Children's Health Lifestyles
Our first research question asks to what extent children's health lifestyles fall along a consistent “healthfulness” continuum versus being internally inconsistent with a mix of healthy and unhealthy behaviors. Many theorists of health would predict the latter. Because a healthy body is a desirable form of capital (Williams 1995), parents are motivated to ensure that their children's lifestyles are healthy. Yet social class leaves families with different resources, knowledge, and practices (Freese and Lutfey 2011) that influence their chances of success. More powerful (e.g., higher-SES) groups also seek to create distinctions between themselves and the less advantaged (Bourdieu 1986) through lifestyles, and in particular, health lifestyles (Williams 1995). Thus, health lifestyles are shaped by the pressures of the “competitive social relations” created by social hierarchies in which different groups' definitions of healthy behaviors are socially contested (Korp 2008).
Parents are motivated to adhere to their social groups' health lifestyle norms. Parents' management of their children's health behaviors is considered a moral responsibility (McCarthy, Edwards and Gillies 2000), monitored and judged by others (Lee, Macvarish and Bristow 2010, Lee 2008). Lee identifies a strong association between good mothering and positive health behaviors. Not only the meaning of “good” parenting, but also “good” health behaviors, likely varies across social groups. Thus, a social group's norm of an appropriate childhood health lifestyle may include some behaviors that are objectively healthier and some that are not, making health lifestyles frequently complex and internally inconsistent. King, Jennings, and Fletcher (2014) found that socioeconomically advantaged parents apparently used off-label attention-deficit/hyperactivity disorder (ADHD)medication selectively to enhance children's academic achievement. Kimbro, Brooks-Gunn, and McLanahan (2011) found that young children in poorer, more disordered neighborhoods watched more television and played more outdoors than advantaged children. These examples point to internal inconsistencies in children's health lifestyles.
Health Lifestyle Development across Childhood
Our second research question asks how the composition of a child's health lifestyle changes across childhood and early adolescence. Our theoretical model (articulated in Figure 1 and assessed preliminarily here) posits that health lifestyles respond to developmental change and shifts in ecological systems. Like other social phenomena such as SES and health (DiPrete and Eirich 2006), health lifestyles may be significantly path-dependent, yet changes can set the child onto a new path. Earlier health behaviors shape later ones as behaviors become more habitual and less deliberate. Health behaviors may change with new influences or preferences, but the inertial effect of earlier health behavior patterns must be overcome. We anticipate that age-related changes—decreased adult monitoring, increased peer influence, and increased agency—make children's health lifestyles less internally consistent and less healthy over time. Compared to early childhood, when parents have considerable control over children's health behaviors, in middle childhood and early adolescence children become increasingly less monitored by parents (Steinberg and Silverberg 1986). This allows them to move toward the interplay of agency and structure that characterizes adults' health lifestyles (Cockerham 2013).
Figure 1. Theoretical Model of Children's Developing Health Lifestyles.
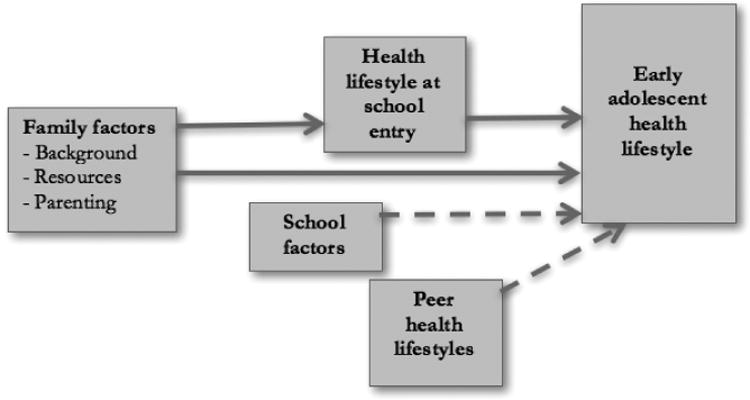
___ Pathway supported by findings
- - - Pathway suggestively supported by findings
Besides SES, other social characteristics such as race, ethnicity, and gender likely shape the social groups whose norms influence children's health lifestyles and the content of those norms. Thus, we expect them to shape the child's health lifestyle development across childhood. Huh and colleagues (2011) found among California fourth graders that gender, ethnicity, and social class differentiated clusters of physical activity and dietary behaviors. Similar relationships were found among adolescents by Mistry et al. (2009). We found no studies that examined developmental change in these relationships. We anticipate that the influences of SES, race/ethnicity, and gender on children's health lifestyles change as children grow and as these social characteristics shape their school and peer group selection and social identities.
Changing Social Contexts and Children's Health Lifestyles
Our third and final research question asks whether peer and school influences join family influences in predicting developing health lifestyles. The social ecologies surrounding children (Bronfenbrenner 1979) change across age with probable implications for health lifestyles. Beyond sociodemographic characteristics such as SES and race/ethnicity, other family factors are expected to shape children's health lifestyles throughout the period (see Figure 1). [Author citation 2014] found that family social disadvantage and low resources predicted compromised health lifestyles among preschoolers. We also expect parenting practices unrelated to health behaviors to affect children's health lifestyles. Parents who engage in more educationally enriching activities with their children may more actively shape their health behaviors, and a warm parent-child relationship may yield more successful parental influence over children's health behaviors.
We expect school and peer influences to increasingly shape health lifestyles across middle childhood as family influences decrease (see Figure 1). Schools and peers join families during this developmental period as major spheres of influence on children's behavior. Schools serve both as arenas for peer interaction (see below) and as institutions that shape children's lives. Schools' racial/ethnic and socioeconomic composition influences peer interactions and student-teacher and student-administrator interactions (Diamond, Randolph and Spillane 2004, Entwisle, Alexander and Olson 2004). Because health lifestyles are classed and raced, exposure to more peers and adults from a specific class or racial group should shape children's health behaviors. Mollborn, Domingue, and Boardman (2014a, 2014b) found that peer interactions, school-level norms, and school sociodemographic characteristics shaped teenagers' sexual behaviors.
Schools are a primary site of peer interaction in middle childhood. Like parents, peers may function as social models, set social norms, shape behaviors through facilitating or impeding behavioral opportunities, and serve as “others” whom individuals try to please (Fitzgerald, Fitzgerald and Aherne 2012, Salvy et al. 2012). Prior research has found that peers shape children's and adolescents' health behaviors(de la Haye et al. 2011, Flay et al. 1994, Pedersen, Grønhøj and Thøgersen 2015). Our study examines multiple health behaviors and longitudinally models multiple social influences across middle childhood, permitting a comparison of their influences on health lifestyles at different ages.
Data and Methods
Data
We analyzed data using the ECLS-K Class of 1998-1999, which provides longitudinal information on the cognitive, social, emotional, and physical development of a nationally representative sample of U.S. kindergartners (Tourangeau et al. 2009). It collected information from 21,260 kindergartners in the fall of 1998, with follow-ups in the spring of kindergarten (1999), the fall (1999) and spring (2000) of first grade, and the springs of third (2002), fifth (2004), and eighth grades (2007). ECLS-K's multistage probability sample design selected geographic regions, schools within regions, and children within schools. Assessors collected information from children in schools, parents completed telephone interviews, and teachers and administrators completed paper questionnaires. For more detail, see https://nces.ed.gov/ecls/kinderdataprocedure.asp. We used four spring waves (first, third, fifth, and eighth grade).
Measuring Children's Health Lifestyles
Theoretical developments in health lifestyles have outpaced their measurement. Health lifestyles should emerge from data rather than being determined a priori, an empirical challenge that has long been recognized (Abel 1991, Cockerham 2005). Many health researchers have used latent class analyses, which inductively identify empirical clusters of health behaviors within individuals and can be used to model correlates and consequences of these patterns (see McAloney et al. 2013 for a discussion). Some researchers have considered multiple health behaviors without an explicit health lifestyles approach (Leventhal, Huh and Dunton 2014, Mistry et al. 2009, Patnode et al. 2011, Skalamera and Hummer 2016), while others have used a health lifestyles framework (De Vries et al. 2008, Krueger, Bhaloo and Rosenau 2009 Mize 2017). Nearly all have focused on adults. One study has analyzed health lifestyles in early childhood [author citation 2014], and another has studied fourth-graders' diet and physical exercise (Huh et al. 2011), but we found no research focusing on broad health lifestyles in middle childhood and early adolescence.
A health lifestyles approach implies that disparate health behaviors should be related within individuals (Stefansdottir and Vilhjalmsson 2007). Here we analyzed children's health behaviors in several domains that have implications for development (e.g., Bates et al. 2002, Cook et al. 2006, Glewwe, Jacoby and King 2001). The mixture of agentic and adult-directed behaviors in childhood make it challenging to decide which to include as the child's health behaviors. We chose to include all available health behaviors experienced in a child's body without adjudicating the child agency involved. We excluded health-related factors that were behaviors of a child's social context rather than experienced in her own body. For example, we included whether the child visited a doctor or was spanked but excluded whether the child's school or neighborhood had high levels of violence.
Measures
Health lifestyles
Figure 1 lays out the main groups of analysis variables. The health lifestyle measures include indicators of nutrition, health care use, sleep, safety, physical activity, and sedentary time, reported by the parent except for three child-reported eighth-grade measures (see Table 1). The measures were similar across waves, but there were some differences based on developmental changes and question wording. For nutrition, all waves measured how many days per week the child eats breakfast and dinner at a regular time (recoded as 0-4, 5, 6-7). Child food insecurity was measured in third, fifth, and eighth grade (but not first grade). Responding “sometimes true” or “often true” to “(I/We) couldn't feed ([CHILD]/the children) a balanced meal because (I/we) couldn't afford that” was coded 1 versus 0 for “never true.”
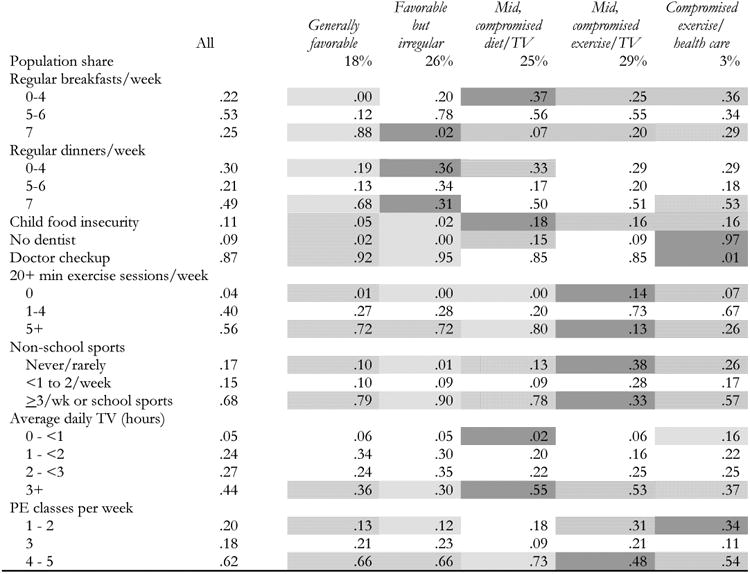
Table 1. Class-Conditional Response Probabilities from Eighth-Grade Latent Class Analyses.
|
Source: ECLS-K, 1998-2007.
Notes: N=8786. Adjusts for weighting, clustering, and strata using Wave 7 weights. Indicator means for the full population do not account for item missingness and may reflect smaller sample sizes. “Heat map” legend: Dark gray = most compromised class for that indicator; stripes = significantly (p<.05) more compromised than sample mean; checks = significantly less compromised than sample mean; light gray = least compromised class for that indicator; white = not significantly different from sample mean, or row not coded. “Compromised” designation is based on the indicator's relationship to child developmental outcomes in the literature.
For health care use, we compared those who had a well-child visit in the last year to others for all waves. The first-grade dentist measure compared three categories: went to the dentist in the last year, last dental appointment was more than a year ago, and never visited a dentist. Later waves compared the first category to the last two combined. For sleep, we measured whether the child went to bed at about the same time each night (1) or if bedtime varied (0; not available in eighth grade). For third grade, we compared parents who reported spanking their child at least once in the previous week to others.
Weekly counts of vigorous physical activity were reported by the parent in third and fifth grades and the child in eighth grade (0, 1-4, and 5-7). For third and fifth grades, parents counted the organizations (e.g., YMCA, sports teams) through which the child got exercise in the past year (0, 1, 2, or ≥3). In first grade parents reported whether the child participated in either dance or athletics, neither, or both. Eighth graders reported on sports participation, coded as: participating in no sports, non-school sports less than once a week, or either school sports or non-school sports most days. All waves (using parent reports except for child reports in eighth grade) captured hours per day of television watching based on weekday and weekend reports: (0-<1, 1-<2, 2-<3, or ≥3).
Background and controls
Child-level kindergarten control variables included child age and mother's age at survey. Social background variables (see Figure 1) included mother's age at first birth, primary household language (English versus other), child race/ethnicity (mutually exclusive categories of non-Hispanic white, non-Hispanic black, Hispanic, Asian/Pacific Islander, American Indian/Alaskan Native, and multiracial), and child gender.
Resources
We measured five household socioeconomic and social resources in kindergarten (see Figure 1). Mother's education was coded as less than high school, high school diploma, some college, college degree, and advanced degree. Income-to-needs was the ratio of the household's income to the U.S. Census-defined poverty threshold by year and household size. Dichotomous measures represented whether the mother was married and whether the child had health insurance. A continuous measure captured the number of siblings in the household.
Parenting
A count of enrichment activities measured the number of kinds of outings that someone in the household participated in with the child (to a zoo, library, concert, museum, or sporting event). The parenting scale averages responses to 13 statements asking about the parent's relations and feelings toward the child (e.g., “[CHILD] and I often have warm, close times together”; reliability=.7).
Schools and peers
ECLS-K sampled children clustered within schools in kindergarten. Over time, many students moved to different schools, resulting in less clustering with each subsequent wave. Most first graders were still clustered in schools, permitting aggregation of individual data to create school-level characteristics. These included categorical measures of school type (private [referent] or public), enrollment size, and the percentage of students who were racial or ethnic minorities. The percentage of students eligible for free or reduced-price lunch captured socioeconomic composition, and the percentage of students who tested at or above grade level for reading represented school-level academic achievement.
We examined first-grade schoolmates' health lifestyles, first measuring the proportion of students in each of the first-grade health lifestyles and then identifying which of the lifestyles was most prevalent (modal health lifestyle). To capture peers' consensus around a common health lifestyle, we also analyzed the proportion of peers who were in the school's modal health lifestyle. For example, the “generally healthy” class could be modal in a school, and the proportion of peers in that class could be 80%, indicating strong consensus.
Analysis
We conducted latent class analyses (LCA) in SAS to identify health lifestyles based on observed health behaviors at each wave. LCA uses observed variables to identify a categorical latent trait that is assumed to account for all associations between observed variables (see Collins and Lanza 2013). We chose the number of classes based on substantive interpretation and fit statistics, focusing on the Bayesian information criterion (BIC) because it penalizes model complexity more than the G2 or the Akaike information criterion (AIC; see online Appendix table A1). We prioritized the lowest BIC value; first- and fifth-grade solutions represent the lowest BIC value. The third-grade solution is within 2 points of the lowest BIC but has higher class assignment probabilities and greater substantive complexity. For eighth grade, we chose the five-class solution (the second-lowest BIC value) over the six-class solution because the latter had one very small class, lower probabilities of class assignment, and made less theoretical sense.
We examined each wave separately because we did not expect health lifestyles, or the health behaviors comprising them, to be the same at every age. Other approaches that simultaneously estimate latent classes at multiple time points constrain lifestyles to be the same at every time point. Given that we examined children from roughly ages 6 to 13, we did not want to assume that predominant health lifestyles would remain the same. Our analyses indeed produced different health lifestyle configurations at each wave.
We assigned each student the health lifestyle at each wave for which she demonstrated the highest probability of membership, then examined descriptive and multivariate associations. This “classify-analyze” approach has limitations (see Bakk, Tekle and Vermunt 2013 for critiques) but is best suited for our aim of identifying relationships across health lifestyles at different waves of data and incorporating many predictor variables. Because we conduct several sets of analyses including average marginal effects, estimating latent classes and relationships with other variables in a single step is not feasible. Perhaps of greatest concern for the classify-analyze approach is the extent to which individuals are assigned to a class in which they do not belong, known as misclassification bias. Assigning membership based on the highest probability results in the lowest average misclassification bias compared to other assignment methods (Goodman 2007). The average probability of class membership was .8 for first grade, .8 for third grade, .7 for fifth grade, and .7 for eighth grade, minimizing concerns over misclassification (Nagin 2005). Further, misclassification bias results in downward bias in associations produced by the classify-analyze approach (Bolck, Croon and Hagenaars 2004). Findings thus represent a conservative test, with actual relationships likely attenuated.
For each latent class analysis, we retained all respondents with a valid sample weight for that wave through full information maximum likelihood. Each latent class analysis thus reflects the national population for the cohort at that age. We then present patterns of health lifestyle membership for first, third, and fifth grades across eighth-grade health lifestyles, for the sample of 8786 children who had a valid weight in eighth grade. All analyses except for latent class analyses were conducted in Stata. In accordance with the software and analysis capabilities, we used multiple imputation to account for missingness.1 Multinomial logistic regressions predicted class membership in first grade based on kindergarten control and resource variables, then predicted eighth-grade class membership based on kindergarten control and resource variables, health lifestyles from previous waves, and first-grade school and peer characteristics. These latter analyses omitted students who did not participate in the first-grade wave (N=96), did not have school identifiers (N=176), or attended schools with fewer than 10 students in the survey (N=685). Results were presented as odds ratios compared to the most favorable class, with average marginal effects using MIMRGNS in Stata (Klein 2017) available in online appendices. In the multinomial models, odds ratios represent the odds for an outcome category compared to the referent outcome category associated with each variable, whereas an average marginal effect is the average of the changes in probabilities for an outcome category across all observations. An average marginal effect can therefore be interpreted as the change in probability (on a 0 to 1 scale) associated with membership (categorical variable) or an instantaneous rate of change that is similar to one unit (continuous variable). Significance is compared to all other classes combined, a notable difference from odds ratios. LCA analyses accounted for wave-specific probability weights and clustering. All other statistics accounted for probability weights, clustering, and stratification for the valid eighth-grade sample. Weights adjusted for base-year child and school nonresponse and longitudinal nonresponse (Tourangeau et al. 2009).
Results
Table 1 displays a “heat map” showing how children's eighth-grade health behaviors co-occurred in distinct latent classes representing health lifestyles. See online Appendix Tables A2-A4 for results from first, third, and fifth grades. These findings show that children's predominant health lifestyles are not uniformly represented by a single “healthfulness” dimension, but are frequently internally inconsistent. Table 1's “generally favorable” class, who had better than average health behaviors in every domain, comprised 18% of eighth graders. Just 3% was assigned to a “compromised exercise/health care” class characterized by nearly universal avoidance of doctor and dentist visits and less optimal health behaviors in every domain except television watching. A “favorable but irregular” class (26%) emerged in which many health behaviors were, if anything, more favorable than in “generally favorable,” but in which mealtimes were especially irregular. This may be related to busy children's schedules since most played sports frequently. Two mixed classes emerged that had strengths and weaknesses in contrasting domains. The “mid, compromised diet/TV” class (25%) exercised but watched television frequently and had problems with consistent nutrition. The “mid, compromised exercise/TV” class (29%) did not have many food concerns but had the lowest levels of physical activity and fairly frequent television watching.
Table 2 presents descriptive information about the characteristics of children in each eighth-grade health lifestyle. Strikingly, two pairs of eighth-grade lifestyles (“generally favorable” versus “favorable but irregular,” and “mid, compromised diet/TV” versus “mid, compromised exercise/TV”) were nearly indistinguishable within the pair on sociodemographic background (except sometimes gender), kindergarten household resources, and parenting. Thus, not everyone with the same background had the same health lifestyle; instead, complex interactions of social factors and agency apparently resulted in distinct lifestyles. Eighth graders with similar backgrounds, resources, and parenting evidenced distinct profiles of health behaviors, supporting a health lifestyles approach.
Table 2. Means of Analysis Variables for Population and by Eighth-Grade Health Lifestyle Class.
| All | Generally favorable (18%) | Favorable but irregular (26%) | Mid, compromised diet/TV (25%) | Mid, compromised exercise/TV (29%) | Compromised exercise/ health care (3%) | |
|---|---|---|---|---|---|---|
|
|
|
|||||
| Controls (Kindergarten) | ||||||
| Age in months (52-102) | 74.75 | 75.02 | 74.74 | 74.94 | 74.48 | 74.46 |
| Male | .52 | .55 | .53 | .58 | .45 | .52 |
| Race/ethnicity | ||||||
| White | .57 | .65 | .70 | .47 | .49 | .30 |
| Black | .17 | .14 | .12 | .24 | .20 | .21 |
| Hispanic | .18 | .13 | .12 | .24 | .23 | .39 |
| Asian/Pacific Islander | .04 | .04 | .03 | .03 | .04 | .04 |
| American Indian/Alaskan Native | .02 | .01 | .01 | .01 | .02 | .01 |
| Multiracial | .02 | .03 | .02 | .02 | .02 | .04 |
| Maternal age (18-83) | 33.55 | 33.95 | 34.03 | 32.80 | 33.49 | 31.98 |
| Maternal age at first birth (12-49) | 23.77 | 24.59 | 24.82 | 22.67 | 23.12 | 21.77 |
| Non-English household | .13 | .10 | .08 | .17 | .16 | .32 |
| Resources (Kindergarten) | ||||||
| Maternal education | ||||||
| Less than high school | .15 | .08 | .10 | .19 | .20 | .33 |
| High school | .29 | .25 | .25 | .34 | .32 | .30 |
| Some college | .32 | .34 | .33 | .31 | .31 | .26 |
| College degree | .18 | .25 | .23 | .12 | .12 | .09 |
| Advanced degree | .06 | .08 | .09 | .03 | .04 | .02 |
| Income-to-needs (0-75) | 2.89 | 3.40 | 3.60 | 2.24 | 2.39 | 1.69 |
| Mother married | .70 | .78 | .74 | .62 | .66 | .66 |
| No health insurance | .10 | .08 | .06 | .13 | .13 | .24 |
| # siblings (0-14) | 1.47 | 1.41 | 1.41 | 1.52 | 1.50 | 1.74 |
| Parenting measures (Kindergarten) | ||||||
| Number of activities (0-5) | 2.07 | 2.27 | 2.29 | 1.95 | 1.86 | 1.43 |
| Parenting scale (-1-3) | 1.96 | 1.98 | 1.97 | 1.93 | 1.95 | 1.87 |
Source: ECLS-K, 1998-2007.
Notes: N=8786. Accounts for complex sampling design.
Findings bolster our expectation of a blend of continuity and change in children's health lifestyles with age. Table 3 displays the mean representation of kindergarten, first-, third-, and fifth-grade health lifestyles in each of the eighth-grade health lifestyles (columns sum to 1; strong relationships highlighted). There was considerable movement between health lifestyles across ages. For example, just 50% of eighth graders in the “generally favorable” class and 43% in the “favorable but irregular” class came from the large first-grade “generally favorable” class. Those percentages fell slightly in third grade and more substantially, to 32% and 18% respectively, in fifth grade. Yet these percentages represent a meaningful relationship between children's earlier and later placement in “generally favorable” classes. The table suggests inconclusively that the “generally favorable” classes may be more regularly associated across ages than other classes.
Table 3. Means of First-, Third-, and Fifth-grade Classes by Eighth-Grade Health Lifestyle Class.
| All | Generally Favorable (18%) | Favorable but irregular (26%) | Mid, compromised diet/TV (25%) | Mid, compromised exercise/TV (29%) | Compromised exercise/ health care (3%) | |
|---|---|---|---|---|---|---|
| Panel A: First grade | ||||||
| First-grade classes | ||||||
| Generally compromised | .07 | .04 | .05 | .09 | .08 | .23 |
| Mixed | .26 | .17 | .31 | .28 | .25 | .15 |
| Generally favorable | .36 | .50 | .43 | .27 | .28 | .10 |
| Mid, compromised exercise | .17 | .17 | .10 | .18 | .23 | .29 |
| Compromised diet/sleep/TV | .15 | .12 | .11 | .18 | .17 | .23 |
|
| ||||||
| Panel B: Third grade | ||||||
| Third-grade classes | ||||||
| Compromised diet/exercise | .08 | .06 | .07 | .09 | .11 | .11 |
| Compromised health care/exercise | .08 | .05 | .04 | .11 | .10 | .26 |
| Compromised except exercise | .09 | .06 | .07 | .12 | .11 | .18 |
| Generally favorable | .39 | .49 | .37 | .36 | .39 | .20 |
| Favorable but irregular | .35 | .35 | .45 | .32 | .30 | .26 |
|
| ||||||
| Panel C: Fifth grade | ||||||
| Fifth-grade classes | ||||||
| Favorable but irregular | .46 | .47 | .57 | .41 | .39 | .30 |
| Compromised except exercise | .20 | .13 | .14 | .29 | .24 | .32 |
| Generally favorable | .20 | .32 | .18 | .14 | .20 | .12 |
| Compromised exercise/health care | .03 | .01 | .01 | .05 | .03 | .18 |
| Compromised exercise/TV | .11 | .07 | .10 | .11 | .15 | .07 |
Source: ECLS-K, 1998-2007.
Notes: N=8786. Accounts for complex sampling design (Wave 7). Means of first-grade, third-grade, and fifth-grade classes for the sample may differ from those in Tables 1 and A1 because the samples differ. Columns sum to 1. Shaded cells are both overrepresented within row and among the most prevalent within column.
Evidence suggests an overall weakening of socioeconomic disparities in health lifestyles and a strengthening of gender disparities as children grew. Tables 4 and 5 present odds ratios (compared to the “generally favorable” class) from multinomial logistic regression models that predicted first-grade (Table 4) and eighth-grade (Table 5, Model 1) health lifestyles based on sociodemographic background, household resources, and parenting. Average marginal effects, which better facilitate comparison of effects across models, appear in online Tables A5 and A6. In first grade (Table 4), maternal education negatively predicted membership in each latent class compared to “generally favorable,” with odds for a child whose mother had a high school degree or less falling between 2 and 7 times as high as for a child whose mother had a graduate degree. Average marginal effects reveal that SES had fewer significant relationships and smaller effects in eighth compared to first grade. In contrast, average marginal effects identified gender differences in eighth (significant for the two “mid” classes), but not first, grade. Table 5, Model 1 shows that the odds of being in the “mid, compromised exercise/TV” class rather than “generally favorable” decreased by a factor of one third for boys compared to girls. Average marginal effects showed no consistent trend between the two ages in racial/ethnic influences on health lifestyles, but like SES, the effects of primary household language weakened with age. Differences by language were fairly strong in first grade (significant for the three middle classes), but only one marginally significant and weaker effect emerged in eighth grade.
Table 4. Odds Ratios from Multinomial Logistic Regression Model Predicting First-Grade Classes (Referent: “Generally Favorable”).
| Generally compromised | Mixed | Mid, compromised exercise | Compromised diet/ sleep/TV | |||||
|---|---|---|---|---|---|---|---|---|
|
|
||||||||
| Controls (Kindergarten) | ||||||||
| Male | 1.02 | .95 | .86 | .96 | ||||
| Race/ethnicity (white) | ||||||||
| Black | 2.96 | *** | 1.85 | **d | 1.86 | **d | 3.87 | ***bc |
| Hispanic | 1.90 | * | 1.19 | 1.33 | 1.51 | + | ||
| Asian/Pacific Islander | 1.72 | 1.09 | cd | 1.87 | **b | 2.14 | **b | |
| American Indian | .41 | c | .62 | 1.18 | a | .67 | ||
| Multiracial | 1.89 | 1.14 | 1.16 | 1.53 | ||||
| Age | 1.02 | 1.00 | 1.01 | 1.01 | ||||
| Maternal age | .99 | 1.00 | 1.01 | 1.01 | ||||
| Maternal age at first birth | .99 | d | .98 | d | .98 | .94 | **ab | |
| Non-English household | 1.60 | +b | .73 | +acd | 2.06 | **b | 1.77 | *b |
| # siblings | 1.14 | 1.03 | 1.06 | 1.01 | ||||
| Resources (Kindergarten) | ||||||||
| Income-to-needs | .84 | * | .99 | c | .83 | ***b | .91 | + |
| Maternal education (advanced degree) | ||||||||
| Less than high school | 7.00 | **b | 2.14 | *a | 3.42 | ** | 4.81 | ** |
| High school | 4.55 | * | 1.97 | ** | 2.32 | ** | 3.33 | * |
| Some college | 2.27 | 1.32 | 1.83 | * | 1.92 | |||
| College degree | 1.27 | 1.16 | 1.14 | 1.21 | ||||
| Married | .68 | + | .75 | * | .74 | * | .72 | + |
| No health insurance | 2.52 | ***bcd | 1.33 | a | 1.44 | a | 1.31 | a |
| Parenting (Kindergarten) | ||||||||
| # activities | .73 | ***b | .88 | **acd | .77 | ***b | .77 | ***b |
| Parenting scale | .42 | ***c | .55 | **c | .81 | abd | .50 | ***c |
| Constant | .15 | 2.71 | .60 | 1.61 | ||||
Source: ECLS-K, 1998-2007.
Notes: N=8786. Accounts for complex sampling design.
p<.10
p<.05
p<.01
p<.001; two-tailed tests.
p<.05 compared to:
generally compromised
mixed
mid, compromised exercise
compromised diet/sleep/TV
Table 5. Odds Ratios from Multinomial Logistic Regression Model Predicting Eighth-Grade Classes (Referent: “GenerallyFavorable”).
| Favorable but irregular | Mid, compromised diet/TV | Mid, compromised exercise/TV | Compromised exercise/health care | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 1 | 2 | 1 | 2 | |||||||||||
| Controls (Kindergarten) | ||||||||||||||||
| Male | .91 | c | .92 | c | 1.08 | c | 1.11 | c | .65 | ***ab | .68 | ***ab | .86 | .92 | ||
| Race/ethnicity (white) | ||||||||||||||||
| Black | .75 | acd | .71 | +ac | 1.32 | b | 1.07 | b | 1.26 | b | 1.04 | b | 2.00 | b | 1.20 | |
| Hispanic | .96 | acd | .99 | acd | 1.86 | **b | 1.78 | **b | 1.82 | ** b | 1.75 | **b | 2.84 | **b | 2.21 | *b |
| Asian/Pacific Islander | .86 | .97 | .87 | .87 | 1.26 | 1.20 | 1.37 | 1.22 | ||||||||
| American Indian | 1.28 | c | 1.54 | 1.12 | c | 1.18 | c | 2.27 | ***ab | 2.33 | **a | .72 | .71 | |||
| Multiracial | .53 | *d | .52 | *d | .80 | d | .83 | d | .85 | d | .83 | d | 3.18 | +abc | 3.70 | *abc |
| Age | .98 | .98 | 1.00 | .99 | .97 | * | .97 | * | .98 | .96 | ||||||
| Non-English household | .70 | + | .81 | .88 | .91 | .72 | .71 | + | 1.08 | .95 | ||||||
| Resources (Kindergarten) | ||||||||||||||||
| Income-to-needs | 1.02 | ac | 1.02 | ac | .93 | *b | .94 | +b | .94 | *b | .95 | +b | .88 | .93 | ||
| Maternal education (advanced degree) | ||||||||||||||||
| Less than high school | 1.42 | c | 1.51 | 2.42 | * | 2.06 | * | 2.49 | **b | 2.06 | * | 3.08 | * | 2.06 | ||
| High school | 1.04 | a | 1.00 | 1.82 | *b | 1.56 | 1.47 | 1.22 | 1.67 | 1.14 | ||||||
| Some college | .95 | .92 | 1.48 | 1.36 | 1.22 | 1.09 | 1.52 | 1.25 | ||||||||
| College degree | .82 | .78 | 1.01 | .94 | .81 | .76 | 1.11 | .86 | ||||||||
| Married | .72 | * | .69 | * | .67 | * | .66 | * | .79 | .80 | 1.00 | .98 | ||||
| Parenting (Kindergarten) | ||||||||||||||||
| # activities | 1.01 | cd | 1.01 | c | .94 | d | .97 | .88 | **b | .91 | *b | .73 | **ab | .82 | + | |
| Parenting scale | .88 | 1.00 | .77 | + | .93 | .82 | .96 | .64 | .83 | |||||||
| First-grade classes (Generally favorable) | ||||||||||||||||
| Generally compromised | 1.31 | d | 1.65 | d | 1.75 | +d | 6.74 | ***abc | ||||||||
| Mixed | 1.92 | *** | 2.05 | *** | 1.96 | *** | 2.43 | * | ||||||||
| Mid, compromised exercise | .70 | +acd | 1.16 | bd | 1.52 | *bd | 3.65 | **abc | ||||||||
| Compromised diet/sleep/TV | 1.00 | d | 1.23 | d | 1.24 | d | 3.15 | **abc | ||||||||
| Third-grade classes (Generally favorable) | ||||||||||||||||
| Compromised diet/exercise | 1.37 | 1.37 | 1.59 | 2.83 | * | |||||||||||
| Compromised health care/exercise | .93 | ad | 1.59 | bd | 1.45 | d | 4.21 | **abc | ||||||||
| Compromised except exercise | 1.33 | d | 1.31 | d | 1.34 | d | 3.40 | **abc | ||||||||
| Favorable but irregular | 1.40 | ** | 1.19 | 1.10 | d | 2.11 | *c | |||||||||
| Fifth-grade classes (Generally favorable) | ||||||||||||||||
| Favorable but irregular | 1.92 | *** | 2.06 | *** | 1.46 | ** | 2.12 | * | ||||||||
| Compromised except exercise | 1.61 | *a | 3.00 | ***bc | 1.88 | **a | 2.93 | ** | ||||||||
| Compromised exercise/health care | 1.60 | ad | 3.98 | **bc | 1.85 | ad | 10.33 | ***bc | ||||||||
| Compromised exercise/TV | 2.24 | *** | 2.87 | *** | 2.81 | *** | 1.98 | |||||||||
| Constant | 7.40 | + | 3.11 | 3.04 | .85 | 20.77 | * | 7.89 | + | 3.01 | .45 | |||||
Source: ECLS-K, 1998-2007.
Notes: N=8786. Accounts for complex sampling design. Nonsignificant covariates (maternal age at survey, maternal age at birth, # siblings, health insurance) not shown.
p<.10
p<.05
p<.01
p<.001; two-tailed tests.
p<.05 compared to:
mid, compromised diet/TV
favorable but irregular
mid, compromised exercise/TV
compromised exercise/health care
Tables 4 and 5 also present evidence to assess our expectation that family influences on developing health lifestyles at school entry are subsequently joined by peers and schools. We first assessed family influences based on our theoretical model that identified sociodemographic background, resources, and parenting as influences on first graders' health lifestyles. Analyses reported in Table 4 supported this model, with multiple factors from each of these three domains in kindergarten predicting the likelihood of membership in different first-grade health lifestyle classes compared to “generally favorable” (with supplemental tests comparing each class to every other class).
Table 5, Model 1 reassessed this model for eighth-grade outcomes. The three family domains still predicted eighth-grade health lifestyles as expected, but average marginal effects in Tables A5 and A6 found less consistent relationships with smaller magnitudes. Taken together, findings suggest that some family influences on health lifestyles waned with age. Model 2 shows that earlier health lifestyles partially explained the associations of some family influences in each domain on eighth-grade health lifestyles. This suggests that developing health lifestyles may be one pathway linking family background to child health.
Table 6 considers family, school, and peer factors together in predicting eighth-grade health lifestyles (average marginal effects available in Table A7). Beyond controls for child background, one first-grade school characteristic, school socioeconomic status, predicted eighth-grade health lifestyles compared to the referent group, which we interpret as suggestive evidence of school effects. School socioeconomic disadvantage (free/reduced-price lunch) decreased the likelihood of belonging to the “favorable but irregular” class (children who may be busy with extracurricular activities but otherwise have healthy behaviors) compared to “generally favorable.” Table 6 provides only suggestive evidence that first-grade peers' health lifestyles influence eighth-grade health lifestyles: A modal “mixed” health lifestyle among first-grade peers compared to “generally favorable” was associated with a higher likelihood of being in the “favorable but irregular” class in eighth grade. Supplemental analyses found that first-grade health lifestyles did not mediate peer health lifestyle effects on eighth-grade lifestyles. In sum, with a seven-year lag between school and peer measurement and health lifestyle outcomes, evidence for school and peer effects was only suggestive.
Table 6. Odds Ratios from Multinomial Logistic Regression Model Predicting Eighth-Grade Classes (Referent: “GenerallyFavorable”).
| Favorable but irregular | Favorable but irregular | Mid, compromised exercise/TV | Compromised exercise/ health care | |||||
|---|---|---|---|---|---|---|---|---|
| Peer characteristics (First grade) | ||||||||
| Modal class (generally favorable) | ||||||||
| Generally compromised | .77 | .75 | .82 | .52 | ||||
| Mixed | 1.46 | * | 1.30 | 1.33 | 1.20 | |||
| Mid, compromised exercise | .98 | .87 | 1.09 | 1.74 | ||||
| Compromised diet/sleep/TV | 1.00 | .69 | .86 | .90 | ||||
| Percent of modal class | 1.97 | ad | .43 | bc | 1.14 | a | .14 | b |
| School characteristics (First grade) | ||||||||
| Public school | 1.06 | 1.35 | 1.34 | 2.58 | + | |||
| % nonwhite | 1.00 | 1.00 | 1.00 | 1.01 | + | |||
| % free/reduced price lunch | .99 | **a | 1.00 | b | .99 | + | .99 | |
| Controls (Kindergarten) | ||||||||
| Male | .91 | c | 1.00 | c | .58 | ***ab | .77 | |
| Race/ethnicity (white) | ||||||||
| Black | .84 | ac | 1.29 | b | 1.37 | b | 1.21 | |
| Hispanic | 1.30 | ac | 1.89 | **b | 1.89 | **b | 1.54 | |
| Asian/Pacific Islander | .90 | .64 | c | 1.14 | a | .85 | ||
| American Indian | 1.30 | a | .68 | bc | 1.78 | +ad | .33 | c |
| Multiracial | .57 | *d | .83 | d | .83 | d | 3.44 | +abc |
| Resources (Kindergarten) | ||||||||
| Income-to-needs | 1.01 | a | .91 | *b | .96 | .87 | ||
| Maternal education (advanced degree) | ||||||||
| Less than high school | 1.30 | 2.22 | * | 2.15 | * | 2.81 | ||
| High school | .94 | 1.51 | 1.27 | 1.44 | ||||
| Some college | .96 | 1.34 | 1.06 | 1.31 | ||||
| College degree | .93 | 1.07 | .77 | 1.45 | ||||
| Married | .68 | ** | .66 | * | .75 | .98 | ||
| No health insurance | .66 | + | .98 | .94 | 1.48 | |||
| Parenting (Kindergarten) | ||||||||
| # activities | .97 | cd | .92 | .84 | ***b | .76 | **b | |
| Constant | 6.72 | 1.51 | 8.54 | .24 | ||||
Source: ECLS-K, 1998-2007.
Notes: N=7829. Accounts for complex sampling design. Nonsignificant covariates (child age, maternal age at survey, maternal age at birth, household language, # siblings, parenting scale, school enrollment, school % passing reading) not shown.
p<.10
p<.05
p<.01
p<.001; two-tailed tests.
p<.05 compared to:
mid, compromised diet/TV
favorable but irregular
mid, compromised exercise/TV
Compromised exercise/health care
Finally, Table 5, Model 2 shows that children's health lifestyles in first grade and throughout elementary school influenced their eighth-grade lifestyles. Latent classes from first, third, and fifth grades predicted eighth-grade health lifestyles independently of all other waves. For example, compared to “generally favorable” at each wave, every health lifestyle class at every wave predicted increased odds of membership in the “compromised exercise/health care” eighth-grade health lifestyle class (odds ratios=2-10). The sole nonsignificant exception was the fifth-grade “compromised exercise/TV” class. Thus, being in almost any sort of less than optimal health lifestyle at any wave made it more likely that a child would have arguably the least optimal health lifestyle in eighth grade. These findings support an approach that considers multiple life stages, not just early childhood or the most proximal age, in understanding later health lifestyles.
Discussion
This study represents a first step in characterizing health lifestyles and their antecedents throughout middle childhood and early adolescence. Rooted in theoretical ideas about the life course and intergenerational, cumulative disadvantage (DiPrete and Eirich 2006, Elder 1994, Seabrook and Avison 2012, Seabrook and Avison 2015), findings support a dynamic conceptualization of developing health lifestyles that incorporates developmental continuity and change, multiple social contexts, and partially path-dependent processes of lifestyle formation. We emphasize two key findings.
First, developing health lifestyles are a combination of consistency and inconsistency. This is true within each time point, with healthier and unhealthier health behaviors often clustering within individuals in complex ways that sometimes reflect social statuses such as gender and sometimes suggest complex interactions of unmeasured social influences and human agency. As others have found for other life phases (Mistry et al. 2009, Saint Onge and Krueger 2017), health lifestyles are not uniformly positive or negative and vary between sociodemographically similar people. These findings support theoretical expectations about health lifestyles (author citation 2014, Cockerham 2005). Our findings contribute by showing that this blend of consistency and inconsistency holds true not just within time points, but across age within individuals. Children's earlier health lifestyles predict later ones but do so fairly weakly. Because health lifestyles at each time point are influential for understanding later lifestyles, social influences throughout childhood, and not just those that occur early or most recently, are important.
Second, multiple social contexts matter for understanding children's developing health lifestyles. Health lifestyle development is partly path dependent, with families shaping first-grade health lifestyles, which are influential for early adolescent health lifestyles. Beyond family influences, characteristics of communities—here, children's schools and peer networks—apparently shape health lifestyle development. The shifting ecologies around middle childhood development have important implications for understanding social determinants of health behaviors. Family influences—household resources, social background, and parenting quality—shape health lifestyles throughout these ages, echoing some findings from [author citation 2014] and Huh et al. (2011) cross-sectionally in childhood and Mistry et al. (2009) in adolescence. We contribute by modeling how family influences may be joined by those of schools and peers as children grow. Because individual health lifestyles were measured seven years after school factors and peer lifestyles, any association suggests that these contexts may matter. Thus, our test was conservative, yielding a few significant school and peer effects interpreted as suggestive evidence. A more detailed and proximal accounting of peers and schools may uncover larger, more persistent patterns of influence. The multiple social influences reflect the widening of children's social worlds as they grow, emphasizing the complexity needed to fully model influences on health lifestyle development throughout early life.
This study's limitations emphasize the importance of future work on health lifestyle development in early life. With observational longitudinal data, causal relationships could not be firmly established and sample attrition limited conclusions for all U.S. children. Our approach prioritized a broad characterization of health lifestyles across middle childhood over approaches providing more focused detail. Domain-specific future research will be an important complement to these findings. Most measures were based on parent reports, likely biasing findings compared to direct observations in ways that may have represented behaviors as healthier than they actually were. We were limited by available health behavior measures, and a lack of variables measuring who controlled those behaviors, child agency, and group-based identities constrained our ability to assess those facets of health lifestyles theory. This limitation is shared by other extant research, and our ongoing qualitative research attempts to shed light on these factors. Additionally, emerging risky health behaviors—such as substance use and sexual activity—are part of some young adolescents' health lifestyles but were not measured here. Our ongoing research examines these behaviors among adolescents using other longitudinal data sources. ECLS-K children were also not followed before elementary school or after middle school, resulting in a limited view of individuals' life courses. Finally, there may have been misclassification error in assigning individuals to health lifestyles that we did not account for, biasing relationships downward and likely attenuating relationships.
This research has implications for understandings of health behaviors and lifestyles and for social policy. Longitudinal examinations of health lifestyles are key, as characterizing a young person's health lifestyle at a single time point results in a very limited picture. The importance of complex measurements over time is joined by the necessity of complex measurement within each time point, as we found evidence that multiple social contexts have important influences on health lifestyle development. These efforts at modeling multifaceted influences on health lifestyles are important because health lifestyles are a promising site for understanding intergenerational transmission processes, both at the family and community levels. Policies aimed at changing health behaviors should incorporate a health lifestyles approach. For instance, a policy targeting eighth graders who watch too much television may not be effective unless it tailors its approach to each of the two predominant health lifestyles in which this behavior is nested, one in which poor dietary practices are the accompanying health risk and one in which low levels of exercise are the accompanying risk. Understanding the role of gender, as well as other complex social factors, in shaping the identities that likely underlie health behavior patterns may result in more effective policy solutions. These efforts will likely require multimethod research.
This study is only a preliminary step towards an understanding of how clusters of child behaviors develop in an interplay between adult control and child agency. Future studies should disentangle the mechanisms through which families, other contexts, and children shape identities and patterns of behavior that underlie health lifestyles. Neighborhoods, siblings, and teachers are social influences on young people's health lifestyles that have yet to be studied. Whereas research on adult health behavior has arguably relied too much on individual agency, research on child health behaviors could benefit from an increased understanding of agency.
Additionally, understandings of health could benefit from a more comprehensive life course perspective. Despite the wealth of research on associations between risk and protective factors and adolescent health, we know much less about the preceding years of middle childhood. Adolescence is noteworthy because it is when individuals make decisions regarding substance use, sex, and other new experiences, but at younger ages, children begin to make decisions regarding other health habits that can have long-term health implications, such as eating, exercise, and sleep. Identifying the developmental and ecological connections between middle childhood and adolescence and young adulthood, when many risk behaviors make their first appearance, can shed new light on patterns of health in individuals and groups.
Supplementary Material
Appendix Table A1. Fit Statistics for Latent Class Analysis Results, by Wave
Appendix Table A2. Class-Conditional Response Probabilities from Latent Class Analyses (LCA) for First Grade
Appendix Table A3. Class-Conditional Response Probabilities from Latent Class Analyses (LCA) for Third Grade
Appendix Table A4. Class-Conditional Response Probabilities from Latent Class Analyses (LCA) for Fifth Grade
Appendix Table A5. Average Marginal Effects from Multinomial Logistic Regression Model Predicting First-Grade Classes
Appendix Table A6. Average Marginal Effects from Multinomial Logistic Regression Model Predicting Eighth-Grade Classes
Appendix Table A7. Average Marginal Effects from Multinomial Logistic Regression Model Predicting Eighth-Grade Classes
Acknowledgments
We thank Richard Jessor and Fred Pampel for their contributions to this study.
Funding: This research is based on work supported by a grant from the National Science Foundation (SES 1423524) and a fellowship from the National Institutes of Health (NICHD F32 HD 085599). Research funds were also provided by the NIH/NICHD funded CU Population Center (P2C HD066613). We are grateful for support from the Population Research Infrastructure Program (P2C HD050924) awarded to the Carolina Population Center at The University of North Carolina at Chapel Hill.
Biographies
Stefanie Mollborn is a professor in the Institute of Behavioral Science and the Department of Sociology at the University of Colorado Boulder. Her multimethod research examines social norms and inequalities in the early life course, with a current focus on health lifestyles.
Elizabeth Lawrence is a postdoctoral fellow in the Carolina Population Center at the University of North Carolina – Chapel Hill. Her research examines social inequality and health, with a focus on how individuals' educational and health trajectories develop together over the life course.
Footnotes
Missingness was about 5% across all items, with the greatest percentage missing for mother's age at kindergarten wave (14%) and at birth (14%). We used a chained equations, or fully conditional specification, approach creating 10 datasets. All independent and dependent variables were used to inform imputation. Separate imputation procedures using the same specifications were used for analyses that included school-level variables.
Contributor Information
Stefanie Mollborn, University of Colorado Boulder.
Elizabeth Lawrence, University of North Carolina.
References
- Abel Thomas. Measuring Health Lifestyles in a Comparative Analysis: Theoretical Issues and Empirical Findings. Social Science & Medicine. 1991;32(8):899–908. doi: 10.1016/0277-9536(91)90245-8. [DOI] [PubMed] [Google Scholar]
- Bakk Zsuzsa, Tekle Fetene B, Vermunt Jeroen K. Estimating the Association between Latent Class Membership and External Variables Using Bias-Adjusted Three-Step Approaches. Sociological Methodology. 2013;43(1):272–311. [Google Scholar]
- Bates John E, Viken Richard J, Alexander Douglas B, Beyers Jennifer, Stockton Lesley. Sleep and Adjustment in Preschool Children: Sleep Diary Reports by Mothers Relate to Behavior Reports by Teachers. Child Development. 2002;73(1):62–74. doi: 10.1111/1467-8624.00392. [DOI] [PubMed] [Google Scholar]
- Bolck Annabel, Croon Marcel, Hagenaars Jacques. Estimating Latent Structure Models with Categorical Variables: One-Step Versus Three-Step Estimators. Political Analysis. 2004:3–27. [Google Scholar]
- Bourdieu Pierre. Distinction: A Social Critique of the Judgement of Taste. London: Routledge & Kegan Paul; 1986. [Google Scholar]
- Bronfenbrenner Urie. The Ecology of Human Development: Experiments by Nature and Design. Cambridge, MA: Harvard University Press; 1979. [Google Scholar]
- Cockerham William C. Health Lifestyles in Russia. Social Science & Medicine. 2000;51(9):1313–24. doi: 10.1016/s0277-9536(00)00094-0. [DOI] [PubMed] [Google Scholar]
- Cockerham William C. Health Lifestyle Theory and the Convergence of Agency and Structure. Journal of Health and Social Behavior. 2005;46(1):51–67. doi: 10.1177/002214650504600105. [DOI] [PubMed] [Google Scholar]
- Cockerham William C. Health Lifestyles and the Absence of the Russian Middle Class. Sociology of Health & Illness. 2007;29(3):457–73. doi: 10.1111/j.1467-9566.2007.00492.x. [DOI] [PubMed] [Google Scholar]
- Cockerham William C. Bourdieu and an Update of Health Lifestyle Theory. In: Cockerham WC, editor. Medical Sociology on the Move: New Directions in Theory. W C Dordrecht: Springer; 2013. pp. 127–54. [Google Scholar]
- Collins Linda M, Lanza Stephanie T. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral, and Health Sciences. New York: John Wiley & Sons; 2013. [Google Scholar]
- Cook John T, Frank Deborah A, Levenson Suzette M, Neault Nicole B, Heeren TC, Black MM, Berkowitz C, Casey PH, Meyers AF, Cutts DB, Chilton M. Child Food Insecurity Increases Risks Posed by Household Food Insecurity to Young Children's Health. Journal of Nutrition. 2006;136(4):1073–76. doi: 10.1093/jn/136.4.1073. [DOI] [PubMed] [Google Scholar]
- Crosnoe Robert. Health and the Education of Children from Racial/Ethnic Minority and Immigrant Families. Journal of Health and Social Behavior. 2006;47(1):77–93. doi: 10.1177/002214650604700106. [DOI] [PubMed] [Google Scholar]
- Dannefer Dale. Cumulative Advantage/Disadvantage and the Life Course: Cross-Fertilizing Age and Social Science Theory. Journals of Gerontology Series B-Psychological Sciences and Social Sciences. 2003;58(6):S327–S37. doi: 10.1093/geronb/58.6.s327. [DOI] [PubMed] [Google Scholar]
- De Genna Natacha M, Stack Dale M, Serbin Lisa A, Ledingham Jane E, Schwartzman Alex E. From Risky Behavior to Health Risk: Continuity across Two Generations. Journal of Developmental and Behavioral Pediatrics. 2006;27(4):297–309. doi: 10.1097/00004703-200608000-00004. [DOI] [PubMed] [Google Scholar]
- de la Haye Kayla, Robins Garry, Mohr Philip, Wilson Carlene. How Physical Activity Shapes, and Is Shaped by, Adolescent Friendships. Social Science & Medicine. 2011;73(5):719–28. doi: 10.1016/j.socscimed.2011.06.023. [DOI] [PubMed] [Google Scholar]
- De Vries Hein, van't Riet Jonathan, Spigt Mark, Metsemakers Job, van den Akker Marjan, Vermunt Jeroen K, Kremers Stef. Clusters of Lifestyle Behaviors: Results from the Dutch Smile Study. Preventive Medicine. 2008;46(3):203–08. doi: 10.1016/j.ypmed.2007.08.005. [DOI] [PubMed] [Google Scholar]
- Diamond John B, Randolph Antonia, Spillane James P. Teachers' Expectations and Sense of Responsibility for Student Learning: The Importance of Race, Class, and Organizational Habitus. Anthropology & Education Quarterly. 2004;35(1):75–98. [Google Scholar]
- DiPrete Thomas A, Eirich Gregory M. Cumulative Advantage as a Mechanism for Inequality: A Review of Theoretical and Empirical Developments. Annual Review of Sociology. 2006;32:271–97. [Google Scholar]
- Duncan Greg J, Magnuson Katherine. The Nature and Impact of Early Achievement Skills, Attention Skills, and Behavior Problems. In: Duncan GJ, Murnane RJ, editors. Whither Opportunity? Rising Inequality, Schools, and Children's Life Chances. New York: Russell Sage Foundation; 2011. pp. 47–69. [Google Scholar]
- Elder Glen H., Jr Time, Human Agency, and Social Change: Perspectives on the Life Course. Social Psychology Quarterly. 1994;57(1):4–15. [Google Scholar]
- Entwisle Doris R, Alexander Karl L, Olson Linda Steffel. The First-Grade Transition in Life Course Perspective. In: Mortimer JT, Shanahan MJ, editors. Handbook of the Life Course. New York: Springer; 2004. [Google Scholar]
- Fitzgerald Amanda, Fitzgerald Noelle, Aherne Cian. Do Peers Matter? A Review of Peer and/or Friends' Influence on Physical Activity among American Adolescents. Journal of Adolescence. 2012;35(4):941–58. doi: 10.1016/j.adolescence.2012.01.002. [DOI] [PubMed] [Google Scholar]
- Flay Brian R, Hu Frank B, Siddiqui Ohidul, Edward Day L, Hedeker Donald, Petraitis John, Richardson Jean, Sussman Steven. Differential Influence of Parental Smoking and Friends' Smoking on Adolescent Initiation and Escalation and Smoking. Journal of Health and Social Behavior. 1994;35(3):248–65. [PubMed] [Google Scholar]
- Freese Jeremy, Lutfey Karen. Fundamental Causality: Challenges of an Animating Concept for Medical Sociology. In: Pescosolido BA, Martin JK, McLeod JD, Rogers A, editors. Handbook of the Sociology of Health, Illness, and Healing: A Blueprint for the 21st Century. New York: Springer; 2011. pp. 67–81. [Google Scholar]
- Frohlich Katherine L, Corin Ellen, Potvin Louise. A Theoretical Proposal for the Relationship between Context and Disease. Sociology of Health & Illness. 2001;23(6):776–97. [Google Scholar]
- Glewwe Paul, Jacoby Hanan G, King Elizabeth M. Early Childhood Nutrition and Academic Achievement: A Longitudinal Analysis. Journal of Public Economics. 2001;81(3):345–68. [Google Scholar]
- Goodman Leo A. On the Assignment of Individuals to Latent Classes. Sociological Methodology. 2007;37(1):1–22. [Google Scholar]
- Huh Jimi, Riggs Nathaniel R, Spruijt-Metz Donna, Chou Chih-Ping, Huang Zhaoqing, Pentz Mary Ann. Identifying Patterns of Eating and Physical Activity in Children: A Latent Class Analysis of Obesity Risk. Obesity. 2011;19(3):652–58. doi: 10.1038/oby.2010.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimbro Rachel Tolbert, Brooks-Gunn Jeanne, McLanahan Sara. Young Children in Urban Areas: Links among Neighborhood Characteristics, Weight Status, Outdoor Play, and Television Watching. Social Science & Medicine. 2011;72(5):668–76. doi: 10.1016/j.socscimed.2010.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King Marissa D, Jennings Jennifer, Fletcher Jason M. Medical Adaptation to Academic Pressure Schooling, Stimulant Use, and Socioeconomic Status. American Sociological Review. 2014;79(6):1039–66. [Google Scholar]
- Klein Daniel. Mimrgns: Stata Module to Run Margins after Mi Estimate. Statistical Software Components 2017 [Google Scholar]
- Korp Peter. The Symbolic Power of ‘Healthy Lifestyles’. Health Sociology Review. 2008;17(1):18–26. [Google Scholar]
- Krueger Patrick M, Bhaloo Tajudaullah, Rosenau Pauline Vaillancourt. Health Lifestyles in the United States and Canada: Are We Really So Different? Social Science Quarterly. 2009;90(5):1380–402. doi: 10.1111/j.1540-6237.2009.00660.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laaksonen Mikko, Prättälä Ritva, Lahelma Eero. Sociodemographic Determinants of Multiple Unhealthy Behaviors. Scandinavian Journal of Public Health. 2003;31(1):37–43. doi: 10.1080/14034940210133915. [DOI] [PubMed] [Google Scholar]
- Laible Deborah J, Carlo Gustavo, Raffaelli Marcela. The Differential Relations of Parent and Peer Attachment to Adolescent Adjustment. Journal of Youth and Adolescence. 2000;29(1):45–59. [Google Scholar]
- Lee Ellie, Macvarish Jan, Bristow Jennie. Risk, Health and Parenting Culture. Health, Risk & Society. 2010;12(4):293–300. [Google Scholar]
- Lee Ellie J. Living with Risk in the Age of ‘Intensive Motherhood’: Maternal Identity and Infant Feeding. Health, Risk & Society. 2008;10(5):467–77. [Google Scholar]
- Leventhal Adam M, Huh Jimi, Dunton Genevieve F. Clustering of Modifiable Biobehavioral Risk Factors for Chronic Disease in Us Adults: A Latent Class Analysis. Perspectives in Public Health. 2014;134(6):331–38. doi: 10.1177/1757913913495780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Link Bruce G, Phelan Jo. Social Conditions as Fundamental Causes of Disease. Journal of Health and Social Behavior. 1995;35:80–94. [PubMed] [Google Scholar]
- McAloney Kareena, Graham Hilary, Law Catherine, Platt Lucinda. A Scoping Review of Statistical Approaches to the Analysis of Multiple Health-Related Behaviours. Preventive Medicine. 2013;56(6):365–71. doi: 10.1016/j.ypmed.2013.03.002. [DOI] [PubMed] [Google Scholar]
- McCarthy Jane Ribbens, Edwards Rosalind, Gillies Val. Moral Tales of the Child and the Adult: Narratives of Contemporary Family Lives under Changing Circumstances. Sociology. 2000;34(4):785–803. [Google Scholar]
- Mistry Ritesh, McCarthy William J, Yancey Antronette K, Lu Yao, Patel Minal. Resilience and Patterns of Health Risk Behaviors in California Adolescents. Preventive medicine. 2009;48(3):291–97. doi: 10.1016/j.ypmed.2008.12.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mize Trenton D. Profiles in Health: Multiple Roles and Health Lifestyles in Early Adulthood. Social Science & Medicine. 2017;178:196–205. doi: 10.1016/j.socscimed.2017.02.017. [DOI] [PubMed] [Google Scholar]
- Mollborn Stefanie, Domingue Benjamin W, Boardman Jason D. Understanding Multiple Levels of Norms About Teen Pregnancy and Their Relationships to Teens' Sexual Behaviors. Advances in Life Course Research. 2014a;20:1–15. doi: 10.1016/j.alcr.2013.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mollborn Stefanie, Domingue Benjamin W, Boardman Jason D. Norms as Group-Level Constructs: Investigating School-Level Teen Pregnancy Norms and Behaviors. Social Forces. 2014b;93(1):241–67. doi: 10.1093/sf/sou063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nagin Daniel. Group-Based Modeling of Development. Harvard University Press; 2005. [Google Scholar]
- Olson Julie Skalamera, Hummer Robert A, Mullan Harris Kathleen. Gender and Health Behavior Clustering among Us Young Adults. Biodemography and Social Biology. 2017;63(1):3–20. doi: 10.1080/19485565.2016.1262238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patnode Carrie D, Lytle Leslie A, Erickson Darin J, Sirard John R, Barr-Anderson Daheia J, Story Mary. Physical Activity and Sedentary Activity Patterns among Children and Adolescents: A Latent Class Analysis Approach. Journal of Physical Activity and Health. 2011;8(4):457–67. doi: 10.1123/jpah.8.4.457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedersen Susanne, Grønhøj Alice, Thøgersen John. Following Family or Friends. Social Norms in Adolescent Healthy Eating. Appetite. 2015;86:54–60. doi: 10.1016/j.appet.2014.07.030. [DOI] [PubMed] [Google Scholar]
- Prochaska Judith J, Spring Bonnie, Nigg Claudio R. Multiple Health Behavior Change Research: An Introduction and Overview. Preventive Medicine. 2008;46(3):181–88. doi: 10.1016/j.ypmed.2008.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saint Onge Jarron M, Krueger Patrick M. Health Lifestyle Behaviors among US Adults. SSM-Population Health. 2017;3:89–98. doi: 10.1016/j.ssmph.2016.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salvy Sarah-Jeanne, de la Haye Kayla, Bowker Julie C, Hermans Roel CJ. Influence of Peers and Friends on Children's and Adolescents' Eating and Activity Behaviors. Physiology & Behavior. 2012;106(3):369–78. doi: 10.1016/j.physbeh.2012.03.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seabrook Jamie A, Avison William R. Socioeconomic Status and Cumulative Disadvantage Processes across the Life Course: Implications for Health Outcomes. Canadian Review of Sociology/Revue Canadienne de Sociologie. 2012;49(1):50–68. doi: 10.1111/j.1755-618x.2011.01280.x. [DOI] [PubMed] [Google Scholar]
- Seabrook Jamie A, Avison William R. Family Structure and Children's Socioeconomic Attainment: A Canadian Sample. Canadian Review of Sociology/Revue Canadienne de Sociologie. 2015;52(1):66–88. doi: 10.1111/cars.12061. [DOI] [PubMed] [Google Scholar]
- Skalamera Julie, Hummer Robert A. Educational Attainment and the Clustering of Health-Related Behavior among U.S. Young Adults. Preventive Medicine. 2016;84:83–89. doi: 10.1016/j.ypmed.2015.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sobel Michael E. Lifestyle and Social Structure: Concepts, Definitions, Analyses. New York: Academic Press; 1981. [Google Scholar]
- Stefansdottir Ingibjorg Katrin, Vilhjalmsson Runar. Dimensions of Health-Related Lifestyle in Young Adulthood: Results from a National Population Survey. Scandinavian Journal of Caring Sciences. 2007;21(3):321–28. doi: 10.1111/j.1471-6712.2007.00479.x. [DOI] [PubMed] [Google Scholar]
- Steinberg Laurence, Silverberg Susan B. The Vicissitudes of Autonomy in Early Adolescence. Child Development. 1986;57(4):841–51. doi: 10.1111/j.1467-8624.1986.tb00250.x. [DOI] [PubMed] [Google Scholar]
- Tourangeau Karen, Christine Nord Thanh Lê, Sorongon Alberto G, Najarian Michelle. Early Childhood Longitudinal Study, Kindergarten Class of 1998-99 (ECLS-K), Combined User's Manual for the ECLS-K Eighth-Grade and K-8 Full Sample Data Files and Electronic Codebooks (NCES 2009-004) National Center for Education Statistics, Institute of Education Sciences, U.S Department of Education; Washington, D.C: 2009. [Google Scholar]
- Wickrama KAS, Conger Rand D, Wallace Lora Ebert, Elder Glen H., Jr The Intergenerational Transmission of Health-Risk Behaviors: Adolescent Lifestyles and Gender Moderating Effects. Journal of Health and Social Behavior. 1999;40(3):258–72. [PubMed] [Google Scholar]
- Williams Simon J. Theorising Class, Health and Lifestyles: Can Bourdieu Help Us? Sociology of Health & Illness. 1995;17(5):577–604. [Google Scholar]
- Woolf Steven H, Aron Laudan Y. US Health in International Perspective: Shorter Lives, Poorer Health. National Academies Press; 2013. [PubMed] [Google Scholar]
- Zimmer-Gembeck Melanie, Adams Gerald R, Berzonsky Michael D, Andrew Collins W. Autonomy Development During Adolescence. Blackwell Publishing; 2003. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix Table A1. Fit Statistics for Latent Class Analysis Results, by Wave
Appendix Table A2. Class-Conditional Response Probabilities from Latent Class Analyses (LCA) for First Grade
Appendix Table A3. Class-Conditional Response Probabilities from Latent Class Analyses (LCA) for Third Grade
Appendix Table A4. Class-Conditional Response Probabilities from Latent Class Analyses (LCA) for Fifth Grade
Appendix Table A5. Average Marginal Effects from Multinomial Logistic Regression Model Predicting First-Grade Classes
Appendix Table A6. Average Marginal Effects from Multinomial Logistic Regression Model Predicting Eighth-Grade Classes
Appendix Table A7. Average Marginal Effects from Multinomial Logistic Regression Model Predicting Eighth-Grade Classes