

Abstract
Background:
Female patients sustain noncontact knee ligament injuries at a greater rate compared with their male counterparts. The cause of these differences in the injury rate and the movements that load the ligaments until failure are still under dispute in the literature.
Purpose/Hypotheses:
This study was designed to determine differences in anterior cruciate ligament (ACL) and medial collateral ligament (MCL) strains between male and female cadaveric specimens during a simulated athletic task. The primary hypothesis tested was that female limbs would demonstrate significantly greater ACL strain compared with male limbs under similar loading conditions. A secondary hypothesis was that MCL strain would not differ between sexes.
Study Design:
Controlled laboratory study.
Methods:
Motion analysis of 67 athletes performing a drop vertical jump was conducted. Kinetic data were used to categorize injury risk according to tertiles, and these values were input into a cadaveric impact simulator to assess ligamentous strain during a simulated landing task. Uniaxial and multiaxial load cells and differential variable reluctance transducer strain sensors were utilized to collect mechanical data for analysis. Conditions of external loads applied to the cadaveric limbs (knee abduction moment, anterior tibial shear, and internal tibial rotation) were varied and randomized. Data were analyzed using 1-way analysis of variance (ANOVA), 2-way repeated-measures ANOVA, and the Fisher exact test.
Results:
There were no significant differences (P = .184) in maximum ACL strain between male (13.2% ± 8.1%) and female (16.7% ± 8.3%) specimens. Two-way ANOVA demonstrated that across all controlled external load conditions, female specimens consistently attained at least 3.5% increased maximum ACL strain compared with male specimens (F 1,100 = 4.188, P = .043); however, when normalized to initial contact, no significant difference was found. There were no significant differences in MCL strain between sexes for similar parameters.
Conclusion:
When compared with baseline, female specimens exhibited greater values of ACL strain at maximum, initial contact, and after impact (33, 66, and 100 milliseconds, respectively) than male specimens during similar loading conditions, with a maximum strain difference of at least 3.5%. During these same loading conditions, there were no differences in MCL loading between sexes, and only a minimal increase of MCL loading occurred during the impact forces. Our results indicate that female patients are at an increased risk for ACL strain across all similar conditions compared with male patients.
Clinical Relevance:
These data demonstrate that female specimens, when loaded similarly to male specimens, experience additional strain on the ACL. As the mechanical environment was similar for both sexes with these simulations, the greater ACL strain of female specimens must be attributed to ligament biology, anatomic differences, or muscular stiffness.
Keywords: anterior cruciate ligament (ACL), cadaveric, simulation, medial collateral ligament (MCL), sex differences, strain
Worldwide annual estimates of anterior cruciate ligament (ACL) injuries are over 2 million; the majority of these injuries occur during sport participation.34 The incidence of sport injuries in female athletes continues to increase, and exercise-related musculoskeletal injuries in female athletes are more prevalent than in male athletes.20,41 In addition, female patients have a 4- to 6-fold increased exposure risk of ACL injuries compared with their male counterparts.1,14,24,31,37 Surgery and rehabilitation costs associated with female ACL injuries total approximately $646 million in the United States annually.16,19
An injury to the ACL is generally noncontact in nature, with estimates of this noncontact mechanism accounting for approximately 75% of all ACL injuries.11,28,29,37 This mechanism of injury indicates that ACL tears are likely influenced by poor neuromuscular control and risky movement strategies that include dynamic knee abduction (valgus),16,27,32 hip adduction,30,43 and internal rotation of the tibia and hip.39 With these multiplanar movement strategies that increase loading on both the ACL and medial collateral ligament (MCL), there are disparities in the literature on whether ACL injuries occur with a multiplanar18,29,31 or sagittal-plane mechanism12,27,33,42 especially because the ACL is considered a primary restraint to anterior tibial translation and the majority of ACL injuries lack a concomitant injury of the MCL.33 Thus, there is a need to clarify the multiplanar mechanisms of an ACL injury and the associated lack of frequent concomitant MCL injuries. By doing so, improved preventive and rehabilitative strategies can be implemented.
To optimize preventive and rehabilitative strategies for all ACL-injured patients and lower the societal burden of these injuries, especially for female patients, it is essential to establish the underlying mechanics that contribute to excessive loads that lead to ligamentous failure.4,13 The specific mechanisms that load the ACL for injuries are still under dispute, and the mechanisms may be different between sexes.31,42 These disputed ACL loading mechanisms include knee abduction moment (KAM), anterior tibial shear (ATS), and internal tibial rotation (ITR). Prevention is essential for reduction of the health burden associated with ACL injuries and their sequelae,9 which include decreased activity levels, further knee injuries, and early-onset osteoarthritis.13,21,23 Enhanced knowledge of the movement strategies that increase ACL strain and lead to failure of the ligament will augment injury prevention, rehabilitation, and return-to-sport criteria.38
Consequently, this study was designed to investigate potential sex-based differences in ligament loading at the knee that strains the ACL and MCL during a common athletic task: the drop vertical jump (DVJ). The primary hypothesis tested was that female cadaveric specimens would demonstrate significantly greater ACL strain compared with male cadaveric specimens under similar loading conditions, and the secondary hypothesis tested was that MCL strain would not differ between the sexes.
Methods
Lower extremity cadaveric specimens (N = 45) were obtained (Anatomy Gifts Registry) according to our inclusion criteria: age 18 to 50 years, no evidence of significant trauma or surgery to the lower extremity, no extensive bed rest, and no evidence of extended chemotherapy. Specimens were not acquired if they had systemic infections, they had a cartilaginous disease (other than typical of regular aging), and the cause of death would have induced significant trauma to the lower extremity. Specimens were dissected and prepared according to specifications outlined in a recent methodology study.7 Briefly, the skin 5 cm proximal to the superior aspect of the patella was resected, and the thigh musculature (quadriceps, biceps femoris, semitendinosus, semimembranosus, and gracilis) was identified and rasped to remove muscle tissue. All other musculature was resected. The denuded tendons (quadriceps, medial hamstrings, gracilis, and lateral hamstrings) were then placed into separate cable clamps and secured with U-bolts such that tension could be applied along the loading axis of the tendon. The femur was then resected 20 cm proximal to the superior patella, and the distal end of the femur was potted with Bondo (3M) aligned with the long axis of the bone in a 2 inch–inner diameter cylinder.
Of the 45 available specimens (22 male and 23 female), 6 were excluded from final analysis because of poor data quality from equipment failure (eg, nonbiomechanical damage to the ACL from the sensor), mechanical weakness due to specimen preparation (eg, tibial fixture screw was the cause of a tibial fracture), or a nonfunctional ACL determined by a board-certified orthopaedic surgeon (A.J.K.). Data analyses were therefore performed on 39 specimens (mean age, 41.5 ± 8.4 years; mean weight, 85.7 ± 25.6 kg; 19 male and 20 female).
In Vivo Input Data for Simulated Impact
Patients consented to participate in this portion of the study according to guidelines of the institutional review board of The Ohio State University. Three-dimensional motion analysis (Motion Analysis Corp) of the DVJ task was performed with 67 healthy patients who participate in sport activities (39 male and 28 female; mean age, 23.2 ± 3.9 years; mean weight, 73.3 ± 13.4 kg). After applying a 12-Hz low-pass fourth-order Butterworth filter, kinematic and kinetic variables were calculated using inverse dynamics and customized software (Matlab; MathWorks) and Visual3D (C-Motion) to determine values of tertiles of the injury risk (ie, low, medium, and high) in 3 degrees of knee dynamics: KAM, ATS, and ITR. Previous work has demonstrated that tertiles of the risk were evident by a cluster analytic technique, latent profile analysis, in which participants were grouped into distinct profiles based on a priori biomechanical characteristics of the DVJ.15 These calculated forces and moments were utilized across tertiles of the risk in a randomized order as inputs into the applied external loads for impact testing for a total of 46 conditions (Table 1).7 If all 46 randomized conditions did not result in soft or hard tissue failure of the specimen, then the values of KAM, ATS, and ITR were all increased by 20% for each successive impact until a failure event occurred.
TABLE 1.
Load Magnitudes Based on In Vivo Population Percentage7
| Population Percentage | Knee Abduction Moment, N·m | Internal Tibial Rotation, N·m | Anterior Tibial Shear, N |
|---|---|---|---|
| 0 | 1.7 | 1.0 | 47 |
| 33 | 13.5 | 9.7 | 64 |
| 67 | 26.8 | 18.6 | 80 |
| 100 | 57.3 | 53.7 | 196 |
Cadaveric Impactor
A custom-designed cadaveric impactor was utilized to simulate athletic DVJs in lower extremities (Figure 1).7 Pneumatic cylinders applied the designated knee forces/moments calculated from the in vivo participants and applied muscular forces to the quadriceps and hamstring tendons at a 1:1 ratio (444 N applied to both the quadriceps and hamstring). The calculated forces and torques (Table 1) were applied in a randomized order to the tibia before the release of a gravity-driven drop sled of 0.5 body weight (34 kg) from a height of 31 cm. Resultant axial loading from the simulated DVJ consistently approximated 4 kN. Single-axis and 6-axis load cells recorded the vertical ground-reaction force and forces and moments at the knee, respectively. In addition, 2 differential variable reluctance transducers (DVRTs) were implanted into the MCL and ACL, respectively, for measurements of ligament strain during simulation.8 Although there can be a large variability in measurements obtained from DVRTs, sensor placement and calibrations were consistently performed to maintain high confidence in the data reported. To provide additional space in the femoral notch for the DVRT sensors, notchplasty procedures were performed if the intercondylar space was deemed to potentially inhibit DVRT implantation or impinge the DVRT during the testing protocol.
Figure 1.
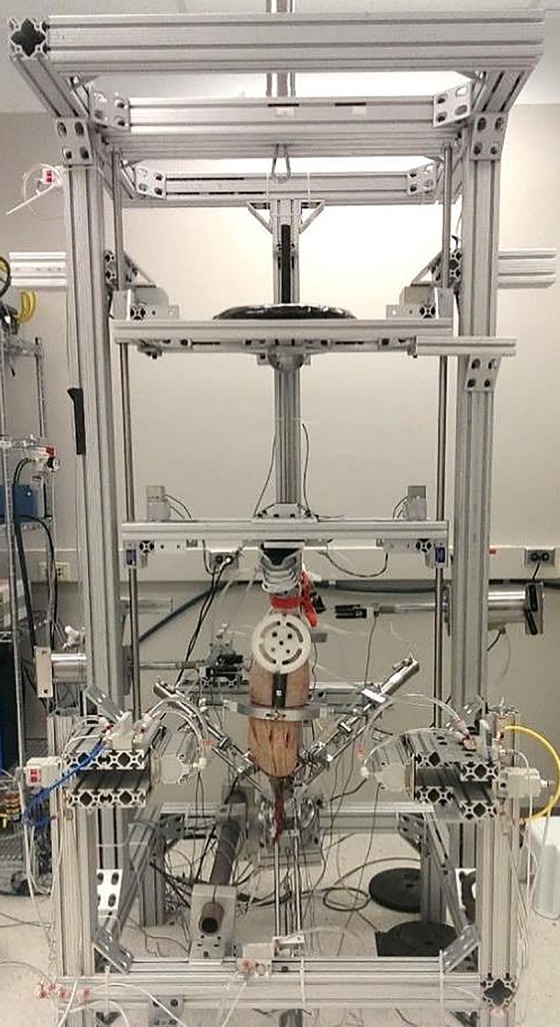
Custom-designed cadaveric impact simulator. The impact simulator applies external loads via programmatically controlled pneumatic cylinders and supplies a gravity-driven sled with customizable height and weight. Figure reproduced from Bates et al.7 Used with permission from Elsevier.
All limbs were oriented in the impactor at 25° to the vertical sagittal plane. A knee flexion angle of 25° is representative of initial contact (IC) knee orientation in young athletes landing from a drop height of 31 cm.3 The long axis of the tibia was then aligned with the axis of impact in both the frontal and sagittal planes. At impact, the limb was allowed to move freely in all planes, although movement was relatively restricted in the sagittal plane. After each impact, the limb was reset so that the long axis of the tibia aligned with the axis of impact again.
Impactor data were collected from load cells and DVRTs at 10 kHz with custom-designed LabVIEW software (National Instruments). During data collection, the software triggered the pneumatic cylinders for external loading/unloading and the electromagnet release of the drop sled to deliver the impact. All data were filtered with a 12-Hz low-pass fourth-order Butterworth filter and then postprocessed with LabVIEW and Matlab.
Data Analysis
Five conditions of the 46 randomized conditions available were analyzed for this study: (1) 0% KAM, 0% ATS, 0% ITR (“00_00_00”), (2) 67% KAM, 67% ATS, 67% ITR (“67_67_67”), (3) the condition in which each specimen experienced maximum ACL strain (“maximum ACL strain”), (4) the condition in which each specimen experienced maximum MCL strain (“maximum MCL strain”), and (5) the condition before specimen failure (“prefailure”). Failure was defined as any soft or hard tissue damage that rendered the specimen unable to pursue further evaluations. Thus, with the latter 3 conditions, the amount of KAM, ATS, and ITR may vary across each specimen, but the data were sorted specifically by which condition produced the highest amount of ACL or MCL strain. The 00_00_00 condition was selected for baseline ligament strain considerations with minimal loading, and the 67_67_67 condition was selected for its high loads in all 3 planes and increased statistical power with greater specimen data compared with a 100_100_100 condition. Maximum, IC, and postimpact (33, 66, and 100 milliseconds) outcomes of both ACL and MCL strains were analyzed during these selected 5 conditions. For subsequent analysis, we normalized the strain data to baseline strain values.
Statistical Analysis
Statistical analyses were performed with JMP 10 (SAS Institute) with utilization of 1-way analysis of variance (ANOVA), 2-way repeated-measures ANOVA, and the Fisher exact test. The Fisher exact test was utilized for statistical analysis of specimen demographics. For all 2-way repeated-measures ANOVAs, we compared sex (male and female) by load (00_00_00, 67_67_67, and prefailure). Statistical significance was set at P < .05.
Results
Demographics
Specimen demographics were similar across sexes for age, body mass index (BMI), limb side, and dominant limb. There were expected significant anthropometric differences of increased body weight and height in male specimens (Table 2). Although the male specimens had significantly increased weight and height over female specimens, the sexes were equivalent in terms of BMI (Table 2). As strain is unitless, there is no normalization necessary for sex differences in terms of weight and height.
TABLE 2.
Specimen Demographics by Sexa
| Male (n = 19) | Female (n = 20) | P Value | |
|---|---|---|---|
| Age, y | 43.1 ± 7.7 | 40.0 ± 9.0 | .249 |
| Weight, kg | 95.4 ± 19.3 | 76.5 ± 27.8 | .019 |
| Height, cm | 181.7 ± 5.4 | 165.4 ± 7.5 | <.001 |
| Body mass index, kg/m2 | 29.1 ± 6.5 | 27.7 ± 9.6 | .612 |
| Limb side, left:right, n | 8:11 | 11:9 | .527 |
| Dominant limb, left:right, n | 5:14 | 3:17 | .451 |
aData are presented as mean ± SD unless otherwise indicated. Age of specimens ranged from 24 to 52 years. Bolded values indicate statistically significant differences between sexes (P < .05).
ACL Failures
Of the 39 specimens, 38 experienced some type of hard or soft tissue failure from the DVJ simulation during the randomized protocol. Of these, 34 suffered ACL ruptures (17 male and 17 female). The ACL failures were distributed clinically, with 71% occurring on the femoral side, 21% at the midsubstance, and 9% on the tibial side.
Maximum Ligament Strains
There was no significant difference in maximum ACL strain between male (13.2%) and female (16.7%) specimens in the condition of maximum ACL strain (F 1,38 = 1.837, P = .184). Similarly, there was no significant difference in maximum MCL strain between male (7.1%) and female (5.4%) specimens in the condition of maximum MCL strain (F 1,38 = 1.056, P = .311) (Table 3). With maximum strain normalized to baseline (strain at the initiation of data collection), ACL strain still failed to achieve significance (F 1,38 = 3.306, P = .077) with female specimens (11.5%) compared with male specimens (7.6%). MCL strain similarly lacked a significant effect (F 1,38 = 2.090, P = .157) between female (3.9%) and male (6.1%) specimens.
TABLE 3.
Absolute ACL and MCL Strains by Sex With 1-Way Analysis of Variancea
| n | Raw | Normalized to Baseline | |||
|---|---|---|---|---|---|
| Mean ± SD, % | P | Mean ± SD, % | P | ||
| Maximum ACL strain | .184 | .077 | |||
| Male | 19 | 13.2 ± 8.1 | 7.6 ± 3.3 | ||
| Female | 20 | 16.7 ± 8.3 | 11.5 ± 8.7 | ||
| Maximum MCL strain | .311 | .157 | |||
| Male | 19 | 7.1 ± 5.8 | 6.1 ± 5.7 | ||
| Female | 20 | 5.4 ± 4.6 | 3.9 ± 3.2 | ||
| 00_00_00 | |||||
| Maximum ACL strain | .230 | .204 | |||
| Male | 19 | 6.9 ± 7.6 | 4.0 ± 4.4 | ||
| Female | 14 | 10.3 ± 8.0 | 6.8 ± 8.0 | ||
| Maximum MCL strain | .326 | .795 | |||
| Male | 19 | 1.7 ± 1.3 | 1.1 ± 1.1 | ||
| Female | 14 | 2.6 ± 3.4 | 1.2 ± 1.3 | ||
| ACL strain at IC | .736 | .221 | |||
| Male | 19 | 3.0 ± 5.5 | 0.0 ± 0.0 | ||
| Female | 14 | 3.5 ± 3.2 | 0.0 ± 0.0 | ||
| ACL strain at 33 ms | .552 | .119 | |||
| Male | 19 | 3.2 ± 5.9 | 0.2 ± 0.6 | ||
| Female | 14 | 4.2 ± 3.1 | 0.7 ± 1.2 | ||
| ACL strain at 66 ms | .224 | .175 | |||
| Male | 19 | 6.2 ± 7.5 | 3.2 ± 3.8 | ||
| Female | 14 | 9.4 ± 7.2 | 5.9 ± 7.1 | ||
| ACL strain at 100 ms | .323 | .368 | |||
| Male | 19 | 4.8 ± 5.8 | 1.8 ± 3.7 | ||
| Female | 14 | 6.9 ± 5.8 | 3.4 ± 5.8 | ||
| 67_67_67 | |||||
| Maximum ACL strain | .170 | .136 | |||
| Male | 19 | 7.7 ± 6.2 | 4.7 ± 3.6 | ||
| Female | 16 | 11.0 ± 7.7 | 7.6 ± 7.2 | ||
| Maximum MCL strain | .304 | .741 | |||
| Male | 19 | 2.4 ± 2.0 | 2.1 ± 1.9 | ||
| Female | 16 | 3.6 ± 4.4 | 2.3 ± 2.5 | ||
| ACL strain at IC | .176 | .056 | |||
| Male | 19 | 3.3 ± 4.3 | 0.3 ± 0.5 | ||
| Female | 16 | 5.6 ± 5.6 | 2.2 ± 4.1 | ||
| ACL strain at 33 ms | .177 | .054 | |||
| Male | 19 | 3.6 ± 4.9 | 0.7 ± 1.1 | ||
| Female | 16 | 6.1 ± 5.6 | 2.7 ± 4.2 | ||
| ACL strain at 66 ms | .123 | .079 | |||
| Male | 19 | 6.0 ± 6.8 | 3.0 ± 3.7 | ||
| Female | 16 | 9.8 ± 7.4 | 6.4 ± 7.1 | ||
| ACL strain at 100 ms | .146 | .106 | |||
| Male | 19 | 5.0 ± 4.8 | 2.0 ± 2.5 | ||
| Female | 16 | 7.8 ± 6.3 | 4.4 ± 5.5 | ||
| Prefailure | |||||
| Maximum ACL strain | .214 | .213 | |||
| Male | 19 | 12.0 ± 7.9 | 7.7 ± 3.4 | ||
| Female | 19 | 15.2 ± 7.6 | 10.3 ± 8.3 | ||
| Maximum MCL strain | .713 | .167 | |||
| Male | 19 | 5.1 ± 4.0 | 4.3 ± 3.3 | ||
| Female | 19 | 4.6 ± 4.3 | 2.9 ± 2.7 | ||
| ACL strain at IC | .700 | .874 | |||
| Male | 19 | 6.8 ± 5.9 | 2.6 ± 2.4 | ||
| Female | 19 | 7.5 ± 5.2 | 2.7 ± 3.1 | ||
| ACL strain at 33 ms | .636 | .723 | |||
| Male | 19 | 7.3 ± 6.3 | 3.1 ± 1.9 | ||
| Female | 19 | 8.2 ± 4.8 | 3.4 ± 3.2 | ||
| ACL strain at 66 ms | .228 | .214 | |||
| Male | 19 | 10.4 ± 8.4 | 6.1 ± 3.8 | ||
| Female | 19 | 13.6 ± 7.7 | 8.7 ± 8.3 | ||
| ACL strain at 100 ms | .328 | .331 | |||
| Male | 19 | 9.8 ± 7.3 | 5.5 ± 3.0 | ||
| Female | 19 | 12.0 ± 6.7 | 7.2 ± 6.9 | ||
aBecause all tests were randomized, n values may differ from the original value (n = 39) as some tests were not able to be performed before knee ligament damage. Because maximum MCL strain lacked demonstrable sex differences in the controlled external load conditions (ie, 00_00_00, 67_67_67, and prefailure), the MCL time values were excluded. ACL, anterior cruciate ligament; IC, initial contact; MCL, medial collateral ligament.
For overall ACL strain across all controlled external load conditions (ie, 00_00_00, 67_67_67, and prefailure), 2-way repeated-measures ANOVA compared the effect of sex and load at maximum, IC, 33 milliseconds, 66 milliseconds, and 100 milliseconds and demonstrated a significance of sex (F 1,100 = 4.188, P = .043) and load (F 2,100 = 5.9669, P = .004) but not sex × load (F 2,100 = 0.068, P = .935). Across all controlled external load conditions, maximum ACL strain differed by at least 3.2% between sexes, with increased strain for female specimens (Table 3). For overall MCL strain across all controlled external load conditions, 2-way repeated-measures ANOVA compared the effect of sex and load at maximum, IC, 33 milliseconds, 66 milliseconds, and 100 milliseconds and demonstrated a significance of load (F 2,100 = 5.1956, P = .007) but not sex (F 1,100 = 0.851, P = .358) or sex × load (F 2,100 = 0.990, P = .375). Across all controlled external load conditions, maximum MCL strain differed by at least 0.5% between sexes, with increased strain for female specimens (Table 3).
Strain normalized to baseline and IC values was also evaluated from maximum strain values across all controlled external load conditions. The data are summarized in Table 4. Across all controlled external load conditions, 2-way repeated-measures ANOVA compared IC-normalized ACL strain of the effect of sex and load at maximum, 33 milliseconds, 66 milliseconds, and 100 milliseconds and demonstrated a lack of significance of sex (F 1,100 = 3.133, P = .080), load (F 2,100 = 0.740, P = .480), and sex × load (F 2,100 = 0.170, P = .844). Maximum ACL strain from IC differed by 2.1% between sexes, with increased strain for female specimens. Similarly, 2-way repeated-measures ANOVA compared baseline-normalized ACL strain of the effect of sex and load at maximum, IC, 33 milliseconds, 66 milliseconds, and 100 milliseconds and demonstrated a significance of sex (F 1,100 = 6.194, P = .015) and load (F 2,100 = 6.669, P = .002) but not sex × load (F 2,100 = 0.207, P = .814). Maximum ACL strain from baseline differed by 2.7% between sexes, with increased strain for female specimens.
TABLE 4.
P Values of ACL and MCL Strains With Repeated-Measures Analysis of Variancea
| Maximum ACL Strain | Maximum MCL Strain | |
|---|---|---|
| Raw | ||
| Sex | .043 | .358 |
| Load | .004 | .007 |
| Sex × load | .935 | .375 |
| Normalized to initial contact | ||
| Sex | .080 | .574 |
| Load | .480 | .284 |
| Sex × load | .844 | .904 |
| Normalized to baseline | ||
| Sex | .015 | .185 |
| Load | .002 | <.001 |
| Sex × load | .814 | .036 |
aRepeated measures were the conditions of 00_00_00, 67_67_67, and prefailure across time. Bolded values indicate statistical significance (P < .05). ACL, anterior cruciate ligament; MCL, medial collateral ligament.
Across all controlled external load conditions for MCL strain, 2-way repeated-measures ANOVA compared IC-normalized MCL strain of the effect of sex and load at maximum, 33 milliseconds, 66 milliseconds, and 100 milliseconds and demonstrated no significance of sex (F 1,100 = 0.319, P = .574), load (F 2,100 = 1.275, P = .284), or sex × load (F 2,100 = 0.101, P = .904). Maximum MCL strain from IC differed by 0.1% between sexes, with increased strain for female specimens. Moreover, 2-way repeated-measures ANOVA compared baseline-normalized MCL strain of the effect of sex and load at maximum, IC, 33 milliseconds, 66 milliseconds, and 100 milliseconds and demonstrated a significance of load (F 2,100 = 12.998, P < .001) and sex × load (F 2,100 = 3.437, P = .036) but not sex (F 1,100 = 1.785, P = .185). Maximum MCL strain from baseline differed by 0.4% between sexes, with increased strain for male specimens.
With all specimens in a similar high external load condition (67_67_67), maximum ACL strain was increased in female specimens by 3.3% compared with male specimens; however, this value was not statistically significant (F 1,38 = 1.970, P = .170). Maximum MCL strain was not significant between sexes (F 1,38 = 1.091, P = .304).
Discussion
Although it did not achieve statistical significance, the absolute maximum increase of strain for female specimens was 3.9% compared with male specimens in the condition of maximum ACL strain. Maximum ACL strain during controlled external load conditions consistently demonstrated 3.2% greater strain in female specimens compared with male specimens (Table 3), although this value was also not statistically significant. Additionally, female specimens had greater ACL strain than male specimens at IC as well as at 33, 66, and 100 milliseconds after impact (Table 3). To offset the wide variability in measurements that can exist with DVRTs, increased power with repeated-measures analysis and appropriate normalization to baseline strain values (effectively reducing strain noise) can improve the overall analysis and appropriately address the true strain experienced by the ligaments. With repeated-measures ANOVA that compared the effects of both sex and load, the values of increased ACL strain by sex (male vs female) achieved significance (P = .043) (Table 4). This effect was even more pronounced once normalization of strain to baseline was performed. On the contrary, the opposite was true with normalization to IC; the lack of significance with IC normalization is logical, as the external loads applied to the specimens before ground impact increase strain on the ligaments before IC and thus would reduce the difference from maximum strain and IC (ie, reduce the signal-to-noise ratio).
Strain is often a difficult biomechanical concept, as it is a unitless measure calculated by displacement over displacement. All materials, including ligaments, have a limit of displacement (strain) that they can encounter before failure. Consequently, as female patients encounter increased values of strain over those of male patients, they are at a higher risk for ACL failure as strain approximates the limit of failure. Thus, although 3.2% to 3.9% increased ligament strain in female patients may not be statistically significant, it may be clinically meaningful. However, according to our knowledge and grasp of the current scientific literature, there are currently no minimal clinically important difference10 guidelines for ACL strain. Future studies should seek to establish a minimal clinically important difference of ACL strain for clinical use. Altogether, this information is important, as it demonstrates that female specimens, when loaded similarly to male specimens, experience additional strain on the ACL. Given that the mechanical environment was similar for both sexes with these simulations, these data demonstrate that the higher ACL strain of female specimens is caused by ligament biology, anatomic differences, or muscular stiffness.
With regard to load, it is not surprising that this variable achieved significance for ligament strain in repeated-measures analysis, as there were considerable increases in loading from the 00_00_00, 67_67_67, and prefailure conditions. This variable achieved significance for both the ACL and MCL (Table 4). With 2 variables, there is a potential for an interaction of the variables (ie, sex × load). Sex × load did not demonstrate any significance regarding the ACL, demonstrating a lack of interaction of these variables for the ACL. For the MCL, however, there was a significant effect of sex × load (P = .036) when normalization to baseline was performed. This indicates that both sex and load variables interact to produce significance for a difference of 0.4% increased strain for male specimens.
The experimental data presented indicate that the likely maximum strain on the ACL occurs before or slightly after 66 milliseconds after impact, as has been reported in the previous literature.6,22,32 Throughout those time points when the ACL experienced large increases of strain, MCL strain did not increase by large amounts and never approached significance between sexes. As the MCL itself bears greater loads at full knee extension than in deep flexion,25,26 the data demonstrate that the MCL is bearing less loads than the ACL at a sagittal knee flexion of 25° and that the ACL is more strained than the MCL in this orientation. Additionally, the ACL resists a greater amount of combinatorial KAM, ATS, and ITR loading (ie, dynamic valgus),31 as is observed by the larger magnitude change in peak ACL strain percentage than peak MCL strain percentage that occurs when external loads are increased. This behavior is congruent with previous literature that examined ACL and MCL strain behavior during simulated athletic tasks.5,6 Most ACL injuries will occur near a knee flexion angle of 20° to 30° given that the majority of athletes will land at this sagittal angle at IC.3,31 Thus, as the current findings demonstrate, the MCL is largely unloaded as the ACL bears an increase in loads at this degree of knee flexion. Further consequences of a lack of neuromuscular control could lead to even greater loads applied to the ACL as joint forces and moments increase.
In a trial of consistent loading across all specimens (67_67_67), the MCL experienced 2.4% to 3.6% strain, whereas the ACL experienced 7.7% to 11.0% strain, with the larger values occurring with female specimens (see Table 3). This is of interest, as in this condition, the knee was heavily loaded with knee abduction torques, and the MCL demonstrated lower values of strain than the ACL, which further demonstrates that the ACL is a significant restraint of the combined loads of KAM, ATS, and ITR.
The male specimens in this study anthropometrically had longer levers and increased weight (see Table 1), both factors that would lead to an increase in joint moments. Both male and female specimens were simulated in drop landings with a 1:1 hamstring-to-quadriceps ratio, a 34-kg drop weight at 31 cm, and precise external loads calculated from tertiles of the injury risk from in vivo participants and applied dynamically via pneumatic cylinders. Despite all of these similar parameters of experimentation and equivalency of BMI, the female specimens exhibited an increase in ACL strain compared with male specimens. Although there are certainly neuromuscular contributions to ACL injury mechanisms3,4,16 that could not be simulated in real time in the experimental protocol, the present findings demonstrate that there are mechanical differences that may predispose female patients to ACL injuries compared with male patients.
This novel, pneumatically driven external loading/gravity-driven cadaveric impactor is capable of producing clinically relevant ACL ruptures with a high rate of success.7 In the current study, there were 34 ACL ruptures (17 male and 17 female; 25 femoral avulsions, 7 midsubstance ruptures, and 2 tibial avulsions) in the 39 specimens (87.2%) included in this analysis, as verified by a board-certified orthopaedic surgeon (A.J.K.). Five of the specimens (2 male and 3 female) survived all testing procedures without an ACL rupture, but 4 of the 5 experienced other soft or hard tissue failure. Consequently, the impactor induced physiologically relevant forces and moments encountered by athletes in typical sport maneuvers of cutting, pivoting, and landing and thus relevant ACL and MCL strains. Many previous impactors have failed to reproduce clinically relevant ruptures in a multiplanar system in a physiologically relevant gravity-driven environment.2,32,36 Consequently, with a high degree of certainty, this cadaveric impactor utilized a dynamic multiplanar knee injury simulation that is highly relevant to loading seen in typical sport maneuvers of landing, cutting, and pivoting.27,36
The current data reported indicate that even with high levels of knee abduction loading, the ACL bears more loads than the MCL during functional movement of the DVJ.6 This is of high interest, as it has been disputed that knee abduction would cause simultaneous loading of both the ACL and MCL and lead to concomitant injuries.32,42 The current data demonstrate that even with high-level knee abduction loading at 25° of knee flexion, the ACL bears significantly more loads than the MCL and thus can be loaded and strained to the limit to produce ligamentous ruptures without injuries to the MCL (see Table 3). Further studies should be performed to evaluate the load that is borne by the MCL subsequent to an ACL rupture.
With the understanding that there may be hormonal, genetic, anatomic, and neuromuscular differences that can contribute to mechanical differences of ACL injuries in patients,17,35,40 continued data analyses will evaluate the anatomic variance to elucidate the possibility that these factors contribute to ACL strain. Unfortunately, these cadaveric analyses will not be able to differentiate genetic or hormonal differences aside from sex hormone differences that occur between sexes (ie, estrogen vs testosterone). Future studies will assess the variability that occurs between sexes with different planes of loading (ie, KAM, ATS, and ITR) in a multiplanar system to determine whether there are differences in the mechanics between sexes as well as changes in the parameters of sagittal flexion and the hamstring-to-quadriceps ratio.
A significant limitation of this study is the large variability in measurements that DVRTs are known to exhibit when implanted in soft tissue structures.6,8 This variability may have resulted in a lack of significance of results that are truly significant. As a result, femoral notch impingement effects for ACL injuries could not be studied. A cadaveric study is typically limited by the number of specimens that can be tested to increase statistical power such as in a clinical trial. Although this study had a large number of cadaveric specimens compared with those typically seen in other studies, the results reported here may still be underpowered statistically. Consequently, although some uncertainty still remains in these reported data because of a lack of statistical power, it is clear that there are definitive differences and potential clinical significance in ligamentous loading between male and female patients, especially of the ACL. Understanding these sex differences is imperative to improve future clinical treatments that can be individualized and sex specific.
Conclusion
Female specimens exhibited greater mean values of ACL strain at maximum, IC, and after impact (33, 66, and 100 milliseconds) than male specimens during similar loading conditions. Strain increases were in the magnitude of approximately 3.5% for female specimens compared with male specimens. During these same loading conditions, there were minimal observed differences of MCL loading between sexes, and only a minimal increase of MCL loading occurred during the impact forces. These increased strain values for female specimens may account for the increased risk that female patients have for ACL injuries.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.J.K. is a paid consultant for Arthrex and DePuy Orthopaedics, receives royalties from Arthrex, and serves on the medical board of trustees for the Musculoskeletal Transplant Foundation. Funding for this study was provided by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01AR056259 and R01AR055563 [to T.E.H.], T32AR056950 [to C.V.N.], and L30AR070273 [to N.D.S.]) and from the National Institute of Child Health and Human Development (K12HD065987 [to N.D.S.]).
Ethical approval for this study was waived by the Mayo Clinic Institutional Review Board.
References
- 1. Arendt EA, Agel J, Dick R. Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train. 1999;34(2):86–92. [PMC free article] [PubMed] [Google Scholar]
- 2. Bakker R, Tomescu S, Brenneman E, Hangalur G, Laing A, Chandrashekar N. Effect of sagittal plane mechanics on ACL strain during jump landing. J Orthop Res. 2016;34(9):1636–1644. [DOI] [PubMed] [Google Scholar]
- 3. Bates NA, Ford KR, Myer GD, Hewett TE. Kinetic and kinematic differences between first and second landings of a drop vertical jump task: implications for injury risk assessments? Clin Biomech (Bristol, Avon). 2013;28(4):459–466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bates NA, Myer GD, Shearn JT, Hewett TE. Anterior cruciate ligament biomechanics during robotic and mechanical simulations of physiologic and clinical motion tasks: a systematic review and meta-analysis. Clin Biomech (Bristol, Avon). 2015;30(1):1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bates NA, Nesbitt RJ, Shearn JT, Myer GD, Hewett TE. Knee abduction affects greater magnitude of change in ACL and MCL strains than matched internal tibial rotation in vitro. Clin Orthop Relat Res. 2017;475(10):2385–2396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bates NA, Nesbitt RJ, Shearn JT, Myer GD, Hewett TE. Relative strain in the anterior cruciate ligament and medial collateral ligament during simulated jump landing and sidestep cutting tasks: implications for injury risk. Am J Sports Med. 2015;43(9):2259–2269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bates NA, Schilaty ND, Nagelli CV, Krych AJ, Hewett TE. Novel mechanical impact simulator designed to generate clinically relevant anterior cruciate ligament ruptures. Clin Biomech (Bristol, Avon). 2017;44:36–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Beynnon B, Howe JG, Pope MH, Johnson RJ, Fleming BC. The measurement of anterior cruciate ligament strain in vivo. Int Orthop. 1992;16(1):1–12. [DOI] [PubMed] [Google Scholar]
- 9. Blackburn JT, Norcross MF, Padua DA. Influences of hamstring stiffness and strength on anterior knee joint stability. Clin Biomech (Bristol, Avon). 2011;26(3):278–283. [DOI] [PubMed] [Google Scholar]
- 10. Cook CE. The minimal clinically important change score (MCID): a necessary pretense. J Man Manip Ther. 2008;16(4):E82–E83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2008;8:141–150. [DOI] [PubMed] [Google Scholar]
- 12. Hashemi J, Breighner R, Chandrashekar N, et al. Hip extension, knee flexion paradox: a new mechanism for non-contact ACL injury. J Biomech. 2011;44(4):577–585. [DOI] [PubMed] [Google Scholar]
- 13. Hewett TE, Bates NA. Preventive biomechanics: a paradigm shift with a translational approach to injury prevention. Am J Sports Med. 2017;45(11):2654–2664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Hewett TE, Ford KR, Hoogenboom BJ, Myer GD. Understanding and preventing ACL injuries: current biomechanical and epidemiologic considerations—update 2010. North Am J Sport Phys Ther. 2010;5(4):234–251. [PMC free article] [PubMed] [Google Scholar]
- 15. Hewett TE, Ford KR, Xu YY, Khoury J, Myer GD. Utilization of ACL injury biomechanical and neuromuscular risk profile analysis to determine the effectiveness of neuromuscular training. Am J Sports Med. 2016;44(12):3146–3151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501. [DOI] [PubMed] [Google Scholar]
- 17. Hewett TE, Myer GD, Ford KR, Paterno MV, Quatman CE. Mechanisms, prediction, and prevention of ACL injuries: cut risk with three sharpened and validated tools. J Orthop Res. 2016;34(11):1843–1855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Hewett TE, Myer GD, Ford KR, Paterno MV, Quatman CE. The 2012 ABJS Nicolas Andry Award. The sequence of prevention: a systematic approach to prevent anterior cruciate ligament injury. Clin Orthop Relat Res. 2012;470(10):2930–2940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43(6):417–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Karakaya İÇ, Karakaya MG. Proprioception and gender In: Kaya D, ed. Proprioception: The Forgotten Sixth Sense. Foster City, CA: OMICS Group eBooks; 2014. [Google Scholar]
- 21. Kiapour AM, Demetropoulos CK, Kiapour A, et al. Strain response of the anterior cruciate ligament to uniplanar and multiplanar loads during simulated landings: implications for injury mechanism. Am J Sports Med. 2016;44(8):2087–2096. [DOI] [PubMed] [Google Scholar]
- 22. Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35(3):359–367. [DOI] [PubMed] [Google Scholar]
- 23. Levine JW, Kiapour AM, Quatman CE, et al. Clinically relevant injury patterns after an anterior cruciate ligament injury provide insight into injury mechanisms. Am J Sports Med. 2012;41(2):385–395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Mall NA, Chalmers PN, Moric M, et al. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42(10):2363–2370. [DOI] [PubMed] [Google Scholar]
- 25. Mancini EJ, Kohen R, Esquivel AO, Cracchiolo AM, Lemos SE. Comparison of ACL strain in the MCL-deficient and MCL-reconstructed knee during simulated landing in a cadaveric model. Am J Sports Med. 2017;45(5):1090–1094. [DOI] [PubMed] [Google Scholar]
- 26. Matsumoto H, Suda Y, Otani T, Niki Y, Seedhom B, Fujikawa K. Roles of the anterior cruciate ligament and the medial collateral ligament in preventing valgus instability. J Orthop Sci. 2001;6(1):28–32. [DOI] [PubMed] [Google Scholar]
- 27. McLean SG, Huang X, Su A, Van Den Bogert AJ. Sagittal plane biomechanics cannot injure the ACL during sidestep cutting. Clin Biomech (Bristol, Avon). 2004;19(8):828–838. [DOI] [PubMed] [Google Scholar]
- 28. Myer GD, Ford KR, Hewett TE. The effects of gender on quadriceps muscle activation strategies during a maneuver that mimics a high ACL injury risk position. J Electromyogr Kinesiol. 2005;15(2):181–189. [DOI] [PubMed] [Google Scholar]
- 29. Myer GD, Ford KR, Khoury J, Succop P, Hewett TE. Biomechanics laboratory-based prediction algorithm to identify female athletes with high knee loads that increase risk of ACL injury. Br J Sports Med. 2011;45(4):245–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Pappas E, Shiyko MP, Ford KR, Myer GD, Hewett TE. Biomechanical deficit profiles associated with ACL injury risk in female athletes. Med Sci Sports Exerc. 2016;48(1):107–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Quatman CE, Hewett TE. The anterior cruciate ligament injury controversy: is “valgus collapse” a sex-specific mechanism? Br J Sports Med. 2009;43(5):328–335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Quatman CE, Kiapour AM, Demetropoulos CK, et al. Preferential loading of the ACL compared with the MCL during landing: a novel in sim approach yields the multiplanar mechanism of dynamic valgus during ACL injuries. Am J Sports Med. 2014;42(1):177–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Quatman CE, Quatman-Yates CC, Hewett TE. A “plane” explanation of anterior cruciate ligament injury mechanisms: a systematic review. Sports Med. 2010;40(9):729–746. [DOI] [PubMed] [Google Scholar]
- 34. Renström PA. Eight clinical conundrums relating to anterior cruciate ligament (ACL) injury in sport: recent evidence and a personal reflection. Br J Sports Med. 2013;47(6):367–372. [DOI] [PubMed] [Google Scholar]
- 35. Sbriccoli P, Solomonow M, Zhou B-H, Lu Y, Sellards R. Neuromuscular response to cyclic loading of the anterior cruciate ligament. Am J Sports Med. 2005;33(4):543–551. [DOI] [PubMed] [Google Scholar]
- 36. Schilaty ND, Bates NA, Hewett TE. Letter to the editor: effect of sagittal plane mechanics on ACL strain during jump landing. J Orthop Res. 2017;35(6):1171–1172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Schilaty ND, Bates NA, Sanders TL, Krych AJ, Stuart MJ, Hewett TE. Incidence of second anterior cruciate ligament tears (1990 - 2000) and associate factors by geographic locale. Am J Sports Med. 2017;45(7):1567–1573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Schilaty ND, Nagelli CV, Hewett TE. Use of objective neurocognitive measures to assess the psychological states that influence return to sport following injury. Sports Med. 2015;46(3):299–303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Shin CS, Chaudhari AM, Andriacchi TP. Valgus plus internal rotation moments increase anterior cruciate ligament strain more than either alone. Med Sci Sports Exerc. 2011;43(8):1484–1491. [DOI] [PubMed] [Google Scholar]
- 40. Shultz SJ, Schmitz RJ, Benjaminse A, Chaudhari AM, Collins M, Padua DA. ACL Research Retreat VI: an update on ACL injury risk and prevention. J Athl Train. 2012;47(5):591–603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Wang D, De Vito G, Ditroilo M, Fong DTP, Delahunt E. A comparison of muscle stiffness and musculoarticular stiffness of the knee joint in young athletic males and females. J Electromyogr Kinesiol. 2015;25(3):495–500. [DOI] [PubMed] [Google Scholar]
- 42. Yu B, Garrett WE. Mechanisms of non-contact ACL injuries. Br J Sports Med. 2007;41(suppl 1):i47–i51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in neuromuscular control of the trunk predict knee injury risk: a prospective biomechanical-epidemiologic study. Am J Sports Med. 2007;35(7):1123–1130. [DOI] [PubMed] [Google Scholar]