

Abstract
The purpose of this systematic review and meta‐analysis was to critically review the (1) prevalence of alcohol mixed with energy drink (AMED) consumption, (2) motives for AMED consumption, (3) correlates of AMED consumption, and (4) whether AMED consumption has an impact on (a) alcohol consumption, (b) subjective intoxication, and (c) risk‐taking behavior.
Overall a minority of the population consumes AMED, typically infrequently. Motives for AMED consumption are predominantly hedonistic and social. Meta‐analyses revealed that AMED consumers drink significantly more alcohol than alcohol‐only (AO) consumers. Within‐subject comparisons restricted to AMED consumers revealed that alcohol consumption does not significantly differ between typical AMED and AO occasions. On past month heaviest drinking occasions, AMED users consume significantly less alcohol on AMED occasions when compared to AO occasions. AMED consumers experience significantly fewer negative consequences and risk‐taking behavior on AMED occasions compared with AO occasions. Meta‐analyses of subjective intoxication studies suggest that AMED consumption does not differentially affect subjective intoxication when compared to AO consumption. In conclusion, when compared to AO consumption, mixing alcohol with energy drink does not affect subjective intoxication and seems unlikely to increase total alcohol consumption, associated risk‐taking behavior, nor other negative alcohol‐related consequences. Further research may be necessary to fully reveal the effects of AMED.
Keywords: alcohol, alcohol mixed with energy drink (AMED), negative consequences, risk taking, subjective intoxication
1. INTRODUCTION
Since their introduction, energy drinks have become increasingly popular. Energy drinks are nonalcoholic beverages that currently constitute less than 5% of the soft drink market.
Energy drinks contain caffeine and other functional ingredients such as glucose, B‐vitamins, glucuronolactone, and taurine. Sometimes, these are complemented with herbal extracts such as ginseng, Ginkgo biloba, and guaraná. There is some evidence that caffeine and glucose may have additive effects on aspects of cognitive performance (Scholey and Kennedy, 2004). Limited studies into the effects of other ingredients conclude that caffeine is largely responsible for most cognitive effects of energy drinks (Giles et al., 2012; Peacock, Bruno, & Martin, 2013. In addition, caffeine consumption via energy drinks, especially when mixed with alcohol, has raised several concerns discussed in this systematic review.
Whereas popular energy drinks such as Red Bull (250 ml, 8.4 oz) contain 80 mg of caffeine, comparable to the amount of caffeine present in one regular cup of coffee, some energy drinks contain substantially higher levels. Despite the increasing popularity of energy drinks, consumption trends for adults show that total daily caffeine intake has remained stable over the past decade (Verster & Konig, 2017). The introduction of energy drinks has not resulted in an increase in total daily caffeine consumption. In fact, total caffeine consumption of children younger than 12 years has significantly declined over the past 10 years, and adolescent caffeine consumption has remained stable (Verster & Konig, 2017). Among children and adolescents, however, over the past 15 years, a significant reduction of caffeinated soft drink consumption is seen, accompanied by an increase of coffee consumption (Verster & Konig, 2017).
In line with previous assessments (Health Canada, 2010; Nawrot, Jordan, Eastwood, et al., 2003), the European Food Safety Authority concluded that, for adults, caffeine consumption up to 400 mg per day does not give rise to safety concerns (European Food Safety Authority, 2015). For children and adolescents, not exceeding 3 mg/kg body weight per day was recommended, and for pregnant women, maximum daily caffeine intake was set at 200 mg per day. The recent review by Verster and Konig (2017) shows that across the world, average daily caffeine intake is below these levels. The contribution of energy drinks to total caffeine intake is relatively low across all age groups.
Nevertheless, some researchers and health organizations have expressed concern regarding the potential health risks associated with mixing alcohol and energy drink. On the basis of the existing literature, Verster, Aufricht, and Alford (2012) identified three potential health risks:
Mixing alcohol with energy drink would increase total alcohol consumption when compared to consuming alcohol only (AO).
Mixing alcohol with energy drink would mask the intoxication effects caused by alcohol (i.e., alcohol mixed with energy drink [AMED] consumers would feel less intoxicated when mixing alcohol with energy drink than when consuming the same level of AO).
Mixing alcohol with energy drink would result in increased risk‐taking behavior and experiencing negative alcohol‐related consequences (e.g., drunk driving and unprotected sex).
In the 2012 review (Verster et al., 2012), developed by most of this paper's authors, we addressed these three topics and concluded that “Although some reports suggest that energy drinks lead to reduced awareness of intoxication and increased alcohol consumption, a review of the available literature shows that these views are not supported by direct or reliable scientific evidence.” Also regarding consumption patterns and their possible negative consequences, it was concluded that supportive research was too limited to be able to draw firm conclusions. We did however postulate that “a personality with higher levels of risk‐taking behavior may be the primary reason for increased alcohol and drug abuse per se” with “the co‐consumption of energy drinks being one of the many expressions of that type of lifestyle and personality” (Verster et al., 2012).
Over the past 5 years, a large number of scientific studies have addressed the proposed concerns with consuming AMED as opposed to consuming AO. Here, we revisit those areas with an updated review of the extant literature. This is important, because among both researchers and lay people, there are persisting misconceptions and myths about the effects of mixing alcohol with energy drink that are not supported by scientific evidence.
2. METHODS
A literature search (PubMed, Embase, and PsycLit) was conducted using the keywords “energy drink” and “alcohol,” covering all years up to March 2, 2017. The literature search revealed 1,039 hits. After removing 290 duplicates, a total of 749 papers remained of which the abstracts and full text were screened.
The aim of this review was to give a critical review on (1) the prevalence of AMED consumption, (2) the motives for AMED consumption, (3) the correlates of AMED consumption, and (4) whether AMED consumption has an impact on (a) alcohol consumption, (b) subjective intoxication, and (c) risk‐taking behavior. Articles addressing these topics and providing data were included in this review. Reviews, commentaries, and editorials were not considered, leaving 80 original articles that were included in the current review.
There were sufficient data on alcohol consumption and subjective intoxication to allow meta‐analyses. The meta‐analyses were conducted using the program Comprehensive Meta‐analysis (Biostat Inc., Englewood, NJ, USA; Borenstein & Rothstein, 1999). Studies were included if outcome measures were reported that could be used to calculate effect sizes (ES), such as the mean, standard deviation, and sample size. The ES and corresponding 95% confidence intervals (CIs) were computed for each of the AMED versus AO comparisons. If the 95% CI did not include zero, the ES was considered statistically significant (p < .05). Homogeneity/heterogeneity analyses were performed to determine if each individual ES had the same distribution as the combined overall ES. If the Q statistic resulting from this analysis was not significant (p ≥ .05), a homogenous distribution was assumed and a fixed effects model to perform the meta‐analysis was applied. If not, a random effects model was applied, correcting for variation between the studies (Lipsey & Wilson, 2000).
3. RESULTS
3.1. Prevalence of AMED consumption
Surveys among U.S. students and young adults reported AMED consumption to vary from 8.1% to 64.7% of their cohorts (Berger, Fendrich, & Fuhrman, 2013; Emond, Gilbert‐Diamond, Tanski, & Sargent, 2014; Gonzales, Largo, Miller, Kanny, & Brewer, 2015; Housman, Williams, & Woolsey, 2016; Martz, Patrick, & Schulenberg, 2015; Marzell, Turrisi, Mallett, Ray, & Scaglione, 2014; Miller, 2012; Patrick, Macuada, & Maggs, 2016; Rutledge, Bestrashniy, & Nelson, 2016; Snipes & Benotsch, 2013; Snipes, Green, Javier, Perrin, & Benotsch, 2014; Snipes, Jeffers, Green, & Benotsch, 2015). Among U.S. active‐duty Navy and Marine Corps, 28% reported consuming AMED (Knapik et al., 2016). Reported rates of past year AMED consumption were considerably lower among Canadian student samples, ranging from 17.3% to 20% (Azagba, Langille, & Asbridge, 2013; Milicic & Leatherdale, 2016; Reid, Hammond, McCrory, Dubin, & Leatherdale, 2015).
Among young Australian adults, AMED consumption ranged from 21.1% to 77% (Peacock et al., 2013; Pennay et al., 2014). In Europe, AMED consumption was reported by 3.4% of Slovakian adolescents (Holubcikova et al., 2016), 10.6% of Polish adolescent athletes (Nowak & Jasionowski, 2016), 20.6% of Dutch students (De Haan, de Haan, van der Palen, Olivier, & Verster, 2012), 39.0% of U.K. students (Johnson, Alford, Stewart, & Verster, 2016; Johnson, Alford, Verster, & Stewart, 2016), 44.4% of Italian students (Vitiello, Diolordi, Donini, & del Balzo, 2016), and 46.1% of Italian teenagers (Flotta et al., 2014). Among Brazilian students and teenagers, AMED consumption was reported by 12.9% to 31% (Bitancourt, Ribeiro Grilli Tissot, Marques Fidalgo, Fernandes Galdurόz, & da Silveira Filho, 2016; Eckschmidt, Guerra de Andrade, dos Santos, & Garcia de Oliviera, 2013; Locatelli, Sanchez, Opaleye, Carlini, & Noto, 2012), and 38% of Puerto Rican students reported AMED consumption (Cabezas‐Bou et al., 2016).
Various criteria were used to classify someone as an AMED consumer, ranging from “ever consumed AMED at least once during their life,” to past year consumption, or past month consumption. Otherwise, drinkers were simply classified as current AMED consumers. This may explain the broad range of percentages of AMED consumers reported across different studies. It should also be stressed that these samples typically comprise students and thus may not be representative of the general population. Also, as the majority of studies used convenience samples, it is unclear whether the observed percentages are representative of the wider student population they were drawn from. The broad range in percentages (ranging from 3.4% to 77%) reported in these studies should therefore be interpreted with caution and not used to illustrate AMED consumption in the general population.
Indeed, studies that have examined AMED consumption in random samples of adults not restricted to students have reported much lower rates of AMED consumption. For example, from a random sample of 2,000 Australians 18 years and older, 4.6% of participants reported past month AMED consumption (Pennay et al., 2015), and among a large random sample of the Taiwanese working population, only 6.0% of 13,501 men and 0.7% of 8,584 women reported consuming AMED (Cheng, Cheng, Huang, & Chen, 2012). Of a Canadian national representative sample of never‐smoking students (Grades 9–12), 13% reported consuming at least one AMED during the past year (Azagba & Sharaf, 2014).
3.2. Motives for AMED consumption
In our previous review, only three studies were included that described motives for AMED consumption. Malinauskas, Aeby, Overton, Carpenter‐Aeby, and Barber‐Heidal (2007) reported that about half of college students (54%) reported AMED consumption “during partying.” O'Brien, McCoy, Rhodes, Wagoner, and Wolfson (2008) surveyed U.S. students and reported percentages of AMED consumers drinking AMED “to hide the flavor of alcohol” (55%), “to drink more and not feel as drunk” (15%), to “not get a hangover” (7%), or “to drink more and not look as drunk” (5%). Marczinski (2011) surveyed 66 regular U.S. energy drink consumers on their motives for AMED consumption using a scale ranging from 1 (highly disagree) to 4 (highly agree). The most important motives for AMED consumption were “like the taste” (mean 3.02), “to celebrate” (3.00), “to socialize” (2.95), and “to get drunk” (2.82).
During the past 5 years, several studies have further addressed this topic. Peacock, Bruno, and Martin (2013) investigated motives for AMED consumption in 403 young Australian adults. Most frequently endorsed motives were “hedonistic motives” and “taste and sensation” related, including “because I like the taste of alcohol and energy drinks together” (69%) and “because I like the taste of energy drinks” (57%). Functional motives including “To feel more energetic” (70%) and “So I could stay out later” (54%) and situational motives such as “Because they are the ingredients in a drink (e.g., Jägerbomb)” (72%) were also frequently reported. To a lesser extent, intoxication‐ and impairment‐related motives were endorsed, including “to get more drunk” (32%), “so I could drink more” (20%), “to feel less drunk” (12%), “to look less drunk” (8%), and “to avoid getting a hangover” (6%). In a subsequent paper, Peacock, Droste, Pennay, Miller et al. (2015) examined motives for AMED consumption among a community sample of 731 Young Australian adults and 594 Australian university students. Participants were divided into four groups corresponding to their primary motives for AMED consumption: (a) taste (31%), (b) energy seeking (24%), (c) hedonistic (33%), and (d) intoxication‐related motives (12%). No significant differences were found between the groups regarding demographics or alcohol and drug use, alcohol consumption on AMED sessions, and AMED consumption‐related risk taking. Finally, Peacock et al. (2016) examined the motives for AMED consumption of 693 Australian ecstasy users. Participants reported consuming AMED to increase alertness (59%), for the taste (25%), to party for longer (23%), and to combat fatigue (16%).
Droste et al., 2014 examined motives for AMED consumption in 594 Australian students. Factor analysis identified four types of motives, which were categorized as being related to either “hedonic,” “social,” “energy/endurance,” and “intoxication reduction” factors. Among AMED consumers, having hedonic motives was associated with consuming significantly more alcohol, and having intoxication‐reduction motives was associated with experiencing significantly more alcohol‐related harm outcomes during the past 3 months. The authors did not infer whether these harmful events, including verbal, physical, and sexual aggression or experiencing alcohol‐related accidents or injury, were experienced on AMED or AO occasions.
Flotta et al. (2014) surveyed 870 Italian teenagers aged 15 to 19 years. Motives for AMED consumption that were rated as either highly important or important included “to celebrate/to party” (10.3% and 26.6%, respectively), “to socialize” (8.2% and 19.1%), and because they “like the taste” (6.1% and 14.9%). Motives that were rated “not at all important” included “to get work done” (53.5%), “because it's cheap” (48.7%), “to feel more comfortable with the opposite sex” (48.5%), and “because everyone else is doing it” (48.1%). Only 12.2% of the sample endorsed “to get drunk” as an important motive to consume AMED.
Bonar et al. (2015) interviewed 439 U.S. youths, aged 14–20 years, who were seeking emergency department care for any reason. Of these, 158 consumed AMED during the past year (36%). Primary motives included “to hide the flavor of alcohol” (39.2%), “like the taste” (35.8%), “stay awake” (32.3%), and “need more energy, in general” (28.5%). To a much lesser extent “drink more and not look as drunk” (2.5%) and “drink more and not feel as drunk” (7.6%) were endorsed.
Magnezi, Bergman, Grinvald‐Vogel, and Cohen (2015) conducted a survey among 802 Israeli youths, aged 14 to 18 years. The most commonly reported motive for AMED consumption was “to improve the taste of their alcoholic beverage” (80.6%). To a lesser extent, participants endorsed consuming AMED “to feel intoxicated” (24.6%), “out of curiosity” (14.6%), “to feel awake” (13.9%), “to consume more alcohol” (11.7%), “for social reasons” (10.4%), and “to reduce the side effects of alcohol” (8.4%).
In another Italian study, Vitiello et al. (2016) surveyed 1,007 students, of which 44.4% acknowledged consuming AMED. Motives for AMED consumption included “because I like it” (63.4%), “because I can maintain high activity levels throughout the night” (14.6%), “because I feel euphoric” (12.2%), “because I end up drinking less alcohol” (6.5%), and “because I can concentrate better” (3.3%).
On‐premise interviews with a small group (N = 10) of Australian bar patrons revealed that functional outcomes (e.g., maintaining wakefulness) were the most important motives for AMED consumption, followed to a lesser extent by social bonding, alcohol taste masking, and facilitating alcohol intoxication (Pennay & Lubman, 2012). Focus group discussions and interviews with 41 young Australian AMED consumers also identified social and functional motives as the most important reasons for AMED consumption (Pettigrew et al., 2016).
In the Netherlands, Verster, Benson, and Scholey (2014) conducted a survey among 6,002 university students, of whom, 1,239 reported consuming AMED. The most frequently reported motives for AMED consumption were “I like the taste” (81.1%), “I wanted to drink something else” (35.3%), and “to celebrate a special occasion” (14.6%). About one in five students (21.6%) also reported at least one negative motive to consume AMED, including “to get drunk” (8.0%), “it feels like it reduces the negative effects of alcohol” (6.9%), “it feels like I can drink more alcohol” (5.6%), “to prevent getting drunk” (3.8%), and “to sober up” (2.9%). Interestingly, in this study, the same motives were also rated for mixing alcohol with other nonalcoholic beverages (e.g., tonic or cola), and it appeared that these were quite similar to the motives for consuming AMED. When students rated motives for their other preferred nonalcoholic mixers, the most frequently reported motives were also “I like the taste” (90.2%), “I wanted to drink something else” (42.6%), and “to celebrate a special occasion” (14.9%). Negative motives included “it feels like it reduces the negative effects of alcohol” (5.1%) and “it feels like I can drink more alcohol” (6.5%), and students significantly more often endorsed the items “to get drunk” (10.9%), “to prevent getting drunk” (9.0%), and “to sober up” (6.0%), when compared to motives for mixing alcohol with energy drink. However, only a minority of students endorsed these negative motives.
Johnson, Alford, Verster, et al. (2016) replicated the study by Verster et al. (2014) in a sample of 1,873 U.K. students. The most frequently endorsed motives for AMED consumption were “I like the taste” (66.5%), “to celebrate a special occasion” (35.3%), and “I wanted to drink something else” (25.1%). In contrast to the Dutch sample where 8.0% reported consuming AMED “to get drunk,” an increased number (45.6%) of U.K. students reported this motive. Also, other negative motives such as “it feels like it reduces the negative effects of alcohol” (10.8%) and “it feels like I can drink more alcohol” (10.0%) were more frequently endorsed when compared to the Dutch student sample. Those who endorsed at least one negative motive (52.6% of the sample) were significantly more often male, younger, a smoker, had an earlier age of onset of regular alcohol consumption, and reported experiencing significantly more negative alcohol‐related consequences when compared to AMED consumers who endorsed only neutral motives.
When compared to other mixers such as tonic or cola, endorsement rates of neutral motives were quite comparable for mixing alcohol with energy drink. The items “to get drunk” and “it feels like it reduces the negative effects of alcohol” were significantly more often endorsed for AMED consumption, whereas the motive “it feels like I can drink more alcohol” was significantly more endorsed for mixing alcohol with other beverages (18.9%).
Cobb, Nasim, Jentink, and Blank (2015) surveyed 1,174 U.S. undergraduate students. Motives for consumption were recorded for (a) premixed AMED drinks, (b) self‐mixed AMED drinks, and (c) other nonalcoholic caffeinated beverages mixed with alcohol. The most frequently endorsed motives were “to hide the flavor of alcohol” (49.2%, 61.8%, and 81.4%, respectively), “I can drink less and get drunk” (45.9%, 17.6%, and 17.5%), “it is the only mixer available at parties” (18.4%, 17.6%, and 34.0%), and “I can stay alert while drinking” (26.5%, 35.3%, and 12.4%). Less frequently endorsed were “to drink more and not feel as drunk” (9.2%, 5.9%, and 8.2%) and “to drink more and not look as drunk” (4.9%, 0%, and 4.1%).
3.3. Characteristics of AMED consumers
A large number of studies have examined dispositional characteristics of AMED consumers. These studies either correlated AMED consumption with a variety of behaviors and personality characteristics (association studies) or directly compared AMED consumers with other drinkers that consume AO. Finally, some studies have examined whether different types of AMED consumers exist. The outcomes of these studies are summarized in the following sections.
3.3.1. Associations with AMED consumption
Many studies have examined behaviors and demographics that may be associated with the consumption of AMED. These studies are of a cross‐sectional nature, using correlations or regression models to determine whether certain variables are related to AMED consumption.
Significant associations have been reported between AMED consumption and binge drinking (Gonzales et al., 2015; Emond et al., 2014; Martz et al., 2015; Patrick et al., 2016; Pennay et al., 2015; Reid et al., 2015), drunkenness (Kristjansson, Mann, Sigfusdottir, & James, 2015), increased alcohol intake, higher blood alcohol concentrations (BACs; Arria, Caldeira, Bugbee, Vincent, & O'Grady, 2016; Azagba et al., 2013; Bonar, Green, & Asfrafioun, 2017; Brache & Stockwell, 2011; Cheng et al., 2012; O'Brien et al., 2008; Pennay et al., 2014; Woolsey, Waigandt, & Beck, 2010), hazardous drinking (Bonar et al., 2015; Eckschmidt et al., 2013), risk of alcohol use disorder (Emond et al., 2014), risk for alcohol dependence (Cheng et al., 2012; Droste et al., 2014; Snipes et al., 2015), and gambling (Pennay et al., 2015).
AMED consumers are significantly more likely to be male (Berger et al., 2011; Bonar et al., 2015; Cheng et al., 2012; Eckschmidt et al., 2013; Flotta et al., 2014; Housman et al., 2016; Martz et al., 2015; Pennay et al., 2015; Snipes et al., 2014; Wells et al., 2013); young (Azagba et al., 2013; Berger et al., 2011; Pennay et al., 2015; Rutledge et al., 2016; Wells et al., 2013); White (Berger et al., 2011), Black or Hispanic (Martz et al., 2015), and Black or other (Azagba et al., 2013; Reid et al., 2015); single (Eckschmidt et al., 2013); a fraternity or sorority member (Patrick et al., 2016); participate in athletics (Patrick et al., 2016) or team sports (Azagba et al., 2013); live off campus (Patrick et al., 2016); and have three or more evenings out per week (Martz et al., 2015). AMED consumption has also been associated with increased impulsivity (Snipes et al., 2015), lower anxiety sensitivity (Snipes et al., 2015), and moderate (but not low and high) psychological distress (Pennay et al., 2015).
In students, AMED consumption has been associated with having a lower grade point average (Martz et al., 2015); more often having a 1‐year class cut (Martz et al., 2015); absence from school (Azagba et al., 2013); students having more weekly spending money (Azagba et al., 2013; Reid et al., 2015); and endorsing greater fun/social, relaxation, and image motives for drinking (Patrick et al., 2016). In workers, AMED consumption was significantly more common in those with manually skilled occupations, with working hours <40 hr or longer than 49 hr per week, in occupations with lower job control, and (in a Taiwanese working population) being on piece‐rated or time‐based pay systems (Cheng et al., 2012).
AMED consumption was associated with higher susceptibility to smoking (Azagba et al., 2013, Bonar et al., 2017, Flotta et al., 2014, Khan, Cottler, & Striley, 2016), the use of electronic cigarettes (Milicic & Leatherdale, 2016), marijuana use (Azagba et al., 2013; Flotta et al., 2014; Khan et al., 2016; Martz et al., 2015; Snipes & Benotsch, 2013), cocaine use (Snipes & Benotsch, 2013), ecstasy use (Snipes & Benotsch, 2013), the use of other illicit drugs (Bonar et al., 2015; Bonar et al., 2017; Martz et al., 2015), and nonmedical use of prescription stimulants (Housman et al., 2016; Khan et al., 2016).
Significant associations were also found between AMED consumption and increased risk of casual sex (Miller, 2012), intoxicated sex (Miller, 2012; Snipes & Benotsch, 2013), unprotected sex (Berger et al., 2013; Snipes & Benotsch, 2013), sex under the influence of drugs (Bonar et al., 2015; Snipes & Benotsch, 2013), having an increased number of sexual partners (Flotta et al., 2014; Snipes & Benotsch, 2013), and sexual victimization in men, but not in women (Snipes et al., 2014). Also, significant associations were found between AMED consumption and being more likely to experience negative alcohol‐related consequences (Berger et al., 2013; Brache & Stockwell, 2011; De Haan et al., 2012; O'Brien et al., 2008), increased risk taking (Berger et al., 2013; Brache & Stockwell, 2011; Peacock, Droste, Pennay, Lubman et al., 2015; Woolsey et al., 2010), being involved in verbal and physical aggression (Miller, Quigley, Elisio‐Arras, & Ball, 2016), experiencing negative behavioral outcomes such as fighting (Holubcikova et al., 2016), and nonviolent alcohol‐related injury (Coomber et al., 2017).
AMED consumption has been associated with being involved in high‐risk traffic behaviors, such as driving after drinking (O'Brien et al., 2008; Peacock, Droste, Pennay, Lubman et al., 2015; Woolsey et al., 2010), speeding, not wearing a seatbelt, traveling with an intoxicated driver (Eckschmidt et al., 2013), riding with a driver that has used alcohol (Flotta et al., 2014), receiving driving tickets and warnings (Martz et al., 2015), and having traffic accidents (Martz et al., 2015). Finally, AMED consumption has been associated with recent (but not former) traumatic brain injuries among Canadian adolescents (Ilie et al., 2015), experiencing depressive symptoms (Bonar et al., 2017), and increased risk for suicidal behaviors among U.S. army personnel (Herberman Mash et al., 2014).
Other studies however, have not found significant associations between AMED consumption and problematic behaviors including binge drinking (Flotta et al., 2014), higher intoxication levels (Droste, Miller, Pennay, Zinkiewicz, & Lubman, 2016; Rossheim and Thombs, 2011), increased levels of sensation seeking (Snipes et al., 2015), being male (Malinauskas et al., 2007; Reid et al., 2015), younger age (Flotta et al., 2014), having a lower grade point average (Azagba et al., 2013; Patrick et al., 2016), school type (Martz et al., 2015), education level (Pennay et al., 2015), income (Pennay et al., 2015), general health (Pennay et al., 2015), sleep problems (Bonar et al., 2017), smoking (Pennay et al., 2015), and nonmedical use of opioids and anxiolytics (Khan et al., 2016). Further studies have also reported no significant associations between AMED consumption and drunk driving (Arria et al., 2016; Berger et al., 2013; Curtis et al., 2016; Flotta et al., 2014), wearing a seatbelt when riding in a car driven by someone else (Flotta et al., 2014), being hurt or injured (Berger et al., 2013), race or ethnic group (Patrick et al., 2016; Wells et al., 2013), sexual identity (Wells et al., 2013), participation in unprotected sex (Miller, 2012), unwanted sexual contact (Berger et al., 2013), and sexual victimization in women (Snipes et al., 2014).
3.3.2. Between‐group comparisons: AMED versus AO consumers
Woolsey, Williams, et al. (2015) compared alcohol consumption in 281 AO consumers with 268 AMED consumers. The authors found that the AMED group reported significantly more past month drinking days, consumed significantly more alcohol on both typical and heaviest past year drinking occasions, and consumed alcohol for longer times during these occasions. They further reported that AMED consumers were significantly more often involved in driving a car while having a BAC > 0.08%, driving after drinking too much to drive safely, and riding as a passenger with someone who had consumed too much alcohol to drive safely. Unfortunately, there was no assessment of whether these occasions were AMED or AO occasions. In a second study, Woolsey, Jacobson, et al. (2015) reported similar findings. AMED consumers were significantly more likely to drive a car while having a BAC > 0.08%, driving after knowing they were too drunk to drive safely, and being a passenger of someone who consumed too much alcohol to drive safely. Again, it was not reported whether these events occurred during AMED or AO consumption occasions. Only 13% of AMED consumers reported feeling more capable to drive on AMED occasions when compared to AO occasions. The fact that the vast majority of drivers do not report a difference in the capability to drive a car after AMED or AO is in line with Woolsey's findings that only a minority of AMED consumers report that after AMED they feel more confident (36%), feel they could drink more alcohol (45%), felt energy drinks reduced the negative effects of alcohol (25%), or felt that energy drinks sober them up quicker (20%). Of note, studies using within‐subject comparisons among AMED consumers show that driving while intoxicated is significantly less frequently reported for AMED occasions when compared to AO occasions (De Haan et al., 2012; Johnson, Alford, Stewart, et al. (2016).
Tucker, Troxel, Ewing, and D'Amico (2016) surveyed 696 U.S. high school students at the age of 14 and again at age 17. Only those that reported consuming alcohol were included in the sample. About 13% reported past month AMED consumption, and these students also reported consuming more alcohol (both frequency and quantity). AMED consumption was associated with having more negative consequences at high school, poorer grades, delinquent behavior, substance use‐related unsafe driving, drug use, and being intoxicated in public. No significant differences in mental health, social functioning, and academic aspirations were found among AMED‐consuming high school students compared to AO‐consuming high school students.
3.3.3. Are there different types of AMED consumers?
In an effort to examine whether all AMED consumers have similar characteristics, several studies have subdivided users into different categories.
Peacock and Bruno (2015) divided 403 young Australian AMED consumers into groups of low‐risk‐taking consumers (38%), disinhibited intake consumers (48%), and high‐risk‐taking consumers (14%). When comparing the three groups, the disinhibited intake and high‐risk‐taking AMED consumers exhibited higher trait impulsivity scores and were also more commonly male and had greater AMED and alcohol consumption. The authors concluded that AMED consumers are not a homogenous group. An alternative interpretation is that the authors arbitrarily divided AMED consumers into three groups according to their level of risk‐taking behavior. Without similar comparisons in other alcohol consumer groups, it is questionable whether this study informs understanding of the characteristics of AMED consumers, and therefore, further research is needed in this area.
Other research categorized AMED consumers according to their motives for AMED consumption.
Varvil‐Weld, Marzell, Turrisi, Mallett, and Cleveland (2013) divided 387 U.S. young AMED consumers into groups of “occasional AMED consumers” (53.7%), “anti‐AMED” (30.5%), “pro‐AMED” (5.2%), and “strong peer influence” (10.6%) drinkers. Whereas occasional drinkers had neutral motives with regard to AMED consumption, pro‐AMED consumers had positive attitudes and neutral expectancies but reported the most AMED use, AO consumption, and alcohol‐related consequences. Again, without comparison to similarly categorized (for example) AO users, it is unclear to what extent this subdivision adds to the understanding of characteristics of AMED consumers compared to AO consumers.
Mallett, Marzell, Scaglione, Hultgren, and Turrisi (2014) divided 195 AMED consumers into four groups of “moderate alcohol consumers with low AMED consumption” (55.9%), “moderate alcohol consumers with high AMED consumption” (10.8%), “heavy drinkers with low AMED consumption” (24.6%), or “heavy drinkers with high AMED consumption” (8.7%). They found that drinkers who consume more AMED have more positive beliefs, expectancies, and attitudes towards AMED consumption. They further observed that heavy drinkers experienced more alcohol‐related consequences when compared to moderate drinkers. Heavy drinkers were 3 times more likely to consume low levels of AMED than high levels of AMED. In subsequent analyses, Mallett, Scaglione, Reavy, and Turrisi (2015) divided student drinkers in (a) nonusers (60.4%), (b) those who initiated AMED consumption (12.4%), (c) those who discontinued AMED consumption (15.6%), and (d) continuous users of AMED (11.6%). Nonusers reported the lowest alcohol consumption and alcohol‐related consequences, whereas continuous users of AMED reported the highest rates. AMED consumers and those who initiate AMED consumption also engage in riskier drinking behaviors and experience higher rates of negative consequences.
3.4. Does AMED consumption increase alcohol consumption?
Table 1 summarizes the main characteristics of studies that investigated energy drink and alcohol consumption. Data were typically gathered by survey or interview. Two types of study design have been used—the chosen design has significant implications regarding study outcome, conclusions, and theoretical underpinnings. First, studies that used between‐group comparisons are discussed. In these studies, alcohol consumption of AMED consumers is compared to alcohol consumption of AO consumers. By definition, these studies show whether there is a group difference in alcohol consumption between AMED and AO consumers. If these groups differ fundamentally only on their AMED consumption status as an independent variable, then one can imply causality—that is, that AMED consumption is wholly or largely responsible for differences in any dependent variable (i.e., alcohol consumption). On the other hand, if the AMED and AO groups also differ on some other fundamental variables (e.g., gender, age, and personality traits), clearly any group differences may be attributable to this other factor. A second approach is to use a within‐subjects design, as AMED consumers do not mix alcohol with energy drink on every drinking occasion. This allows comparison of outcomes between AMED and AO occasions. The advantage of this design is that the same individuals are investigated on two occasions thus abolishing the potential, underlying group difference effects. In theory, the only main difference between the two drinking occasions would be the co‐consumption of energy drinks. On the other hand, given that even within AMED consumers the frequency where drinking episodes include AMED is significantly lower than AO occasions (e.g., De Haan et al., 2012; Johnson, Alford, Stewart, et al., 2016), it is possible that consequences associated with AMED consumption have less salience, skewing remembered instances towards AO occasions.
Table 1.
Overview of studies examining alcohol consumption of AMED and AO consumers
| Study | Year | Country | Design and recall period | Subjects | Between‐groups comparison | Within‐subjects comparison | Outcome |
|---|---|---|---|---|---|---|---|
| O'Brien et al. | 2008 | USA |
Web‐based survey Recall period: Past 30 days |
College students. AO: N = 2.189 AMED: N = 697 |
Typical number of alcoholic drinks on a single occasion. AO: 4.5 (7.0) AMED: 5.8 (4.5) p < .0011 Maximum number of alcoholic drinks on a single occasion. AO: 6.1 (7.0) AMED: 8.3 (5.0) p < .001 |
Not conducted |
BG: AMED > AO |
| Price et al. | 2010 | Canada |
Structured face‐to‐face interviews Recall period: Past week |
Past month ED‐consuming students AMED: N = 10 |
Not conducted |
Past week AMED and AO consumption on an average occasion. AO: 4.7 AMED: 8.6 p = .016 |
WS: AMED > AO |
| Woolsey et al. | 2010 | USA |
Web‐based survey Recall period: Past 12 months |
Student athletes AO: N = 165 AMED: N = 150 |
Typical number of alcoholic drinks on a single occasion. AO: 5.20 (3.91) AMED: 8.40 (5.22) p < .0001 Maximum number of alcoholic drinks on a single occasion. AO: 9.80 (5.84) AMED: 18.35 (10.74) p < .0001 |
N = 123 Typical number of alcoholic drinks on a single occasion. AO: 8.60 (5.14) AMED: 6.28 (4.41) Maximum number of alcoholic drinks on a single occasion (past 12 months) AO: 18.23 (10.56) AMED: 10.83 (7.94) |
BG: AMED > AO WS: AMED < AO |
| Brache and Stockwell | 2011 | Canada |
Web‐based survey Recall period: Past 30 days |
University students AO: N = 305 AMED: N = 105 |
Typical number of alcoholic drinks on a single occasion. AO: 3.04 (2.04) AMED: 5.34 (3.52) p < .001 Maximum number of alcoholic drinks on a single occasion. AO: 6.32 (3.93) AMED: 10.42 (5.31) p < .001 |
Typical number of alcoholic drinks on a single occasion. AO: 5.29 (5.91) AMED: 6.5 (3.56) p < .01 |
BG: AMED > AO WS: AMED > AO |
| Penning et al. | 2011 | The Netherlands |
Survey Recall period: Variable |
University students, 20.4 years old AO: N = 480 AMED: N = 24 |
Number of alcoholic drinks the day before latest alcohol hangover: AO: 10.9 (6.1) AMED: 8.5 (4.2) p = .056 |
Not conducted |
BG: AMED = AO |
| De Haan et al. | 2012 | The Netherlands |
Web‐based survey Recall period: 30 days |
University and college students, 18–30 years old AO: N = 3.185 AMED: N = 1.239 |
Typical number of alcoholic drinks on a single occasion. AO: 4.1 (3.1) AMED: 6.0 (3.9) p < .001 Maximum number of alcoholic drinks on a single occasion (past 30 days). AO: 7.7 (6.0) AMED:10.7 (6.7) p < .001 |
Typical number of alcoholic drinks on a single occasion (past 30 days). AO: 6.0 (3.9) AMED: 5.4 (3.7) p < .001 Maximum number of alcoholic drinks on a single occasion (past 30 days). AO: 10.7 (6.8) AMED:4.5 (5.7) p < .001 |
BG: AMED > AO WS: AMED < AO |
| Peacock et al. | 2012 | Australia |
Web‐based survey Recall period: Past 6 months for AMED occasions, past month for AO occasions. |
Convenience sample, 18–35 years old AMED: N = 387 |
Not conducted |
Typical number of alcoholic drinks on a single occasion. AO: 6.5 (4.8) AMED: 7.1 (5.6) p = .012 |
WS: AMED > AO |
| Lubman et al. | 2013 | Australia |
Web‐based survey (Study A) Recall period: Past 12 months |
Convenience sample, 16–70 years old (mean age 26.5 years) AO: N = 996 AMED: N = 731 |
Typical number of alcoholic drinks on a single occasion. AO: 3.65 (2.84) AMED: 6.67 (3.93) p < .001 |
N = 698 Typical number of alcoholic drinks on a single occasion. AO: 6.7 (4.0) AMED: 6.0 (4.2) p < .001 Maximum number of alcoholic drinks on a single occasion. AO: 14.7 (8.3) AMED: 8.3 (6.7) p < .001 |
BG: AMED > AO WS: AMED < AO |
| Lubman et al. | 2013 | Australia |
On‐premise interviews (Study B) Recall period: Past 12 months and number of drinks consumed on premise on the interview day |
Bar patrons, 16–55 years old (mean age 22.71 years). Past 12 months: AO: 718 AMED: 474 On premise: AO: N = 887 AMED: N = 128 |
Typical number of alcoholic drinks on a single occasion. AO: 7.42 (5.50) AMED:9.54 (5.62) p < .001 Number of alcoholic drinks consumed on premise: AO: 4.76 (5.46) AMED: 5.65 (5.60) p < .01 |
N = 358 Typical number of alcoholic drinks on a single occasion. AO: 9.7 (5.8) AMED: 8.4 (5.9) p < .001 |
BG: AMED > AO WS: AMED < AO |
| Eckschmidt et al. | 2013 | Brazil |
Survey Recall period: Past 12 months and number of drinks consumed on premise on the interview day |
College students AO: N = 4.192 AMED: N = 1.119 |
Typical number of alcoholic drinks on a single occasion. AO: 3.3 (13.2) AMED: 6.1 (13.7) p < .001 |
Not conducted |
BG: AMED > AO |
| Lubman et al. | 2014 | Australia |
On‐premise interview Recall period: Number of drinks consumed on premise on the interview day |
Secondary school completers, 17–18 years old AO: N = 471 AMED: N = 87 |
Number of alcoholic drinks on the night of interview. AO: 8.30 AMED: 11.34 p < .001 |
Not conducted |
BG: AMED > AO |
| Trapp et al. | 2014 | Australia |
Survey Recall period: Not reported |
Western Australian Pregnancy Cohort, 20 years old AO: N = 644 AMED: N = 590 |
Total alcohol intake per day (g/day) AO: 12.1 (15.7) g AMED: 20.3 (19.7) g p < .001 |
Not conducted |
BG: AMED > AO |
| Woolsey, Jacobson, et al. (2015) | 2015 | USA |
Web‐based survey Recall period: Past 30 days, up to 12 months |
University students. AO: N = 174 AMED: N = 107 |
Typical number of alcoholic drinks on a single occasion. AO: 3.35 (2.30) AMED: 5.42 (3.46) p < .0001 Maximum number of alcoholic drinks on a single occasion (past 30 days). AO: 4.62 (3.79) AMED: 8.03 (5.84) p < .001 |
Not conducted |
BG: AMED > AO |
| Woolsey, Williams, et al. (2015) | 2015 | USA |
Web‐based survey Recall period: Past 30 days, up to 12 months |
University students AO: N = 281 AMED: N = 268 |
Typical number of alcoholic drinks on a single occasion. AO (N = 274): 3.76 (2.58) AMED (N = 266): 5.52 (3.29) p < .001 Maximum number of alcoholic drinks on a single occasion (past month). AO (N = 280): 5.14 (3.95) AMED (N = 267): 9.26 (6.14) p < .001 |
Not conducted |
BG: AMED > AO |
| Verster et al. | 2015 | The Netherlands |
On‐premise interview Recall period: Number of drinks consumed on the interview day (at home and on premise) |
Bar patrons, 18–30 years old AO: N = 482 AMED1: N = 185 (consumed AMED that day) AMED2: N = 246 (no AMED consumed that day) |
Number of alcoholic drinks consumed on the day of the interview. AO: 8.8 (5.4) AMED1: 9.4 (6.3) AMED2: 10.1 (6.8) p < .05 |
AMED1: AO: 9.4 (5.9) AMED: 10.1 (6.8) p = .148 AMED2: AO: 9.4 (6.3) AMED: 9.8 (6.0) p = .360 |
BG: AMED > AO WS: AMED = AO |
| Johnson, Alford, Stewart, et al. (2016) | 2016 | UK |
Web‐based survey Recall period: Past 30 days, up to 12 months |
University and college students, 18–30 years old AO: N = 865 AMED: N = 732 |
Typical number of alcoholic drinks on a single occasion. AO: 6.4 (4.1) AMED: 8.9 (6.0) p < .05 Maximum number of alcoholic drinks on a single occasion (past 30 days). AO: 9.4 (6.4) AMED: 12.8 (8.5) p < .05 |
Typical number of alcoholic drinks on a single occasion (past 30 days). AO: 9.0 (6.1) AMED: 6.0 (4.9) p < .001 Maximum number of alcoholic drinks on a single occasion (past 30 days). AO: 12.9 (8.6) AMED: 7.0 (7.9) p < .001 |
BG: AMED > AO WS: AMED < AO |
Note. If available, mean (SD) number of alcoholic drinks are reported and corresponding p‐values. ED = energy drink; AMED = alcohol mixed with energy drink; AO = alcohol only, WS = within‐subject comparison; BG = between‐group comparison.
For the meta‐analyses, studies were included only if they provided sufficient data regarding the typical number of alcoholic drinks on a single drinking occasion. Therefore, not all studies could be included.
For example, Penning, de Haan, and Verster (2011) examined alcohol consumption on a heavy drinking occasion that resulted in a hangover. This drinking occasion cannot be considered to be representative for a typical (average) drinking episode, nor is it sure this was their past month heaviest drinking occasion. Therefore, it was excluded from the meta‐analysis. Also, the on‐premise studies by Lubman, Droste, Pennay, Hyder, and Miller (2014) and Verster, Benjaminsen, van Lanen, van Stavel, and Olivier (2015) were excluded from the analyses as it is not known whether the on‐premise night represents a typical drinking episode.
The other 11 studies were included in the meta‐analyses.
3.4.1. Between‐group comparisons: AMED versus AO consumers
Combined, the 11 studies provided data on alcohol consumption on typical single drinking occasions of 6,061 AMED consumers and 14,496 AO consumers (Brache & Stockwell, 2011; De Haan et al., 2012; Eckschmidt et al., 2013; Johnson, Alford, Stewart, et al., 2016; Johnson, Alford, Verster, et al., 2016; Lubman et al., 2013a; Lubman et al., 2013b; O'Brien et al., 2008; Trapp et al., 2014; Woolsey et al., 2010; Woolsey, Jacobson, et al., 2015; Woolsey, Williams, et al., 2015).
The results of the meta‐analysis on between‐group comparisons confirmed that AMED consumers drink significantly more alcohol than AO consumers on a typical drinking occasion (p = .0001, ES = 0.535, 95% CI [0.378, 0.692]; see Figure 1).
Figure 1.
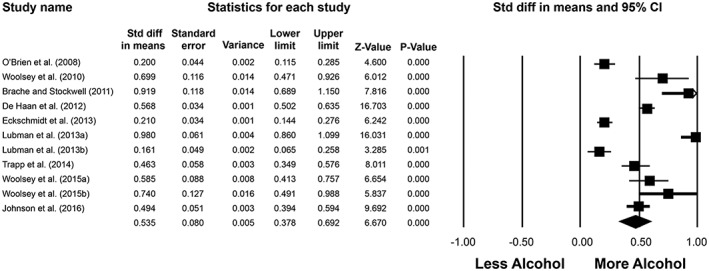
Alcohol consumption during typical drinking occasions in AMED and AO consumers. Between‐group comparisons revealed that on a typical drinking occasion, AMED users consumed significantly more alcohol compared to AO occasions. Tests for heterogeneity: Q = 230.9, p = .0001. A random effects model was applied. Z = 6.670, p = .0001. AMED = alcohol mixed with energy drink; AO = alcohol only; CI = confidence interval
Seven studies also examined the maximum number of alcoholic drinks consumed on a single occasion during the past month (Brache & Stockwell, 2011; De Haan et al., 2012; Johnson, Alford, Stewart, et al., 2016; O'Brien et al., 2008; Woolsey et al., 2010; Woolsey, Jacobson, et al., 2015; Woolsey, Williams, et al., 2015). The meta‐analysis combined data from between‐group comparisons of 3,301 AMED consumers and 7,167 AO consumers. AMED consumers reported a significantly higher maximum number of alcoholic drinks consumed on a single past month occasion when compared to AO consumers (p = .0001, ES = 0.651, 95% CI [0.496, 0.807]; see Figure 2).
Figure 2.
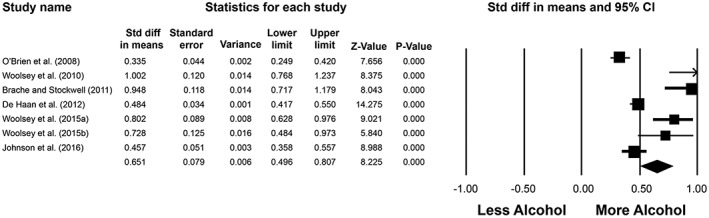
Alcohol consumption during the past month's heaviest drinking occasion among AMED and AO consumers. Between‐group comparisons revealed that on the past month's heaviest drinking occasion, AMED users consumed significantly more alcohol when compared to AO occasions. Tests for heterogeneity: Q = 62.2, p = .0001. A random effects model was applied. Z = 8.225, p = .0001. AMED = alcohol mixed with energy drink; AO = alcohol only; CI = confidence interval
3.4.2. Within‐subject comparisons: AMED versus AO occasions
Eight studies used a within‐subject design to compare alcohol consumption on a typical AMED and a typical AO occasion (Brache & Stockwell, 2011; De Haan et al., 2012; Johnson, Alford, Stewart, et al., 2016; Lubman et al., 2013; Peacock, Bruno, & Martin, 2012; Price, Hilchey, Darredeau, Fulton, & Barrett, 2016 Verster et al., 2014; Woolsey et al., 2010). Alcohol intake of 3,480 AMED consumers was compared for both occasions. Figure 3 summarizes the results of the meta‐analysis. Alcohol consumption of AMED consumers does not significantly differ on typical AMED occasions when compared to typical AO occasions (p = .170, ES = −0.095, 95% CI [−0.230, 0.041]). Four studies collected data on the maximum number of alcoholic drinks consumed on a single episode during the past month (De Haan et al., 2012; Johnson, Alford, Stewart, et al., 2016; Lubman et al., 2013; Woolsey et al., 2010). Data from 2,743 AMED consumers were combined into the meta‐analysis. The analysis revealed that for the maximum number of alcoholic drinks consumed on a single occasion during the past month, the total alcohol consumption on AMED occasions was significantly lower than on AO occasions (p = .015, ES = −0.577, 95% CI [−1.039, −0.114]; see Figure 4).
Figure 3.
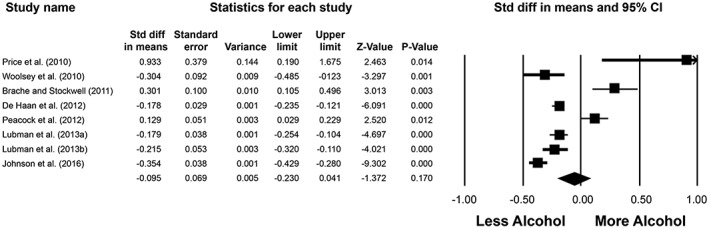
Alcohol consumption during a typical AMED and AO occasion. Within‐subject comparisons revealed that alcohol consumption of AMED consumers does not significantly differ on a typical AMED occasion when compared to a typical AO occasion. Tests for heterogeneity: Q = 91.3, p = .0001. A random effects model was applied. Z = −1.372, p = .170. AMED = alcohol mixed with energy drink; AO = alcohol only; CI = confidence interval
Figure 4.
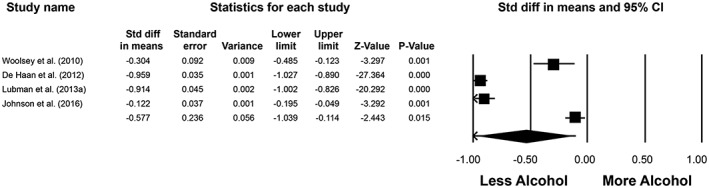
Alcohol consumption during the past month's heaviest drinking AMED and AO occasion. Within‐subject comparisons revealed that AMED consumers used significantly less alcohol on their past month heaviest drinking AMED occasion when compared to their past month heaviest drinking AO occasion. Tests for heterogeneity: Q = 327.7, p = .0001. A random effects model was applied. Z = −2.443, p = .015. AMED = alcohol mixed with energy drink; AO = alcohol only; CI = confidence interval
3.4.3. Prospective studies
Marzell et al., 2014 conducted a survey in 386 U.S. students followed up 1 year thereafter. AMED consumers reported significantly higher amounts of alcohol consumption and associated negative sexual, academic, and physical consequences when compared to AO consumers. AMED consumers had more positive attitudes towards AMED consumption when compared to AO consumers. AMED consumption in the first survey predicted the behaviors observed in the follow‐up survey.
Patrick, Evans‐Polce, & Maggs, 2014 conducted a prospective study to examine whether AMED consumption predicted alcohol‐related consequences 2 years later. They found that AMED consumption was associated with significantly increased AUDIT scores, greater alcohol intake, and corresponding negative consequences. In a second paper, 508 AMED consumers were followed for 56 days (Patrick & Maggs, 2014). Within‐subjects, occasions of AMED consumption were compared to AO occasions. The analyses revealed that on AMED occasions significantly more alcohol was consumed. Interpretation is difficult as no data were presented regarding estimated or measured amounts of alcohol consumed on AMED and AO occasions, nor on the relative frequency of both types of drinking occasions. After controlling for estimated BAC, no significant differences in subjective intoxication were found.
3.5. Comparisons of energy drink with other mixers
To examine whether energy drinks have unique properties relative to other nonalcoholic mixers such as cola and tonic, direct comparisons were made in two studies.
In the Netherlands, Verster et al. (2014) compared alcohol consumption of 1,239 AMED consumers on occasions when they consumed AMED with occasions when they mixed alcohol with other nonalcoholic beverages (AMOB). Overall, the motives for consuming AMED and AMOB were similar. Although significantly more often subjects endorsed negative motives for AMOB compared to AMED, negative motives were endorsed only by a small number of subjects. Therefore, the relevance of these differences can be questioned. Alcohol consumption on a typical AMED occasion (5.4 alcoholic drinks) was significantly higher than alcohol on a typical AMOB occasion (5.1 alcoholic drinks), representing a difference of 0.3 drinks per occasion. Regarding the past month greatest number of drinks on a single drinking occasion, significantly less alcohol was consumed on the AMED occasion (4.5 alcoholic drinks) when compared to the AMOB occasion (5.4 alcoholic drinks).
This study also attempted to differentiate between neutral and negative motives. Within‐subject analyses were conducted to compare alcohol consumption (quantity and frequency) on AMED occasions and AO occasions. Alcohol consumption of AMED consumers with neutral motives was compared to alcohol consumption of those who reported at least one negative motive (the latter comprising 21% of the sample [n = 257]). Irrespective of their motives, both groups reported consuming significantly less alcohol on occasions when they consumed AMED compared to AO occasions and to occasions when consuming alcohol mixed with other nonalcoholic beverages.
Johnson, Alford, Stewart, et al. (2016) performed a partial replication of the Dutch study in 732 U.K. AMED consumers. Significantly more subjects reported consuming AMED “to celebrate a special occasion” and “to get drunk” because they “received the drink from someone else” or “because others drink it as well”. However, significantly fewer subjects reported consuming AMED compared to AMOB because “It feels like I can drink more alcohol.” Alcohol consumption was significantly lower on typical AMED occasions (6.1 alcoholic drinks) compared to typical AMOB occasions (6.7 alcoholic drinks). Regarding the past month greatest number of drinks on a single drinking occasion, significantly less alcohol was consumed on the AMED occasion (7.1 alcoholic drinks) when compared to the AMOB occasion (8.3 alcoholic drinks).
In both the U.K. and Dutch studies, irrespective of the type of mixer, on both AMED and AMOB occasions, total alcohol consumption was significantly less when compared to AO occasions of the same subjects.
Taken together, results from these two large studies suggest that most alcohol is consumed on AO occasions. Significantly less alcohol is consumed on mixing occasions. However, the type of nonalcoholic mixer has little influence on the total amount of alcohol that is consumed.
Cobb et al. (2015) also reported data from a between‐group comparison regarding alcohol consumption of those who (a) consume premixed AMED drinks, (b) consume self‐mixed AMED drinks, and (c) mix other nonalcoholic caffeinated beverages with alcohol. The analyses revealed that those who consume premixed AMED drinks consumed significantly more standard drinks but were engaged in mixing caffeine and alcohol for significantly fewer months than the other two groups. No significant differences we observed with regard to the average number of past month drinking days of alcohol mixed with caffeine, hours spent drinking alcohol on a typical night mixing alcohol with caffeine, average number of days of alcohol consumption per month (without caffeine), or the average alcohol quantity consumed. Unfortunately no AO group was included. Also of note, in the United States premixed AMED drinks are no longer marketed.
3.6. The desire to drink more alcohol
Four studies have examined the desire to drink more alcohol after consuming AMED or AO.
Marczinski, Fillmore, Henges, Ramsey, and Young (2013) reported that consumption of AMED increased the motivation to consume more alcohol when compared to AO consumption. However, the observed difference between AMED and AO group was not statistically significant (p = .075). Similarly, no significant differences were observed in ratings of sedation.
McKetin and Coen (2014) compared a group who consumed AMED with a group who consumed AO. They administered to each subject 60 ml of vodka, mixed with either Red Bull Silver Edition (AMED group, N = 36) or soda (AO group, N = 39). As body weight and gender were not taken into account, the AO group had a significantly higher breath alcohol concentration (BrAC) when compared to the AMED group (0.030% vs. 0.025%, p = .042). No significant differences between the groups were found for ratings of stimulation, sedation, feeling the effects of the cocktail, or feeling high. The group that received Red Bull as the mixer reported significantly higher scores of wanting more of the cocktail than those who received soda as mixer (a difference of 17 mm on the 100‐mm scale, p = .006).
Marczinski, Fillmore, Stamates, and Maloney (2016) conducted a six‐way crossover study in 26 healthy young subjects examining the desire to drink more alcohol after administering alcohol (1.21 ml/kg vodka) or placebo, mixed with different dosages of energy drink (3.63 or 6.05 ml/kg, i.e., one or two 80‐ml cans of Red Bull for a 70‐kg person) or placebo, alone or in combination. Twenty minutes after drinking, the desire to drink more alcohol after receiving a low or high AMED dose was significantly higher when compared to the AO condition (p = .032). A transitory statistically significant increase from a score of 23.8 (AO) to 34.5 (AMED) on a 100‐point desire scale was observed 20 min after consumption, but the effect was not significant 10, 40, 60, and 80 min after beverage consumption.
Marczinski, Fillmore, Maloney, and Stamates (2017) examined the rate of drinking AMED versus AO. In a crossover design, 16 subjects consumed (a) 1.97 ml/kg vodka and 5.91 ml/kg decaffeinated soft drink, (b) 1.97 ml/kg vodka and 5.91 ml/kg energy drink, (c) 5.91 ml/kg decaffeinated soft drink, or (d) 5.91 ml/kg energy drink. The drinks were divided into 10 cups, and subjects were told that they had 2 hr to consume the beverages. The mean BrAC achieved after 2 hr was 0.066%. No significant differences were observed on ratings of stimulation or sedation, nor between the AMED and AO condition on a cued go/no‐go task. The AMED beverage was consumed significantly faster (i.e., 16 min) than the AO beverage.
It should be taken into account that the urge or desire to drink does not automatically imply that this results in greater alcohol intake. For example, in a recent study, participants could choose their preferred beverage of choice, and the subsequent number of self‐administered drinks were recorded (Sweeney, Meredith, Evatt, & Griffiths, 2017). The alcoholic drinks each contained 14 g alcohol, with added caffeine (60 mg) or placebo. Quinine was added to mask the bitter taste of caffeine. Sixty‐five percent of participants choose to consume the caffeinated alcoholic beverage above the AO beverage. However, no significant difference was observed in the number of self‐administered drinks.
3.7. Does mixing alcohol with energy drink change the drinker's perception of intoxication?
It has been hypothesized that the stimulant effects of caffeine may counteract the depressant effects of alcohol. In other words, that co‐consumption of energy drinks may mask the intoxication effects of alcohol. The masking effect implies that drinkers would feel less intoxicated than they actually are when they consume AMED. The presence of a masking effect could have serious consequences, for example, when considering driving. People who are objectively intoxicated could perceive themselves as being less intoxicated or even sober and thus would be more willing to drive a car. This example illustrates the importance of research to determine whether such a masking effect actually exists after coconsumption of energy drinks and alcohol.
The most frequently cited study to support the existence of a masking was conducted by Ferreira, de Mello, Pompéia, and de Souza‐Formigoni (2006). However, the study by Ferreira et al. did not directly assess subjective intoxication. Instead, it assessed 18 symptoms of alcohol consumption and reported significant differences on subjective assessments of four of these symptoms. It can be questioned to what extent these four symptoms (i.e., higher scores of headache, weakness, salivation, and reduced motor coordination) are related to subjective intoxication and masking. Of note, Ferreira's findings were not confirmed in a recent replication study with twice the number of subjects (Ulbrich et al., 2013). In this study, Ulbrich et al. (2013) found no significant difference on any of the 18 symptoms that were examined by Ferreira et al. (2006). Similarly, Alford, Hamilton‐Morris, and Verster (2012) could not find significant differences in subjective effects to support the findings of Ferreira et al.
In 2014, Benson, Verster, Alford, and Scholey (2014) conducted a literature review and meta‐analysis on the effects of consuming alcohol mixed with caffeinated beverages on subjective intoxication. Sixteen articles were summarized, and nine were included in the meta‐analysis. In addition to studies that combined alcohol with energy drink, also clinical trials examining the effects of alcohol with caffeine (e.g., powder) or other nonalcoholic caffeinated beverages were included (e.g., colas or caffeinated beer). One study included two doses of caffeine in a within‐subjects design (Marczinski and Fillmore, 2006). The meta‐analyses by Benson et al. (2014) revealed that no significant masking effect was found with the higher or lower caffeine level (p = .404 and .406, respectively). The authors concluded that
Despite the large range of caffeine doses (2.0–5.5 mg/kg resulting in absolute levels of 46–383 mg) and alcohol levels 0.29–1.068 g/kg (resulting in blood alcohol concentration (BAC) from 0.032 to 0.12%) investigated, caffeine had no effect on the judgement of subjective intoxication.
This conclusion was adopted in 2015 by the European Food Safety Authority (2015) who referred to this review in their assessment on the safety of caffeine and concluded that “Single doses of caffeine up to 200 mg, corresponding to about 3 mg/kg bw for a 70‐kg adult are unlikely to […] mask the subjective perception of alcohol intoxication.”
3.7.1. Masking studies: AMED versus AO
Data on the masking effect examined when combining alcohol with actual energy drinks (rather than with caffeine or cola‐type drinks) come from six experimental studies directly comparing subjective intoxication after consuming AMED with AO (Benson & Scholey, 2014; Marczinski, Fillmore, Bardgett, & Howard, 2011; Marczinski, Fillmore, Henges, Ramsey, & Young, 2012; Marczinski et al., 2013; Peacock, Bruno, Martin, & Carr, 2013; Van de Loo et al., 2016). In addition, an on‐premise study was conducted in the Netherlands assessing subjective intoxication in a natural setting, including higher consumption levels of alcohol when compared to laboratory settings. These studies are summarized in Table 2.
Table 2.
Summary of studies examining subjective intoxication after administering AMED or AO
| Study | Peak BrAC (%) | Caffeine (mg/kg) | Design | Alcohol alone | Alcohol + energy drink | Primary aim of study | Scale | Alcohol drink | Alcohol caffeine drink | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Rating | N | Rating | ||||||||
| Marczinski et al. (2011) | 0.08 | 1.2 | B | 14 | 3.61 (1.62) | 14 | 3.32 (1.6) | Effects of energy drink on alcohol impairment of behavioral control | BRS (0–10) | Squirt soda + alcohol | Red Bull + alcohol |
| Marczinski et al. (2012) | 0.064 | 1.2 | B | 18 | 3.53 (1.59) | 18 | 3.28 (1.36) | Energy drink/alcohol on information processing, motor coordination, subjective intoxication | BRS (0–10) | Squirt soda + alcohol | Red Bull + alcohol |
| Marczinski et al. (2013) | 0.032 | 0.6 | B | 20 | 2.95 (1.59) | 20 | 2.2 (1.01) | Energy drink/alcohol effects on motivation for more alcohol | BRS (0–10) | Squirt soda + alcohol | Red Bull + alcohol |
| Peacock, Bruno, Martin, & Carr, 2013 | 0.068 | 3.57 | W | 28 | 2.8 (1.0) | 28 | 2.9 (1.2) | Energy drink/alcohol effects on risk taking | BRS(0–10) | Red Bull vehicle + alcohol | Red Bull + alcohol |
| Benson and Scholey (2014) | 0.051 | 1.12 | W | 24 | 5.0 (0.44) | 24 | 5.8 (0.40) | Energy drink/alcohol effects on mood and intoxication | Sober–drunk VAS (0–10) | Red Bull vehicle + alcohol | Red Bull + alcohol |
| Van de Loo et al. (2016) | 0.075 | 80 mg | W | 46 | 4.81 (1.96) | 46 | 4.46 (1.60) | Energy drink/alcohol effects on subjective intoxication | Sober–highly intoxicated VAS (0–10) | Red Bull vehicle + alcohol | Red Bull + alcohol |
Note. In case there was more than one AO or AMED comparison, the peak alcohol comparison was used. Van de Loo et al. (2016) administered one 250‐ml can of Red Bull to each participant, containing 80 mg of caffeine. BrAC = blood alcohol concentration; AMED = alcohol mixed with energy drink; AO = alcohol only; W = within subjects; B = between groups; BRS = Beverage Rating Scale; VAS = visual analogue scale; N = number of subjects.
In the six experimental studies, alcohol was consumed to achieve a peak BrAC ranging from 0.03% to 0.08% (i.e., the equivalent of one to four alcoholic drinks). Coadministered caffeine levels that varied from 0.6 to 3.57 mg/kg bodyweight (i.e., the equivalent of 0.5 to three 250‐ml cans of an 80‐mg‐caffeine energy drink). Subjective intoxication was assessed using the Beverage Rating Scale (Marczinski et al., 2011, 2012, 2013; Peacock et al., 2013) or visual analogue scales ranging from sober to drunk/highly intoxicated (Benson & Scholey, 2014; Van de Loo et al., 2016). On the Beverage Rating Scale, drinkers rate their perceived intoxication in terms of equivalence to that felt after consuming bottles of beer containing 5% alcohol. The scale ranges from 0 to 10 bottles of beer, in 0.5‐bottle increments.
Marczinski et al. (2011, 2012, 2013) conducted three studies in healthy volunteers that examined the effect of AMED consumption on subjective intoxication. In the first study, subjective intoxication was assessed after administering 0.65 g/kg alcohol to achieve a peak BAC of approximately 0.08%, with or without 3.57 ml/kg energy drink (equivalent to 1.14 mg/kg caffeine, that is, a 250‐ml can containing 80 mg caffeine for a 70‐kg person). No significant difference in subjective intoxication was found between the group that consumed AMED and the group that consumed AO (Marczinski et al., 2011). In the second study, Maczinski et al. (2012) administered less alcohol (to achieve a peak BAC of approximately 0.065%) while administering the same amount of energy drink as in the first study. Again, no significant difference in subjective intoxication was found between AMED and AO consumers. In the third study, Marczinski et al. (2013) administered 0.29 g/kg alcohol to reach a peak BAC of approximately 0.03%. In this study, 1.82 ml/kg energy drink (0.6 mg/kg caffeine) was administered (equivalent to half a 250‐ml can containing 80 mg caffeine for a 70‐kg person). Also, in this study, no significant difference in subjective intoxication was observed between the group that consumed AMED and the AO group.
In N = 28 healthy subjects, and Peacock, Bruno, Martin, and Carr (2013) examined subjective intoxication after administering alcohol (0.5 g/kg), AMED (3.57 ml/kg), or a placebo drink. Subjective intoxication was assessed with the Beverage Rating Scale and a 100‐mm visual analogue scale (the subjective effects scale). Both scales showed that alcohol alone significantly increased subjective intoxication ratings. Coadministering energy drink did not significantly alter these ratings. Similarly, the observed physiological and psychological side effects in this study must be attributed to the independent effects of alcohol or energy drink alone; interactions between the two were generally absent (Peacock, Bruno, Martin, & Carr, 2014).
In a crossover design in N = 24 healthy subjects, Benson and Scholey (2014) examined subjective intoxication after administering alcohol (0.6 g/kg), alcohol mixed with 250 ml Red Bull energy drink (80 mg caffeine), or a placebo drink (matched except for functional ingredients). Subjective intoxication was assessed with a 100‐mm visual analogue scale ranging from sober to drunk. Consumption of alcohol alone and AMED both significantly increased subjective intoxication ratings. No significant differences were observed in subjective intoxication ratings between the alcohol alone and AMED condition.
Van de Loo et al. (2016) examined the effects of energy drink (250 ml Red Bull, 80 mg caffeine) versus placebo energy drink mixed with alcohol to achieve a BrAC of 0.08%, 0.05%, 0.02%, and 0%. Subjective intoxication was assessed on a scale ranging from 0 (sober) to 10 (highly intoxicated). Fifty‐six healthy social drinkers participated in this double‐blind study. No significant difference in subjective intoxication was observed at BAC 0.08% and 0.05%. At BAC 0.02%, a significant difference was found between energy drink and the placebo drink (0.93 vs. 0.61, respectively, on a range from 0 to 10), with the low scores indicating that at that point subjects were relatively unintoxicated. A significant increase in sleepiness scores was observed in the AO condition, whereas in the alcohol and energy drink condition, sleepiness scores remained stable. Taken together, this study confirmed that also at higher BAC levels no evidence of a masking effect was present.
The meta‐analysis of six studies that examined subjective intoxication on AMED and AO occasions revealed no significant masking effect (p = .747, ES = −0.021, 95% CI [−0.310, 0.268]; see Figure 5).
Figure 5.
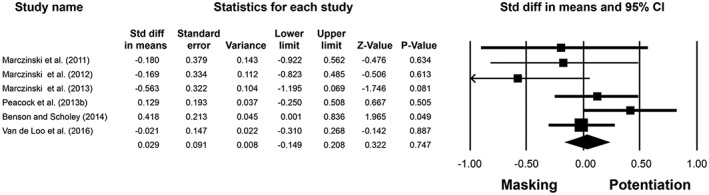
Subjective intoxication following the consumption of AMED or AO. The analysis revealed no significant differences in subjective intoxication after consuming AMED or AO. Tests for heterogeneity: Q = 7.76, p = .170. A fixed effects model was applied. Z = 0.322, p = .747. AMED = alcohol mixed with energy drink; AO = alcohol only; CI = confidence interval
3.7.2. Higher dosages on premise
In the Netherlands, Verster et al. (2015) assessed subjective intoxication on‐premise in 997 people leaving the bar after an evening of alcohol consumption. Breath alcohol tests were conducted followed by a short interview. One hundred eighty‐five subjects consumed alcohol and energy drink on the night of the interview. Both objective intoxication (BrAC 0.074%) and subjective intoxication did not significantly differ between those who consumed AO and those who consumed AMED. Regression analyses revealed that gender, time of the interview, and BrAC were significant predictors of subjective intoxication and together explained 37.7% of variance. Whether subjects coconsumed energy drink or not was unrelated to subjective intoxication levels. This study showed that also under real‐life circumstances, including achieving higher BrACs when compared to the six controlled laboratory experiments, no evidence was found for the existence of a so‐called masking effect.
3.8. Does AMED consumption affect risk‐taking behavior?
A number of studies showed that AMED consumers experience significantly more risk‐taking behaviors when compared to AO consumers (see section on characteristics of AMED consumers for an overview). As stated earlier, these associations do not necessarily reflect a causal relationship with AMED consumption, as energy drinks may simply appeal more to people with higher levels of risk‐taking behavior than does AO consumption. To examine whether there is a direct relationship between AMED consumption and risk taking, studies applying a within‐subject design are needed. Up to now, four studies have used such a design.
Peacock et al. (2012) interviewed 403 Australian AMED consumers. Relative to AO occasions, on AMED occasions the rates of engagement in 26 different alcohol‐related risk‐taking behaviors were significantly lower. In a subsequent placebo controlled double‐blind clinical trial in 28 healthy subjects, no significant difference in risk‐taking behavior was observed on the Balloon Analogue Risk Task after administering alcohol (0.5 g/kg body weight) and energy drink (3.57 ml/kg body weight Red Bull) or alcohol mixed with placebo energy drink.
Similar findings of reduced chances of engaging in risk‐taking behavior on AMED occasions compared to AO occasions were found among 1,239 Dutch AMED consumers (De Haan et al., 2012) and 732 AMED consumers from the United Kingdom (Johnson, Alford, Verster, et al., 2016).
It has been argued that risk‐taking behavior may be less commonly experienced or remembered on AMED occasions simply because AMED occasions occur significantly less frequently than AO occasions. Therefore, Peacock, Droste, Pennay, Lubman et al., 2015 examined a sample of 273 Australian and New Zealand AMED consumers with matched frequencies of AMED and AO occasions. Again, significantly lower odds of 18 out of 25 risk‐taking behaviors were found for AMED occasions. No significant difference was found for the other seven risk‐taking behaviors that were assessed.
4. DISCUSSION
This review of the literature shows that, compared with alcohol alone, mixing alcohol with energy drink has little significant effect on total alcohol consumption, subjective intoxication, and alcohol‐associated risk‐taking behavior or other negative consequences. Alcohol itself seems to be the cause of many negative consequences of high alcohol intake per se. The literature is overwhelmingly consistent with the notion that AMED consumption is just one manifestation of an underlying trait for greater alcohol consumption along with a cluster of other risky behaviors.
4.1. Prevalence of AMED consumption
In our previous review (Verster et al., 2012), we noted that studies reported percentages of AMED consumption ranging from 6% to 44%. These figures have not significantly changed over the past 5 years. Sample size, and the extent of targeted recruitment, and geographical and demographic variables likely all contribute to the large disparity in prevalence. Data from the few studies that have used truly random sampling suggest that the prevalence of AMED consumption in the general population is at or below 5% (e.g., Pennay et al., 2015).
4.2. Motives for AMED consumption
The most frequently reported motives for AMED consumption are neutral motives such as “I like the taste.” Negative motives such as “To drink more and not feel as drunk” are less frequently reported. Additionally, the subdivision into neutral and negative motives is straightforward for some items; for others, it can be problematic. For example, “I like the taste” may be considered a neutral motive. However, if those who endorse this motive engage in a significant increase in alcohol consumption, then it could also be considered a negative one. On the other hand, the different motives for AMED consumption appear unrelated to total alcohol consumption on AMED versus AO occasions.
4.3. Characteristics of AMED consumers
A large number of studies presented associations with AMED consumption. These studies should be interpreted with some caution. A significant association should not necessarily imply causal relationships with AMED consumption. Any association may be driven by some third factor. Alternatively, there may be reverse causation. For example, Rossheim et al. (2016) suggested that the association between heavy drinking and being an AMED consumer should be interpreted in an alternative way; that is, the more alcohol you consume, the more likely you also consume an AMED drink. They found a significant association between total alcohol consumption and the number of different types of alcohol consumed.
Between‐group comparisons illustrate that AMED consumers may differ in a cluster of characteristics from those who consume AO. For example, several studies showed that AMED consumers drink more alcohol than those who consume AO. One interpretation is that this is caused by the coconsumption of energy drinks. However, there are other possible explanations. For example, AMED consumers show higher scores on sensation seeking and express more risk‐taking behavior than AO consumers. An alternative interpretation is that AMED consumption is one of a cluster of behaviors expressed by some underlying trait or phenotype. In fact, the within‐subject comparisons show that AMED consumers do not drink more alcohol on AMED occasions when compared to AO occasions (see Figure 3 and 4).
Thus, the observed differences between AMED and AO consumers seem to be presently independent of the consumption of AMED. In other words, the groups may already differ from each other in many respects, and AMED consumption is just one of them. The available data further show that associations that are found in one study may be absent in other studies. This observation illustrates that the occurrence of significant associations depends highly on the characteristics of the sample under investigation. One reason for the conflicting results is that most cross‐sectional studies included relatively small convenience samples of students. It is unclear to what extent these samples are representative for the whole student population, whether they are nationally representative, or how the results translate to other countries.
4.4. Overall alcohol consumption, subjective intoxication, and associated risk‐taking behavior
The meta‐analysis revealed that among AMED consumers, alcohol consumption is not significantly higher on typical AMED occasions when compared to typical AO occasions. Moreover, for the heaviest drinking occasion during the past month, it was shown that AMED consumers drink significantly less alcohol on AMED occasions when compared to AO occasions (see Figures 3 and 4).
When consuming the same amount of alcohol, mixed with energy drink or placebo, experimental studies and on‐premise data showed no evidence of the existence of a “masking effect.” This finding is in line with those from studies examining mixing alcohol with caffeine (Benson et al. (2014). Across various alcohol and caffeine concentrations, no significant difference was found in subjective intoxication scores on AMED and AO occasions.
Within‐subject comparisons show that on AMED occasions, significantly less risk‐taking behavior and negative alcohol‐related consequences were experienced when compared to AO occasions. Higher levels of risk‐taking behavior seem to be a preexisting characteristic of people that also engage in energy drink consumption. The meta‐analyses show that significantly less alcohol is consumed on heaviest drinking AMED occasions when compared to heaviest drinking AO occasions. As the relationship between alcohol consumption and risk taking per se has been established, this finding may also explain why less risk taking is experienced on AMED occasions when compared to AO occasions.
In conclusion, current evidence suggests that mixing alcohol with energy drink does not increase overall alcohol consumption and associated risk‐taking behavior, nor does it have an effect on subjective intoxication. The data do, however, show that excessive alcohol consumption is common among certain populations (e.g., students). The latter deserves attention, and we fully support the notion by authorities such as National Institute on Alcohol Abuse and Alcoholism (NIAAA) that future research should focus on the causes, consequences, and prevention of excessive alcohol consumption per se.
CONFLICT OF INTEREST
This review was supported by Red Bull GmbH. Red Bull GmbH was not involved in the design and conduct of the study, collection, management, analysis, interpretation of the data, or preparation of the manuscript. Joris Verster has received grants/research support from the Dutch Ministry of Infrastructure and the Environment, Janssen Research and Development, Nutricia, Takeda, and Red Bull and has acted as a consultant for Canadian Beverage Association, Centraal Bureau Drogisterijbedrijven, Clinilabs, Coleman Frost, Danone, Deenox, Eisai, Janssen, Jazz, Purdue, Red Bull, Sanofi‐Aventis, Sen‐Jam Pharmaceutical, Sepracor, Takeda, Transcept, Trimbos Institute, and Vital Beverages. Andrew Scholey has received research funding from Abbott Nutriton, Arla Foods, Bayer Healthcare, Cognis, Cyvex, GlaxoSmithKline, Kemin Foods, Naturex, Nestlé, Martek, Masterfoods, Red Bull GmbH, Sanofi, Verdure Sciences, and Wrigley and has acted as a consultant/expert advisor to Abbott Nutrition, Barilla, Bayer Healthcare, Danone, Flordis, GlaxoSmithKline Healthcare, Masterfoods, Martek, Neurobrands, and Wrigley. Chris Alford has undertaken sponsored research, or provided consultancy, for a number of companies and organizations including Airbus Group Industries, Astra, British Aerospace/BAeSystems, Civil Aviation Authority, Duphar, FarmItalia Carlo Erba, Ford Motor Company, ICI, Innovate UK, Janssen, LERS Synthélabo, Lilly, Lorex/Searle, Ministry of Defense, Quest International, Red Bull GmbH, Rhone‐Poulenc Rorer, and Sanofi Aventis. Sean Johnson has undertaken sponsored research for Pfizer, AstraZeneca, Merck, Gilead, Novartis, Roche, Red Bull GmbH, the Department for Transport, and Road Safety Trust. Sarah Benson has received funding from Red Bull GmbH, Kemin Foods, Sanofi Aventis, and GlaxoSmithKline. Samuel Benrejeb Godefroy's research activities are funded by the Ministry of Agriculture, Fisheries, and Food, Government of Quebec, Canada; the Ministry of Science, Technology, and Innovation, Government of Quebec; Canada's Innovation Foundation; the U.S. Department of Agriculture Foreign Agriculture Service; r‐Biopharm GmbH; and r‐Biopharm Canada Inc. Samuel Godefroy acts as an expert advisor for members of the food and beverage industry, international organizations (the Food and Agriculture Organization of the United Nations, the United Nations Industrial Development Organization, and the World Bank), and international food regulators such as the China National Centre for Food Safety Risk Assessment and consumer organizations such as Food Allergy Canada.
Verster JC, Benson S, Johnson SJ, Alford C, Godefroy SB, Scholey A. Alcohol mixed with energy drink (AMED): A critical review and meta‐analysis. Hum Psychopharmacol Clin Exp. 2018;33:e2650 https://doi.org/10.1002/hup.2650
REFERENCES
- Alford, C. , Hamilton‐Morris, J. , & Verster, J. C. (2012). The effect of energy drink in combination with alcohol on performance and subjective awareness. Psychopharmacology, 222, 519–532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arria, A. M. , Caldeira, K. M. , Bugbee, B. A. , Vincent, K. B. , & O'Grady, K. E. (2016). Energy drink use patterns among young adults: Associations with drunk driving. Alcoholism, Clinical and Experimental Research, 40, 2456–2466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Azagba, S. , Langille, D. , & Asbridge, M. (2013). The consumption of alcohol mixed with energy drinks: Prevalence and key correlates among Canadian high school students. CMAJ Open, E19‐E26. https://doi.org/10.9778/cmajo.20120017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Azagba, S. , & Sharaf, M. F. (2014). Is alcohol mixed with energy drinks associated with susceptibility to smoking? Preventive Medicine, 61, 26–28. [DOI] [PubMed] [Google Scholar]
- Benson, S. , & Scholey, A. (2014). Effects of alcohol and energy drink on mood and subjective intoxication: A double‐blind, placebo‐controlled, crossover study. Human Psychopharmacology, 29, 360–369. [DOI] [PubMed] [Google Scholar]
- Berger, L. K. , Fendrich, M. , Chen, H‐Y. , Arria, A. M. , & Cisler, R. A. (2011). Sociodemographic correlates of energy drink consumption with and without alcohol: results of a community survey. Addict Behav, 36, 516–519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benson, S. , Verster, J. C. , Alford, C. , & Scholey, A. (2014). Effects of mixing alcohol with caffeinated beverages on subjective intoxication: a critical review and meta‐analysis. Neuroscience & Biobehavioral Reviews, 47, 16–21. [DOI] [PubMed] [Google Scholar]
- Berger, L. , Fendrich, M. , & Fuhrman, D. (2013). Alcohol mixed with energy drinks: Are there associated negative consequences beyond hazardous drinking in college students? Addictive Behaviors, 38, 2428–2432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bitancourt, T. , Ribeiro Grilli Tissot, M. C. , Marques Fidalgo, T. , Fernandes Galdurόz, J. C. , & da Silveira Filho, D. X. (2016). Factors associated with illicit drugs' lifetime and frequent/heavy use among students results from a population survey. Psychiatry Research, 237, 290–295. [DOI] [PubMed] [Google Scholar]
- Bonar, E. E. , Cunningham, R. M. , Polshkova, S. , Chermack, S. T. , Blow, F. C. , & Walton, M. A. (2015). Alcohol and energy drink use among adolescents seeking emergency department care. Addictive Behaviors, 43, 11–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonar, E. E. , Green, M. R. , & Asfrafioun, I. (2017). Characteristics of university students who mix alcohol and energy drinks. Journal of American College Health. https://doi.org/10.1080/07448481.2017.1280799 [DOI] [PubMed] [Google Scholar]
- Borenstein, M. , & Rothstein, H. (1999). Comprehensive meta‐analysis In A computer program for research synthesis. USA: Biostat Inc. [Google Scholar]
- Brache, K. , & Stockwell, T. (2011). Drinking patterns and risk behaviors associated with combined alcohol and energy drink consumption in college drinkers. Addict Behav, 36, 1133–1140. [DOI] [PubMed] [Google Scholar]
- Cabezas‐Bou, E. , De Leon‐Arbucias, J. , Matos‐Vergara, N. , A'lvarez‐Bagnarol, Y. , Ortega‐Guzman, J. , Narvarez‐Perez, K. , … Dıaz‐Rıos, M. (2016). A survey of energy drink consumption patterns among college students at a mostly Hispanic university. Journal of Caffeine Research, 6, 154–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng, W.‐J. , Cheng, Y. , Huang, M.‐C. , & Chen, C.‐J. (2012). Alcohol dependence, consumption of alcoholic energy drinks and associated work characteristics in the Taiwan working population. Alcohol and Alcoholism, 47, 372–379. [DOI] [PubMed] [Google Scholar]
- Cobb, C. O. , Nasim, A. , Jentink, K. , & Blank, M. D. (2015). The role of caffeine in the alcohol consumption behaviors of college students. Substance Abuse, 36, 90–98. [DOI] [PubMed] [Google Scholar]
- Coomber, K. , Mayshak, R. , Hyder, S. , Droste, N. , Curtis, A. , Pennay, A. , … Miller, P. G. (2017). Demographic and substance use factors associated with non‐violent alcohol‐related injuries among patrons of Australian night‐time entertainment districts. International Journal of Environmental Research and Public Health, 14, 75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtis, A. , Coomber, K. , Hyder, S. , Droste, N. , Pennay, A. , Jenkinson, R. , … Miller, P. G. (2016). Prevalence and correlates of drink driving within patrons of Australian night‐time entertainment precincts. Accident Analysis and Prevention, 95, 187–191. [DOI] [PubMed] [Google Scholar]
- De Haan, L. , de Haan, H. A. , van der Palen, J. , Olivier, B. , & Verster, J. C. (2012). The effects of consuming alcohol mixed with energy drinks (AMED) versus consuming alcohol only on overall alcohol consumption and alcohol‐related negative consequences. International Journal of General Medicine, 5, 953–960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Droste, N. , Miller, P. , Pennay, A. , Zinkiewicz, L. , & Lubman, D. I. (2016). Environmental contexts of combined alcohol and energy drink use: Associations with intoxication in licensed venues. International Journal of Drug Policy, 36, 58–66. [DOI] [PubMed] [Google Scholar]
- Droste, N. , Tonner, L. , Zinkiewicz, L. , Pennay, A. , Lubman, D. I. , & Miller, P. (2014). Combined alcohol and energy drink use: Motivations as predictors of consumption patterns, risk of alcohol dependence, and experience of injury and aggression. Alcoholism, Clinical and Experimental Research, 38, 2087–2095. [DOI] [PubMed] [Google Scholar]
- Eckschmidt, F. , Guerra de Andrade, A. , dos Santos, B. , & Garcia de Oliviera, L. (2013). The effects of alcohol mixed with energy drinks (AmED) on traffic behaviors among Brazilian college students: A national survey. Traffic Injury Prevention, 14, 671–679. [DOI] [PubMed] [Google Scholar]
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies) (2015). Scientific opinion on the safety of caffeine. EFSA Journal, 13, 4102 https://doi.org/10.2903/j.efsa.2015.4102 [Google Scholar]
- Emond, J. A. , Gilbert‐Diamond, D. , Tanski, S. E. , & Sargent, J. D. (2014). Energy drink consumption and the risk of alcohol use disorder among a national sample of adolescents and young adults. The Journal of Pediatrics, 165, 1194–1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferreira, S. E. , de Mello, M. T. , Pompéia, S. , & de Souza‐Formigoni, M. L. O. (2006). Effects of energy drink ingestion on alcohol intoxication. Alcoholism, Clinical and Experimental Research, 30, 598–605. [DOI] [PubMed] [Google Scholar]
- Flotta, D. , Mico, R. , Nobile, C. G. , Pileggi, C. , Bianco, A. , & Pavia, M. (2014). Consumption of energy drinks, alcohol, and alcohol‐mixed energy drinks among Italian adolescents. Alcoholism, Clinical and Experimental Research, 38, 1654–1661. [DOI] [PubMed] [Google Scholar]
- Giles, G. E. , Mahoney, C. R. , Brunyé, T. T. , Gardony, A. L. , Taylor, H. A. , & Kanarek, R. B. (2012). Differential cognitive effects of energy drink ingredients: caffeine, taurine, and glucose. Pharmacol Biochem Behav, 102, 569–577. [DOI] [PubMed] [Google Scholar]
- Gonzales, K. R. , Largo, T. W. , Miller, C. , Kanny, D. , & Brewer, R. D. (2015). Consumption of alcoholic beverages and liquor consumption by Michigan high school students, 2011. Preventing Chronic Disease, 12, 150290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Health Canada (2010). Caffeine. Ministry of Health: Ottawa. [Google Scholar]
- Herberman Mash, H. B. , Fullerton, C. S. , Ramsawh, H. J. , Ng, T. H. , Wang, L. , Kessler, R. C. , … Ursano, S. J. (2014). Risk for suicidal behaviors associated with alcohol and energy drink use in the US Army. Social Psychiatry and Psychiatric Epidemiology, 49, 1379–1387. [DOI] [PubMed] [Google Scholar]
- Holubcikova, J. , Kolarcik, P. , Geckova, A. M. , Joppova, E. , van Dijk, J. P. , & Reijneveld, S. A. (2016). Young adolescents who combine alcohol and energy drinks have a higher risk of reporting negative behavioural outcomes. International Journal of Public Health. https://doi.org/10.1007/s00038-016-0862-4 [DOI] [PubMed] [Google Scholar]
- Housman, J. M. , Williams, R. D. , & Woolsey, C. L. (2016). Impact of alcohol and alcohol mixed with energy drinks on non‐medical prescription stimulant use in a nationally representative sample of 12th‐grade students. The American Journal of Addictions, 25, 378–384. [DOI] [PubMed] [Google Scholar]
- Ilie, G. , Boak, A. , Mann, R. E. , Adlat, E. M. , Hamilton, H. , Asbridge, M. , … Cusimano, M. D. (2015). Energy drinks, alcohol, sports and traumatic brain injuries among adolescents. PLOS One. https://doi.org/10.1371/journal.pone.0135860 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson, S. J. , Alford, C. , Stewart, K. , & Verster, J. C. (2016). A UK student survey investigating the effects of consuming alcohol mixed with energy drinks on overall alcohol consumption and alcohol‐related negative consequences. Preventive Medicine Reports, 4, 496–501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson, S. J. , Alford, C. , Verster, J. C. , & Stewart, K. (2016). Motives for mixing alcohol with energy drinks and other non‐alcoholic beverages and its effects on overall alcohol consumption among UK students. Appetite, 56, 588–597. [DOI] [PubMed] [Google Scholar]
- Khan, S. R. , Cottler, L. B. , & Striley, C. W. (2016). Correlates of use of alcohol mixed with energy drinks among youth across 10 US metropolitan areas. Drug and Alcohol Dependence, 163, 236–241. [DOI] [PubMed] [Google Scholar]
- Knapik, J. J. , Trone, D. W. , McGraw, S. , Steelman, R. A. , Austin, K. G. , & Lieberman, H. R. (2016). Caffeine use among active duty Navy and Marine Corps personnel. Nutrients, 8, 620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kristjansson, A. L. , Mann, M. J. , Sigfusdottir, I. D. , & James, J. E. (2015). Mode of daily caffeine consumption among adolescents and the practice of mixing alcohol with energy drinks: Relationship to drunkenness. Journal of the Study on Alcohol and Drugs, 76, 397–405. [DOI] [PubMed] [Google Scholar]
- Lipsey, M. W. , & Wilson, D. (2000). Practical meta‐analysis (applied social research methods). London: Sage Publications, Inc. [Google Scholar]
- Locatelli, D. , Sanchez, Z. , Opaleye, E. , Carlini, C. , & Noto, A. (2012). Socioeconomic influences on alcohol use patterns among private school students in Sao Paulo. Revista Brasileira de Psiquiatria, 34, 193–200. [DOI] [PubMed] [Google Scholar]
- Lubman, D. L. , Peacock, A. , Droste, N. , Pennay, A. , Miller, P. , Bruno, R. , … Brown, J. (2013). Alcohol and energy drinks in NSW. (a,b). Available at: http://www.health.nsw.gov.au
- Lubman, D. I. , Droste, N. , Pennay, A. , Hyder, S. , & Miller, P. (2014). High rates of alcohol consumption and related harm at schoolies week: A portal study. Australian and New Zealand Journal of Public Health, 2014(38), 536–541. [DOI] [PubMed] [Google Scholar]
- Magnezi, R. , Bergman, L. C. , Grinvald‐Vogel, H. , & Cohen, H. A. (2015). A survey of energy drink and alcohol mixed with energy drink consumption. Israel Journal of Health Policy Research, 4, 55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malinauskas, B. M. , Aeby, V. G. , Overton, R. F. , Carpenter‐Aeby, T. , & Barber‐Heidal, K. (2007). A survey of energy drink consumption patterns among college students. Nutrition Journal, 6, 35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallett, K. A. , Marzell, M. , Scaglione, N. , Hultgren, B. , & Turrisi, R. (2014). Are all alcohol and energy drink users the same? Examining individual variation in relation to alcohol mixed with energy drink use, risky drinking, and consequences. Psychology of Addictive Behaviors, 28, 97–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallett, K. A. , Scaglione, N. , Reavy, R. , & Turrisi, R. (2015). Longitudinal patterns of alcohol mixed with energy drink use among college students and their associations with risky drinking and problems. Journal of Studies on Alcohol and Drugs, 76, 389–396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marczinski, C. A. (2011). Alcohol mixed with energy drinks: consumption patterns and motivations for use in US college students. International Journal of Environmental Research and Public Health, 8, 3232–3245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marczinski, C. A. , & Fillmore, M. T. (2006). Clubgoers and their trendy cocktails: Implications of mixing caffeine into alcohol on information processing and subjective reports of intoxication. Experimental and Clinical Psychopharmacology, 14, 450–458. [DOI] [PubMed] [Google Scholar]
- Marczinski, C. A. , Fillmore, M. , Bardgett, M. , & Howard, M. (2011). Effects of energy drinks mixed with alcohol on behavioral control: Risks for college students consuming trendy cocktails. Alcoholism, Clinical and Experimental Research, 35, 1282–1292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marczinski, C. A. , Fillmore, M. T. , Henges, A. L. , Ramsey, M. A. , & Young, C. R. (2012). Effects of energy drinks mixed with alcohol on information processing, motor coordination and subjective reports of intoxication. Alcoholism, Clinical and Experimental Research, 20, 129–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marczinski, C. A. , Fillmore, M. T. , Henges, A. L. , Ramsey, M. A. , & Young, C. R. (2013). Mixing an energy drink with an alcoholic beverage increases motivation for more alcohol in college students. Alcoholism, Clinical and Experimental Research, 37, 276–283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marczinski, C. A. , Fillmore, M. T. , Stamates, A. L. , & Maloney, S. F. (2016). Desire to drink alcohol is enhanced with high caffeine energy drink mixers. Alcoholism, Clinical and Experimental Research, 40, 1982–1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marczinski, C. A. , Fillmore, M. T. , Maloney, S. F. , & Stamates, A. L. (2017). Faster self‐paced rate of drinking for alcohol mixed with energy drinks versus alcohol alone. Psychology of Addictive Behaviors, 31(2), 154–161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martz, M. E. , Patrick, M. E. , & Schulenberg, J. E. (2015). Alcohol mixed with energy drink use among U.S. 12th‐grade students: Prevalence, correlates, and associations with unsafe driving. Journal of Adolescent Health, 56, 557–563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marzell, M. , Turrisi, R. , Mallett, K. , Ray, A. E. , & Scaglione, N. M. (2014). Combining alcohol and energy drinks: An examination of psychosocial constructs and alcohol outcomes among college students using a longitudinal design. Addiction Research and Theory, 22, 91–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKetin, R. , & Coen, A. (2014). The effect of energy drinks on the urge to drink alcohol in young adults. Alcoholism, 38, 2279–2285. [DOI] [PubMed] [Google Scholar]
- Milicic, S. , & Leatherdale, S. T. (2016). The associations between e‐cigarettes and binge drinking, marijuana use, and energy drinks mixed with alcohol. Journal of Adolescent Health, in press. [DOI] [PubMed] [Google Scholar]
- Miller, K. E. (2012). Alcohol mixed with energy drink use and sexual risk‐taking: Causal, intoxicated, and unprotected sex. Journal of Caffeine Research, 2, 62–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller, K. E. , Quigley, B. M. , Elisio‐Arras, R. K. , & Ball, N. J. (2016). Alcohol mixed with energy drink use as an event‐level predictor of physical and verbal aggression in bar conflicts. Alcoholism, Clinical and Experimental Research, 40, 161–169. [DOI] [PubMed] [Google Scholar]
- Nawrot, P. , Jordan, S. , Eastwood, J. , Rotstein, J. , Hugenholtz, A. , & Feeley, M. (2003). Effects of caffeine on human health. Food Additives and Contaminants, 20(1), 1–30. [DOI] [PubMed] [Google Scholar]
- Nowak, D. , & Jasionowski, A. (2016). Analysis of consumption of energy drinks by a group of adolescent athletes. International Journal of Environmental Research and Public Health, 13, 768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Brien, M. C. , McCoy, T. P. , Rhodes, S. D. , Wagoner, A. , & Wolfson, M. (2008). Caffeinated cocktails: Energy drink consumption, high‐risk drinking, and alcohol‐related consequences among college students. Academic Emergency Medicine, 15, 453–460. [DOI] [PubMed] [Google Scholar]
- Patrick, M. E. , & Maggs, J. L. (2014). Energy drinks and alcohol: Links to alcohol behaviors and consequences across 56 days. Journal of Adolescent Health, 54, 454–459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patrick, M. E. , Evans‐Polce, R. J. , & Maggs, J. L. (2014). Use of alcohol mixed with energy drinks as a predictor of alcohol‐related consequences two years later. Journal of Studies on Alcohol and Drugs, 75, 753–757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patrick, M. E. , Macuada, C. , & Maggs, L. (2016). Who uses alcohol mixed with energy drinks? Characteristics of college student users. Journal of American College Health, 64, 74–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peacock, A. , & Bruno, R. (2015). Young adults who mix alcohol with energy drinks: Typology of risk‐taking behavior. Addictive Behaviors, 45, 252–258. [DOI] [PubMed] [Google Scholar]
- Peacock, A. , Bruno, R. , & Martin, F. H. (2012). The subjective physiological, psychological, and behavioral risk‐taking consequences of alcohol and energy drink co‐ingestion. Alcoholism, Clinical and Experimental Research, 36, 2008–2015. [DOI] [PubMed] [Google Scholar]
- Peacock, A. , Bruno, R. , Martin, F. H. , & Carr, A. (2013). The impact of alcohol and energy drink consumption on intoxication and risk‐taking behaviour. Alcoholism, Clinical and Experimental Research, 37, 1234–1242. [DOI] [PubMed] [Google Scholar]
- Peacock, A. , Bruno, R. , & Martin, F. H. (2013). Patterns of use and motivations for consuming alcohol mixed with energy drinks. Psychology of Addictive Behaviors, 27, 202–206. [DOI] [PubMed] [Google Scholar]
- Peacock, A. , Bruno, R. , Martin, F. H. , & Carr, A. (2014). Self‐reported physiological and psychological side‐effects of an acute alcohol and energy drink dose. Appetite, 76, 60–65. [DOI] [PubMed] [Google Scholar]
- Peacock, A. , Droste, N. , Pennay, A. , Lubman, D. I. , Miller, P. , Newcombe, D. , & Bruno, R. (2015). Self‐reported risk‐taking behavior during matched‐frequency sessions of alcohol versus combined alcohol and energy drinks consumption: Does co‐ingestion increase risk‐taking? Alcoholism, Clinical and Experimental Research, 39, 911–918. [DOI] [PubMed] [Google Scholar]
- Peacock, A. , Droste, N. , Pennay, A. , Miller, P. , Lubman, D. I. , & Bruno, R. (2015). Typology of alcohol mixed with energy drink consumers: Motivations for use. Alcoholism, Clinical and Experimental Research, 39, 1083–1092. [DOI] [PubMed] [Google Scholar]
- Peacock, A. , Sindicich, N. , Dunn, M. , Whittaker, E. , Sutherland, R. , Entwistle, G. , … Bruno, R. (2016). Co‐ingestion of energy drinks with alcohol and other substances among a sample of people who regularly use ecstasy. Drug and Alcohol Review, 35, 352–358. [DOI] [PubMed] [Google Scholar]
- Pennay, A. , & Lubman, D. I. (2012). Alcohol and energy drinks: A pilot study exploring patterns of consumption, social contexts, benefits and harms. BMC Research Notes, 5, 369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pennay, A. , Miller, P. , Busija, L. , Jenkinson, R. , Droste, N. , Quinn, B. , … Lubman, D. I. (2014). ‘Wide awake drunkenness’? Investigating the association between alcohol intoxication and stimulant use in the night‐time economy. Addiction, 110, 356–365. [DOI] [PubMed] [Google Scholar]
- Pennay, A. , Cheetham, A. , Droste, N. , Miller, P. , Lloyd, B. , Pennay, D. , … Lubman, D. I. (2015). An examination of the prevalence, consumer profiles, and patterns of energy drink use, with and without alcohol, in Australia. Alcoholism, Clinical and Experimental Research, 39, 1485–1492. [DOI] [PubMed] [Google Scholar]
- Penning, R. , de Haan, L. , & Verster, J. C. (2011). Caffeinated drinks, alcohol consumption, and hangover severity. The Open Neuropsychopharmacology Journal, 4, 36–39. [Google Scholar]
- Pettigrew, S. , Biagioni, N. , Jones, S. C. , Stafford, J. , Chikritzhs, T. , & Daube, M. (2016). Factors influencing young people's use of alcohol mixed with energy drinks. Appetite, 96, 408–415. [DOI] [PubMed] [Google Scholar]
- Price, S. R. , Hilchey, C. A. , Darredeau, C. , Fulton, H. G. , & Barrett, S. P. (2016). Energy drink co‐administration is associated with increased reported alcohol ingestion. Drug and Alcohol Review, 29, 331–333. [DOI] [PubMed] [Google Scholar]
- Reid, J. L. , Hammond, D. , McCrory, C. , Dubin, J. A. , & Leatherdale, S. T. (2015). Use of caffeinated energy drinks among secondary school students in Ontario: Prevalence and correlates of using energy drinks and mixing with alcohol. Canadian Journal of Public Health, 106, e101–e108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rossheim, M. E. , & Thombs, D. L. (2011). Artificial sweeteners, caffeine, and alcohol intoxication in bar patrons. Alcohol Clinical Experimental Research, 35, 1891–1896. [DOI] [PubMed] [Google Scholar]
- Rossheim, M. E. , Thombs, D. L. , Weiler, R. M. , Barry, A. E. , Suzuki, S. , Walters, S. T. , … Cannell, B. (2016). Alcohol mixed with energy drink: Use may be a consequence of heavy drinking. Addictive Behaviors, 57, 55–61. [DOI] [PubMed] [Google Scholar]
- Rutledge, P. , Bestrashniy, J. R. B. M. , & Nelson, T. F. (2016). Problematic drinking among postgraduate students: Binge drinking, prepartying, and mixing alcohol with energy drinks. Substance Use & Misuse, 51, 972–982. [DOI] [PubMed] [Google Scholar]
- Scholey, A. B. , & Kennedy, D. O. (2004). Cognitive and physiological effects of an “energy drink”: An evaluation of the whole drink and of glucose, caffeine and herbal flavouring fractions. Psychopharmacology (Berl), 176, 320–330. [DOI] [PubMed] [Google Scholar]
- Snipes, D. J. , & Benotsch, E. G. (2013). High‐risk cocktails and high‐risk sex: Examining the relation between alcohol mixed with energy drink consumption, sexual behavior, and drug use in college students. Addictive Behaviors, 38, 1418–1423. [DOI] [PubMed] [Google Scholar]
- Snipes, D. J. , Green, B. A. , Javier, S. J. , Perrin, P. B. , & Benotsch, E. G. (2014). The use of alcohol mixed with energy drinks and experiences of sexual victimization among male and female college students. Addictive Behaviors, 39, 259–264. [DOI] [PubMed] [Google Scholar]
- Snipes, D. J. , Jeffers, A. J. , Green, B. A. , & Benotsch, E. G. (2015). Alcohol mixed with energy drinks are robustly associated with patterns of problematic alcohol consumption among young adult college students. Addictive Behaviors, 41, 136–141. [DOI] [PubMed] [Google Scholar]
- Sweeney, M. M. , Meredith, S. E. , Evatt, D. P. , & Griffiths, R. R. (2017). Effects of caffeine on alcohol reinforcement: Beverage choice, self‐administration, and subjective rating. Psychopharmacology. https://doi.org/10.1007/s00213-017-4528-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trapp, G. S. , Allen, K. L. , O'Sullivan, T. , Robinson, M. , Jacoby, P. , & Oddy, W. H. (2014). Energy drink consumption among young Australian adults: Associations with alcohol and illicit drug use. Drug and Alcohol Dependence, 134, 30–37. [DOI] [PubMed] [Google Scholar]
- Tucker, J. S. , Troxel, W. M. , Ewing, B. A. , & D'Amico, E. J. (2016). Alcohol mixed with energy drinks: Associations with risky drinking and functioning in high school. Drug and Alcohol Dependence, 167, 36–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ulbrich, A. , Hemberger, S. H. , Loidl, A. , Dufek, S. , Pablik, E. , Fodor, S. , … Aufricht, C. (2013). Effects of alcohol mixed with energy drink and alcohol alone on subjective intoxication. Amino Acids, 45, 1385–1393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van de Loo, A. J. A. E. , van Andel, N. , van Gelder, C. A. G. H. , Janssen, B. S. G. , Titulaer, J. , Jansen, J. , & Verster, J. C. (2016). The effects of alcohol mixed with energy drink (AMED) on subjective intoxication and alertness: Results from a double‐blind placebo‐controlled clinical trial. Human Psychopharmacology, 31, 200–205. [DOI] [PubMed] [Google Scholar]
- Varvil‐Weld, L. , Marzell, M. , Turrisi, R. , Mallett, K. A. , & Cleveland, M. J. (2013). Examining the relationship between alcohol–energy drink risk profiles and high‐risk drinking behaviors. Alcoholism, Clinical and Experimental Research, 37, 1410–1416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verster, J. C. , Aufricht, C. , & Alford, C. (2012). Energy drinks mixed with alcohol: Misconceptions, myths, and facts. International Journal of General Medicine, 5, 187–198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verster, J. C. , Benjaminsen, J. M. E. , van Lanen, J. H. M. , van Stavel, N. M. D. , & Olivier, B. (2015). Effects of mixing alcohol with energy drink on objective and subjective intoxication: Results from a Dutch on‐premise study. Psychopharmacology, 232, 835–842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verster, J. C. , Benson, S. , & Scholey, A. (2014). Motives for mixing alcohol with energy drinks and other nonalcoholic beverages, and consequences for overall alcohol consumption. International Journal of General Medicine, 7, 285–293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verster, J. C. , & Konig, J. (2017). Caffeine intake and its sources: A review of national representative studies. Critical Reviews in Food Science and Nutrition, in press. [DOI] [PubMed] [Google Scholar]
- Vitiello, V. , Diolordi, L. , Donini, L. M. , & del Balzo, V. (2016). Energy drink consumption in Italian university students: Food habits and lifestyle. Clinical Therapeutics, 6, 175–181. [DOI] [PubMed] [Google Scholar]
- Wells, B. E. , Kelly, B. C. , Pawson, M. , LeClair, A. , Parsons, J. T. , & Golub, S. A. (2013). Correlates of concurrent energy drink and alcohol use among socially active adults. The American Journal of Drug and Alcohol Abuse, 39, 8–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woolsey, C. , Waigandt, A. , & Beck, N. C. (2010). Athletes and energy drinks: Reported risk‐taking and consequences from the combined use of alcohol and energy drinks. Journal of applied sport psychology, 22, 65–71. [Google Scholar]
- Woolsey, C. L. , Jacobson, B. H. , Williams, R. D. Jr. , Barry, A. E. , Davidson, R. T. , Evans, M. W. Jr. , & Beck, N. C. (2015). A comparison of the combined‐use of alcohol & energy drinks to alcohol‐only on high‐risk drinking and driving behaviors. Substance Use & Abuse, 50, 1–7. [DOI] [PubMed] [Google Scholar]
- Woolsey, C. L. , Williams, R. D. , Housman, J. M. , Barry, A. E. , Jacobson, B. H. , & Evans, M. W. (2015). Combined use of alcohol and energy drinks increases participation in high‐risk drinking and driving behaviors among college students. Journal of Studies on Alcohol and Drugs, 76, 615–619. [DOI] [PubMed] [Google Scholar]