

Abstract
Objective
To define the demographic and clinical characteristics of persons with spinal cord injury, rehabilitated in a primary referral rehabilitation center in Turkey.
Design
Retrospective study.
Setting
Ankara Physical Medicine and Rehabilitation Training and Research Hospital, Ankara, Turkey.
Methods
Medical records of all patients with spinal cord injury (acute-subacute-chronic) at a single academic referral center over the course of one year were reviewed. Variables of each patient were recorded, including: age, sex, etiology, length of rehabilitation stay, neurological level of injury, level of neurological impairment and severity of injury.
Results
Among 262 persons with spinal cord injury, 69.8% were male (male:female ratio is 2.31 : 1). Mean age was 38.3 ± 17.6 years. Falls were the most common cause of injury. The majority of falls were falls from a height (93.3%). More than 20% of falls from a height were related to occupational injury. The most common neurological level of injury was L1. Of all persons 46.2% had thoracic, 27.5% had lumbar and 26.3% had cervical lesions. The mean length of rehabilitation stay was 52.1 ± 25.5 days. Persons with motor complete injury and with a shorter (<12 months) time since injury had longer length of rehabilitation stay.
Conclusion
The mean age of SCI population is increasing. Falls constitute the majority of etiologic factors and are more common in persons >60 years old. More than 20% of falls from a height are related to occupational injury. Male-female ratio is decreasing. Thoraco-lumbar injures are more common than cervical injuries.
Keywords: Demographics, Epidemiology, Etiology, Spinal cord injury, Turkey
Introduction
Epidemiological and demographic characteristics of spinal cord injury (SCI) vary according to region and time. In Turkey an incidence of 8–21 cases per million population has been reported from different regions and at different times.1,2 Investigations about the demographic and clinical characteristics of SCI provide better understanding about the reasons, risk factors, clinical consequences and complications of SCI, leading to improvement of preventive strategies. In the literature there are only a few outdated studies from Turkey about the demographics and clinical properties of SCI.1–5
The aim of the present study was to identify the up to date clinical and demographic characteristics of persons with SCI admitted to a referral rehabilitation center which represents the whole segments of Turkish population.
Methods
The hospital ethical committee's approval was obtained. The medical records of all persons with SCI (acute-subacute-chronic) rehabilitated in Ankara Physical Medicine and Rehabilitation (APMR) Training and Research Hospital during 1-year period between June 1, 2013 and May 31, 2014 were reviewed retrospectively. The persons whose rehabilitation programme had been started before June 1, 2013 or lasted after May 31, 2014 were excluded even if they were on inpatient rehabilitation programme between these dates. APMR Training and Research Hospital is a major rehabilitation center of Turkey, where the persons with SCI are most commonly referred nation-wide, and is located in the capital city Ankara. Ankara is located in the middle part of Turkey and transportation to Ankara is easy from all parts of Turkey. APMR Training and Research Hospital has the maximal bed capacity among all rehabilitation centers affiliated to the Turkish Ministry of Health. Each year 350–400 persons with SCI from all parts of Turkey are rehabilitated at this center.
Two hundred sixty-two consecutive persons with SCI were included in the study. For missing information, patient interviews were carried out by telephone calls. The demographic and clinical characteristics of the persons including the age at the time of injury, sex, etiology, time since injury (time passed since the first day of SCI), length of rehabilitation stay (LORS), neurological level of injury (NLI), level of neurological impairment (LNI), lesion severity, existence of associated injuries, existence of vertebral fracture/dislocation, history of surgical management and discharge destination were recorded. The persons were divided into six age groups as 0–15, 16–30, 31–45, 46–60, 61–75 and ≥76.6 Causes of injury were grouped as motor vehicle accident (MVA), fall (fall from height, simple fall), iatrogenic, gunshot wound (GW), stab-wound (SW), fall of weight, tumor and diving accident. Fall from height is defined according to ICD 10 codes W 10–15 as fall from stairs/ steps/ ladder/ scaffolding/ building/ structure/ tree/ cliff. Simple fall is defined as a low energy fall while standing or walking on ground level . Fall of weight is defined as being trapped in the wreckage or being crushed under a falling heavy object . Etiologic factors were also grouped into two categories as traumatic (MVA, fall, GW, SW, fall of weight, diving accident) and non-traumatic (tumor, iatrogenic) for further statistical analysis. NLI refers to the most caudal segment of the spinal cord with normal sensory and antigravity motor function on both sides of the body, provided that there is normal (intact) sensory and motor function rostrally.7 It was defined from cervical 1st vertebra (C1) to lumbar 5th vertebra (L5) and also grouped as cervical, thoracic and lumbar for further analysis. Level of neurological impairment was determined according to the American Spinal Injury Association (ASIA) Impairment Scale (AIS) as AIS A-B-C-D and E.8 Persons were further categorized as motor complete SCI (including subjects AIS A and B) and motor incomplete SCI (including subjects AIS C, D and E) for some statistical analysis.9,10 Lesion severity was defined as, complete tetraplegia, incomplete tetraplegia, complete paraplegia and incomplete paraplegia.7
The study protocol was approved by the hospital ethics committee.
Statistical analysis
Statistical analyses were performed by using SPSS version 11.5 software (SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was used to determine whether the continuous variable distribution was normal. Descriptive statistics were provided as mean ± standard deviation or median (minimum–maximum) for continuous variables while the number of cases and percentages were used for nominal variables. The Mann–Whitney U test was used to determine whether a statistically significant difference was present for continuous or orderable variables not normally distributed. χ2 test was used for categorical comparisons. When comparing more than 2 groups, Kruskal-Wallis test was used for non-normally distributed numerical variables. Bonferroni corrected Mann-Whitney U test was used for paired comparisons. A P value <0.05 was considered statistically significant.
Results
During 1-year study period, 262 persons with SCI were admitted to APMR Training and Research Hospital.
Age and sex
Of all persons 183 were male (69.8%) and 79 were female (30.2%). Male:female ratio is 2.31:1. Mean age at the time of injury was 38.3 ± 17.6 years (median: 35, range: 2–80 years). Most of the study population were aged 16–30 years (n=86, 32.8%) at the time of injury, followed by the group of 31–45 years (n = 68, 26%). Age group distribution of males and females was shown on Fig. 1. Mean age of males was 37.3 ± 16.7 (median: 34, range: 2–80) years and mean age of females was 40.7 ± 19.5 (median: 39, range: 9–77) years at the time of injury and there was no statistically significant difference between them. (P = 0.248) (Mann-Whitney U test) When sex distribution between different age groups was analysed male dominancy in 16–30, 31–45, 46–60 age groups was observed and rates were similar in 0–15, 61–75 and ≥76 age groups.
Figure 1.
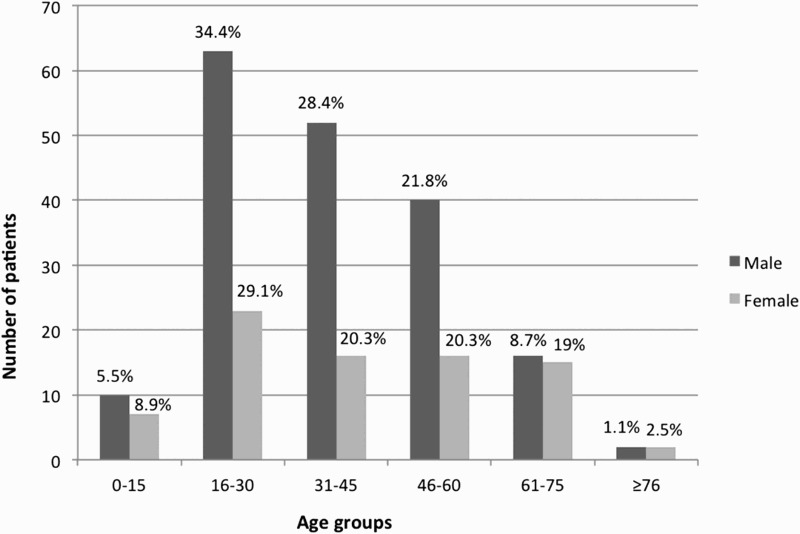
Age distribution of male and female persons with SCI (percentages at the top of columns mean % value of all males/females).
Etiology
The most common cause of injury was falls (34.4%), followed by MVA (30.2%), iatrogenic (9.9%), tumors (8%), violence (7.6%) (GW 6.46% and SW 1.14%), fall of weight (4.6%), and diving accidents (1.9%). The remaining 3.4% was due to miscellanous etiology. Among 26 persons with iatrogenic SCI, there were 11 with failed neck surgery, 10 with failed back surgery, 1 with thoracic spine surgery, 3 with scoliosis/kyphosis surgery and 1 with abdominal aortic aneurysm repair. Etiologic distribution according to gender was shown on Fig. 2. The majority of falls were falls from a height (93.3%). More than 20% of falls from a height and 75% of falls of weight were related to occupational injury. Occupational causes constitute up to 10.3% of all SCIs and 13.1% of traumatic SCIs. Only 1.9% of all SCIs were attempted suicide and all of them were due to fall from a height. A significant difference was observed when the median age of the persons in different etiologic groups were compared (Table 1). The subgroup analysis revealed statistically significant difference between the median ages of falls and iatrogenic SCIs (P < 0.001), MVAs and iatrogenic SCIs (P < 0.001), MVAs and tumors (P = 0.001), violence and iatrogenic SCIs (P = 0.000), violence and tumors (P = 0.001), fall of weight and iatrogenic SCIs (P < 0.001), diving accidents and iatrogenic SCIs (P = 0.002), diving accidents and tumors (P = 0.004). Age group distribution according to etiology was shown in Table 2. NLI and sex distribution according to different etiologies were also given in Table 3.
Figure 2.
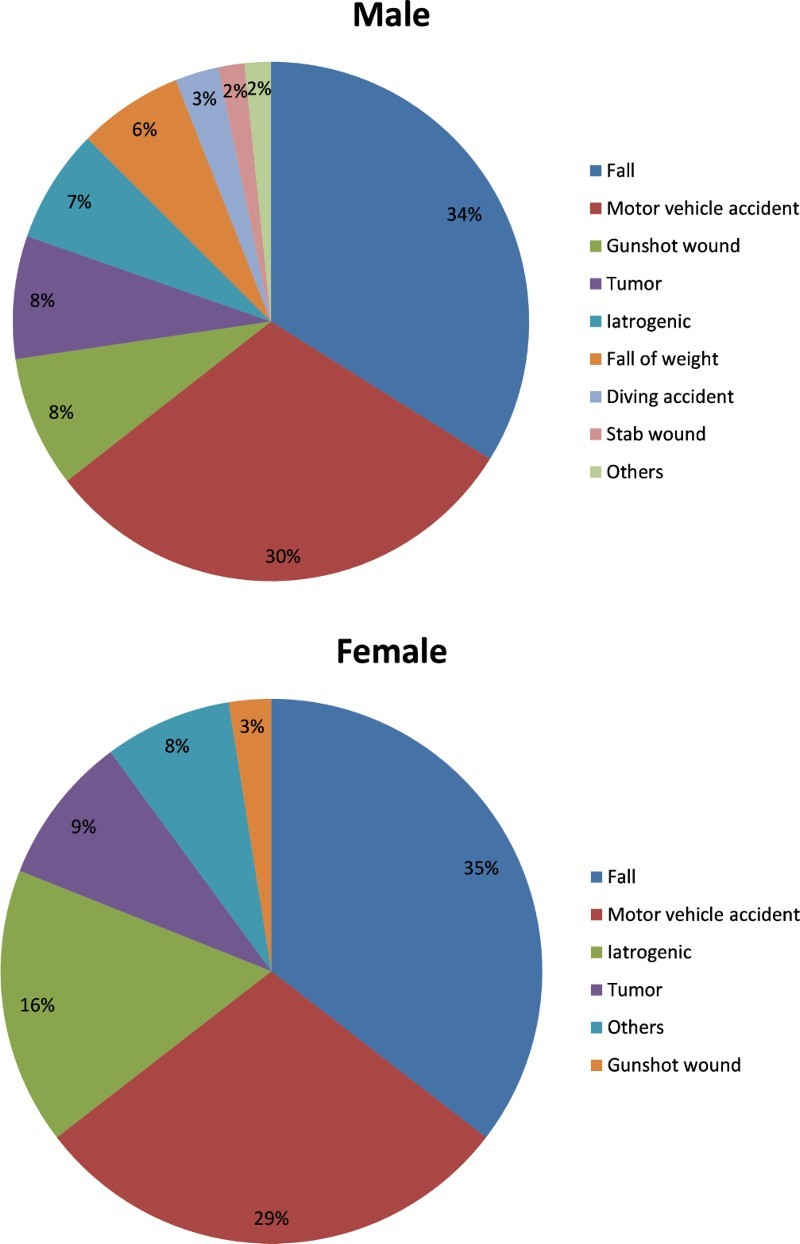
Etiologic distribution of male and female persons with SCI.
Table 1.
Age at the time of injury according to SCI etiology.
| Etiology | Age mean ± SD, median (min-max) | P |
|---|---|---|
| Fall (n = 90) | 38.1 ± 17.8, 34 (2–77) | 0.000 |
| Motor vehicle accident (n = 79) | 33.3 ± 15.3, 30 (11–75) | |
| Iatrogenic (n = 26) | 55 ± 18, 56.5 (14–80) | |
| Tumor (n = 21) | 46 ± 15.4, 49 (15–73) | |
| Violence (n = 20) | 29.5 ± 11.8, 30 (3–51) | |
| Fall of weight (n = 12) | 38 ± 12, 36 (17–59) | |
| Diving accident (n = 5) | 19.4 ± 6.1, 17 (13–28) | |
| Others (n = 9) | 48.7 ± 18.5, 53 (19–72) |
***Kruskal Wallis test, Bonferroni correction.
Table 2.
Age group distribution of patients according to SCI etiology.
| Etiology | 0–15 years | 16–30 years | 31–45 years | 46–60 years | 61–75 years | ≥76 |
|---|---|---|---|---|---|---|
| Fall (n = 90) | ||||||
| Fall from a height (n = 84) | ||||||
| Occupational (n = 18) | 7(38.9%) | 9(50%) | 2(11.1%) | |||
| Accidental (n = 61) | 5 (8.2%) | 17(27.9%) | 15(24.6%) | 14(23%) | 9(14.8%) | 1(1.6%) |
| Suicide (n = 5) | 1(20%) | 4(80%) | ||||
| Simple fall (n = 6) | 1(16.7%) | 1(16.7%) | 1(16.7%) | 1(16.7%) | 2(33.3%) | |
| Motor vehicle accident (n = 79) | 4 (5.1%) | 36(45.6%) | 22(27.8%) | 12(15.2%) | 5(6.3%) | |
| Iatrogenic (n = 26) | 2(7.7%) | 4(15.4%) | 8(30.8%) | 11(42.3%) | 1(3.8) | |
| Tumor (n = 21) | 1(4.8%) | 3(14.3%) | 5(23.8%) | 9(42.9%) | 3(14.3%) | |
| Gunshot wound (n = 17) | 2(11.8%) | 6(35.3%) | 6(35.3%) | 3(217.6%) | ||
| Fall of weight (n = 12) | ||||||
| Occupational (n = 9) | 3(33.3%) | 3(33.3%) | 3(33.3%) | |||
| Accidental (n = 3) | 1(33.3%) | 2(66.7%) | ||||
| Diving accident (n = 5) | 1 (20%) | 4(80%) | ||||
| Stabwound (n = 3) | 2(66.7%) | 1(33.3%) | ||||
| Others (n = 9) | 2(22.2%) | 1(11.1%) | 4(44.4%) | 2(22.2%) |
Table 3.
Neurological level of injury and sex distribution of patients according to SCI etiology.
| Neurological level of injury (n,%) |
Sex (n,%) |
||||
|---|---|---|---|---|---|
| Etiology (n) | Cervical | Thoracal | Lumbar | Male | Female |
| Fall (n = 90) | 6 (6.7%) | 51 (56.7%) | 33 (36.7%) | 62 (68.9%) | 28 (31.1%) |
| MVA (n = 79) | 36 (45.6%) | 31 (39.2%) | 12 (15.2%) | 56 (70.9%) | 23 (29.1%) |
| Iatrogenic (n = 26) | 9(34.6%) | 8(30.8%) | 9(34.6%) | 13 (50%) | 13 (50%) |
| Tumor (n = 21) | 5(23.8%) | 11(52.4%) | 5(23.8%) | 14 (66.7%) | 7 (33.7%) |
| Gunshot wound (n = 17) | 4(23.5%) | 12(70.6%) | 1(5.9%) | 15 (88.2%) | 2 (11.8%) |
| Fall of weight (n = 12) | 0(0%) | 3 (25%) | 9(75%) | 12 (100%) | 0 (0%) |
| Diving accident (n = 5) | 5(100%) | 0(0%) | 0(0%) | 5 (100%) | 0 (0%) |
| Stab wound (n = 3) | 1 (33.3%) | 2(66.7%) | 0(0%) | 3 (100%) | 0 (0%) |
| Others (n = 9) | 3(33.3%) | 3(33.3%) | 3(33.3%) | 3 (33.3%) | 6 (66.7%) |
Level and severity of injury
The most common NLI was L1, followed by T12, L2 and then C4 respectively. L1 was the most common level in males, whereas T12 was the most common level among females. Injury level distribution was shown on Fig. 3. There is a bimodal distribution of lesion level which is similar for both males and females. The most prominent peak is at T12-L1-L2 levels followed by C4-C5-C6-C7. (Fig. 3) When NLI was grouped as cervical, thoracic and lumbar, there was no statistically significant difference between males and females in the means of NLI (P = 0.207) (χ2 test). Of all persons 46.2% had thoracic, 27.5% had lumbar and 26.3% had cervical lesions. The distribution of persons according to lesion severity and AIS was shown in Tables 4 and 5.
Figure 3.
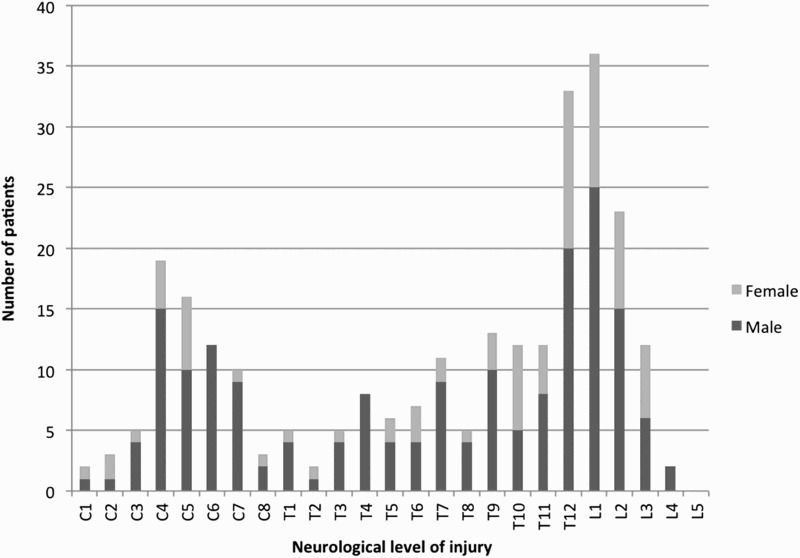
Injury level distribution of male and female persons with SCI.
Table 4.
Severity of SCI (n = 262).
| Complete n, (%) | Incomplete n, (%) | |
|---|---|---|
| Tetraplegia n (%) | 16 (6.1%) | 53 (20.2%) |
| Paraplegia n (%) | 76 (29%) | 117 (44.7%) |
Table 5.
LNI of SCI patients (n = 262).
| AIS | n (%) |
|---|---|
| A | 93 (35.5%) |
| B | 43 (16.4%) |
| C | 56 (21.4%) |
| D | 69 (26.3%) |
| E | 1 (0.4%) |
Surgical intervention, associated lesions, length of rehabilitation stay and discharge destination
Among all persons with SCI, 71.8% had vertebral fracture and/or dislocation and 89.6% had some kind of surgical intervention of the spine. Associated injuries, including upper/lower extremity fractures, thoracic injury, head injury and abdominal injuries, were found in 27.5% of the study population.
The mean length of rehabilitation stay (LORS) was 52.1 ± 25.5 days, (median: 49). Persons with motor complete SCI had a longer LORS (median: 56, min-max: 1–149 days) compared to persons with motor incomplete SCI (median: 44, min-max: 4–165 days), and this was statistically significant. (P = 0.002) (Mann-Whitney U) Moreover persons with a disease duration < 12 months had longer LORS (median: 56, min-max: 4–165 days) than persons with a disease duration > 12 months (median: 43, min-max: 1–96 days). (P < 0.001) (Mann Whitney U) Age (P = 0.142) (Kruskal Wallis), sex (P = 0.163)(Mann Whitney U)and NLI (P = 0.956) (Kruskal Wallis) had no statistically significant effect on LORS. All of the study population was discharged at the end of the rehabilitation period., 90.8% were discharged home and 9.2% were discharged to other facilities like nursing home, emergency units of other hospitals for acute problems, etc.
Discussion
The present study is an update study which represents the whole SCI population in Turkey. The former studies from Turkey are either outdated4 or regional1–3 or from military hospitals5,11,12 and as a result can not provide current information about the whole SCI population in Turkey.
The current population of Turkey is approximately 80 million.13 Acording to the incidence rate given above, there are approximately 650–1700 new SCI cases in Turkey each year. The number of persons with SCI rehabilitated in our center each year, corresponds to 15–42% of the number of new cases in that period. But in fact there are also chronic SCI patients in that population. This situation is mainly originated from the health-care system in Turkey. In our country, all Turkish citizens have health coverage and all medical costs (including rehabilitation) are paid by government in any case of trauma/disease but patients are not directed to rehabilitation hospitals systematically. Persons with SCI admit to outpatient rehabilitation units on an individual basis after the primary care in surgical units. After their first time assessment by a physiatrist at the outpatient units, persons with SCI who are likely to benefit from rehabilitation are hospitalized. This gives way to delay in hospitalization for rehabilitation. Psychological, social and cultural factors associated with SCI in Turkey, such as poverty, limited education and low literacy, make rehabilitation access more difficult too. Combined with the low inpatient rehabilitation bed capacity, these factors give way to late rehabilitation access in Turkey and people are usually cared by a family member at home during the acute and subacute period. In addition to these, a small number of patients are also hospitalized for control of their orthosis and control urodynamic evaluation. So this study is not an incidence study, but instead a study reflecting the clinical and demographic characteristics of persons with SCI rehabilitated in the primary rehabilitation center in Turkey. As a result, this work may provide an insight to the general SCI population in Turkey.
Age and Sex
In previous studies from Turkey the mean age of persons with SCI ranged between 30.6 and 35.5.1–5 The avarage age of study population at the time of injury in our study was 38.3 years, up from the mean ages reported previously from Turkey.
Moreover when the age group distribution was investigated 13.35% of SCI population in our study were over 60 years old at the time of injury (Fig. 1). This ratio is also higher than the ratios reported in the former studies from Turkey, such as 6.4%,5 8.4%,12 8.7%4 and 4.45%.2 The mean age of persons with SCI is slowly increasing in the literature12,14 with a shift to higher SCI rates in the elderly population.16,17 The results of our study confirms that these findings are also true for Turkish population. New aging SCI population is most likely due to the increasing overall life expentancy in Turkey.13
Studies from all over the world show that males have a higher risk of SCI compared to females.15,18–20 Previous studies from Turkey reported male/female ratios between 2.5/1 and 3.38/1.2,4,5 The male to female ratio in our study was 2.31/1, lower compared to the former studies from Turkey. In fact there seems to be a lowering trend in this ratio worldwide over time.2,16,20 This may be due to socioeconomic changes and cultural development resulting in women being more integrated into the labor market. According to Gür2 and Pickett,16 however, this rate decline is due to the decrease in male persons not an increase in females. Further longitudinal studies are needed to explain the underlying reasons for the shift in male/female ratio.
Etiology
The overwhelming cause of SCI was MVA in the previous reports from Turkey.2,4,5 This information was also valid for other parts of the world.15,18,20 But as the population gets older, the ratio of falls among etiologic factors also increase.21 According to our results, 37.1% of the study population >60 years old were injured due to a fall. Our results were also in concordance with a recent study from Turkey by Güzelküçük et al.12 This study investigated SCI in older population, and reported that 32.8% of SCI were due to falls, much more than MVA in persons with SCI > 60 years old. Elderly people are more prone to falls because of vertigo and poor postural stability.22 In addition to this, falls related to occupational injury are also very common in our country,23 as reported in our study (more than 20% of falls from a height), and this also increases the percentage of falls as an etiologic factor.
In our study, for all causes of injury males outnumbered females except iatrogenic SCI. Moreover falls and MVAs are most common in 16–30 age group. Also mean age in diving accidents (19.4) and violence (29.5) are the lowest compared to mean ages in other etiologies. These findings are concordant with the previous studies.5,11
Level and severity of injury
Previously published reports from developed countries report that cervical lesions constitute the majority of SCI (50–75%),15,18,19,24 and C5 and C4 are the most common levels. Contrary to these findings our results showed only 26.3% of SCI were cervical but 46.2% were thoracic and 27.5% were lumbar. Our data showed L1 is the most common level followed by T12, L2 and then C4. These are similar with the previous studies from Turkey2,5,11 and other developing parts of the world.25 There is also a remarkable bimodal lesion level distribution with the most prominent peak between T12-L2 and the second most prominent peak between C4-C7 (Fig. 3). This is partly associated with the falls being the most common etiology of SCI from our referrals in Turkey. SCI due to falls predominately results in thoracic and lumbar lesions.5 Poor seat belt wearing habits may also be a significant contributing factor to the high incidence to thoracolumbar injuries. In underdeveloped or developing countries such as Turkey seat belt use is low, and this may result in increased mortality instead of cervical lesions in head-on passenger car collisions.26 AIS of the persons with SCI in our study were compatible with the other parts of the world, as the most common AIS was AIS A, followed by AIS D.15,18
Surgical intervention, associated lesions, length of rehabilitation stay and discharge destination
Vertebral fracture-dislocation ratio in our study (71.8%) is similar to literature.15 According to the literature from different parts of the world, surgical intervention is performed in 44.2–58.9% of SCIs,15,18,26 much lower compared to our results (89.6%). Another study from Turkey also correlates with our surgical intervention ratio too.11 It is worth investigating why SCI requires more surgery in Turkey. The rate of associated injuries is similar to studies from Turkey and other parts of the world.2,4,18
The mean LORS is 52.1 days in our study, in association with the new trends in rehabilitation. In the past, rehabilitation periods for SCI were much more longer,20 but over time LORS has diminished according to more developed surgical stabilization techniques and the lower complication rates such as severe infections/ pressure ulcers/sepsis, etc.5 According to our results motor complete SCI is associated with a longer LORS and this finding is in concordance with the literature.5,20 Furthermore persons with a shorter (<12 months) time since injury have a longer LORS, as in acute and subacute periods after SCI, functional loss is distinct and longer periods of rehabilitation is needed.
Most (90.8%) of the study population were discharged home. Although this ratio seems high,19,26 in our opinion it is partly due to relatively late time of rehabilitation phase according to the factors discussed above. So persons with SCI commonly have already passed the acute SCI period necessiating a nursing facilty at the time of discharge. Moreover there are only a few number of these kind of facilities, and they are not covered by public health insurance in Turkey. As a result, persons with SCI are mainly discharged home after rehabilitation in our center.
Conclusion
This study reflects the results of the persons with SCI rehabilitated at a single rehabilitation center in Turkey. At this rehabilitation center the mean age of SCI population is increasing, falls constitute the majority of etiologic factors and are more common after the age of 60. More than 20% of falls from a height, are related to occupational injury. Male-female ratio is decreasing and thoraco-lumbar injures are more common than cervical injuries. Although our sample does not reflect all of the new SCI population in Turkey, this data is pertinent since Turkey does not have a national SCI registry. These results also may help define public health initiatives, such as,policies protecting elderly from falls, diminishing work related injuries with priority to policies about road quality, vehicle safety, seat belt use and adherence to traffic rules. Moreover developing rehabilitation access (both by increasing bed availability and raising public awareness about rehabilitation) and nursing facilities that serve people after discharge from rehabilitation are additional public health concerns for persons with SCI in Turkey.
Disclaimer statements
Contributors None.
Funding None.
Conflict of Interest The authors declare no conflict of interest.
Ethics approval None.
ORCiD
Rabia Daylak http://orcid.org/0000-0001-5504-9424
References
- 1.Karamehmetoğlu SS, Ünal S, Karacan I, Yilmaz H, Tagay HS, Ertekin M, et al Traumatic spinal cord injuries in Istanbul, Turkey. An epidemiological study. Paraplegia 1995;33(8):469–71. [DOI] [PubMed] [Google Scholar]
- 2.Gür A, Kemaloğlu MS, Çevik R, Saraç JA, Nas K, Kapukaya A, et al Characteristics of traumatic spinal cord injuries in south-eastern Anatolia, Turkey: a comparative approach to 10 years’ experience. Int J Reh Res 2005;28(1):57–62. doi: 10.1097/00004356-200503000-00008 [DOI] [PubMed] [Google Scholar]
- 3.Karamehmetoğlu SS, Nas K, Karacan I, Sarac AJ, Kayun H, Ataoglu S, et al Traumatic spinal cord injuries in southeast Turkey. An epidemiological study. Spinal Cord 1997;35(8):531–3. doi: 10.1038/sj.sc.3100404 [DOI] [PubMed] [Google Scholar]
- 4.Karacan I, Koyuncu H, Pekel O, Sumbuloglu G, Kirnap M, Dursun H, et al Traumatic spinal cord injuries in Turkey: a nationwide epidemiological study. Spinal Cord 2000;38(11):697–701. doi: 10.1038/sj.sc.3101064 [DOI] [PubMed] [Google Scholar]
- 5.Tuğcu I, Tok F, Yılmaz B, Göktepe AS, Alaca R, Yazıcıoğlu K, et al Epidemiologic data of the patients with spinal cord injury: seven years’ experience of a single center. Ulus Travma Acil Cerrahi Derg 2011;17(6):533–38. doi: 10.5505/tjtes.2011.95676 [DOI] [PubMed] [Google Scholar]
- 6.DeVivo MJ, Biering-Sorensen F, New P, Chen Y.. Standardization of data analysis and reporting of results from the International Spinal Cord Injury Data Set. Spinal Cord 2011;49(5):596–9. doi: 10.1038/sc.2010.172 [DOI] [PubMed] [Google Scholar]
- 7.Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, et al International standarts for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med 2011;34(6):535–46. doi: 10.1179/204577211X13207446293695 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kirshblum S, Waring W 3rd. Updates for the international standards for neurological classification of spinal cord injury. Phys Med Rehabil Clin N Am 2014;25(3):505–17. doi: 10.1016/j.pmr.2014.04.001 [DOI] [PubMed] [Google Scholar]
- 9.Marino RJ, Barros T, Biering-Sorensen F, Burns SP, Donovan WH, Graves DE, et al International standards for neurological classification of spinal cord injury. J Spinal Cord Med 2003;26(Suppl 1):S50–56. doi: 10.1080/10790268.2003.11754575 [DOI] [PubMed] [Google Scholar]
- 10.Waring WP, Biering-Sorensen F, Burns S, Donovan W, Graves D, Jha A, et al 2009 review and revisions of the international standards for the neurological classification of spinal cord injury. J Spinal Cord Med 2010;33(4):346–52. doi: 10.1080/10790268.2010.11689712 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Güzelküçük Ü, Kesikburun S, Demir Y, Aras B, Özyörük E, Yılmaz B, et al Demographic and clinical characteristics of patients with traumatic cervical spinal cord injury: a Turkish hospital-based study. Spinal Cord 2015;53(6):441–5. doi: 10.1038/sc.2014.211 [DOI] [PubMed] [Google Scholar]
- 12.Güzelküçük Ü, Demir Y, Kesikburun S, Yaşar E, Yılmaz B.. Spinal cord injury in older population in Turkey. Spinal Cord 2014;52(11):850–4. doi: 10.1038/sc.2014.103 [DOI] [PubMed] [Google Scholar]
- 13.WorldOMeters Available at: www.worldometers.info/world-population/turkey-population/. Accessed 10 August 2016.
- 14.DeVivo MJ. Epidemiology of Traumatic spinal cord injury: trends and future implications. Spinal Cord 2012;50(5):365–72. doi: 10.1038/sc.2011.178 [DOI] [PubMed] [Google Scholar]
- 15.Pickett GE, Campos-Benitez M, Keller JL, Duggal N.. Epidemiology of traumatic spinal cord injury in Canada. Spine 2006;31(7):799–805. doi: 10.1097/01.brs.0000207258.80129.03 [DOI] [PubMed] [Google Scholar]
- 16.Pickett W, Simpson K, Walker J, Brison RJ.. Traumatic spinal cord injury in Ontario, Canada. J Trauma 2003;55(6):1070–6. doi: 10.1097/01.TA.0000034228.18541.D1 [DOI] [PubMed] [Google Scholar]
- 17.Sekhon LH, Fehlings MG.. Epidemiology, demographics, and pathophysiology of acute spinal cord injury. Spine 2001;26(24 Suppl):S2–12. doi: 10.1097/00007632-200112151-00002 [DOI] [PubMed] [Google Scholar]
- 18.O'Connor RJ, Murray PC.. Review of spinal cord injuries in Ireland. Spinal Cord 2006;44(7):445–8. doi: 10.1038/sj.sc.3101856 [DOI] [PubMed] [Google Scholar]
- 19.Couris CM , Guilcher SJ, Munce SE, Fung K, Craven BC, Verrier M, et al Characteristics of adults with incident traumatic spinal cord injury in Ontario, Canada. Spinal Cord 2010;48(1):39–44. doi: 10.1038/sc.2009.77 [DOI] [PubMed] [Google Scholar]
- 20.Biering-Sørensen E, Pedersen V, Clausen S.. Epidemiology of spinal cord lesions in Denmark. Paraplegia 1990;28(2):105–18. [DOI] [PubMed] [Google Scholar]
- 21.Chen Y, Tang Y, Vogel LC, DeVivo MJ.. Causes of spinal cord injury. Top Spinal Cord Inj Rehabil 2013;19(1):1–8. doi: 10.1310/sci1901-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Tuunainen E, Rasku J, Jantii P, Pyykkö I.. Risk factors of falls in community dwelling active elderly. Auris nasus Larynx 2014;41(1):10–6. doi: 10.1016/j.anl.2013.05.002 [DOI] [PubMed] [Google Scholar]
- 23.Celik K, Yılmaz F, Kavalcı C, Özlem M, Demir A, Durdu T, et al Occupational injury patterns of Turkey. World J Emerg Surg 2013;8(1):57. doi: 10.1186/1749-7922-8-57 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Gjone R, Nordlie L.. Incidence of traumatic paraplegia and tetraplegia in Norway: a statistical survey of the years 1974 and 1975. Paraplegia 1978;6(1):88–93. [DOI] [PubMed] [Google Scholar]
- 25.Chiu WT, Lin HC, Lam C, Chu SF, Chiang YH, Tsai SH.. Review paper: epidemiology of traumatic spinal cord injury: comparisons between developed and developing countries. Asia Pac J Public Health 2010;22(1):9–18. doi: 10.1177/1010539509355470 [DOI] [PubMed] [Google Scholar]
- 26.van Asbeck FW, Post MW, Pangalila RF.. An epidemiological description of spinal cord injuries in The Netherlands in 1994. Spinal Cord 2000;38(7):420–4. doi: 10.1038/sj.sc.3101003 [DOI] [PubMed] [Google Scholar]