

Abstract
Vitamin D-dependent rickets type II is a rare hereditary disorder. It occurs due to mutations in the gene chr. 12q12-q14, which codes for vitamin D receptor. End-organ resistance to 1,25-(OH)2 vitamin D3 and alopecia in severe cases are the characteristic features. We report a case of a 4-year-old boy with loss of hair over the scalp and body – first observed after 1 month of birth. The boy also developed difficulty in walking at the age of 2 year. On analysis, reduced serum calcium level (7.5 mg/dL) and elevated alkaline phosphatase level (625 IU/L) were reported. Initially, the treatment included intramuscularly administered single dose of 600,000 IU vitamin D, followed by 400 IU of vitamin D along with 1 g of supplemental calcium every day. Periodic follow-up was conducted for 2 months. Improvement was observed in the biochemical parameters and X-rays of the distal radial and ulnar metaphyses, although no improvement was observed in alopecia.
Keywords: Alopecia, hereditary, rickets, vitamin D treatment, vitamin D-dependent rickets type II
What was known?
Vitamin D-dependent rickets type II is a hereditary autosomal recessive disorder. It presents as rachitic changes due to mutations in the vitamin D receptor gene.
Introduction
Vitamin D-dependent rickets (VDDR) type II, also known as hereditary vitamin D-resistant rickets type II, is a hereditary autosomal recessive disorder. It is caused due to the mutations of the gene chr. 12q12-q14, which codes for vitamin D receptor (VDR). The characteristic features are end-organ resistance to 1,25-(OH)2 vitamin D3 and alopecia in severe cases. VDDR type II causes rachitic changes that are not responsive to vitamin D treatment. Alopecia along with VDDR type II is observed in severe cases.[1,2]
Case Report
A 4-year-old boy presented with loss of hair on the scalp and body, first observed after 1 month of birth. Difficulty in walking was observed at the age of 2 year. Although second-degree consanguinity among parents was present, the abnormality was not detected among parents and the elder sibling.
Clinical presentation and diagnosis
On clinical examination, typical features of VDDR type II associated with alopecia were observed including loss of hair on the scalp, eyelids, and the entire body. However, few terminal hairs were present over the vertex and upper eyelids [Figures 1 and 2]. He had features of rickets including bowing of legs (genu varum; Figure 3), widened wrist [Figure 4], frontal bossing, and rachitic rosary [Figure 5]. The anterior fontanelle was not closed and clinically showed hypoplastic anterior teeth along with signs of exposure of pulp [Figure 6]. Based on the clinical observations, VDDR type II with alopecia was suspected and further investigations were performed.
Figure 1.

Loss of hair over the scalp (few terminal hairs present over the vertex and upper eyelids)
Figure 2.

Loss of hair all over the body
Figure 3.

Bowing of legs (genu varum)
Figure 4.

Widened wrist
Figure 5.

Rachitic rosary
Figure 6.

Hypoplastic anterior teeth along with signs of exposure of pulp
On investigations, hypocalcemia (serum calcium levels: 7.5 mg/dL; reference range: 8.5–10.2 mg/dL) and increased alkaline phosphatase level (625 IU/L; reference range: 50–155 IU/L) were observed. Renal function test was within normal limits. However, due to financial constraints of the patient, 1,25(OH)2D and parathyroid hormone levels were not assessed. Anteroposterior X-ray of the bilateral wrist showed metaphyseal fraying, flaying, and cupping of the distal radius and ulna [Figure 7]. Skin biopsy from alopecic patch showed reduced number of follicles and increased number of miniaturized follicles throughout mid-dermis without inflammatory cell infiltration, along with lack of hair shafts in the hair follicles [Figure 8].
Figure 7.

Metaphyseal fraying, flaying, and cupping of the distal radius and ulna
Figure 8.
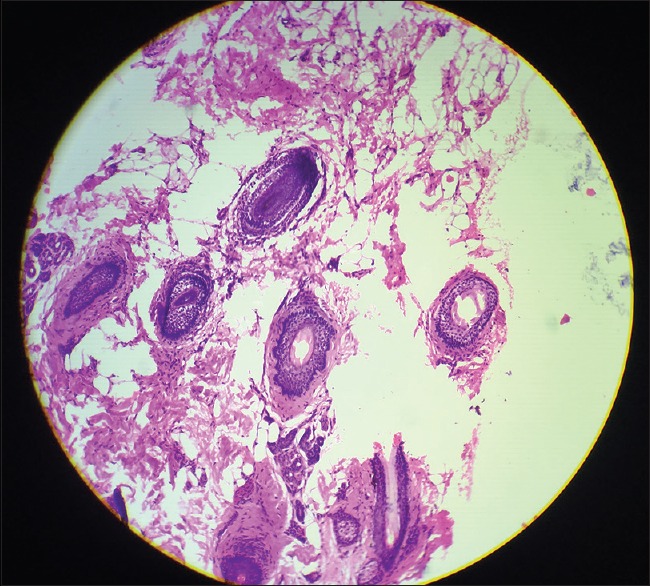
Horizontally sectioned scalp biopsy showing lack of hair shafts in some of the hair follicles with absent lymphocytic infiltration (H and E, ×100)
Treatment and follow-up
The treatment involved the administration of high doses of calcium and vitamin D. Initially, the treatment included a single dose of intramuscularly administered vitamin D (600,000 IU), followed by 400 IU of vitamin D along with 1 g of supplemental calcium every day. The patient was followed up for 2 months. Improvement was observed in the biochemical parameters and the X-rays of the distal radial and ulnar metaphyses; however, no improvement was observed in alopecia. Due to financial constraints, the patient could not attend further follow-up sessions. The patient was advised to continue the treatment schedule until improvements were observed.
Discussion
The present case is one of the few VDDR type II associated with alopecia cases reported in India. The prevalence of VDDR was approximately 30% two decades ago; however, in the present time, it has reduced to 0.8%. The clinical presentations include weak bones causing bone pain, delayed growth, short stature, and bowed legs due to impaired weight bearing capacity of weakened legs. The syndrome usually presents with these symptoms and is also associated with alopecia in severe cases.[3] In VDDR, the serum calcium levels are either normal or low along with elevated alkaline phosphatase level and low serum phosphorus levels. The diagnostic hallmark of VDDR type II is the increased serum levels of 1,25-dihydroxyvitamin D3 due to the mutations of VDR gene. The mutations alter the absorption of calcium and phosphate resulting in hypocalcemia and hypophosphatemia, leading to VDDR type II and deranged vitamin D activity in other organs.[4]
Vitamin D is essential for bone growth, mineralization, and absorption of calcium and phosphate, which is deficient in rickets.[2] Vitamin D is obtained by dietary intestinal absorption and through the skin and is available as vitamin D2 and vitamin D3. Initially, in the liver, vitamin D is hydroxylated to 25-hydroxyvitamin D3 (25-OHD3). Later, 25-OHD3 bound to the vitamin-binding protein is transported to the kidney, where it undergoes hydroxylation to form the hormonally active metabolite, 1,25-dihydroxyvitamin D3 (1,25-OH2D3).[5] The tissue receptors for vitamin D metabolites are localized in various organs, including kidney, intestine, pancreas, parathyroid gland, muscle, pituitary, skin, and bones and 1,25-OH2D3 binds specifically to a receptor in the nuclei to stimulate calcium transport and also controls the expression of target genes mediated through the nuclear VDR. Mutations of the VDR gene lead to VDDR type II.[6]
Mutations of the VDR gene also suppress specific genes during the hair cycle, resulting in their alteration. The protein by-products formed during the mutation disrupt the hair cycle leading to alopecia.[6] The absence of ligand-independent function of the VDR in keratinocytes, required for anagen initiation, is hypothesized to be the reason of alopecia. The alopecia usually starts at birth and ends at childhood. The extent of alopecia ranges from decreased hair on the body parts including eyebrows, eyelashes, and body hair (alopecia areata/partial alopecia) to complete hair loss over the body (alopecia totalis/complete alopecia).[3]
VDDR type II is usually resistant to normal doses of vitamin D treatment; therefore, massive doses of 1,25-dihydroxyvitamin D are recommended although varying results are seen.[7] In literature, many studies have reported VDDR type II with partial alopecia; however, one case of VDDR type II with total alopecia was reported by Stojanov.[3] In a case report by Takeda et al., improvement was observed in two siblings with VDDR type II associated with alopecia. The treatment included 50,000 IU of vitamin D2. The treatment was continued for 2 years, and no recurrence was observed 14 years after cessation of therapy.[8] Similarly, Lin and Uttley observed improvement in a 8-year-old girl with VDDR type II, who was treated with oral calcium supplements.[9] According to animal model of hereditary VDDR type II conducted by Li et al., VDDR plays an important role in the hair cycle rather than in the primary hair growth.[10] In India, only few cases of VDDR type II with alopecia have been reported. A case of VDDR type II with alopecia in a 2-year-old child was reported by Murali and Usharani.[7]
The present study suggested that continuous treatment with large doses of vitamin D is valuable in treating VDDR type II associated with alopecia. Further, awareness of clinicians is required to determine VDDR type II when a patient presents with rickets along with alopecia.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
What is new?
VDDR type associated with alopecia is rare; however, it can be treated with supplemental calcium and large doses of vitamin D. Cases presenting with rickets along with alopecia should be further evaluated for VDDR type II.
Acknowledgments
All authors contributed equally in the development of the manuscript.
References
- 1.Shafeghati Y, Momenin N, Esfahani T, Reyniers E, Wuyts W. Vitamin D-dependent rickets type II: Report of a novel mutation in the Vitamin D receptor gene. Arch Iran Med. 2008;11:330–4. [PubMed] [Google Scholar]
- 2.Sahay M, Sahay R. Rickets-Vitamin D deficiency and dependency. Indian J Endocrinol Metab. 2012;16:164–76. doi: 10.4103/2230-8210.93732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Azemi M, Berisha M, Ismaili-Jaha V, Kolgeci S, Hoxha R, Grajçevci-Uka V, et al. Vitamin D – Dependent rickets, type II case report. Mater Sociomed. 2014;26:68–70. doi: 10.5455/msm.2014.26.68-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Feldman D, Malloy PJ. Mutations in the Vitamin D receptor and hereditary Vitamin D-resistant rickets. Bone Key Reports. 2014:3. doi: 10.1038/bonekey.2014.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Christakos S, Ajibade DV, Dhawan P, Fechner AJ, Mady LJ. Vitamin D: Metabolism. Rheum Dis Clin North Am. 2012;38:1–11, vii. doi: 10.1016/j.rdc.2012.03.003. [DOI] [PubMed] [Google Scholar]
- 6.Malla KK, Malla T, Shaw C, Thapalial A. Type II Vitamin D dependent rickets: A case report. J Nepal Paediatr Soc. 2010;30:46–9. [Google Scholar]
- 7.Murali MV, Usharani T. Vitamin D dependent rickets type II with alopecia. J Life Sci. 2013;5:57–9. [Google Scholar]
- 8.Takeda E, Yokota I, Kawakami I, Hashimoto T, Kuroda Y, Arase S, et al. Two siblings with Vitamin-D-dependent rickets type II: No recurrence of rickets for 14 years after cessation of therapy. Eur J Pediatr. 1989;149:54–7. doi: 10.1007/BF02024336. [DOI] [PubMed] [Google Scholar]
- 9.Lin JP, Uttley WS. Intra-atrial calcium infusions, growth, and development in end organ resistance to Vitamin D. Arch Dis Child. 1993;69:689–92. doi: 10.1136/adc.69.6.689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Li YC, Pirro AE, Amling M, Delling G, Baron R, Bronson R, et al. Targeted ablation of the Vitamin D receptor: An animal model of Vitamin D-dependent rickets type II with alopecia. Proc Natl Acad Sci U S A. 1997;94:9831–5. doi: 10.1073/pnas.94.18.9831. [DOI] [PMC free article] [PubMed] [Google Scholar]