

Abstract
BACKGROUND:
Mortality and disability rates were reported to be respectively 2-3 and 5-10 times higher in C-sections compared to Vaginal delivery.
OBJECTIVES:
This study was aimed to explore the factors involved in selecting the birth type among primiparous women.
METHODS:
The present cross-sectional research was conducted on 220 primiparous women, who visited the health-care centers of Bandar Abbas. They were recruited in their first trimester of pregnancy with a simple randomized clustering method. Data were collected in a researcher-designed questionnaire. Its validity was confirmed by a panel of experts and reliability was tested and approved through the test–retest method. Mean, standard deviation, independent sample t-test, and Chi-squared tests for data analysis were done by SPSS 16. P < 0.05 was considered statistically significant.
RESULTS:
The mean age of the participants was 27.40 ± 6.07 years. The main barriers to the choice of vaginal delivery were the fear of pain and fear of vaginal area tears and ruptures, fear of injury to fetus, and doctor's recommendation. A statistically significant correlation was observed between the age, education, employment, income, awareness, and the reasons for preferring surgical childbirth.
CONCLUSIONS:
To reduce the rate of unnecessary cesarean sections (C-section), the following recommendations are suggested: Reducing fear of pain in expectant mothers, modifying wrong beliefs about the culture of natural childbirth, increasing awareness of fewer adverse effects of vaginal delivery including the vaginal tears if the mother abides by all midwife(s) instructions during the delivery procedure, providing educational courses for the necessary movements during the delivery, decreasing surgeons’ payment for C-section, and increasing payment for natural childbirth and implementing barriers for optional delivery to reduce the C-section.
Keywords: Birth type, cesarean section, Iran, primiparous women, vaginal delivery
Introduction
Natural childbirth is the preferred type of childbirth and cesarean section (C-section) should be limited, according to rules and regulations, to the cases which have no chance of natural childbirth, or it is accompanied by severe threat to mother's or infant's life.[1] Surgical childbirth is recommended, when either mother's or fetus’ health is at risk. However, there has been an ever-growing rate of cesarean for nonemergent cases.[2,3] The rate of C-section has an immense variation globally and has constantly increased. It has raised from 6.7% in 1990 to 19.1% in 2014.[4] The rate of C-section in Iran has been increasing within the past three decades. The rate of C-section in 1976 was 19.5% in Iran, which reached 24% in the mid-90s.[5] In 2010, this rate, according to the multifaceted health and population index reached 45.5%.[6] In 2013, Iran had 54% of C-section and ranked the second among countries with C-section in the world which shows an undesirable state.[7] Therefore, in countries, where the prevalence of cesarean is 20%–30%, many attempts have been made to reduce it. In other countries, the prevalence of this type of childbirth is maximally one-fourth.[8] Cesarean is accompanied by undesired consequences for mother's and child's health. The mortality rate of cesarean is about 2–3 times as high as natural childbirth, and the rate of induced disability is 5–10 times as high. The main reasons for the mortality induced by cesarean are uterine infection, hemorrhage, urinary system infection, and thromboembolisms.[9] On the other hand, recent research has shown that cesarean reduces reproductive power and preterm birth weight.[10] Special attempts should be made to reduce the rate of C-section. It seems logical to delve into the factors involved in selecting the surgical type of childbirth to arrange the suitable strategies to reduce this rate. Although recently many researches have been conducted on C-section and its underlying factors, it still requires further investigation for several reasons. The majority of related research in Iran has focused on the prevalence of C-section, women's tendency toward delivery, pregnant women's awareness and attitude toward the type of delivery, and the correlation of several factors with the type of delivery. Limited research has attempted to determine the factors involved in the selected type of delivery. The results of this limited body of research have been divergent for several reasons: different instrumentation, demographic features of the target women population, cultural, psychological, and social differences of the women participants. Therefore, the factors involved in women's decision to select the delivery type needs to be investigated region by region. Then, the design of conducted research will be able to show the factors affecting women's decision to select the type of childbirth. Thus, the present research was aimed to investigate the key factors involved in primiparous women's choice of the type of delivery.
Objectives
Current research was conducted among the primiparous women in Bandar Abbas, and the results are hoped to help planning to prepare mother to welcome natural childbirth and decrease the rate of cesarean.
Methods
Study design and participants
This descriptive/analytical research was designed as a cross-sectional study. The setting was comprised of all primiparous women who visited the health-care centers of Bandar Abbas in their 3rd month of pregnancy. The sample size was calculated 220 (coefficient = 0.25, test power = 0.8, and confidence interval = 0.95). The sampling method was a combination of the simple randomization and clustering. Initially, 8 clusters were randomly selected from all the health-care centers in Bandar Abbas. Once mothers’ medical files were studied, those who met the inclusion criteria were selected through a simple randomization and were invited to take part in the research. The inclusion criteria were age range of 18–35 years, height above 145 cm, weight range of 50–90 kg, primiparity, pregnancy age of 28 weeks or more, and consent to participate. Exclusion criteria were placental problems, diagnosis with multiple pregnancy, immature pelvis, pregnancy diabetes, history of hypertension, and pregnancy poisoning. Informed written consent was obtained from all the participants (as there were no illiterate participants in this study). This study was approved by Hormozgan University of Medical Sciences Ethics Board.
Instruments
The data were collected by a researcher-designed questionnaire and was comprised of four sections. The first section contained demographic information (mother's individual, social, and midwifery items) and consisted of eight items overall. The second section with 20 items enquired awareness about the advantages and disadvantages of each delivery type (the first 15 items were four-choice and the last 5 was three-choice). This section was to be scored between 0 and 20. The awareness was finally scored between 0 and 8 and interpreted as low between 8 and 15 as moderate, and between 15 and 20 interpreted as high awareness. The third section included 12 items on a Likert scale (totally agree, agree, no comment, disagree, and totally disagree) that enquired about women's agreement or disagreement with the C-section (Questions such as C-section is accompanied by the risk of the adhesion of abdominal organs). The underlying reason for choice of C-section consisted of 12 items rated. The fourth section had only one item, which about the behavioral intention construct in the theory of logical action (natural and surgical types of childbirth). To test the content validity of the questionnaire, it was availed to a panel of ten experts. They were asked to evaluate the items in terms of the legibility, difficulty, and comprehensibility. The required adaptations were accordingly made to the questionnaire. To test the reliability of the test, the test–retest method was followed in a pilot test, which took a period of 3 weeks. The questionnaire was provided to participants similar to the real research participants in two periods and at a time interval of ten days. and then, Cronbach's alpha was estimated as the correlation coefficient of internal consistency. It was estimated at 88 and thus the reliability of the test was confirmed.
Procedures and ethical considerations
Once the required permissions were approved by the deputy of research at the target university, the participants were familiarized with the purpose of the research and were ensured of the confidentiality of the information they produced. They were allowed to leave the study anytime they chose to.
Data analysis
Once the data were collected, they entered SPSS ver. 16 (IBM Company, Armonk, NY, USA) for statistical analyses and were described through mean and standard deviation. T-test and Chi-squared test were used to analyze the data. The significance level was set at P < 0.05
Results
The mean age of the research participants was 27.40 ± 6.07 and the mean age of marriage was estimated at 23.40 ± 5.20 years.
The present findings revealed a statistically significant correlation between the age and choice of birth type (P = 0.014). Those below 20 years of the age showed a tendency toward C-section. No statistically significant correlation was found between spouse's education, accommodation, and the birth type (P > 0.05) [Table 1].
Table 1.
Correlation of demographic information and the birth type
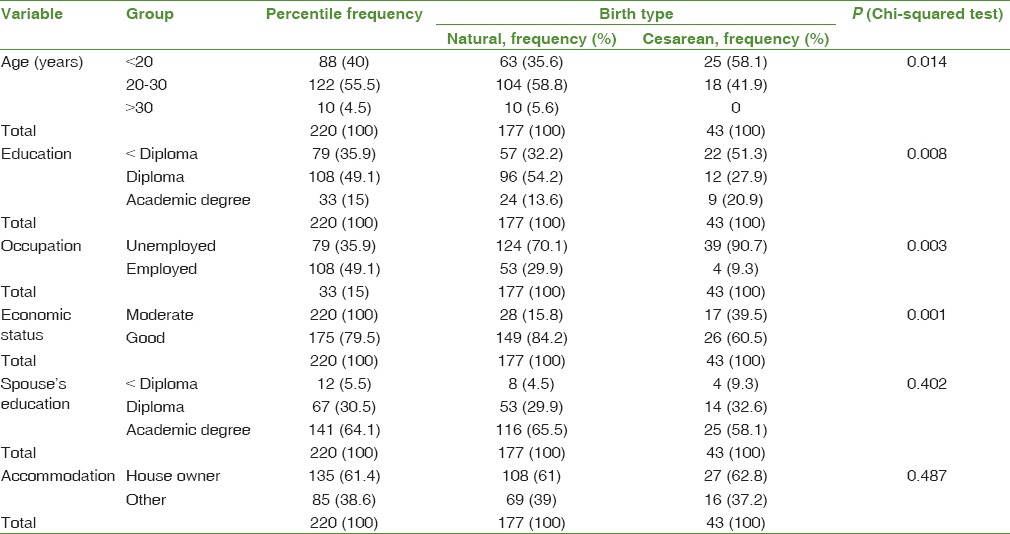
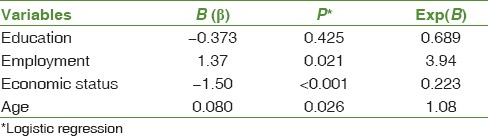
The age, education, income, and occupation entered the logistic model. The test results revealed that the occupation variable (odds ratio [OR] = 3.94) and only then the age (OR = 1.08) were the strongest predictors of the choice of natural childbirth. Accordingly, those of lower education level, the unemployed and those of low income as well as older women selected natural childbirth more [Table 2].
Table 2.
Factors predictive of vaginal delivery, according to the study variables
According to the findings, the choice of birth type and awareness were significantly correlated (P < 0.001). The highest level of awareness showed appeared among those willing to have a natural childbirth [Figure 1].
Figure 1.
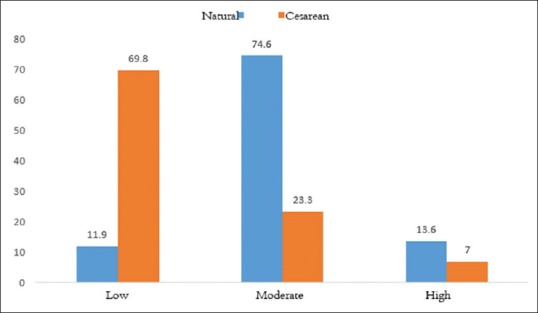
Levels of awareness of the birth type among primiparous women
The primary reasons showed to be the fear of pain, fear of vaginal tearing, and fear of altering fetus’ health [Figure 2].
Figure 2.
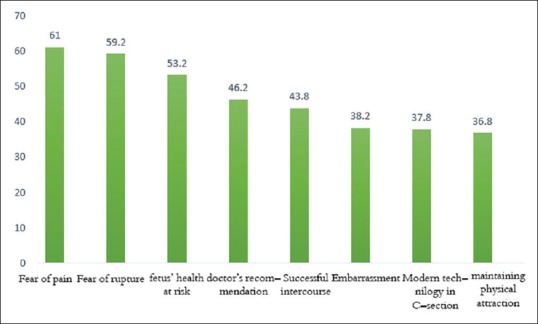
Key factors involved in cesarean-section preference (n = 43)
Discussion
A number of factors involved in selecting the birth type were investigated among primiparous women in Bandar Abbas. A statistically significant correlation was found between preferring natural childbirth and awareness. Women with higher awareness showed to prefer natural childbirth more. In a number of studies, mother's awareness was reported as the key factor involved in going for natural abortion.[11,12] In a systematic review, Alimohammadzadeh et al. found that the majority of researcher had suggested raising women's awareness about the hazards of C-section and the advantages of natural childbirth.[8] In some other research, women's unawareness was considered as the main factor involved in preferring cesarean as among all social and cultural issues.[13] Therefore, it seems essential for health authorities to increase mothers’ awareness and help to reduce the rate of cesarean delivery.
In the present research, the highest percentage of preferring cesarean delivery was because of the fear of pain in natural childbirth, fear of tears in the genital tract including the vagina, fear of altered fetus’ health, and finally doctor's recommendation. Ghadimi et al., mentioned in their research, concerns about fetus’ health, fear of pain, and ruptures[14] as the main reasons of avoiding natural childbirth. Similarly, Saisto and Halmesmäki maintained that fetus’ health, fear of pain, and ruptures were the primary reasons for preferring cesarean delivery.[15] The above-mentioned research findings all confirm the present findings. It appears that one reason, why the fear of pain ranked first among the factors explored in the present study was that all participants were primiparous women. Similarly, Abad indicated that primiparous women were more afraid of natural childbirth than those with an experience of prior delivery.[16] On the other hand, mother's fear can stem from their lack of awareness about or facilities of natural childbirth. Empowering women to overcome the fear of natural childbirth seems to be capable of reducing the rate of unessential cesarean.
Another factor involved in preferring C-section turned out to be doctor's recommendation. In their research, Bani et al. indicated that a doctor is a main source of inspiration for mothers and families and plays a major role in persuading patients toward a certain type of delivery.[17] Azizi and Salari showed that financial reasons and doctor's priority were among the main reasons involved in the high rate of cesarean delivery.[18] Doctors seem to be motivated by financial reasons on the one hand and tend to avoid prospective complaints and choose the more conservative way, that is, a C-section as it is associated with fewer hazards for both mother and child. It, thus, appears that the presence of a monitoring system to evaluate the indications of natural and C-section deliveries can manage to reduce the rate of unessential C-section to a certain degree.
A significant negative correlation was found between age and preference of natural childbirth. Those of a younger age showed to tend more toward a C-section, which was consistent with the finding reported by Tabandeh and Kashani.[19] Unlike the present findings, Ghadimi et al. found that mother's higher age was the main reason, why they preferred a C-section.[2] Zasloff et al. noticed that mother's higher age and multiple pregnancies were associated with their less fear of natural childbirth.[20] The present findings were not consistent with those reported by Eynsheykh et al.,[21] Bushehr et al.,[9] Mohammadbeygi et al.,[22] and Gould et al.[23] These divergences can be explained by younger mothers’ inadequate awareness, experience, and sensitivity to the side effects of a cesarean.[24] On the other hand, it seems that education and raising women's awareness of the disadvantages of cesarean and advantages of natural childbirth is essential in all age groups.
The present findings revealed a statistically significant correlation between education and the choice of birth type. Those of a lower education level showed to preferred cesarean more than others. In their research in Sweden, Karlström et al. reported similar results.[25] The present findings were not in line with those reported by Alimohamadian et al.,[26] Ziaghm et al.,[27] and Leone et al.[28] No significant correlation was found between education and the choice of birth type in a body of research by Eynsheykh et al.,[21] Vafaee et al.,[29] and Chong and Mongelli.[30] Since in the present research, mothers’ lower education showed to be correlated with a preference of a C-section, it can be concluded that those with a lower education had less awareness and knowledge of the side effects of a C-section. Moreover, the slight divergences between the present findings and other investigations can be due to different social, cultural, and geographical differences.
In this research, a statistically significant correlation was found between occupation and the preference of the birth type. The employed showed less tendency toward a C-section. This finding was consistent with that of Garmaroudi et al.[31] To the contrary, Ghahfarokhi et al.[32] found no effect of mother's employment on preferring a C-section. This finding was not consistent with that of Eynsheykh et al.[21] It appears that employed women may be exposed to information, which can raise their awareness of the disadvantages of C-section. This divergence can be explained by social and geographical differences of the research populations.
The present research found a significant correlation between income and the preference for a certain birth type. Those with a higher income showed a more tendency toward a C-section. This was in line with what Mohammadi et al.[33] reported along with a research in Brazil and Chile,[34] Leone et al.,[28] Garmaroudi et al.,[31] and Klemetti et al.[35] High economic status seems to create more tendency to modern symbols. C-section is considered as a symbol of high social status and dignity while natural childbirth is taken as that of low social status. Therefore, the existence of such attitude in society inhibits all attempts to reduce the rate of cesarean to a great extent.
Among the limitations of the present research were incomplete questionnaires and missing data, exclusion of rural participants, mere primiparity, and exclusion of multiple pregnancies. In the light of the present findings, a number of suggestions can be made. Increasing mothers’ awareness about the side effects of cesarean delivery and the advantages of natural childbirth by the medical and midwifery staff can contribute to reducing the rate of unnecessary C-sections. Using physiological delivery methods as well as ways to reduce pain, high-tech facilities in the delivery room can all help to cut down on the rate of C-section. One of these facilities, which can be very helpful, is the presence of a companion in the delivery room.
Conclusions
The present findings revealed that the key factors involved in preferring a C-section are the fear of pain involved in natural childbirth, avoiding vaginal tears, fetus’ health, and doctor's recommendation. Considering the factors involved in choosing the birth type, a number of actions can be taken to reduce the rate of unemergent C-section. These include empowering mothers to overcome the fear of pain and get familiarized with the advantages of natural childbirth and disadvantages of a C-section through mass media and medics themselves. Planning to persuade primiparous women toward natural childbirth can affect the trend of childbirth in the near future and can prevent the rate of unnecessary cesarean surgeries.
Financial support and sponsorship
This study was financially supported by Hormozgan University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank Hormozgan University of Medical Sciences, Bandar Abbas, Iran and also Center for Development of Clinical Research of Shahid Mohammad Hospital.
References
- 1.Ebrahimipour S, Nakhaee N. The obstacles of choosing vaginal delivery and policies to increase it from the point of view of gynecologists and midwives. J Health Dev. 2016;5:71–8. [Google Scholar]
- 2.Safari-Moradabadi A, Mehraban M, Alavi A, Pormehr-Yabandeh A, Ghiaspour T, Dadipoor S. Investigating the delivery type among primiparous women in Bandar Abbas according to the health belief model. Middle East J Fam Med. 2018;7(10):121. [Google Scholar]
- 3.Safari Moradabadi A, Alavi A, Eqbal Eftekhaari T, Dadipoor S. The reproductive behavior of families with thalassemic children in hormozgan. J Reprod Infertil. 2015;16:167–70. [PMC free article] [PubMed] [Google Scholar]
- 4.Dadipoor S, Alavi A, Safari-Moradabadi A. A survey of the growing trend of caesarian section in Iran and the world: A review article. Iran J Obstet Gynecol Infertil. 2016;19:8–17. [Google Scholar]
- 5.Dadipoor S, Aghamolaei T, Ramezankhani A, Safari-Moradabadi A. Comparison of health belief model constructs according to birth type by nulliparous pregnant women in bandar abbas. J Educ Community Health. 2017;4:65–71. [Google Scholar]
- 6.Safari Moradabadi A, Hassani L, Ghanbarnejad A, Madani A, Rajaei I, Dadipoor S. The effect of education on knowledge and preferred method of delivery in nulliparous women. J Health Care. 2014;16:74–83. [Google Scholar]
- 7.Zarei E, Majidi S, Bay V. Achievement of health sector evolution objectives in the vaginal delivery promotion plan: A study in a large public hospital in Tehran. J Health Field. 2017;3:27–32. [Google Scholar]
- 8.Alimohammadzadeh K, Mohebi S, Labaf T. Systematic review of research papers in the recent three decades on the” reasons of cesarean section” and population health management strategies in Iran. Womens Strateg Stud. 2013;16:8–57. [Google Scholar]
- 9.Bushehr IH, Bushehr IG, Committee SR, Committee SR. Assessing the Factors Influencing Delivery Method Selection in Pregnant Women Referred to Public Hospitals in Shirazr. 2014 [Google Scholar]
- 10.Boskabadi H, Zakerihamidi M, Bagheri F. Outcomes of vaginal delivery and cesarean in Mashhad Ghaem University Hospital. Tehran Univ Med J TUMS Publ. 2014;71:807–15. [Google Scholar]
- 11.Dadipoor S, Safari Moradabadi A, Esmaeelion F, Eghbal Eftekhaari T, Alavi A, Fallahi S, et al. Prevalence of legal abortions and correlated causes in a central women's hospital in South of Iran (2009-2012) Life Sci J. 2013;10(12s):91–4. [Google Scholar]
- 12.Faraji Darkhaneh R, Zahiri Sooroori Z, Farjad Bastani F. A survey of knowledge and attitude of pregnant women about delivery methods. J Guilan Univ Med Sci. 2003;12:69–75. [Google Scholar]
- 13.Bick D. National Collaborating Centre for Women's and Children's Health, National Institute for Clinical Excellence. Caesarean section. Clinical guideline. National collaborating centre for women's and children's health: Commissioned by the national institute for clinical excellence. Worldviews Evid Based Nurs. 2004;1:198–9. doi: 10.1111/j.1524-475X.2004.04060.x. [DOI] [PubMed] [Google Scholar]
- 14.Ghadimi M, Rasouli M, Motahar S, Lajevardi Z, Imani A, Chobsaz A, et al. Affecting factors the choice of delivery and attitude of pregnant women admitted to the civil hospitals, the Social Security Organization in 2013. J Sabzevar Univ Med Sci. 2014;21:310–9. [Google Scholar]
- 15.Saisto T, Halmesmäki E. Fear of childbirth: A neglected dilemma. Acta Obstet Gynecol Scand. 2003;82:201–8. [PubMed] [Google Scholar]
- 16.Abad M. Elective Caesarean; Ethical or non-Ethical a Approach? Medical Ethics Journal. 2016;3(8):103–25. [Google Scholar]
- 17.Bani S, Seyedrasooli E, Shams GT, Ghoojazadeh M, Hassanpoor S. Preference of delivery attendants regarding mode of delivery for themselves and pregnant women. Payesh. 2012;11:629–35. [Google Scholar]
- 18.Azizi M, Salari P. Ethical approach in cesarean delivery by maternal request. Iran J Med Ethics Hist Med. 2009;2:55–66. [Google Scholar]
- 19.Tabandeh A, Kashani E. The prevalence of cesarean among employed educated women of medical science groups in Gorgan, 2005. J Gorgan Univ Med Sci. 2007;9:67–70. [Google Scholar]
- 20.Zasloff E, Schytt E, Waldenström U. First time mothers’ pregnancy and birth experiences varying by age. Acta Obstet Gynecol Scand. 2007;86:1328–36. doi: 10.1080/00016340701657209. [DOI] [PubMed] [Google Scholar]
- 21.Eynsheykh ZD, Shaahmadi F, Taslimi S, Emamiureh F, Moeinaldini S. Investigating the relationship between demographic factors and choice of delivery method in pregnant women in the city of Savojbolagh. J Family Reprod Health. 2013;7:35–8. [PMC free article] [PubMed] [Google Scholar]
- 22.Mohammadbeygi A, Tabatabaei S, Mohammad SN, Yazdani M. Factors influencing cesarean delivery method in Shiraz hospitals. Iran J Nurs. 2009;21:37–45. [Google Scholar]
- 23.Gould JB, Davey B, Stafford RS. Socioeconomic differences in rates of cesarean section. N Engl J Med. 1989;321:233–9. doi: 10.1056/NEJM198907273210406. [DOI] [PubMed] [Google Scholar]
- 24.Reza Soltani P, Hosseinjani A, Etebari S. Causes of cesarean section performed in an educational health care center. J Holist Nurs Midwifery. 2012;22:16–22. [Google Scholar]
- 25.Karlström A, Rådestad I, Eriksson C, Rubertsson C, Nystedt A, Hildingsson I. Cesarean section without medical reason, 1997 to 2006: A Swedish register study. Birth. 2010;37:11–20. doi: 10.1111/j.1523-536X.2009.00373.x. [DOI] [PubMed] [Google Scholar]
- 26.Alimohamadian M, Shariat M, Mahmoodi M, Ramezanzadeh F. The influence of maternal request on the elective cesarean section rate in maternity hospitals in Tehran. Iran Payesh. 2003;2:133–9. [Google Scholar]
- 27.Ziaghm S, Bakhshandeh Bavarsad M, Haghighi S, Sayhi M, Zargar-Natage M, Abadian S. Assessment of educational needs in pregnancy to choose the mode of delivery for nulliparous women. Nurs Dev Health Aligoodarz Nurs Faculty Analytic Res J. 2014;3:31–40. [Google Scholar]
- 28.Leone T, Padmadas SS, Matthews Z. Community factors affecting rising caesarean section rates in developing countries: An analysis of six countries. Soc Sci Med. 2008;67:1236–46. doi: 10.1016/j.socscimed.2008.06.032. [DOI] [PubMed] [Google Scholar]
- 29.Vafaee R, Hosseini F, Dashdebi K, Momen Bellah Fard MJ, Ghalandari M, Gharlipour Z, et al. Assessing the factors influencing delivery method selection in pregnant women referred to public hospitals in Shirazr. J Nurs Midwifery. 2013;81:13–8. [Google Scholar]
- 30.Chong ES, Mongelli M. Attitudes of Singapore women toward cesarean and vaginal deliveries. Int J Gynaecol Obstet. 2003;80:189–94. doi: 10.1016/s0020-7292(02)00391-0. [DOI] [PubMed] [Google Scholar]
- 31.Garmaroudi G, Eftekhar H, Batebi A. Study of risk factors for cesarean section in pregnant women. Payesh. 2012;1:45–9. [Google Scholar]
- 32.Ghahfarokhi Z, Khalajabadi F, Saraei H. Determinants of intention for cesarean section vs. normal delivery among pregnant women in Esfahan. J Popul Assoc Iran. 2016;9:199–224. [Google Scholar]
- 33.Mohammadi TS, Kiani AA, Heydari M. The survey on tendencies of primiparous women for selecting the mode of delivery. J Babol Univ Med Sci. 2009;11:54–9. [Google Scholar]
- 34.Béhague DP, Victora CG, Barros FC. Consumer demand for caesarean sections in Brazil: Informed decision making, patient choice, or social inequality? A population based birth cohort study linking ethnographic and epidemiological methods. BMJ. 2002;324:942–5. doi: 10.1136/bmj.324.7343.942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Klemetti R, Che X, Gao Y, Raven J, Wu Z, Tang S, et al. Cesarean section delivery among primiparous women in rural China: An emerging epidemic. Am J Obstet Gynecol. 2010;202:65.e1–6. doi: 10.1016/j.ajog.2009.08.032. [DOI] [PubMed] [Google Scholar]