

Abstract
BACKGROUND:
Prehypertension is one of the cardiovascular disease predicators. Management of prehypertension is an appropriate objective for clinicians in a wide range of medical centers. Massage therapy is primarily nonpharmacological treatment that is used to control blood pressure (BP). This study intends to investigate the long-term effect of massage therapy on BP in prehypertensive women.
METHODS:
This was a single-blind clinical trial study conducted on 50 prehypertensive women who referred to Sedigheh Tahereh Cardiovascular Center, during 6 months in 2009. Participants were selected by simple random sampling and were divided into control and intervention groups. The test group (25 patients) received massage for 10–15 min, three times a week for 10 sessions, and the control group (25 patients) was relaxed in the same environment but with no massage. Their BP was measured before and after each session and 72 h and 2 weeks after finishing the massage therapy. Analyzing the data was done using descriptive and inferential statistical methods (Chi-square, Mann–Whitney, paired t-test, and Student's t-test) through SPSS software version 18 and a significant level was considered as P < 0.05.
RESULTS:
The results indicated that the mean systolic BP (SBP) and diastolic BP (DBP) in the massage group were significantly lower in comparison with the control group (P < 0.001). Evaluation of durability of the massage effects on BP also indicated that 72 h after finishing the study, still there was a significant difference between the test and control groups in SBP and DBP (P < 0.001), but after 2 weeks, there was not a significant difference in SBP and DBP (P > 0.05) between the two groups.
CONCLUSIONS:
Although massage therapy seems to be a safe, effective, applicable, and cost-effective intervention to control BP of prehypertensive women, its effects do not persist for a long time.
Keywords: Blood pressure, long-term effect, massage therapy, prehypertension
Introduction
One of the major causes of increase of cardiovascular diseases in the world is the prevalence of hypertension,[1] which is considered as an important issue in public health and the risk of death all over the world.[2,3] Most of the people would realize high blood pressure (BP) when they experience heart attack or stroke and/or when they undergo a physical examination.[4] Today, in developed countries, one in every three adults has hypertension,[5,6] and the prevalence of hypertension in studies of other countries was higher in men, but in the studied researches in Iran, it was higher in women.[7]
Prevalence of hypertension in Isfahan also has a high percentage and is unexpected.[8] Obtained statistics in Iran in 2013 indicated that the prevalence of hypertension among the urban women was more than that in rural women.[9]
Recent studies showed that hypertension was not a definite biological process and it can be prevented or postponed through some certain measures.[10]
A previous term such as “high-normal” which was used in this BP range was not so applicable for the health staff, but they focused on the medical treatment with the new classifications.[11]
If someone undergoes two separate BP control, each control at least two times, and average BP is lower than 140/90 mmHg and higher than 120/80 mmHg, he/she would be placed in prehypertension group. Vasan et al. with a 10-year follow-up of the prehypertensive people and comparison of them with people with normal BP announced that the risk of cardiovascular disease in women and men with prehypertension was 2.5 and 1.6 times more than normal people, respectively.[12]
Many researchers while criticizing the researchers who use pharmacological therapy to treat them stated that focusing on lifestyle and using nonpharmacological methods are the first-line treatments to be provided to hypertensive people;[13,14] these treatments provide an effective means to lower the BP and have been emphasized increasingly as a useful method for both the prevention and treatment of hypertension.[15]
According to some studies, massage therapy is the most popular among the patients,[16] and more researches for exploring its effects are continuing.[17] In 1997, the Americans spent $27 billon to use complementary medicine like massage so that today due to increase of people's interest to use some of these techniques, particularly massage therapy, this medicine is a part of care plan in hospitals.[18]
Many researchers believed that massage is effective in reducing the systolic BP (SBP) and diastolic BP (DBP).
Mok and Woo during their study aimed to determine the effect of surface stroke back massage on anxiety, shoulder pain, SBP and DBPs, and heart rate of the people with brain stroke and showed a significant difference between average SBP and DBPs before and after the intervention in the test group (P < 0.05).[19]
Olney, also in his studies on patients with hypertension and on patients with high BP and prehypertensive clients, measured the average SBP and DBPs before and after the intervention in the different test groups and stated that massage therapy can be effective in controlling high BP.[8,20]
Another study aimed to determine the effect of massage therapy on BP of the patients with stroke in the massage group and showed lower average SBP) after the study (125.4 [11.8]) compared to that before the study (136.0 [14.8]) (P < 0.05) and also lower average DBP after the study (78.8 [9.0]) compared to that before the study (86.7 [12.4]) (P < 0.05); the differences were both significant.[21]
Hence, the effect of massage on BP almost is a fact, but no studies have examined the durability effects of massage. This study aimed to evaluate the persistence effect of Swedish massage (face, neck, shoulders, and chest) on BP of the women with prehypertension.
Methods
This was a two-group, two-phase single-blind clinical trial study, Iranian Register clinical trial (code: 389006), which was done with massage therapy intervention (independent variable) on BP changes (dependent variable).
The study population included adult nonpregnant women (18–60 years) referred to Sedigheh Tahereh Cardiovascular Center who were at the prehypertensive phase and had inclusion criteria.
The inclusion criteria were two separate BP measurements, each time at least two times, with the average BP of <140/90 and >120/80 mmHg, lack of diseases affecting the BP, lack of skin disease in the massage area, lack of taking medication affecting the BP, no specific diet, no obesity, no severe or acute stress, and lack of using relaxing techniques.
After obtaining the written informed consent, all the participants filled in the demographic data forms.
The study participants of control group were ensured that provided with intervention effectiveness and their willingness, and massage therapy would also be done on them. They were asked not to change their lifestyle during the study and continue their daily and routine habits, workout, and diet. The effective variables on BP were controlled as much as possible; however, individual differences, incidents, and daily stress and also the way individuals adapted themselves with life affairs were the uncontrollable variables of the study.
The samples were selected by the simple sampling method. Therefore, they were randomly divided into intervention and control groups.
Intervention
In the present study, we used Swedish Massage Therapy, which was performed using a nonaromatic topical lotion on face, neck, shoulders, and upper chest using superficial and deep stroking, three times a week (morning to noon, 8 am to 12 pm) each time for 10–15 min for 10 sessions in 3.5 weeks in the supine state. One of the researchers sat near the patient and her hand was parallel to the heart; she measured and recorded the BP of the client from the right hand before and after each intervention in each session [Figures 1 and 2].
Figure 1.

Swedish massage: (a) Deep stroking frontal, (b) Deep stroking up and down eyes, (c) Deep stroking the chin and jaw
Figure 2.
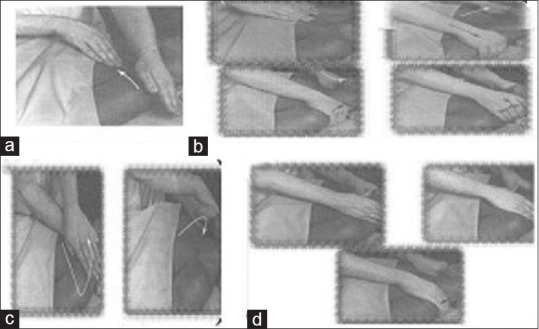
Swedish massage: (a) Stroking the upper chest area, (b) Deep stroking the shoulders and neck (c) Stroking fingers around the neck (d) Stroking the deep on vein
The control group had all the criteria of the test group except receiving massage. The test group lied down on the bed with the arbitrary position – close eyes and breathe deeply and relax their muscles when massage therapy was done. In addition, to assess the durability of the intervention effect, 72 h and 2 weeks after the study, all the study samples were called again to check their BP for the last time.
Data collection
The data of the present study were collected through discussion, case studies, and BP measurements. A Richter sphygmomanometer (made in England) and a standard Littmann® stethoscope (made in USA), the reliability and validity of which had been confirmed and calibrated at the beginning and middle of the study, were used by the researcher who was unaware of the samples’ group (test or control).
Measurement was done with respect to the American Heart Association suggested tips to accurately measure the BP. Furthermore, demographic data of the samples such as age, educational level, occupation, and marital status, and also menstrual status, height, and weight were recorded.[21]
To achieve the study results, collected data were encoded and analyzed by SPSS software version 16(233 South Wacker Drive, 11th Floor, Chicago). To do so, descriptive and inferential statistic methods were used. The obtained data were evaluated through descriptive statistics such as frequency, mean, and standard deviation and also inferential statistics such as Chi-square, Mann–Whitney, Fisher's exact test, paired t-test, and independent t-test.
Ethical considerations
This study was approved according to the research project No. 389006. The researcher introduced herself to the Sedigheh Tahereh Cardiovascular Center and obtained their approval. Moreover, the study objectives and method were explained to all participants, and written consent forms were obtained from them. All participants were free to accept or decline participation in the study and to leave the study during the exercise sessions.
Results
Reviewing the obtained results in the two groups indicated that there was no significant difference in terms of demographic data, menstrual status, and body mass index between the two groups (P > 0.05).
A comparison of the average SBP and DBP before and after the intervention and also durability of massage therapy effects on the BP of the prehypertensive clients at different times after the intervention is shown in Tables 1–4. The study results indicated that mean SBP and DBP in the massage group were significantly lower in comparison with the control group immediately after intervention and 3 days after intervention (P < 0.001), However, 2 weeks after finishing the study, there was not a significant difference in SBP and DBP between the two groups (P > 0.05).
Table 1.
The comparison of the mean systolic blood pressure of intervention and control groups before and after the intervention
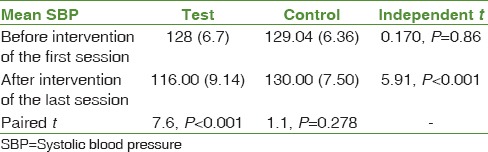
Table 4.
The comparison of the mean systolic and diastolic blood pressures of intervention and control groups 2 weeks after the study

Table 2.
The comparison of the mean diastolic blood pressure of intervention and control groups before and after the intervention
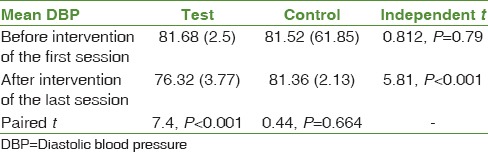
Table 3.
The comparison of the mean systolic and diastolic blood pressures of intervention and control groups 72 h after the study

Discussion
According to the results obtained from this study, it can be concluded that during the ten sessions of intervention, the mean SBP and DBP changes were different. The results indicated that mean SBP and DBP in the massage group were significantly lower in comparison with the control group immediately after the intervention (P < 0.001). Evaluation of long-term effect of the massage therapy indicated that 3 days after finishing the study, still there was a significant difference between the experimental and control groups in SBP and DBP (P < 0.001), However, 2 weeks after finishing the study, there was not a significant difference in SBP and DBP between the two groups in SBP and DBP (P > 0.05). It shows that massage therapy does not have a long-term effect. Few studies have examined the long-term effects of massage therapy. Meanwhile Olney's study showed significant differences in SBP and DBP between the two groups only 48 h after the study.[8] The study of Givi showed the durability of the massage on BP 72 h after the study. After finishing the study, Xiong et al.'s[22] meta-analyses showed that massage appears beneficial for reducing SBP for hypertensive patients as compared with antihypertensive drugs. Study results of Liao et al.'s (2016) showed that massage contributes to significantly enhanced reduction in SBP and as compared with control treatments in patients with hypertension and prehypertension[23] Chen et al.'s (2016) meta-analysis study demonstrated a medium effect of massage on SBP and a small effect on DBP in patients with hypertension or prehypertension. All these support the results of this study.
However, Supa’at et al. (2013)[24] showed a significant SBP reduction of 12 mmHg and DBP reduction of 5 mmHg in hypertensive women after four sessions with no significant difference between groups which does not support this study's results. This difference may be due to the difference between the number of sessions and massage technique between the two studies.
Many of the researchers also have considered that the slight BP reduction is worthwhile and believed that it can cause immunization from the hypertension side effects. Now, according to the obtained findings of the present study, it can be concluded that massage therapy, regardless of its unknown mechanism, can significantly reduce the BP of the clients and prevent from its side effects so that average SBP and DBP from the prehypertension range from the beginning of the study have been led to the normal BP. Furthermore, the effects of massage for at least 3 days after the intervention will remain. However, if you do not use long, loses its effectiveness. Therefore, the researchers introduced the massage therapy as an effective intervention on adjusting BP of the prehypertensive clients, and for the lasting effect, it is better to teach self-massage therapy to clients to do it at home regularly. Researchers are suggesting more studies to evaluate the long-term effect of massage therapy, because this study has some limitations such as low number of samples, the absence of male samples, and only prehypertension clients are evaluated.
Conclusions
There are few studies about the long-term effects of massage. Previous studies all discussed only the effects of massage, but they did not investigate the long-term effects of massage and how long it lasted. Of course, the present study also has limitations that are suggested it comparatively be repeated in men and women, in prehypertensive people, and those with hypertension in further study, and also the sustainability and durability of massage therapy effects on the BP of the prehypertensive clients at different times after the intervention be evaluated.
Financial support and sponsorship
This study was financially supported by School of Nursing and Midwifery, Isfahan University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We thank all the clients and also employees at the Sedigheh Tahereh Cardiovascular Center who cooperated.
References
- 1.Givi M. Durability of effect of massage therapy on blood pressure. Int J Prev Med. 2013;4:511–6. [PMC free article] [PubMed] [Google Scholar]
- 2.Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J, et al. Global burden of hypertension: Analysis of worldwide data. Lancet. 2005;365:217–23. doi: 10.1016/S0140-6736(05)17741-1. [DOI] [PubMed] [Google Scholar]
- 3.Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ, et al. Comparative Risk Assessment Collaborating Group, Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347–60. doi: 10.1016/S0140-6736(02)11403-6. [DOI] [PubMed] [Google Scholar]
- 4.Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. Brunner and Suddarth's Textbook of Medical-Surgical Nursing. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2008. Chapter: Assessment and management of patients with hypertension; p. 1022. [Google Scholar]
- 5.Lewis SM, Heitkemper MM, Bucher L, O’Brien PG. 7th ed. Philadelphia: Mosby Elsevier; 2007. Chapter: Nursing management hypertension. Medical-Surgical Nursing: Assessment and Management of Clinical Problems; p. 761. [Google Scholar]
- 6.Kaye AD, Kaye AJ, Swinford J, Baluch A, Bawcom BA, Lambert TJ, et al. The effect of deep-tissue massage therapy on blood pressure and heart rate. J Altern Complement Med. 2008;14:125–8. doi: 10.1089/acm.2007.0665. [DOI] [PubMed] [Google Scholar]
- 7.Azizi A, Abbasi MR, Abdoli GR. The prevalence of hypertension and its relationship with age, sex and Body Mass Index in people over 15 years the population covered by community based medical education arena Kermanshah in 2003. J Endocrinol Metab. 2008;10:323–31. [Google Scholar]
- 8.Yosefei H. MSc Thesis. Tehran: Tarbiat Modares University; 1994. Effect of Nonpharmacologic Methods of Reducing Blood Pressure in of High Blood Pressure Patients. [Google Scholar]
- 9.Malekzadeh MM, Etemadi A, Kamangar F, Khademi H, Golozar A, Islami F, et al. Prevalence, awareness and risk factors of hypertension in a large cohort of Iranian adult population. J Hypertens. 2013;31:1364–71. doi: 10.1097/HJH.0b013e3283613053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cohen GD. Promoting mental health, treating mental illness. Broadening the focus on intervention. Geriatrics. 2002;57:47–8. [PubMed] [Google Scholar]
- 11.Svetkey LP. Management of prehypertension. Hypertension. 2005;45:1056–61. doi: 10.1161/01.HYP.0000167152.98618.4b. [DOI] [PubMed] [Google Scholar]
- 12.Vasan RS, Larson MG, Leip EP, Evans JC, O’Donnell CJ, Kannel WB, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001;345:1291–7. doi: 10.1056/NEJMoa003417. [DOI] [PubMed] [Google Scholar]
- 13.Schunkert H. Pharmacotherapy for prehypertension – Mission accomplished? N Engl J Med. 2006;354:1742–4. doi: 10.1056/NEJMe068057. [DOI] [PubMed] [Google Scholar]
- 14.Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, et al. Seventh report of the joint national committee on prevention, detection, evaluation and treatment of high blood pressure. Hypertension. 2003;42:1206–52. doi: 10.1161/01.HYP.0000107251.49515.c2. [DOI] [PubMed] [Google Scholar]
- 15.Garakyaraghi M, Givi M, Moeini M, Eshghinezhad A. Qualitative study of women's experience after therapeutic massage. Iran J Nurs Midwifery Res. 2014;19:390–5. [PMC free article] [PubMed] [Google Scholar]
- 16.Buttagat V, Eungpinichpong W, Chatchawan U, Kharmwan S. The immediate effects of traditional Thai massage on heart rate variability and stress-related parameters in patients with back pain associated with myofascial trigger points. J Bodyw Mov Ther. 2011;15:15–23. doi: 10.1016/j.jbmt.2009.06.005. [DOI] [PubMed] [Google Scholar]
- 17.Moeini M, Givi M, Ghasempour Z, Sadeghi M. The effect of massage therapy on blood pressure of women with pre-hypertension. Iran J Nurs Midwifery Res. 2011;16:61–70. [PMC free article] [PubMed] [Google Scholar]
- 18.American Massage Therapy Association. Demand for Massage Therapy: Use and Acceptance Increasing. 2017. [Last accessed on 2018 Feb 02]. Available from: https://www.amtamassage.org/infocenter/economic_industryfact-sheet.html .
- 19.Mok E, Woo CP. The effects of slow-stroke back massage on anxiety and shoulder pain in elderly stroke patients. Complement Ther Nurs Midwifery. 2004;10:209–16. doi: 10.1016/j.ctnm.2004.05.006. [DOI] [PubMed] [Google Scholar]
- 20.Olney CM. The effect of therapeutic back massage in hypertensive persons: A preliminary study. Biol Res Nurs. 2005;7:98–105. doi: 10.1177/1099800405280827. [DOI] [PubMed] [Google Scholar]
- 21.Jouzi M, Amini R, Nourbakhsh V. Effects of massage therapy on blood pressure of patients with CVA. IJNR. 2007;1:15–21. [Google Scholar]
- 22.Xiong XJ, Li SJ, Zhang YQ. Massage therapy for essential hypertension: A systematic review. J Hum Hypertens. 2015;29:143–51. doi: 10.1038/jhh.2014.52. [DOI] [PubMed] [Google Scholar]
- 23.Liao IC, Chen SL, Wang MY, Tsai PS. Effects of massage on blood pressure in patients with hypertension and prehypertension: A Meta-analysis of randomized controlled trials. J Cardiovasc Nurs. 2016;31:73–83. doi: 10.1097/JCN.0000000000000217. [DOI] [PubMed] [Google Scholar]
- 24.Supa’at I, Zakaria Z, Maskon O, Aminuddin A, Nordin NA. Effects of Swedish massage therapy on blood pressure, heart rate, and inflammatory markers in hypertensive women. Evid Based Complement Alternat Med. 2013:171852. doi: 10.1155/2013/171852. [DOI] [PMC free article] [PubMed] [Google Scholar]