

Abstract
Hematospermia is a relatively frequent, distressing, and frightening symptom for the majority of men. Although the differential diagnosis list is extensive, it is usually a benign, self‐limiting disorder, including inflammatory and infective pathologies, resolving in several weeks. However, in some cases, hematospermia is the harbinger of more serious pathological lesions that should not be missed. In younger patients below 40 years of age, infection of the urogenital tract is the most common etiology. Simple routine laboratory studies should identify the pathological factors. In patients 40 years or older, or those with persistent or recurrent conditions or associated symptoms, it is necessary to exclude urogenital malignant disorders. Patients should also undergo medical history taking, physical examination including temperature and blood pressure assessment, digital rectal palpation, and laboratory blood, urine, and semen tests. If the diagnosis is still unclear, further investigations involve transrectal ultrasonography, magnetic resonance imaging, urethrocystoscopy, and histological confirmation by biopsy. Treatment for hematospermia depends on the underlying pathological lesions, but often involves only minimal examinations and simple reassurance in most cases. Hematospermia caused by genitourinary infections is effectively treated with appropriate antiviral, antibiotic, or antiparasitic agents. Hematospermia due to malignant disorders including prostate, testis, and seminal vesicle cancers resolves with definitive treatment of the primary lesions.
Keywords: Hematospermia, Genitourinary infection, Management, MRI imaging, Reassurance
Introduction
Hematospermia is traditionally defined as the macroscopic presence of blood in the semen. The condition is not uncommon, and can be a source of considerable anxiety in patients and their partners. Affected males and their partners are often frightened that they have a malignant disorder or venereal disease, or that their sex life will be adversely affected. Irrespective of whether the blood condition is fresh or old, hematospermia is most often caused by inflammatory or infectious disorders and follows a benign, self‐limiting course. This condition is rarely linked to serious dysfunctions, although, in males over 40 years of age, a more serious pathology may be underlying, consequently requiring further investigations. It has been reported that hematospermia comprises 1% of all urological symptoms [1]. The disorder may occur as a single or multiple episodes, or persist chronically. Patients typically visit a clinic after a single episode of hematospermia, being concerned about serious conditions including malignancy. In this article, we review the etiology, diagnosis, and treatment of hematospermia and provide an algorithm for the management of the disorder.
Ejaculation process and anatomical considerations
Physiologically, male sexual function consists of three stages: erection, ejaculation, and detumescence. Ejaculation includes two phases: emission and ejection. The former function is associated with the deposition of semen in the prostate urethra, while the latter is responsible for consecutive expulsion of the fluid to the outside of the body. The ejaculate contains secretions originating from the testis, epididymis, and several accessory sex glands, which come together in the prostate urethra [2]. The prostate adds secretions to the seminal fluid through numerous pores located in the prostate urethra.
Bulbourethral or Cowper's glands situated below the prostate also add fluid with a small volume. Hematospermia clinically depends on the emission and ejection processes [3]. The sympathetic nervous system is associated with the control of emission. Emission consists of the sequential contraction of the epididymis, vas deferens, seminal vesicles, and prostate and then the seminal fluid is deposited in the prostatic urethra. The bladder neck and external urethral sphincter are closed, which produces a spindle‐shaped space containing the deposited fluid. Therefore, in someone with retrograde ejaculation, hematospermia may be demonstrated as an expression of hematuria. The ejection process involves the tight closure of the bladder neck and the relaxation of the external urethral sphincter, and is followed by rhythmic contraction of the prostate and pelvic floor muscles, including the bulbocavernosus and ischiocavernosus muscles. The seminal fluid passes through the anterior urethra and exits the body.
Pathological changes at any point along the anatomical passage of the seminal fluid throughout the ejaculation process can lead to hematospermia.
Etiology
Hematospermia has been, historically, related to sexual overindulgence, prolonged sexual abstinence, and interrupted sexual intercourse. The presence of blood in the semen is known to be induced by inflammation, infection, tumors, blockage or injury, vascular abnormalities, systemic disease, and iatrogenic factors in any region within the male reproductive organs. The condition is most commonly caused by urogenital infections, especially in males younger than 40 years old [4, 5]. Some of the infectious etiologies of hematospermia include bacteria, Chlamydia trachomatis, ureaplasma, herpes simplex virus, Cytomegalovirus, and parasites [6, 7, 8]. Urogenital infections and inflammatory conditions are considered to account for 39–55% of the patients. Urogenital malignancies and trauma account for 4–13%. In 30–70% of cases, the pathology is not clarified after thorough assessment (Table 1).
Table 1.
Causes of hematospermia
| Inflammation and infections |
| Prostatitis, seminal vesiculitis, urethritis, epididymo‐orchitis |
| Sexually transmitted infections (gonorrhea, Chlamydia trachomatis, syphilis, trichomoniasis, herpes simplex) |
| Tuberculosis, schistosomiasis, Cytomegalovirus |
| Calculi of seminal vesicle, ejaculatory duct, prostate, urethra, bladder |
| Tumors |
| Benign |
| Granulation, adenomatous polyps of urethra |
| Condylomata acuminate |
| Benign prostatic hypertrophy |
| Leiomyoma of seminal vesicle |
| Malignant |
| Carcinoma of seminal vesicle, prostate, testis, epididymis |
| Sarcoma of seminal vesicle, prostate |
| Metastatic disease (melanoma) |
| Iatrogenic/trauma |
| Prostatic biopsy, prostatic injection, brachytherapy, cryotherapy, high‐intensity focused ultrasound therapy, urethral stents, self‐instrumentation, vasectomy, orchiectomy, hemorrhoidal sclerotherapy |
| Antithrombolytic, antifibrinolytic agents |
| Trauma to perineum, genitalia, or pelvis |
| Ductal obstruction and cysts |
| Ejaculatory duct obstruction, urethral stricture |
| Ejaculatory duct cyst, utricular cysts, prostatic cysts |
| Dilatation of seminal vesicles |
| Diverticula of seminal vesicles |
| Vascular abnormalities |
| Seminal vesicle‐venous fistula |
| Hemangioma of urethra |
| Varicosis of prostatic urethra |
| Arteriovenous malformation |
| Systemic factor |
| Severe hypertension |
| Hemophilia, purpura, von Willebrand's disease |
| Liver cirrhosis |
| Amyloidosis of seminal vesicles |
| Lymphoma |
| Idiopathic |
The fear of underlying malignancy prompts many people with hematospermia to undergo examination, and although men over 40 years old have a slightly increased risk of malignancy, urogenital malignancy is an infrequent cause of hematospermia, with prostate, testis, and seminal vesicle tumors having been reported [9, 10, 11]. It has been postulated that friable aberrant vessels produced by tumor angiogenic stimuli are associated with the condition. A review of the English literature revealed a total of 33 tumors in 931 patients in etiological studies of malignancy, for a low but still significant percentage of 3.5%. Twenty‐five of the 33 tumors were identified as of prostate origin. The remaining tumors were: 6 in the seminal vesicle, 1 in the testis, and 1 in the epididymis [12]. Han et al. [11] demonstrated in a prostate screening study that men with hematospermia, which comprised 0.5% of the screening population and had a mean age of 61 years, were 1.73‐fold more likely to have prostate cancer after adjusting for age, prostate‐ specific antigen, and rectal palpation results. Testicular tumors also rarely present with hematospermia [13, 14]. In a HIV‐positive man with malignant melanoma that metastasized to the seminal vesicles, persistent hematospermia was observed [15]. Resolution of the symptom would be expected after treatment of the underlying malignancy. The trend shows an increase in diagnostic pickup in more recent series, probably due to improved imaging techniques.
Various benign tumors may also induce hematospermia. Prostatic polyps in the urethra, condyloma acuminate, benign prostatic hypertrophy, or leiomyoma of the seminal vesicle have been described as causing hematospermia.
Iatrogenic manipulation is considered to be the most frequent cause of hematospermia because of recent developments in instrumental diagnosis and treatment, and this can be easily clarified by looking into the recent medical history of subjects. Because of increasing screening for prostate cancer, prostate biopsy has become the most common source of hematospermia, with a frequency of 6–13% [16, 17, 18]. However, a large survey demonstrated a hematospermia rate of only 1.2% with either the transrectal or transperineal approach [19]. Other less frequent causes include radiotherapy, cryotherapy, and high‐intensity focused ultrasound therapy for prostate cancer, as well as urethral instrumentation. Urethral stent migration and urethral foreign bodies reportedly induce hematospermia [12]. Drugs including aspirin for antithrombolytic treatments can also be related to hematospermia. In addition, external trauma to the genitalia, perineum, and pelvis may result in hematospermia. These causes of hematospermia should be evident through taking the patient's history and are expected to be self‐limiting.
Ejaculatory duct obstruction or cysts can induce hematospermia [20, 21, 22, 23]. Ductal obstruction and cyst formation can cause the distension and rupture of mucosal blood vessels through an increased pressure in those structures. Patients may also present with a low volume of ejaculate and infertility [24, 25]. Other reported causes include dilatation and diverticulum of the seminal vesicles, and prostatic and utricular cysts.
Hematospermia has been associated with vascular abnormalities including hemangioma, arteriovenous fistula, and other vascular malformations [26, 27, 28]. A patient with aberrant vessels of the posterior urethra presenting with hematospermia has been reported. Seminal vesicle‐venous communication can also induce recurrent hematospermia [29]. In such cases with direct blood vessel involvement, it is understandable that massive hematospermia can be recognized, which may possibly induce the serious complication of urinary retention due to blood clots. Wang et al. [30] demonstrated adequate success without sexual dysfunction in 5 patients with arterial fistula treated by pelvic angiography and embolization.
Although systemic conditions are less clearly related to hematospermia, severe uncontrolled hypertension and coagulation disorder, such as hemophilia and von Willebrand's disease, have to be considered [31, 32]. Severe liver dysfunction can lower blood platelets, which also induces hematospermia [33]. However, it remains to be clarified whether increased portal pressure via connections to prostatic venous plexuses can induce hematospermia. Amyloidosis of seminal vesicles, which mostly shows localized lesions, is associated with hematospermia in older men [34, 35, 36]. Furthermore, hematospermia may even be a rare and sole symptom of lymphoma [37]. Treatment of the systemic pathology should generally resolve the hematospermia.
Clinical assessment
Most patients visit their doctors promptly after the first episode of hematospermia because of an impressing experience that provokes great anxiety. The diagnostic process can be initiated by systematic clinical history taking, which may help to evaluate the causes of hematospermia. It is recommended to question the patient concerning the duration and amount of bleeding, as well as sexual and voiding conditions. Symptoms are generally only present for a short time, with an average of 1–24 months [4]. To exclude the partner as a source of the bleeding, the condition at the onset of hematospermia should be confirmed. A ‘condom test’ can be carried out where the patient is asked to collect the semen in the condom which is checked for blood.
Physical examination includes an assessment of body temperature, blood pressure, palpation of the abdomen for pelvic masses, and examination of the external genitalia. The testes, epididymis, vas deferens, and penile urethra are carefully examined for any lesions that may bleed. The presence of a rash or blisters warrants elucidation of further details concerning sexual behavior. A digital rectal examination of the prostate and seminal vesicles should be performed to exclude prostatitis, or pathological lesions. The urethral meatus should be re‐examined for the presence of bloody discharge after palpation of the prostate.
Laboratory tests include a blood cell count, serum coagulation profile, and prostate‐specific antigen in males of 40 years or older. Coagulation studies are recommended for all patients with persistent hematospermia since this status is associated with coagulation disorder. Urine analysis and bacterial culture of urine will help to confirm whether or not urinary infection and hematuria are present. Urine culture is recommended for all cases with hematospermia because the test is of low cost and a positive result suggests an etiology. Analysis of the ejaculate may reveal the presence of white blood cells, which warrants further examination regarding infectious disorder. Semen culture, mycobacterial culture, and viral serology are recommended. A urethral swab for sexually transmitted disease should be carried out. Analysis for parasites is also required, if indicated. It has been reported that, in a traveler returning from overseas with hematospermia and Schistosoma haematobium infection, numerous ova were demonstrated in the ejaculate, with negative urinalysis, and fecal tests, and negative serology [38].
In patients below 40 years old, infection of the urogenital tract is the most common etiology. Simple routine laboratory studies should determine the pathological factors. In patients 40 years or older, or those with persistent or recurrent hematuria or associated symptoms including hematuria, it is necessary to rule out urogenital malignant diseases (Fig. 1).
Figure 1.
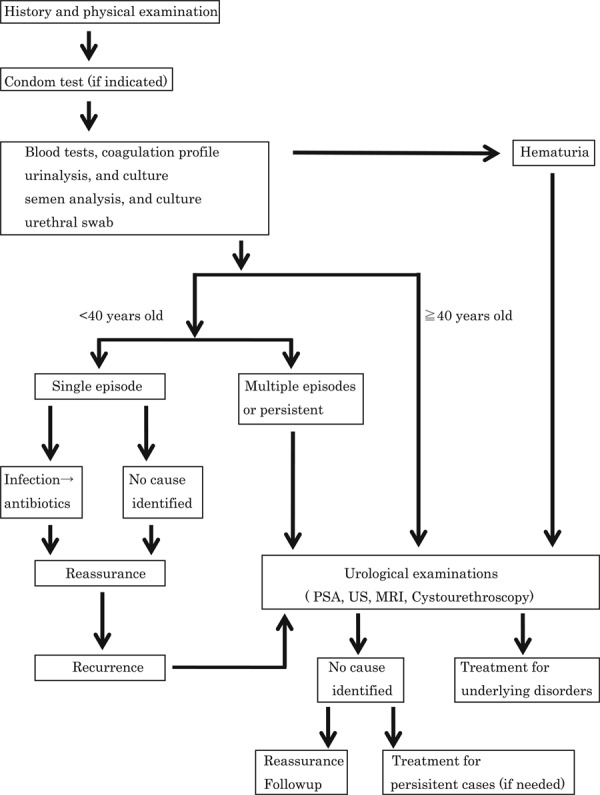
An algorithm for management of hematospermia
Imaging technique
Transrectal ultrasonography (TRUS) may help in the diagnosis of disorders of the prostate and seminal vesicle. TRUS allows excellent visualization of the prostate, seminal vesicle, and adjacent anatomies. TRUS is thus less invasive and a safer procedure, and is recommended as the first imaging investigation. Various studies have revealed its high‐level efficacy in the evaluation of hematospermia [39, 40]. The pathological findings yielded by this procedure include prostatic calculi, ejaculatory duct calculi, ejaculatory duct cyst, benign prostatic hypertrophy, prostate cancer, dilated seminal vesicle, and seminal vesicle calculi. Seminal vesicle puncture guided by TRUS is performed to ascertain the site of bleeding in selected cases, while the pathological ultrasonographic findings yielded by this technique do not always demonstrate the origin of bleeding [41]. If the scrotal examination results are abnormal, scrotal ultrasonography may be considered to rule out testicular neoplasia, while testicular tumors with hematospermia are rare.
Other imaging modalities are intravenous urography (IVU), computerized tomography (CT), and magnetic resonance imaging (MRI). IVU is rarely required and CT with its limited resolution, radiation exposure, and technical complexity may not be useful for diagnosing the etiology of hematospermia. MRI is considered to be the technique of choice, and it improves visualization of the pelvic structures if TRUS shows entirely normal findings [42, 43, 44, 45]. MRI is accurate for detecting seminal vesicle bleeding and can also demonstrate if the seminal vesicle bleeding is fresh or old [46].
Minimally invasive procedures, including flexible urethrocystoscopy [47], may be needed in some cases. Endoscopic examination allows the direct visualization of urethral disorders including urethritis, polyps, stones, vascular abnormalities, foreign bodies, and bladder neck pathology, and then histological studies by biopsy are also performed. Cystoscopic observation of the openings of ejaculatory or prostatic ducts with simultaneous prostate massage may be useful to localize bleeding [3]. Recently, Liu et al. [48] demonstrated that transurethral seminal vesiculoscopy is useful in the diagnosis and treatment as well (Fig. 1).
Treatment
Treatment for hematospermia depends on the underlying pathological conditions, if detected. In most cases, bleeding is slight and self‐limiting, and relieving patients’ anxieties is fundamental for management. In patients younger than 40 years with a single episode of the disorder, clinical evaluation with basic examinations to exclude any genitourinary infection or inflammation is considered to be sufficient. When no pathological findings are determined, watchful waiting and reassurance of the patient might be a therapeutic modality. Leary and Aguilo [49] followed 150 patients with idiopathic hematospermia for 5–23 years, and none showed serious disorders. If an organism of urogenital infection is confirmed, the administration of adequate antiviral, antibiotic, or antiparasitic drugs is indicated on the basis of the sensitivity of the cultured organisms [50] (Fig. 1).
Cystic lesions of the prostate, seminal vesicles, ejaculatory ducts, or embryological remnants including the Müllerian duct may be treated with ultrasound‐ or CT‐guided aspiration. In previous hematospermia patients, anticoagulant substances, including antibiotics and steroid hormones, were injected into dilated seminal vesicles under TRUS guidance, and the disorder transiently resolved for a maximum of 3 months [41]. Transurethral unroofing of cysts or ductal obstruction as well as laparoscopic procedures can also be performed. Ejaculatory duct obstruction has also been managed by a transurethral incision at the duct opening [23, 51]. Recently, new invasive and noninvasive techniques have been employed. Transrectal heat rotating magnet fields showed an 81% cure rate for persistent disorders [52]. Perineal bilateral seminal vesicle puncture along with continuous irrigation with agents yielded a >90% cure rate in patients with refractory hematospermia [53]. Further development of new therapeutic modalities should be expected.
It has recently been demonstrated that empirical evidence suggests a role for antifibrinolytic agents including finasteride in treating certain causes of the disorder [12]. However, further studies are required before the treatments are considered as possible drugs for hematospermia.
A more extensive examination is needed involving patients 40 years or older, for those with recurrence or macroscopic hematuria. As persistent or recurrent hematospermia could be the only symptom of prostate cancer, surveillance with PSA monitoring over a period of time is recommended, especially in middle‐aged individuals with a family history of prostate cancer.
The presence of blood in the ejaculate can be very stressful for both patients and their sexual partners. Especially, younger patients may also be concerned through associating it with infertility or sexual dysfunction. On the other hand, older subjects may worry about underlying malignant disorders. It is considered important to accurately recognize the stress levels of individual subjects. When a patient's anxiety cannot be appropriately relieved through good communication and a full investigation, psychological consultation may be warranted.
Conclusions
Hematospermia is usually a benign, self‐limited condition but an anxiety‐provoking sign for the majority of males. Although the differential diagnosis list is extensive, most cases are induced by inflammatory and infective pathologies, resolving in several weeks. In younger patients below 40 years of age, infection of the urogenital tract is the most common etiological condition. In patients 40 years or older, or those with persistent or recurrent conditions or associated symptoms, it is necessary to exclude malignant urogenital disorders. With modern imaging modalities, the number of idiopathic cases should be much lower than historically reported.
Specific treatment for hematospermia depends on the underlying pathological lesions but often involves only minimal examinations and simple reassurance in most cases.
Hematospermia due to malignant disorders including prostate, testis, and seminal vesicle cancers resolves with definitive treatment of the primary lesions.
References
- 1. Polito M, Giannubilo W, d'Anzeo G, Muzzonigro G. Hematospermia: diagnosis and treatment. Arch Ital Urol Androl, 2006, 78, 82–85 [PubMed] [Google Scholar]
- 2.Schlegel PN, Hardy MP, Goldstein M. Male reproductive physiology. In: Wein AJ, editor. Campbell‐Walsh urology. 9th ed. Philadelphia: Saunders Elsevier; 2007. p. 577–608.
- 3. Munkelwitz R, Krasnokutsky S, Lie J, Shah SM, Bayshtok J, Khan SA. Current perspectives on hematospermia: a review. J Androl, 1997, 18, 6–14 [PubMed] [Google Scholar]
- 4. Mulhall JP, Albertsen PC. Hemospermia: diagnosis and management. Urology, 1995, 46, 463–467 10.1016/S0090‐4295(99)80256‐8 [DOI] [PubMed] [Google Scholar]
- 5. Fuse H, Ichikawa T, Ishii H, Sumiya H, Shimazaki J. Clinical observations on hematospermia. Nishinihon J Urol, 1987, 49, 1057–1061 [Google Scholar]
- 6. Bamberger E, Madeb R, Steinberg J, Paz A, Satinger I, Kra‐Oz Z et al. Detection of sexually transmitted pathogens in patients with hematospermia. Isr Med Assoc J, 2005, 7, 224–227 [PubMed] [Google Scholar]
- 7. Koment RW, Poor PM. Infection by human cytomegalovirus associated with chronic hematospermia. Urology, 1983, 22, 617–621 10.1016/0090‐4295(83)90309‐6 [DOI] [PubMed] [Google Scholar]
- 8. Elem B, Patil PS. Haemospermia: observations in an area of endemic bilharziasis. Br J Urol, 1987, 60, 170–173 10.1111/j.1464‐410X.1987.tb04957.x [DOI] [PubMed] [Google Scholar]
- 9. Fujisawa M, Ishigami J, Kamidono S. Adenomyosis of the seminal vesicle with hematospermia. Acta Urol Jpn, 1993, 39, 73–76 [PubMed] [Google Scholar]
- 10. Vilandt J, Sønksen J, Mikines K, Torp‐Pedersen S, Colstrup H. Seminoma in the testes associated with haemospermia. BJU Int, 2002, 89, 633 10.1046/j.1464‐410X.2002.02684.x [DOI] [PubMed] [Google Scholar]
- 11. Han M, Brannigan RE, Antenor JA, Roehl KA, Catalona WJ. Association of hemospermia with prostate cancer. J Urol, 2004, 172, 2189–2192 10.1097/01.ju.0000144565.76243.b1 [DOI] [PubMed] [Google Scholar]
- 12. Ahmad I, Krishna NS. Hemospermia. J Urol, 2007, 177, 1613–1618 10.1016/j.juro.2007.01.004 [DOI] [PubMed] [Google Scholar]
- 13. Maheshkumar P, Otite U, Gordon S, Berney DM, Nargund VH. Testicular tumor presenting as hematospermia. J Urol, 2001, 165, 188 10.1097/00005392‐200101000‐00050 [DOI] [PubMed] [Google Scholar]
- 14. Weissbach L, Janson R, Bastian HP, Müller R, Tschubel K, Vahlensieck W. Rare metastasizing of a testicular tumor. Differential diagnosis of hemospermia. Münch Med Wochenschr, 1977, 119, 297–298 [PubMed] [Google Scholar]
- 15. Meng MV, Werboff LH. Hematospermia as the presenting symptom of metastatic malignant melanoma of unknown primary origin. Urology, 2000, 56, 330 10.1016/S0090‐4295(00)00634‐8 [DOI] [PubMed] [Google Scholar]
- 16. Gustafsson O, Norming U, Nyman CR, Ohström M. Complications following combined transrectal aspiration and core biopsy of the prostate. Scand J Urol Nephrol, 1990, 24, 249–251 [PubMed] [Google Scholar]
- 17. Celebi I, Irer B, Kefi A, Kurtulan E, Goktay Y, Ergin T. Relationship between complications due to prostate biopsy and the scores of pain and discomfort. Urol Int, 2004, 72, 303–307 10.1159/000077682 [DOI] [PubMed] [Google Scholar]
- 18. Song SH, Kim JK, Song K, Ahn H, Kim CS. Effectiveness of local anaesthesia techniques in patients undergoing transrectal ultrasound‐guided prostate biopsy: a prospective randomized study. Int J Urol, 2006, 13, 707–710 10.1111/j.1442‐2042.2006.01390.x [DOI] [PubMed] [Google Scholar]
- 19. Kakehi Y, Naito S Japanese Urological Association . Complication rates of ultrasound‐guided prostate biopsy: a nation‐wide survey in Japan. Int J Urol, 2008, 15, 319–321 10.1111/j.1442‐2042.2008.02048.x [DOI] [PubMed] [Google Scholar]
- 20. Poppel H, Vereecken R, Geeter P, Verduyn H. Hemospermia owing to utricular cyst: embryological summary and surgical review. J Urol, 1983, 129, 608–609 [DOI] [PubMed] [Google Scholar]
- 21. Weintraub MP, Mouy E, Hellstrom WJ. Newer modalities in the diagnosis and treatment of ejaculatory duct obstruction. J Urol, 1993, 150, 1150–1154 [DOI] [PubMed] [Google Scholar]
- 22. Neustein P, Hein PS, Goergen TG. Chronic hemospermia due to müllerian duct cyst: diagnosis by magnetic resonance imaging. J Urol, 1989, 142, 828 [DOI] [PubMed] [Google Scholar]
- 23. Fuse H, Nishio R, Murakami K, Okumura A. Transurethral incision for hematospermia caused by ejaculatory duct obstruction. Arch Androl, 2003, 49, 433–438 10.1080/01485010390219890 [DOI] [PubMed] [Google Scholar]
- 24. Colpi G, Roveda M, Tognetti A, Balerna M. Seminal tract inflammation and male infertility. Acta Eur Fertil, 1988, 19, 69–77 [PubMed] [Google Scholar]
- 25. Fuse H, Mizuno I, Iwasaki M, Akashi T. Transurethral treatment of ejaculatory duct obstruction in infertile men. Arch Androl, 2003, 49, 429–431 [PubMed] [Google Scholar]
- 26. Glancy RJ, Gaman AJ, Rippey JJ. Polyps and papillary lesions of the prostatic urethra. Pathology, 1983, 15, 153–157 10.3109/00313028309084703 [DOI] [PubMed] [Google Scholar]
- 27. Cattolica EV. Massive hemospermia: a new etiology and simplified treatment. J Urol, 1982, 128, 151–152 [DOI] [PubMed] [Google Scholar]
- 28.Saito S. Posterior urethral hemangioma: one of the unknown causes of hematuria and/or hematospermia. Urology. 2008;71:168.e11–4. [DOI] [PubMed]
- 29. Magid MA, Hejtmancik JH. Hematospermia. J Urol, 1957, 78, 82–88 [DOI] [PubMed] [Google Scholar]
- 30. Wang LJ, Tsui KH, Wong YC, Huang ST, Chang PL. Arterial bleeding in patients with intractable hematospermia and concomitant hematuria: a preliminary report. Urology, 2006, 68, 938–941 10.1016/j.urology.2006.06.015 [DOI] [PubMed] [Google Scholar]
- 31. Close CF, Yeo WW, Ramsay LE. The association between haemospermia and severe hypertension. Postgrad Med J, 1991, 67, 157–158 10.1136/pgmj.67.784.157 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Lemesh RA. Case report: recurrent hematuria and hematospermia due to prostatic telangiectasia in classic von Willebrand's disease. Am J Med Sci, 1993, 306, 35–36 10.1097/00000441‐199307000‐00009 [DOI] [PubMed] [Google Scholar]
- 33. Marshall VF, Fuller NL. Hemospermia. J Urol, 1983, 129, 377–378 [DOI] [PubMed] [Google Scholar]
- 34. Botash RJ, Poster RB, Abraham JL, Makhuli ZM. Senile seminal vesicle amyloidosis associated with hematospermia: demonstration by endorectal MRI. J Comput Assist Tomogr, 1997, 21, 748–749 10.1097/00004728‐199709000‐00017 [DOI] [PubMed] [Google Scholar]
- 35. Schaeffer EM, Epstein JI, Walsh PC. Amyloidosis of the seminal vesicle and hematospermia. J Urol, 2004, 171, 2382 10.1097/01.ju.0000124043.25456.1b [DOI] [PubMed] [Google Scholar]
- 36. Vandwalle J, Dugardin F, Petit T, Surga N, Paul A, Petit J. Haemospermia due to seminal vesicle amyloidosis: treatment by laparoscopic vesiculectomy: a case report. Prog Urol, 2007, 17, 1382–1384 10.1016/S1166‐7087(07)78583‐4 [DOI] [PubMed] [Google Scholar]
- 37. Geoghegan JG, Bonavia I. Haematospermia as a presenting symptom of lymphoma. Br J Urol, 1990, 66, 658 10.1111/j.1464‐410X.1990.tb07204.x [DOI] [PubMed] [Google Scholar]
- 38. Torresi J, Sheori H, Ryan N, Yung A. Usefulness of semen microscopy in the diagnosis of a difficult case of schistosoma haematobium infection in a returned traveler. J Travel Med, 1997, 4, 46–47 10.1111/j.1708‐8305.1997.tb00774.x [DOI] [PubMed] [Google Scholar]
- 39. Worischeck JH, Parra RO. Chronic hematospermia: assessment by transrectal ultrasound. Urology, 1994, 43, 515–520 10.1016/0090‐4295(94)90243‐7 [DOI] [PubMed] [Google Scholar]
- 40. Yagci C, Kupeli S, Tok C, Fitoz S, Baltaci S, Gogus O. Efficacy of transrectal ultrasonography in the evaluation of hematospermia. J Clin Imaging, 2004, 28, 286–290 10.1016/S0899‐7071(03)00157‐8 [DOI] [PubMed] [Google Scholar]
- 41. Fuse H, Sumiya H, Ishii H, Shimazaki J. Treatment of hemospermia caused by dilated seminal vesicles by direct drug injection guided by ultrasonography. J Urol, 1988, 140, 991–992 [DOI] [PubMed] [Google Scholar]
- 42. Maeda H, Toyooka N, Kinukawa T, Hattori R, Furukawa T. Magnetic resonance images of hematospermia. Urology, 1993, 41, 499–504 10.1016/0090‐4295(93)90519‐G [DOI] [PubMed] [Google Scholar]
- 43. Cho IR, Lee MS, Rha KH, Hong SJ, Park SS, Kim MJ. Magnetic resonance imaging in hemospermia. J Urol, 1997, 157, 258–262 10.1016/S0022‐5347(01)65340‐0 [PubMed] [Google Scholar]
- 44. Lencioni R, Ortori S, Cioni D, Morelli G, Ceretti E, Cosottini M et al. Endorectal coil MR imaging findings in hemospermia. MAGMA, 1999, 8, 91–97 10.1007/BF02590525 [DOI] [PubMed] [Google Scholar]
- 45. Torigian DA, Ramchandani P. Hematospermia: imaging findings. Abdom Imaging, 2007, 32, 29–49 10.1007/s00261‐006‐9013‐3 [DOI] [PubMed] [Google Scholar]
- 46. Furuya S, Furuya R, Masumori N, Tsukamoto T, Nagaoka M. Magnetic resonance imaging is accurate to detect bleeding in the seminal vesicles in patients with hemospermia. Urology, 2008, 72, 838–842 10.1016/j.urology.2008.05.058 [DOI] [PubMed] [Google Scholar]
- 47. Li L, Jiang C, Song C, Zhou Z, Song B, Li W. Transurethral endoscopy technique with a ureteroscope for diagnosis and management of seminal tracts disorders: a new approach. J Endourol, 2008, 22, 719–723 10.1089/end.2007.0130 [DOI] [PubMed] [Google Scholar]
- 48. Liu ZY, Sun YH, Xu CL, Hou JG, Gao X, Lu X et al. Transurethral seminal vesiculoscopy in the diagnosis and treatment of persistent or recurrent hemospermia: a single‐institution experience. Asian J Androl, 2009, 11, 566–570 10.1038/aja.2009.47 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Leary FJ, Aguilo JJ. Clinical significance of hematospermia. Mayo Clin Proc, 1974, 49, 815–817 [PubMed] [Google Scholar]
- 50. Jones DJ. Haemospermia: a prospective study. Br J Urol, 1991, 67, 88–90 10.1111/j.1464‐410X.1991.tb15076.x [DOI] [PubMed] [Google Scholar]
- 51. Razvi HA, Denstedt JD. Endourologic management of seminal vesicle cyst. J Endourol, 1994, 8, 429–431 10.1089/end.1994.8.429 [DOI] [PubMed] [Google Scholar]
- 52.Jin HM, Zhan BY, Wang LL. Massage of transrectal heat rotating magnetic field in the treatment of obstinate hemospermia. Natl J Androl. 2006;12:60–1, 65. [PubMed]
- 53. Zhang XR, Gu BJ, Xu YM, Chen R, Zhang J, Qiao Y. Transrectal ultrasonography‐guided transperineal bilateral seminal vesicle puncture and continuous irrigation for the treatment of intractable hematospermia. Chin Med J, 2008, 121, 1052–1054 [PubMed] [Google Scholar]