

Abstract
This study investigated (a) the stress spillover pathways linking contextual stressors, changes in couple relationship functioning and depressive symptoms, and changes in individuals’ physical health, and (b) the stress-buffering effect of participation in an efficacious, family-centered prevention program designed to protect couples from the deleterious effects of stressors. The sample consisted of 346 rural African American couples (63% married) who participated in a randomized controlled trial of the Protecting Strong African American Families (ProSAAF) program. Participants were assessed at three time points across 17 months. Results examining stress spillover within the control group indicated that elevated current, but not prior, financial hardship was associated with decreased effective communication, relationship satisfaction, and relationship confidence as well as increased depressive symptoms; current levels of racial discrimination also predicted greater depressive symptoms. Relationship confidence and relationship satisfaction, but not communication or depressive symptoms, in turn predicted declines in self-reported physical health. Results examining stress-buffering effects suggested that participation in ProSAAF protected individuals’ relationship confidence from declines associated with elevated financial hardship. In addition, the indirect effect linking financial hardship to declines in physical health through relationship confidence that emerged among participants in the control group was no longer evident for ProSAAF couples. Results highlight the effect of contextual stressors on African Americans’ couple and individual well-being and the potential for the ProSAAF program to provide a constructed resilience resource, protecting couple’s confidence in their relationship from the negative effects of financial hardship and, consequently, promoting physical health.
Keywords: African American, financial hardship, health, prevention, stress
The rural southeastern United States (US) is one of the most impoverished regions of the country (DeNavas-Walt & Proctor, 2014). For many African American adults living in this region, experiences with financial hardship, racial discrimination, and other contextual stressors can have pronounced, harmful effects on their romantic relationships and personal health (Barton & Bryant, 2016; Kahn & Pearlin, 2006; Williams & Mohammed, 2009). Furthermore, consistent with the broader literature on racial health disparities, rural African American adults are at an elevated risk for a variety of chronic diseases associated with aging, such as cardiovascular disease and type 2 diabetes (Hartley, 2004; Office of Minority Health, 2016a, 2016b).
Prior research has examined various psychosocial mechanisms that potentially underlie elevated health risks among individuals of low socioeconomic status, including individual, family, and neighborhood factors (see Chen & Miller, 2013 for review). Conspicuously absent from much of this literature are the potential intermediary effects of couple processes. This lack of attention is somewhat surprising given the robust associations between contextual stress and marital quality (Randall & Bodenmann, 2009) as well as those between marital quality and individual health (Robles, Slatcher, Trombello, & McGinn, 2014). These respective literatures suggest that changes in couple processes attributable to contextual stressors may act as one mechanism through which contextual stressors affect physical health. Hence, preventive interventions designed to protect couples’ relational well-being from the deleterious effects of financial hardship may yield additional indirect benefits for individuals’ physical well-being.
The present study was designed to investigate these questions. Data for the study are from a sample of rural African American couples participating in a randomized controlled trial (RCT) of the Protecting Strong African American Families (ProSAAF) program. ProSAAF is a newly developed, family-centered preventive intervention designed to prevent stress spillover and promote positive couple, parenting, and family interactions within two-parent African Americans families living in the impoverished rural South. Two central aims guided the current study. First, using the control sample, we examined whether financial hardship and racial discrimination predicted change in multiple facets of couples’ relationship functioning as well as change in depressive symptoms, and whether the facets influenced by stress serve as a mechanism through which contextual stress affects change in rural African Americans’ self-reported health. Second, using the full randomized sample, we examined whether participation in the ProSAAF program buffered African Americans’ relational and physical health from the negative effects of contextual stress.
Stress spillover in couples: Linking contextual stress to physical health
Stressful experiences in one domain of life are often associated with deteriorations in other domains, a phenomenon referred to as stress spillover (Neff, 2012). Higher levels of financial hardship, for example, have been associated with lower levels of relationship functioning and satisfaction (Falconier & Epstein, 2011). An equally robust body of literature has documented that distressing couple and marital relationships can have pronounced effects on individuals’ physical health (for review, see Robles et al., 2014). Despite these findings, few studies have investigated the hypothesis that, among adults in romantic relationships, changes in couple relationship processes serve as a mechanism through which financial hardship negatively affects individuals’ physical health. To date, research on psychosocial mechanisms implicated in socioeconomic health disparities has instead focused on intrapersonal measures (e.g., depressive symptoms) and, within the family, constructs such as parenting, conflict, and routinized family environments (see Chen & Miller, 2013). Our review of the literature identified only a select few longitudinal studies that examined the associations among contextual stress, couple processes, and African Americans’ health, whose results provide some evidence of the potential intermediary role of couple process (e.g., Lei et al., 2016; O’Neal, Arnold, Lucier-Greer, Wickrama, & Bryant, 2015).
Given the lack of research on relationship factors that link contextual stressors to changes in physical health, many relationship facets could be examined. Two of the most evident potential mechanisms include couple communication and relationship satisfaction, both of which have been shown to be influenced by financial hardship (Falconier & Epstein, 2011) and to predict individuals’ health (Slatcher, 2010). In addition to these two frequently-studied measures, the present study also considers the intervening effect of relationship confidence, which reflects an individual’s perceived efficacy in both managing relationship conflicts as a couple and maintaining a healthy relationship in the future (Whitton et al., 2007). In research to date, relationship confidence has been found to predict changes in individuals’ psychological distress, life satisfaction, and depressive symptoms in addition to promoting couple time together and overall relationship quality (Johnson & Anderson, 2013; Whitton et al., 2007; Whitton, Rhoades, & Whisman, 2014). Further supporting this intermediatary role of couple relationship confidence are findings at the intra-personal level indicating that individuals’ self-confidence and self-efficacy predict individuals’ physical well-being (Reed, Duncan, Lucier-Greer, Fixelle, & Ferraro, 2016) and are influenced by financial hardship (Caplan & Schooler, 2007).
In addition to examining psychosocial mechanisms of stress spillover, the present study also sought to inform research on the temporal nature of stress spillover effects. Most research on stress spillover in families has used one of two approaches. The first body of research, originating from longitudinal studies, has investigated prospective associations between stress at an earlier time point and couple and family functioning many months later. The Family Stress Model (Conger & Elder, 1994) is a prime example of this approach. Although supported in many studies, it is worth noting that many of these studies do not control for prior levels of relationship processes (Parke et al., 2004; Robila & Krishnakumar, 2005); consequently, limited conclusions that can be drawn from these studies about the effects of stress on change in couple processes over time. A second body of research, originating from cross-sectional and short-term daily diary studies, has drawn attention to the contemporaneous, or immediate, effect of stress on couple and family functioning. This approach is illustrated in conceptual models and related findings by Neff (2012) and Repetti and colleagues (2009). Although positively capturing the effects of stress on within- and between-person variability, this second approach is limited in its ability to identify long-term change in couple functioning. Thus, the present study additionally sought to investigate empirically whether long-term change in couple processes is predicted by carryforward effects of earlier levels of stress (i.e., prospective associations) and/or concurrent levels of stress (i.e., contemporaneous associations).
Stress-buffering in couples: Protective-stabilizing effects of family-centered prevention
As highlighted in a seminal paper by Cohen and Wills (1985), supportive social relationships can buffer individuals’ physical and psychological well-being against stressful life experiences. Although this assertion has been largely supported with respect to social support for individuals generally (Cohen, 2004), findings regarding the protective function of spousal support are mixed (Brock & Lawrence, 2008; Cranford, 2004).1 Beginning in the late 20th century and continuing today, a variety of prevention programs have been developed for couples (Markman & Rhoades, 2012), many of which focus on spousal support and aim to promote resiliency to stressful events in a manner consistent with the stress-buffering hypothesis. Despite this focus, little empirical research has been conducted to determine whether program participation actually buffers couples’ relationship quality from stress. This emphasis on direct (rather than stress-buffering) effects from program participation is evident even in programs specifically designed to help couples cope with stress (Bodenmann & Shantinath, 2004). Thus, whether family-centered prevention programming can buffer couples’ relationship quality and personal health from the negative spillover effects of financial hardship and other contextual stressors remains unknown.
This type of program-related moderation effect is identical to the protective-stabilizing effects described in the resilience literature (Rutter, 2005), in which a resilience resource reduces the association between a risk factor and a subsequent outcome that emerge in the general population. From this perspective, a prevention program can be viewed as providing a “constructed resilience resource” when it buffers participants’ well-being from the negative effects of stress or adversity that is evident in the control condition (also see Brody, Yu, Beach, & Philibert, 2015). ProSAAF was conceptualized as such a resource for African American couples. Previous analyses from the ProSAAF RCT have indicated that treatment couples, compared with couples in the control condition, demonstrated improved functioning in various couple and coparenting measures (Barton et al., 2017; Barton et al., unpublished data); no research, however, has examined ProSAAF’s capacity to buffer couples’ relationship outcomes and subsequent physical health from the negative effects of financial hardship and other contextual stressors.
The Present Study
The present study was designed to address two aims. First, we sought to identify how two contextual stressors – financial hardship and racial discrimination – affect African Americans couples’ relationship processes and their subsequent effects on physical health (see Figure 1a). Historically, most research on contextual stressors and couple functioning among African Americans has focused on financial hardship, despite calls for longitudinal studies that investigate the unique stressor of racial discrimination experienced by racial minority couples (Bryant et al., 2010). The inclusion of both financial hardship and racial discrimination in these analyses also demonstrates the unique effect of each stressor, controlling for the presence of the other. In addition to examining spillover effects on couple processes, we also examine depressive symptoms as an alternative, intra-individual pathway that might also link contextual stress to physical health (Chen & Miller, 2013). As described earlier, spillover effects of stress were investigated prospectively (i.e., lagged effect of earlier stress) and contemporaneously (i.e., effect of concurrent stress). Dependent variables in all models included prior levels as control variables, thereby permitting the examination of factors associated with change over time. The second aim of this study sought to determine whether participation in ProSAAF could protect couple functioning and personal health from the negative effects of stress (see Figure 1b).
FIGURE 1.
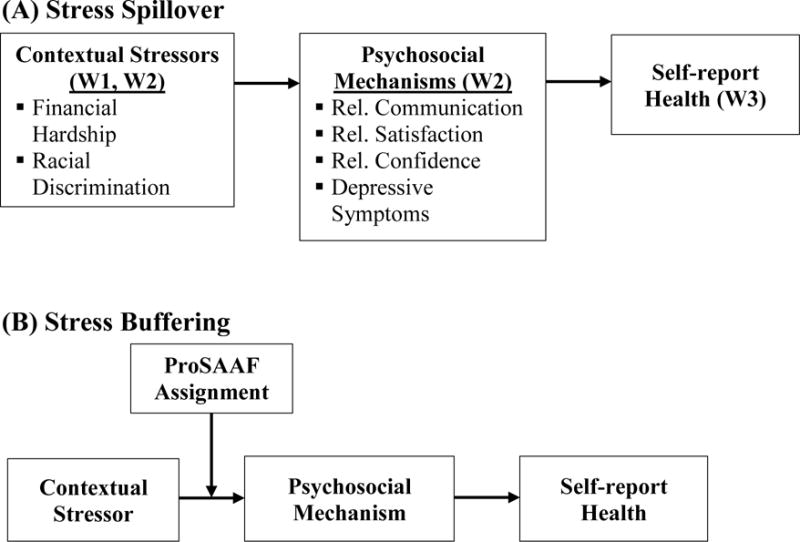
Conceptual Models (control variables, including prior levels of dependent variables, not shown).
Method
Participants
Participants in the study were African American couples2 with at least one pre- or early adolescent youth residing in the home. All participants lived in small towns and communities in Georgia where poverty rates are among the highest in the nation and unemployment rates are above the national average (DeNavas-Walt & Proctor, 2014). Of the random sample of 346 families, 63% were married; the mean length of marriage was 9.97 years (range 0 – 56 years). Unmarried couples had been living together for an average of 6.73 years (range 0.25 – 23). Approximately 25% of the men and 19% of the women had been previously married. Men’s mean age was 39.89 years (SD = 9.62; range 21 – 83) and women’s mean age was 36.51 (SD = 7.44; range 23 – 73). Men’s median education level was high school or GED (ranging from less than grade 9 to a doctorate or professional degree) and women’s median education level was some college or trade school (ranging from less than grade 9 to a master’s degree). The majority of men (76% [66% full-time]) and women (60% [46% full-time]) reported full- or part-time employment. Median monthly pre-tax income was $1,400 (range $1 – $7,500) for men and $1,200 (range $1 – $10,000) for women. The incomes of 53% of the families were below 100% of the poverty line, and incomes of 69% of the families were below 150% of the poverty line. The number of children residing in the home ranged from 1 to 8, with a mean of 2.96.
Procedures
Recruitment and implementation procedures for the ProSAAF RCT are provided in detail elsewhere (Barton et al., 2017). Briefly, families were recruited by mail and phone from lists provided by local schools and through the use of flyers and advertisements posted in their communities. Those who responded were screened for eligibility. At Wave 1 (W1), project staff visited couples’ homes, explained the study in more detail, and obtained informed consent from adult participants and informed assent from youth. Parents and youth then completed the W1 assessments on laptop computers. Families were randomly assigned to the control or treatment condition following the completion of W1 measures. Families were then visited for Wave (W2) and Wave (W3) assessments an average of 9.4 and 17.0 months after W1, respectively. Participant progress through the study is illustrated in the CONSORT flowchart in Figure 2. Adults were compensated with a $50 check and youth with a $20 gift card at each wave of data collection. Attrition at W2 was 14% for women and 19% for men; at W3, it was 13% for women and 20% for men. Attrition analyses indicated that retained men and women did not differ from those who left the study on primary indicators of family processes, sociodemographic variables, or treatment assignment. This lack of attrition bias was evident at both W2 and W3. All procedures were approved by the institutional review board of the sponsoring institution.
FIGURE 2.
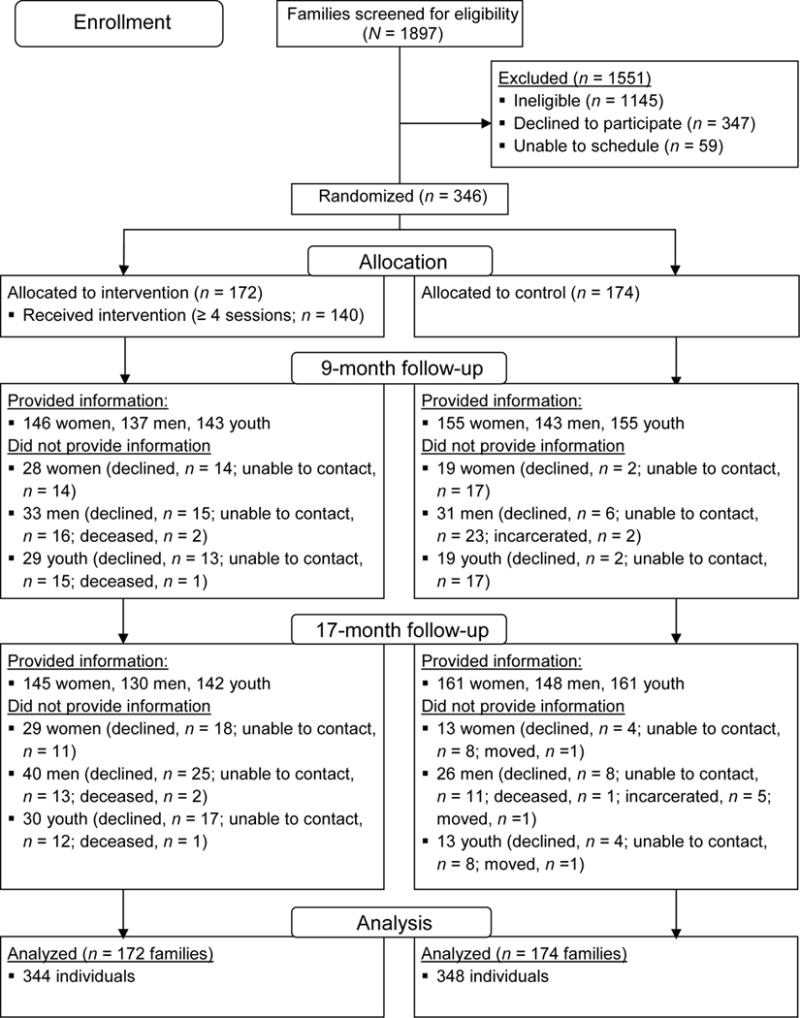
Consort Diagram
The ProSAAF program
ProSAAF comprises six 2-hour sessions and uses an in-home delivery format to facilitate participation. Sessions focused primarily on parents, with the target youth involved in the final 30 minutes of each session. Within each session, time was devoted to both couple issues and parenting/coparenting issues. Facilitators came from local communities and received 40 hours of training in program content, facilitation and delivery methods, and adherence to the program manual (see Barton et al., unpublished data for additional details).
Each session began with a focus on a particular domain of stress experienced by African American couples, and couples were instructed in cognitive and behavioral techniques for handling stressors. Session content then transitioned into encouraging the development of other protective couple and parenting processes. In each session, particular emphasis was given to partners’ use of enhanced communication in response to daily stressors and engagement in pro-relationship behaviors and cognitions. Two booster sessions were offered at approximately 3 and 9 months after program completion to reinforce program material (corresponding to approximately 2 months before W2 and 4 months before W3).
Program attendance
Of the 172 families assigned to the intervention condition, 81% (n = 139) completed all six sessions. Nine percent (n = 16) of families attended 0 sessions, 9% (n = 16) attended 1 - 3 sessions, and 1% (n = 1) attended five sessions. With respect to booster session attendance, 73% (n = 126) of intervention families participated in booster session 1 and 59% (n = 101) participated in booster session 2.
Program fidelity
All sessions were audiotaped to allow implementation to be monitored. Twenty five percent (n = 220) of all sessions were coded for adherence to intervention guidelines, and all facilitators were assessed at least once. Of the audiotapes reviewed, 10% (n = 22) were coded by more than one rater. The intraclass correlation between raters was .94. Mean fidelity adherence across facilitators was 91% (SD = 9.0%).
Control group
Couples in the control group were assessed on the same schedule as the intervention group. The book, “12 Hours to A Great Marriage” (Markman, Stanley, Blumberg, Jenkins, & Whaley, 2004) and an accompanying workbook were mailed to control couples after the baseline assessment. Thus, this group represented an information-only control condition.
Measures
Financial hardship
Couples’ levels of financial hardship were assessed at W1 and W2 using a two- item indicator of inability to make ends meet that has appeared in previous studies of family economic pressure (e.g., Masarik et al., 2016). The two items were “How much difficulty have you had paying your bills?” (1 = a great deal of difficulty to 5 = no difficulty at all; [reverse coded]) and “Generally, at the end of each month did you end up with…?" (1 = more than enough to 5 = not enough to make ends meet).
Racial discrimination
Everyday experiences of perceived racial discrimination were assessed at W1 and W2 using 9 items from the Racism and Life Experiences Scale (Harrell, 2000). This measure asks participants to report the frequency with which they experienced several racial stressors over the last 6 months (1 = never to 4 = frequently). Sample items included: “Have you been treated rudely or disrespectfully because of your race?” and “Have you been called a name or harassed because of your race?”. At W1, the majority of men (87.5%) and women (81.3%) reported at least one discriminatory experience in the last 6 months.
Relationship communication
Participants’ reports of effective communication at W1 and W2 were measured using an eight-item version of the Communication Skills Test (Jenkins & Saiz, 1995). The items assessed effective communication patterns between partners. Sample items included, “When discussing an issue, my mate and I both take responsibility to keep us on track” and “When [partner name] and I discuss relationship issues, I show that I am listening by repeating what I heard”. Response options for seven of the items ranged from 1 (almost never) to 7 (almost always) and, for the 8th item, from 1 (never) to 4 (very often or always). Individual items were standardized prior to computing the composite score.
Relationship satisfaction
Relationship satisfaction was measured at W1 and W2 using the Quality of Marriage Index (Norton, 1983). This six-item scale measures global perceptions of relationship satisfaction using a scale ranging from 1 (strongly disagree [questions 1-5] and very unhappy [question 6]) to 5 (strongly agree [questions 1-5] and perfectly happy [question 6]). A sample item is, “[Partner name] and I have a good relationship.”
Relationship confidence
Relationship confidence was measured at W1 and W2 using 4 items from the Relationship Confidence Scale (RCS; Stanley, Hoyer, & Trathen, 1994). The RCS assesses partners’ confidence in the future of their relationship, and similar versions of the current scale have demonstrated good reliability and predictive validity (e.g., Whitton et al., 2014). Response options ranged from 1 (strongly disagree) to 5 (strongly agree). The items comprising this measure are: “I am very confident when I think of my future with [partner name]”, “I believe [partner name] and I can handle whatever conflicts arise in the future”, “I feel good about my and my partner’s prospects to make this relationship work for a lifetime”, and “My partner and I have the skills a couple needs to make a relationship last.”
Depressive Symptoms
Individuals’ depressive symptoms were measured at W1 and W2 using 20 items from the Center for Epidemiological Studies Depression scale (Radloff, 1977), a commonly used measure in community samples for gauging individuals’ mental health. Sample items include “In the past week, how often did you feel depressed?” and “In the past week, How often did you think your life was a failure?”. Response options ranged from 0 (Rarely or none of the time [0-1 day]) to 3 (Most or all of the time [6-7 days]).
Self-reported health
Individuals reported their health problems at Waves 2 and 3 using items from the General Health Perceptions subscale of the RAND 36-Item Short-Form Health Survey (Hays, Sherbourne, & Mazel, 1993). The 4-item subscale assessed perceptions of current health status. Response options ranged from 1 (strongly disagree) to 4 (strongly agree). Sample items include, “I am as healthy as anybody I know” and “I seem to get sick a little easier than other people” (reverse scored).
Descriptive statistics, range, and reliability information for study variables as well as equivalence analyses are presented in Table 1. Individual items were summed together to create each composite construct. No differences at baseline3 emerged between treatment and control conditions for family characteristics or study variables, except for financial hardship, wherein the intervention group had slightly higher scores. As financial hardship was already included in all analytic models, no additional alterations to models were required.
Table 1.
Descriptive Statistics and Equivalence of Treatment and Control Groups (N = 692 individuals)
| Treatment (n =344)
|
Control (n =348)
|
Test Statisticd |
Entire Sample
|
||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Range (W1) | Alpha (W1, W2) | ||
| Demographic Characteristics | |||||||
| Marrieda | 0.65 | NA | 0.61 | NA | 0.58 | — | — |
| Children in home | 3.12 | 1.54 | 2.86 | 1.43 | 0.13 | 1 – 12 | — |
| Incomeb | 1.71 | 1.47 | 1.60 | 1.33 | 0.72 | 0 – 10 | — |
| Education | 5.48 | 1.84 | 5.46 | 1.66 | 0.15 | 1 – 10 | — |
| Age | 38.12 | 8.64 | 38.25 | 8.87 | 0.15 | 21 – 83 | — |
| Study Variables | |||||||
| Financial hardship | 5.56 | 2.03 | 5.26 | 1.90 | 1.98* | 2.00 – 10.00 | .69, .70 |
| Racial Discrimination | 16.39 | 6.00 | 16.11 | 6.21 | 0.59 | 9.00 – 36.00 | .91, .92 |
| Relationship communication | −0.07 | 5.74 | 0.07 | 5.32 | 0.28 | −15.80 – 9.76 | .84, .90 |
| Relationship satisfaction | 24.48 | 4.92 | 25.14 | 4.03 | 1.36 | 6.00 – 30.00 | .92, .96 |
| Relationship confidence | 17.30 | 3.34 | 17.61 | 2.94 | 1.18 | 4.00 – 20.00 | .89, .92 |
| Depressive Symptoms | 11.84 | 7.95 | 11.28 | 7.73 | 1.14 | 0.00 – 48.00 | .82, .83 |
| Self-reported health c | 12.14 | 2.40 | 12.30 | 2.26 | 0.81 | 5.00 – 16.00 | .69, .68 |
Note. W1 = Wave 1; W2 = Wave 2. W3 = Wave 3.
1 = Married (0 = Cohabiting).
Monthly income divided by 1,000.
Not assessed at W1; wave 2 assessment for descriptive statistics, and W2 and W3 for Cronbach’s alpha (n = 579).
T-test for continuous and ordinal variables; chi-square cross-tab statistic for binary variables.
p ≤ .05, two-tailed
Plan of Analysis
Analyses were conducted using path analysis in Mplus version 7.4 (Muthén & Muthén, 1998-2015). As there were no gender-specific hypotheses, analyses were executed at the individual level, with individuals nested within dyads to account for the interdependence between partners. Sex was included as a control variable in all analyses. We first examined the presence of stress spillover within the control group. These analyses were designed to document the naturally occurring associations among contextual stressors, inter- and intrapersonal psychosocial mechanisms (i.e., communication, satisfaction, confidence, depressive symptoms), and physical health in a community sample of African Americans. We calculated indirect effects using 2,000 bootstrapped samples with bias-corrected confidence intervals, consistent with recommendations of Preacher and Hayes (2008). With four different psychosocial mechanisms (i.e., communication, satisfaction, confidence, and depressive symptoms) and two different time points of stress (W1 and W2), a total of eight models were run. For each mechanism, indirect effects on health were calculated from financial hardship and from racial discrimination.
For significant indirect effect pathways, a second set of analyses were conducted to test whether participation in ProSAAF can alter or offset spillover associations identified in the control group, thereby constituting a constructed resilience resource. All interaction analyses were executed based on conventions recommended by Aiken and West (1991). Interactions were interpreted through the plotting the psychosocial mechanism (e.g., relationship satisfaction) by centered contextual stressor (e.g., financial hardship) according to prevention status, controlling for other variables in the model. Missing data (approximately 13% of all variables used in modeling) were handled using full information maximum likelihood estimation.
Results
Stress Spillover Effects
Our first set of analyses were designed to assess stress spillover in the control group by examining: (a) the effects of financial hardship and racial discrimination on changes in relationship communication, satisfaction, confidence, and depressive symptoms between W1 and W2; and (b) the effect of each of these intervening variables at W2 on changes in health between W2 and W3. Table 2 summarizes results for prospective (W1) stress spillover (top half of table) and contemporaneous (W2) stress spillover (bottom half of table). For prospective stress effects (Models 1-4), financial hardship at W1 was not associated with any W2 outcomes; similarly, exposure to racial discrimination at W1 was not associated any W2 outcomes. For contemporaneous stress effects (Models 5-8), financial hardship at W2 was associated with changes in relationship communication, satisfaction, confidence, and depressive symptoms, with greater financial hardship predicting declines in relationship communication (B[β] = −.41 [−.11], p = .04), relationship satisfaction (B[β] = −.35 [−.15], p = .03), relationship confidence (B[β] = −.33 [−.17], p < .01), and increases in depressive symptoms (B[β] = .82 [.18], p < .07). Exposure to racial discrimination at W2 was associated with changes in depressive symptoms (B[β] = .20 [.15], p < .01), but not relationship processes. Hence, these results were more supportive of the effect of current, rather than prior, levels of contextual stressors, particularly financial hardship, predicting changes in couple processes and individuals’ mental health.
Table 2.
Summary of stress spillover analyses within control group (N = 297 – 348 individuals)
| W2 Mechanism | Communication
|
Satisfaction
|
Confidence
|
Dep. Symptoms
|
||||
|---|---|---|---|---|---|---|---|---|
| B | se | B | se | B | se | B | se | |
| Prospective Spillover | Model 1 | Model 2 | Model 3 | Model 4 | ||||
| Dependent Variable: W2 Mechanism | ||||||||
| Financial Hardship (W1) | −.24 | .18 | −.19 | .15 | −.21 | .13 | .36 | .26 |
| Racial Discrimination(W1) | −.10 | .05 | −.01 | .80 | −.02 | .03 | .09 | .06 |
| Sex | .79 | .58 | .47 | .41 | .34 | .33 | .10 | .73 |
| Mediating Variable (W1) | .71** | .06 | .59** | .11 | .47** | .11 | .63** | .07 |
| Dependent Variable: W3 Self-reported Health | ||||||||
| W2 Mechanism | .03 | .02 | .05* | .02 | .12** | .03 | −.02 | .01 |
| Financial Hardship (W1) | −.06 | .06 | −.05 | .39 | −.04 | .06 | −.04 | .06 |
| Racial Discrimination(W1) | −.03* | .02 | −.03* | .02 | −.03 | .02 | −.03 | .02 |
| Sex | .12 | .20 | .08 | .20 | .07 | .19 | .12 | .20 |
| Self-reported health (W2) | .61* | .05 | .61** | .00 | .59** | .05 | .60** | .05 |
|
| ||||||||
| Contemporaneous Spillover | Model 5 | Model 6 | Model 7 | Model 8 | ||||
| Dependent Variable: W2 Mechanism | ||||||||
| Financial Hardship (W2) | −.41* | .20 | −.35* | .16 | .33** | .12 | .82** | .23 |
| Racial Discrimination (W2) | −.08 | .05 | −.05 | .04 | −.01 | .03 | .20** | .07 |
| Sex | .61 | .59 | .41 | .43 | .20 | .34 | .32 | .68 |
| Baseline | .71** | .06 | .58** | .10 | .46** | .10 | .56** | .05 |
| Dependent Variable: W3 Self-reported Health | ||||||||
| W2 Mechanism | .03 | .02 | .05* | .02 | .12** | .03 | −.03 | .02 |
| Financial Hardship (W2) | −.03 | .06 | −.01 | .06 | −.01 | .06 | −.00 | .07 |
| Racial Discrimination (W2) | −.02 | .02 | −.02 | .02 | −.02 | .02 | −.02 | .02 |
| Sex | .07 | .20 | .06 | .20 | .04 | .02 | .09 | .20 |
| Self-reported health (W2) | .63** | .05 | .63** | .05 | .59** | .05 | .61** | .05 |
Note. W1 = Wave 1; W2 = Wave 2. W3 = Wave 3. Model fit statistics: All CFI > 0.94, RMSEA ≤ = 0.09, p > .10. Complete fit statistics available from first author. Individual correlations between predictor variables not detailed for clarity purposes.
p ≤ .01;
p ≤ .05 (two-tailed tests).
For effects of intervening variables on self-report health, results indicated that greater levels of W2 relationship satisfaction (B[β] = .05 [.12], p = .01) and W2 relationship confidence (B[β] = .12 [.19], p < .01) were each associated positively with changes in self-reported health from W2 to W3; W2 relationship communication and W2 depressive symptoms did not predict change in self-reported health. Indirect effect analyses are summarized in Table 3. Two significant pathways were confirmed, consistent with findings from Table 2. Specifically, indirect effects were observed from W2 financial hardship to changes in physical health through relationship satisfaction and through relationship confidence. No other significant indirect effects were detected. In addition, to further clarify the unique contribution of W2 relationship confidence and relationship satisfaction on self-reported health, we ran a post hoc dual mediation model including both constructs. Results indicated that relationship confidence (B [β] = 0.14 [.22], se=.11, p <.01), but not satisfaction (B [β] = −0.02 [-.05], se=.03, p = .46), continued to exhibit a significant effect on W3 self-reported health. The total indirect effect through both mediators was significant (IE = −.029, 95% CI [−.071, −.009]); because of the attenuation of indirect effects stemming from correlated mediators, result interpretation focuses on the total, rather than specific, indirect effect across the set of mediators (Preacher & Hayes, 2008). Pairwise contrasts of these two specific indirect effects, however, indicated the magnitude of the specific indirect effect (SIE) were significantly different (SIE for relationship confidence: −.035, 95% CI [−.090, −.008]; SIE for relationship satisfaction: .007 [−.010, .042]; contrast = −.042, 95%CI [−.126, −.004]). With these stress spillover pathways identified, we then tested the ability of participation in ProSAAF to interrupt this pathway.
Table 3.
Summary of indirect effects on self-reported health within control group (N = 297 – 348 individuals)
| Psychosocial Mechanism
|
||||||||
|---|---|---|---|---|---|---|---|---|
| Communication
|
Satisfaction
|
Confidence
|
Dep. Symptoms
|
|||||
| IE | 95% CI | IE | 95% CI | IE | 95% CI | IE | 95% CI | |
| Prospective Stress Spillover | ||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
| Financial Hardship (W1) | −.007 | [−.030, .002] | −.009 | [−.031, .002] | −.025 | [−.057, .008] | −.007 | [−.023, .008] |
| Racial Discrimination (W1) | −.003 | [−.011, .000] | .000 | [−.005, .004] | −.002 | [−.011, .004] | −.010 | [−.031, .011] |
| Contemporaneous Stress Spillover | ||||||||
| Model 5 | Model 6 | Model 7 | Model 8 | |||||
| Financial Hardship (W2) | −.013 | [−.040, .001] | −.018 | [−.050, −.002] | −.040 | [−.074, −.006] | −.020 | [−.054, .000] |
| Racial Discrimination (W2) | −.003 | [−.010, .000] | −.002 | [−.010, .001] | −.001 | [−.008, .006] | .001 | [.000, .002] |
Note. W1 = Wave 1; W2 = Wave 2. Boldface type indicating 95% confidence interval (CI) for indirect effect (IE) does not contain zero. 2,000 bootstrapped samples.
ProSAAF Stress-Buffering Effect
The second set of analyses used data from the entire sample to assess the ability of the ProSAAF program to buffer individuals from the negative spillover effect of financial hardship and racial discrimination. Interaction effects were tested for each of the two significant indirect effects identified in Table 3. Results, summarized in Table 4, indicated a significant Financial Hardship × ProSAAF interaction for individuals’ relationship confidence (B[β] = .40 [.17], p < .01), but not for individuals’ relationship satisfaction (B[β] = .35 [.21], p = .09).
Table 4.
– Summary of models examining ProSAAF stress-buffering effects
|
Rel. Satisfaction (N=578)
|
Rel. Confidence (N=692)
|
|||||
|---|---|---|---|---|---|---|
| B (β) | se | p | B (β) | se | p | |
| Dependent Variable: Wave 2 Mechanism | ||||||
| Financial Hardship | −0.37 (−.14)* | .15 | .01 | −0.33 (−.19)** | .12 | <.01 |
| ProSAAF a | −0.78 (−.08) | 1.12 | .48 | 0.69 (.10)* | .28 | .02 |
| Financial Hardship × ProSAAF | 0.35 (.21) | .21 | .09 | 0.40 (.17)** | .15 | <.01 |
| Racial Discrimination | −0.03 (−.04) | .03 | .27 | −0.01 (−.01) | .02 | .72 |
| Sex | 0.46 (.05) | .30 | .13 | 0.28 (.04) | .24 | .24 |
| W1 Mechanism | 0.55 (.49)** | .06 | .00 | 0.43 (.40)** | .07 | .00 |
| Dependent Variable: W3 Self-report Health | ||||||
| W2 Mechanism | 0.04 (.09)** | .02 | .01 | 0.10 (.14)** | .02 | <.01 |
| Financial Hardship | 0.00 (.00) | .06 | .99 | −0.00 (−.00) | .06 | .98 |
| ProSAAFa | −0.26 (−.01) | .42 | .95 | −0.09 (−.02) | .15 | .56 |
| Financial Hardship × ProSAAF | −0.01 (−.02) | .08 | .88 | −0.02 (−.01) | .08 | .79 |
| Racial Discrimination | −0.02 (−.05) | .01 | .15 | −0.02 (−.05) | .01 | .14 |
| Sex | 0.19 (.04) | .15 | .21 | 0.18 (.04) | .15 | .21 |
| Self-report Health (W2) | 0.61 (.65)** | .06 | .00 | 0.63 (.64)** | .04 | .00 |
Note:
1 = ProSAAF assignment. Individual correlations between predictor variables not detailed for clarity purposes. Model fit statistics: Relationship Satisfaction Model: χ2(2) = 2.31; p = .31. CFI = 1.00. RMSEA = 0.02, p = .70. Relationship Confidence Model: χ2(7) = 21.78; p < .01. CFI = 0.96. RMSEA = 0.06, p = .33.
p ≤ .01;
p ≤ .05 (two-tailed tests).
To better interpret and illustrate the significant interaction involving relationship confidence, we plotted estimated levels of relationship confidence by levels of financial hardship for ProSAAF and control participants. Plots of these interactions are presented in Figure 3. Findings indicated that greater levels of financial hardship were associated with corresponding declines in relationship confidence, but only among individuals in the control group (b = −.33, p < .01). Relationship confidence among individuals assigned to the ProSAAF condition did not vary with higher levels of financial hardship (b = .07, p = .46). Thus, the stress-buffering effect of ProSAAF participation on individuals’ relationship confidence was confirmed.
FIGURE 3.
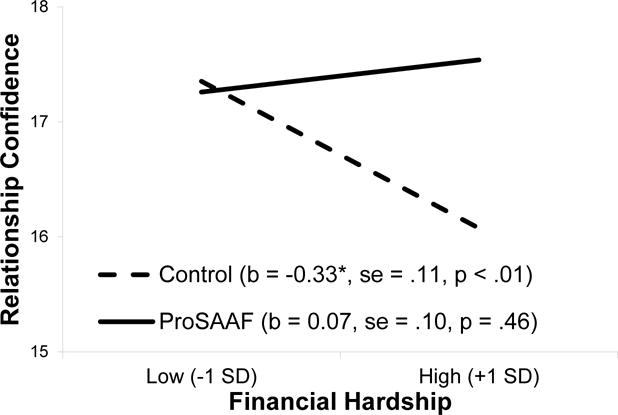
The effect of financial hardship by intervention status on relationship confidence.
Lastly, conditional indirect effect analyses were conducted to quantify whether ProSAAF participation interrupted associations among financial hardship, relationship confidence, and self-reported health. As identified previously, a significant indirect effect emerged for the control group (IE = −.032, 95% Confidence Interval [−.069, −.012]), indicating that relationship confidence functioned as an intervening variable linking financial hardship to changes in physical health. However, this indirect effect was not significant for individuals in the ProSAAF condition (IE = .007, 95% Confidence Interval [−.011, .032]. In addition, we conducted multi-group comparisons by constraining the indirect effect linking financial hardship, relationship confidence, and self-reported health to be equivalent across treatment and control groups. The constrained model demonstrated significantly worse fit than the baseline (unconstrained) model, Δχ2(2) = 9.748, p < .01, supporting the presence of group differences for this indirect effect.4
Discussion
African Americans in the rural South reside in some of the poorest areas of the US and are at an elevated risk for a variety of health disparities (DeNavas-Walt & Proctor, 2014; Hartley, 2004). Given the deleterious effects of economic hardship and other contextual stressors on physical health, scientists have endeavored to understand the pathways through which this cascade of effects occurs and to identify effective ways to prevent it. The current study was designed to inform this area of research by exploring (a) the intermediate role of relationship processes and depressive symptoms in linking financial hardship to worsened physical health among African American couples, and (b) prevention programming designed to strengthen couples’ relationship quality as a means to protect rural African Americans’ relational and physical health from the negative effects of financial hardship.
Results from stress spillover models confirm the importance of considering couple processes as mechanisms linking stress to individuals’ health, as other studies have similarly suggested (e.g., Lei et al., 2016). While the significant indirect effect of relationship satisfaction has appeared previously (Lei et al., 2016), the present study uniquely highlights the ability of relationship confidence to transmit this effect similarly. Thus, in addition to its effect on mental health (Whitton et al., 2007; Whitton et al., 2014), current results support the physical health benefits of relationship confidence and extend prior research at the individual-level of the importance of individuals’ sense of self-efficacy and hopefulness of the future for individuals’ health (Tindle et al., 2012). Moreover, the pattern of results suggests the value of increased attention on relationship confidence and its potential role in couple resilience. The current investigation provides, to our knowledge, the first demonstration that relationship confidence may play an important role linking financial hardship to physical health and may be a malleable target for enhancement through preventive interventions. Although the precise underlying factors that account for how relationship confidence exerts physical health benefit are beyond the scope of the current study, we speculate that less felt insecurity, less worry about the partner leaving, and less activation of negative attachment schemas may confer this beneficial effect for individuals’ physical well-being.
The significance on concurrent, but not prior, levels of stress predicting change in couple and individual well-being informs research on the temporal effects of stress. These effects also introduce some questions regarding previous studies examining the prospective associations between stress and couple functioning that do not control for prior levels of couple functioning (e.g., Parke et al., 2004; Robila & Krishnakumar, 2005). Additional research continues to be needed in this area, including that which considers effects resulting from chronic levels of contextual stressors as well as change in levels of contextual stress over time.
Spillover effects from financial hardship were documented across all three couple processes as well as depressive symptoms. Racial discrimination experiences, in contrast, were only associated with increases in depressive symptoms. Despite cross-sectional associations identified elsewhere (Lavner, Barton, Bryant, & Beach, unpublished data), current results suggest the longitudinal effect of racial discrimination on relationship functioning (at least with respect to the constructs of communication, satisfaction, and confidence) may be more indirect than direct, resulting from increases in individuals’ depressive symptoms. Given the overall lack of research in this area, identifying ways that couples respond to, and are influenced by each partner’s experience of discrimination remains an important focus for future research.
With respect to stress buffering effects, a significant Financial Hardship × ProSAAF interaction was evident for relationship confidence but not other constructs with stress spillover effects. Simple slope analyses showed the nature of interaction to be consistent with a stress-buffering effect. Thus, in addition to main effects on couples’ outcomes (Barton et al., unpublished data), current results support the capacity of ProSAAF to protect relationships against declines attributable to elevated levels of financial hardship and, in this manner, function as a “constructed resilience resource” (Brody et al., 2015). Further, this moderation effect is consistent with one of the primary aims of the program, namely fostering couples’ beliefs in the longevity of their relationship despite facing various contextual challenges and hardships. Such results also importantly indicate that the progression from financial hardship to reductions in relationship confidence and subsequent general health is not immutable.
Findings from this study provide various implications for both clinicians and practitioners. First, underscoring prior recommendations (e.g., Neff, 2012; Tesser & Beach, 1998), results emphasize the importance of fostering couples’ awareness of the spillover effects of stress onto their relationship, particularly in light of research suggesting individuals’ tendency to not acknowledge the effect of contextual factors on relationship outcomes (Berscheid, Lopes, Ammazzalorso, & Langenfeld, 2001). Second, research and practice can continue to devote greater attention to fostering partners’ confidence in their relationship. The shift in attention to constructs apart from the predominant focus on relationship satisfaction appears increasingly warranted given the potential for focusing on relationship satisfaction to undermine (rather than bolster) efforts to promote healthy relationships. As Barton and Bishop (2014) note, by focusing on the emotional fulfillment and satisfaction of individual spouses and encouraging participants to evaluate their marriage similarly, researchers may encourage a mindset within individuals that directs focus away from accessions and accommodations to the other and towards expectations for personal self-fulfillment. Ideals of self-fulfillment and self-satisfaction in marriage tend to undermine, rather than bolster, fundamental constructs and practices needed for healthy, stable marriages (Fowers, 1998). Third, at a time when the appropriateness of couple-focused prevention programs for low-income couples are being questioned (Lavner, Karney, & Bradbury, 2015), direct and stress-buffering effects of ProSAAF highlight the ability of a culturally sensitive, contextually focused cognitive-behavioral therapy-approach to prevention to promote the strength and well-being of low income and minority couples exposed to number contextual stressors and provide a model for future interventions.
Several limitations of the current investigation are noted. First, all measures were based on self-reports. Future research with home-based observations of change in interactions and more extensive assessments of individuals’ physical health, including biomarkers of health-related processes and direct physical examination, would be valuable. Second, financial hardship was assessed in terms of a general inability to make ends meet. Financial hardship can take various other subjective and objective forms, and patterns of spill over on couple and family dynamics may differ depending on the way financial hardship is assessed. Third, individuals in the ProSAAF condition reported higher levels of financial hardship than individuals in the control condition; hence, the buffering effect of ProSAAF may be more evident for more financially disadvantaged couples. Fourth, the current study only considered contextual stressors of financial hardship and racial discrimination. A variety of other factors, including unequal access to health care, community-level disadvantage, poverty, and segregation can also shape the health and well-being of rural African Americans and their families. Depending on the desired outcome of interest, interventions and social programs other than ProSAAF may be more pertinent for rural African Americans and the stressors they experience. However, current results do support the efficacy of ProSAAF in promoting relationship quality among low-income couples and continue research exploring of its effects on individual and family well-being.
These limitations notwithstanding, the present results highlight changes in couple processes through which contextual stressors influence physical health outcomes and indicate that a culturally specific, stress-spillover prevention program can protect rural African American couples’ relational and physical health from the negative spillover effects of financial hardship by enhancing relationship confidence. Future research focused on contextual stressors, relationship processes, and their interplay remains valuable for efforts to inform the etiology, and potential prevention, of health risks affecting rural African Americans.
Acknowledgments
The authors thank Eileen Neubaum-Carlan for her editorial assistance in the preparation of this article. Portions of this article were presented at the annual conference of the Society for Prevention Research, Washington, DC, in June 2017. We also thank the families for their willingness to participate in this research and staff at Center for Family Research for their assistance implementing this study.
Funding:
This study was funded in part by grants from the National Institute of Child Health and Human Development (grant number R01 HD069439) and from the National Institute on Drug Abuse (grant number P30 DA027827). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health
Footnotes
Given these mixed results concerning spousal support, there is some possibility that couple interventions designed to foster spousal support may inadvertently pose some iatrogenic effects for relationships (e.g., Rogge, Cobb, Lawrence, Johnson, & Bradbury, 2013).
Eligibility guidelines required the target child to be African American, but not both parents. Racial and ethnicity information was not assessed in surveys completed by participants. Notes from research staff indicated that two caregivers (from different families) were not African American. All participants were comfortable being identified as part of an African American family. No information is available to distinguish between African American and Black Caribbean participants. However, based on targeted county demographics and previous studies, the percentage of Black Caribbean participants in the current sample is likely very low to none.
Data on self-reported health were collected for the first time at Wave 2; these data are used in the comparison.
In addition to analyses constraining the overall indirect effect to be equivalent across treatment and control groups, we also conducted analyses comparing the baseline (unconstrained) model to a model in which just the effect of financial hardship on relationship confidence was equivalent across the two groups and a model in which just the effect of relationship confidence on self-reported health was equivalent across the two groups. There was a significant worsening in model fit when constraining the effect of financial hardship on relationship confidence (Δχ2(1) = 8.771, p < .01), but not when constraining the effect of relationship confidence on health (Δχ2 (1) = 1.03, p = .31). Hence, results indicate the group difference in the overall indirect effect was attributable to group differences in the effect of financial hardship on relationship confidence, consistent with Figure 3.
References
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Thousand Oaks, CA: Sage; 1991. [Google Scholar]
- Barton AW, Beach SRH, Lavner JA, Bryant CM, Kogan SM, Brody GH. Is Communication a Mechanism of Relationship Education Effects Among Rural African Americans? Journal of Marriage and Family. 2017;79:1450–1461. doi: 10.1111/jomf.12416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barton AW, Beach SRH, Wells AC, Ingels JB, Corso PS, Sperr MC, Brody GH. The Protecting Strong African American Families Program: A Randomized Controlled Trial with Rural African American Couples. Manuscript submitted for publication. doi: 10.1007/s11121-018-0895-4. unpublished data. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barton AW, Bishop RC. Paradigms, processes, and values in family research. Journal of Family Theory & Review. 2014;6(3):241–256. doi: 10.1111/jftr.12043. [DOI] [Google Scholar]
- Barton AW, Bryant CM. Financial Strain, Trajectories of Marital Processes, and African American Newlyweds’ Marital Instability. Journal of Family Psychology. 2016:657–664. doi: 10.1037/fam0000190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berscheid E, Lopes J, Ammazzalorso H, Langenfeld N. Causal attributions of relationship quality. New York: Cambridge University Press; 2001. [Google Scholar]
- Bodenmann G, Shantinath SD. The Couples Coping Enhancement Training (CCET): A new approach to prevention of marital distress based upon stress and coping*. Family Relations. 2004;53(5):477–484. doi: 10.1111/j.0197-6664.2004.00056.x. [DOI] [Google Scholar]
- Brock RL, Lawrence E. A longitudinal investigation of stress spillover in marriage: Does spousal support adequacy buffer the effects? Journal of Family Psychology. 2008;22(1):11–20. doi: 10.1037/0893-3200.22.1.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brody GH, Yu T, Beach SRH, Philibert RA. Prevention Effects Ameliorate the Prospective Association Between Nonsupportive Parenting and Diminished Telomere Length. Prevention Science. 2015;16(2):171–180. doi: 10.1007/s11121-014-0474-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryant CM, Wickrama KAS, Bolland J, Bryant BM, Cutrona CE, Stanik CE. Race matters, even in marriage: Identifying factors linked to marital outcomes for African Americans. Journal of Family Theory & Review. 2010;2(3):157–174. doi: 10.1111/j.1756-2589.2010.00051.x. [DOI] [Google Scholar]
- Caplan LJ, Schooler C. Socioeconomic status and financial coping strategies: The mediating role of perceived control. Social Psychology Quarterly. 2007;70(1):43–58. doi: 10.1177/019027250707000106. [DOI] [Google Scholar]
- Chen E, Miller GE. Socioeconomic Status and Health: Mediating and Moderating Factors. Annual Review of Clinical Psychology. 2013;9(1):723–749. doi: 10.1146/annurev-clinpsy-050212-185634. [DOI] [PubMed] [Google Scholar]
- Cohen S. Social Relationships and Health. American Psychologist. 2004;59(8):676–684. doi: 10.1037/0003-066X.59.8.676. [DOI] [PubMed] [Google Scholar]
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological bulletin. 1985;98(2):310–357. [PubMed] [Google Scholar]
- Conger RD, Elder GH., Jr . Families in troubled times. New York: Aldine De Grutyer; 1994. [Google Scholar]
- Cranford JA. Stress-buffering or stress-exacerbation? Social support and social undermining as moderators of the relationship between perceived stress and depressive symptoms among married people. Personal Relationships. 2004;11(1):23–40. doi: 10.1111/j.1475-6811.2004.00069.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeNavas-Walt C, Proctor BD. Income and poverty in the United States: 2013 (Current Population Reports P60-249) Washington, DC: U.S. Census Bureau; 2014. [Google Scholar]
- Falconier MK, Epstein NB. Couples experiencing financial strain: What we know and what we can do. Family Relations. 2011;60(3):303–317. doi: 10.1111/j.1741-3729.2011.00650.x. [DOI] [Google Scholar]
- Fowers BJ. Psychology and the Good Marriage. American Behavioral Scientist. 1998;41(4):516–541. doi: 10.1177/0002764298041004005. [DOI] [Google Scholar]
- Harrell SP. A multidimensional conceptualization of racism-related stress: Implications for the well-being of people of color. American Journal of Orthopsychiatry. 2000;70(1):42–57. doi: 10.1037/h0087722. [DOI] [PubMed] [Google Scholar]
- Hartley D. Rural Health Disparities, Population Health, and Rural Culture. American Journal of Public Health. 2004;94(10):1675–1678. doi: 10.2105/AJPH.94.10.1675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hays RD, Sherbourne CD, Mazel RM. The RAND 36-item health survey 1.0. Health Economics. 1993;2:217–227. doi: 10.1002/hec.4730020305. [DOI] [PubMed] [Google Scholar]
- Jenkins NH, Saiz CC. The Communication Skills Test. University of Denver; Denver, CO: 1995. Unpublished manuscript. [Google Scholar]
- Johnson MD, Anderson JR. The longitudinal association of marital confidence, time spent together, and marital satisfaction. Family Process. 2013;52(2):244–256. doi: 10.1111/j.1545-5300.2012.01417.x. [DOI] [PubMed] [Google Scholar]
- Kahn JR, Pearlin LI. Financial Strain over the Life Course and Health among Older Adults. Journal of Health and Social Behavior. 2006;47(1):17–31. doi: 10.1177/002214650604700102. [DOI] [PubMed] [Google Scholar]
- Lavner JA, Barton AW, Bryant CM, Beach SRH. Racial Discrimination and Relationship Functioning among African American Couples. Manuscript submitted for publication. Manuscript submitted for publication unpublished data. [Google Scholar]
- Lavner JA, Karney BR, Bradbury TN. New directions for policies aimed at strengthening low-income couples. Behavioral Science and Policy. 2015;1:13–24. [Google Scholar]
- Lei MK, Beach SRH, Simons RL, Barr AB, Cutrona CE, Philibert RA. Stress, relationship satisfaction, and health among African American women: Genetic moderation of effects. Journal of Family Psychology. 2016;30(2):221–232. doi: 10.1037/fam0000140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markman HJ, Rhoades GK. Relationship Education Research: Current Status and Future Directions. Journal of Marital and Family Therapy. 2012;38(1):169–200. doi: 10.1111/j.1752-0606.2011.00247.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markman HJ, Stanley SM, Blumberg S, Jenkins NH, Whaley C. Twelve Hours to a Great Marriage. San Francisco: Jossey-Bass; 2004. [Google Scholar]
- Masarik AS, Martin MJ, Ferrer E, Lorenz FO, Conger KJ, Conger RD. Couple Resilience to Economic Pressure Over Time and Across Generations. Journal of Marriage and Family. 2016;78(2):326–345. doi: 10.1111/jomf.12284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User’s Guide. 7th. Los Angeles, CA: Muthén & Muthén; 1998–2015. [Google Scholar]
- Neff LA. Putting marriage in its context: The influence of external stress on early marital development. In: Campbell L, Loving TJ, editors. Interdisciplinary research on close relationships: The case for integration. Washington, DC: APA Books; 2012. [Google Scholar]
- Norton R. Measuring marital quality: A critical look at the dependent variable. Journal of Marriage and Family. 1983;45(1):141–151. [Google Scholar]
- O’Neal CW, Arnold AL, Lucier-Greer M, Wickrama K, Bryant CM. Economic pressure and health and weight management behaviors in African American couples: A family stress perspective. Journal of Health Psychology. 2015;20(5):625–637. doi: 10.1177/1359105315579797. [DOI] [PubMed] [Google Scholar]
- Office of Minority Health. Diabetes and African Americans. 2016a Retrieved March 7, 2017, from https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=18.
- Office of Minority Health. Heart Disease and African Americans. 2016b Retrieved March 7, 2017, from https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=19.
- Parke RD, Coltrane S, Duffy S, Buriel R, Dennis J, Powers J, Widaman KF. Economic Stress, Parenting, and Child Adjustment in Mexican American and European American Families. Child Development. 2004;75(6):1632–1656. doi: 10.1111/j.1467-8624.2004.00807.x. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods. 2008;40(3):879–891. doi: 10.3758/brm.40.3.879. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES–D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1(3):385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- Randall AK, Bodenmann G. The role of stress on close relationships and marital satisfaction. Clinical Psychology Review. 2009;29(2):105–115. doi: 10.1016/j.cpr.2008.10.004. [DOI] [PubMed] [Google Scholar]
- Reed K, Duncan JM, Lucier-Greer M, Fixelle C, Ferraro AJ. Helicopter parenting and emerging adult self-efficacy: Implications for mental and physical health. Journal of Child and Family Studies. 2016;25(10):3136–3149. doi: 10.1007/s10826-016-0466-x. [DOI] [Google Scholar]
- Repetti R, Wang S-W, Saxbe D. Bringing It All Back Home: How Outside Stressors Shape Families’ Everyday Lives. Current Directions in Psychological Science. 2009;18(2):106–111. doi: 10.1111/j.1467-8721.2009.01618.x. [DOI] [Google Scholar]
- Robila M, Krishnakumar A. Effects of Economic Pressure on Marital Conflict in Romania. Journal of Family Psychology. 2005;19(2):246–251. doi: 10.1037/0893-3200.19.2.246. [DOI] [PubMed] [Google Scholar]
- Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital quality and health: A meta-analytic review. Psychological Bulletin. 2014;140(1):140–187. doi: 10.1037/a0031859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogge RD, Cobb RJ, Lawrence E, Johnson MD, Bradbury TN. Is skills training necessary for the primary prevention of marital distress and dissolution? A 3-year experimental study of three interventions. Journal of Consulting and Clinical Psychology. 2013;81(6):949–961. doi: 10.1037/a0034209. [DOI] [PubMed] [Google Scholar]
- Rutter M. Environmentally Mediated Risks for Psychopathology: Research Strategies and Findings. Journal of the American Academy of Child & Adolescent Psychiatry. 2005;44(1):3–18. doi: 10.1097/01.chi.0000145374.45992.c9. http://dx.doi.org/10.1097/01.chi.0000145374.45992.c9. [DOI] [PubMed] [Google Scholar]
- Slatcher RB. Marital Functioning and Physical Health: Implications for Social and Personality Psychology. Social and Personality Psychology Compass. 2010;4(7):455–469. doi: 10.1111/j.1751-9004.2010.00273.x. [DOI] [Google Scholar]
- Stanley SM, Hoyer L, Trathen DW. The Confidence Scale. University of Denver; Denver, CO: 1994. Unpublished manuscript. [Google Scholar]
- Tesser A, Beach SRH. Life events, relationship quality, and depression: An investigation of judgment discontinuity in vivo. Journal of Personality and Social Psychology. 1998;74(1):36–52. doi: 10.1037/0022-3514.74.1.36. [DOI] [PubMed] [Google Scholar]
- Tindle H, Belnap BH, Hum B, Houck PR, Mazumdar S, Scheier MF, Rollman BL. Optimism, Response to Treatment of Depression, and Rehospitalization After Coronary Artery Bypass Graft Surgery. Psychosomatic medicine. 2012;74(2):200–207. doi: 10.1097/PSY.0b013e318244903f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitton SW, Olmos-Gallo PA, Stanley SM, Prado LM, Kline GH, St Peters M, Markman HJ. Depressive Symptoms in Early Marriage: Predictions From Relationship Confidence and Negative Marital Interaction. Journal of Family Psychology. 2007;21(2):297–306. doi: 10.1037/0893-3200.21.2.297. [DOI] [PubMed] [Google Scholar]
- Whitton SW, Rhoades GK, Whisman MA. Fluctuation in relationship quality over time and individual well-being: Main, mediated, and moderated effects. Personality and Social Psychology Bulletin. 2014;40(7):858–871. doi: 10.1177/0146167214528988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams D, Mohammed S. Discrimination and racial disparities in health: evidence and needed research. Journal of Behavioral Medicine. 2009;32(1):20–47. doi: 10.1007/s10865-008-9185-0. [DOI] [PMC free article] [PubMed] [Google Scholar]