

Description
A 56-year-old man presented with acute left-sided chest pain at rest with associated dyspnoea. His heart rate was 35 beats/min and ECG revealed a complete heart block. A temporary cardiac pacing was implemented on the right side via transcutaneous leads. He was also diagnosed with non-ST elevation myocardial infarction due to raised cardiac enzymes and was managed with medical therapy. The pacemaker was removed after 3 days when he reverted to sinus rhythm. Coronary angiogram was subsequently performed and revealed a critically obstructed triple coronary vessel disease. Echocardiography revealed an ejection fraction of 40%, competent valves and normal chamber size. Coronary artery bypass graft (CABG) surgery was performed via median sternotomy. Interestingly, there were no innominate veins identified intraoperatively and a dilated coronary sinus was seen on transoesophageal echocardiography. Cardiopulmonary bypass was initiated following aortic and two-stage right atrial venous cannulation. The heart was cooled and intentionally stopped by antegrade cardioplegia. On lifting the heart, a left superior vena cava was identified adjacent to the left atrial appendage (figure 1). Two vein grafts were grafted to the posterior descending artery and distal left circumflex. The left internal mammary artery harvested was grafted to left anterior descending artery.
Figure 1.
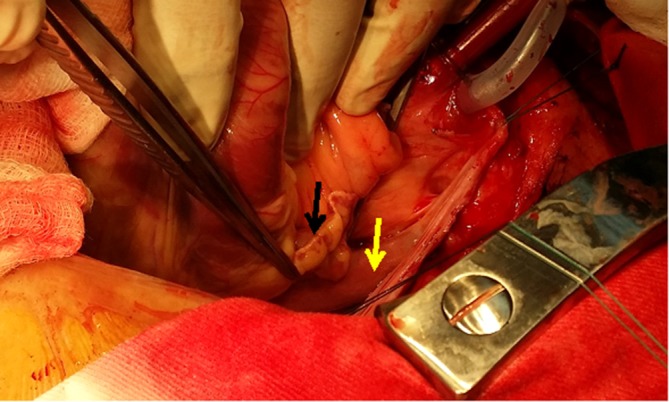
Picture showing tip of the forceps pointing on the left superior vena cava (yellow arrow) with the left atrial appendage (black arrow) just adjacent to it.
Persistent left superior vena cava (PLSVC) is a rare congenital vascular anomaly due to the failure of left superior cardinal vein caudal to the innominate vein to regress in utero.1 2 The incidence of PLSVC is 0.3%. It is usually asymptomatic and is an incidental finding on cardiac catheterisation or echocardiography.3 Two-thirds of such case is associated with the absence of innominate vein.1 In rare cases, the left SVC drains into left atrium which is usually associated with some desaturation and possible paradoxical embolism.
For patients undergoing CABG surgery, the recognition or failure to recognise the left SVC would be of no dire consequences. It is true also for most valve surgery which is performed with a single venous cannula. The PLSVC is important when bicaval cannulation is necessary and the right atrium is explored. In that instance, a third caval cannulation will be required.
In patients with PLSVC, placement of a transvenous permanent pacemaker is technically more difficult. Fortunately, in this case the patient reverted to sinus rhythm successfully with transcutaneous pacing. However, it also precluded the opportunity for us to identify this vascular anomaly prior to cardiac catheterisation. If transvenous pacing was required, it may still be straightforward as the right SVC is present. Nonetheless, 10% of cases with absent right SVC may lead to the advancement of catheter through left SVC, left atrium, coronary sinus, right atrium and into right ventricle. To avoid the difficult course and potential complication, implanting lead at left atrial or ventricle has been reported.
Another practical issue of left SVC draining into coronary sinus is the difficulty to achieve retrograde cardioplegia. The options for retrograde cardioplegia in this case include placing a sucker in the coronary sinus, setting up a separate vent up the coronary sinus and snaring it off, separating cannulation (with three venous cannulae), or simply snaring it off during the procedure.
Learning points.
Persistent left superior vena cava (PLSVC) has no dire consequences in most coronary artery bypass graft or valve surgery with single caval cannulation. However, its significance when inserting a pacemaker or giving cardioplegia should be taken into consideration pre-emptively.
An enlarged and dilated coronary sinus on echocardiography should serve as an indicator to suspect PLSVC.
Footnotes
Contributors: JHT designed the study, collected and analysed the data, drafted the article and approved the final version of the article to be published. ZQN analysed the data, revised the article and approved the final version of the article to be published. SV codesigned the study, analysed the data, critically reviewed the article, supervised the study and approved the final version of the article to be published.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Goyal SK, Punnam SR, Verma G, et al. Persistent left superior vena cava: a case report and review of literature. Cardiovasc Ultrasound 2008;6:50 doi:10.1186/1476-7120-6-50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Paval J, Nayak S. A persistent left superior vena cava. Singapore Med J 2007;48:e90–3. [PubMed] [Google Scholar]
- 3.Akpinar I, Sayin MR, Karabag T, et al. Persistent left superior vena cava, absence of the innominate vein, and upper sinus venosus defect : a rare anomaly detected using bubbles. Herz 2013;38:317–20. doi:10.1007/s00059-012-3704-z [DOI] [PubMed] [Google Scholar]