

Sir,
Rafael Blanco (ESRA XXVI, 2007) conceived the original concept of an ultrasound-guided quadratus lumborum block (QLB) and later Børglum et al.[1] suggested the transmuscular approach of QLB. Transmuscular QLB provides effective post-operative pain relief after lower segment caesarean section.[2] Although the exact site of action of local anaesthetic is not yet clear,[3] a clinical study by Børglum et al.[1] and a cadaveric study by Dam et al.[4] clearly depicted the spread of injectate cranially along the QL and psoas major reaching the arcuate ligaments and beyond. However, this block is technically cumbersome to perform since the patient is placed in lateral decubitus position keeping the side to be blocked upwards and needs to be turned over to perform the block on the contralateral side.[1,2,3,4,5,6]
We suggest an approach through which bilateral block can be performed in a single lateral decubitus position, without changing the side from the original lateral decubitus position to the contralateral side. This technique increases the ease of the procedure by avoiding repositioning of the patient and thus decreases the procedure time. After completion of surgery and sterile dressing of the wound, the patient was placed in lateral decubitus position, and a curvilinear ultrasound probe (2–6 MHz, SonoSite M-Turbo) was placed cephalad and parallel to the iliac crest and moved posteriorly until 'Shamrock' sign was clearly identified. A 10 cm blunt tip needle (Stimuplex™, B. Braun, Melsungen, Germany) was inserted from posterior to anterior direction to target the fascial layer between quadratus lumborum and psoas muscle as described earlier.[1,2,3] After confirmation of needle position, 20 ml of local anaesthetic solution (ropivacaine 0.375%) was injected slowly after careful and repeated negative aspiration for blood [Figure 1a and b]. To block the other side, the transducer was placed on the opposite side in the same line at a lower level keeping the orientation of marker and distance from midline similar to first injection. The identification and orientation of structures remain similar, and the block was performed in a similar manner as done previously [Figure 2a and b] following which the patient was made supine.
Figure 1.
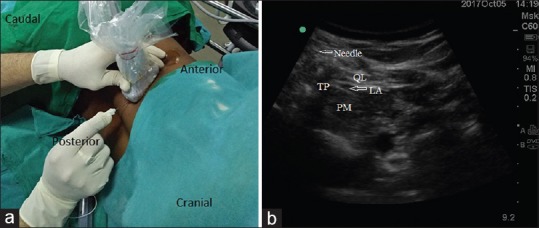
(a) The patient is in lateral position; curvilinear probe (2–6 MHz) is just above and posterior to iliac crest and needle entering at the edge of probe in posterior to anterior direction. (b) Sonoanatomy. QL – Quadratus lumborum; PM – Psoas muscle; TP – Transverse process (L4); LA – Local anaesthetic spread
Figure 2.

(a) Ultrasound position and needle entry for quadratus lumborum block for other side. (b) Sonoanatomy. QL – Quadratus lumborum; PM – Psoas muscle; TP – Transverse process (L4); LA – Local anaesthetic spread
We have been using this approach regularly for post-caesarean analgesia done under spinal anaesthesia. However, the extent of sensory blockade could not be assessed due to residual effects of anaesthesia. Most individuals reported satisfaction with pain relief (Numeric Rating Score 2/10–3/10 on the scale of 0–10 where 0 = no pain and 10 = maximum pain) when the block was used as a component of multimodal regimen which included round the clock nonsteroidal anti-inflammatory drugs and opioids for breakthrough pain. In addition, supplemental analgesic requirements were reduced with the block in most of the individuals and no complications have been noted so far. However, these preliminary results need to be substantiated further in a randomised clinical trial, which is currently underway (CTRI/2017/12/010987).
To the best of our knowledge, this approach is not documented earlier and we hope, this approach will avoid repositioning for performing bilateral transmuscular quadratus lumborum block.
The QL-3 block is an advanced (competency level 3) block. It has inherent challenges due to anatomical difficulties and requires high level of anatomical understanding and eye-needle coordination. Therefore, it is advisable that, transmuscular quadratus lumborum block should always be given by an experienced anaesthesiologist.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Børglum J, Moriggl B, Jensen K, Lønnqvist PA, Christensen AF, Sauter A, Bendtsen TF. Ultrasound-guided transmuscular quadratus lumborum blockade. Br J Anaesth 2013;111: eLetters Supplement, 22 April. [Last accessed on 2017 Dec 01]. Available from: http://www.bja.oxfordjournals.org/forum/topic/brjana_el%3b9919 .
- 2.Mænchen N, Hansen CK, Dam M, Børglum J. Ultrasound-guided Transmuscular Quadratus Lumborum (TQL) block for pain management after caesarean section. Int J Anesth Anesthesiol. 2016;3:48. [Google Scholar]
- 3.Elsharkawy H. Quadratus lumborum blocks. In: McLoughlin TM, Salinas FV, Torsher LC, editors. Advances in Anesthesia. New York: Elsevier Health Science; 2017. pp. 145–55. [DOI] [PubMed] [Google Scholar]
- 4.Dam M, Moriggl B, Hansen CK, Hoermann R, Bendtsen TF, Børglum J, et al. The pathway of injectate spread with the transmuscular quadratus lumborum block: A Cadaver study. Anesth Analg. 2017;125:303–12. doi: 10.1213/ANE.0000000000001922. [DOI] [PubMed] [Google Scholar]
- 5.Ashok J, Mayur M, Asit KP, Neelam S. Postoperative analgesia by transmuscular quadratus lumborum block catheters. J Anesth Int Care Med. 2016;1:555–62. [Google Scholar]
- 6.Nair A. Bilateral quadratus lumborum block for post-caesarean analgesia. Indian J Anaesth. 2017;61:362–3. doi: 10.4103/ija.IJA_204_17. [DOI] [PMC free article] [PubMed] [Google Scholar]