

Summary:
Syndactyly is a congenital condition characterized by fusion of the fingers. If not treated correctly during infancy, syndactyly may hinder the normal development of hand function. Many surgical techniques have been developed, with the main goal to create a functional hand with the smallest number of operative corrections. Therefore, exact preoperative planning of the reconstructive procedure is essential. An imaging method commonly used for preoperative planning is 3-dimensional (3D) surface imaging. The goal of this study was to implement the use of this technique in hand surgery, by designing a virtual planning tool for a desyndactylization procedure based on 3D hand images. A 3D image of a silicon syndactyly model was made on which the incision pattern was virtually designed. A surgical template of this pattern was printed, placed onto the silicon model and delineated. The accuracy of the transfer from the virtual delineation toward the real delineation was calculated, resulting in a mean difference of 0.82 mm. This first step indicates that by using 3D images, a virtual incision pattern can be created and transferred back onto the patient successfully in an easy and accurate way by using a template. Thereafter, 3D hand images of 3 syndactyly patients were made, and individual virtual incision patterns were created. Each pattern was transferred onto the patient by using a 3D printed template. The resulting incision pattern needed minor modifications by the surgeon before the surgery was performed. Further research and validation are necessary to develop the virtual planning of desyndactylization procedures.
INTRODUCTION
Three-dimensional (3D) stereophotogrammetry imaging was recently introduced into the hand surgery field.1,2 The advantages of this technique are its lack of radiation, cost-effectiveness, and good patient tolerance. It allows for accurate, immediately available 3D soft-tissue hand images.
To demonstrate its usefulness in clinical practice, we used 3D hand images during the preoperative planning process of a desyndactylization procedure. Syndactyly is a congenital abnormality, in which the fingers are fused. Preoperative evaluation of the soft and bony tissue elements in the syndactylized hand is necessary in every patient and done using conventional radiology images and computed tomography (CT) scan images.3 Hynes et al.3 found that CT angiographically guided release of adjacent webspaces benefits the patient. However, CT imaging has numerous disadvantages, like radiation, costs, and need for anesthesia when used for children.4,5 Until now, no harmless imaging technique exists that evaluates the soft tissues in a 3D method. The goal of this study was to implement the use of 3D stereophotogrammetry in hand surgery, by designing a method to virtually plan the incision pattern for a desyndactylization procedure and transfer this planning onto the patient.
SUBJECTS AND METHODS
A 3D image of an adult subject was made to simulate syndactyly and scaled down to an average toddler size hand. This was used as a reference to create a silicon syndactyly model, and a new 3D image of this model was created. All images were obtained with the 3dMD cranial system (3dMD cranial system, Atlanta, Ga.), which consists of 5 pods with a total of 15 cameras. The obtained 3D image was loaded into 3ds Max 2016 (Autodesk Inc, San Rafael, Calif.). Thereafter, the incision pattern was virtually planned on the dorsal side by an experienced hand surgeon (T.W.) in 3ds Max (Fig. 1). Using a transparent filter setting of the model, the surgeon was able to plan the palmar side using the dorsal side as a reference (Fig. 2). To transfer the virtual planning to the silicon model, a patient-specific surgical template was designed and printed using the Laser-Sinter-System EOS P 396 3D printer (Oceanz, Ede, Netherlands). This template could then be placed exactly onto the silicon syndactyly model (Fig. 3), after which the planning could be marked with a marker pen. To evaluate the transfer of the virtual planning onto the model, another 3D image of this model with the markings was obtained. This image was loaded into Maxilim (Medicim, Leuven, Belgium) and matched with the virtual planning using an Iterative Closest Point algorithm. Thereafter, landmarks were placed at the corners of the virtually planned and real delineation to calculate the accuracy. Next, 3D images of 3 patients (2 male, 1 female, average age, 3.2 years) were obtained, and a virtual incision pattern was planned by the surgeon (T.W.). This planning was transferred onto the patient preoperatively. Postoperatively, the experiences of the surgeon using this template were obtained.
Fig. 1.
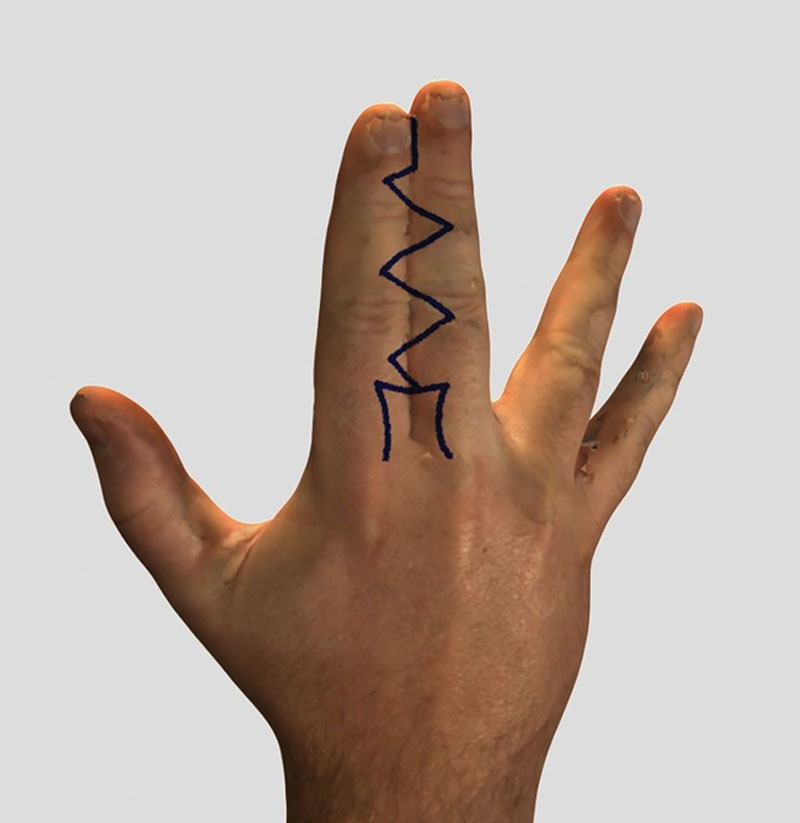
Drawing of incision pattern on a 3D image. This figure shows the virtually planned incision pattern, drawn on the dorsal side of a 3D image of a syndactyly model in 3ds Max.
Fig. 2.
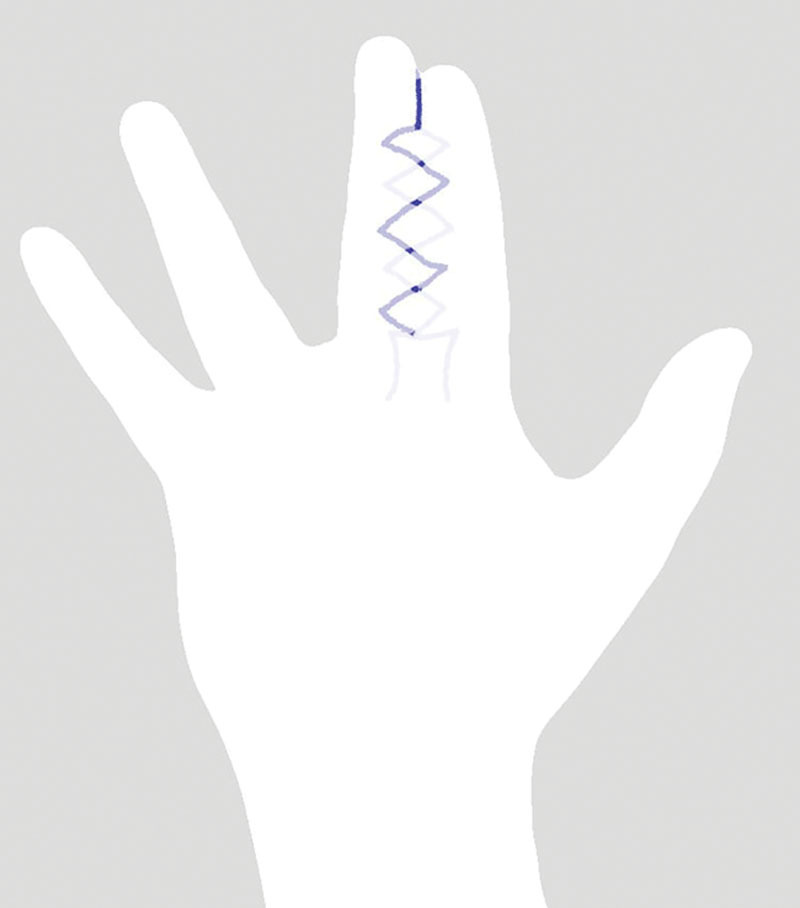
Drawing of palmar incision pattern on 3D transparent image. The 3D image was made transparent as shown in this figure. By using this transparent model, the surgeon was able to plan the palmar side with reference of the dorsal side.
Fig. 3.

Template fitted to the silicon syndactyly model. The custom-made template was placed onto a silicon syndactyly model. Thereafter, the planning could be marked with a marker pen.
RESULTS
The virtual planning process was simple to perform, because the model could be viewed from any possible angle and using the transparent filter setting, an exact mirror image of the dorsal side could be drawn on the palmar side. The template had a precise fit onto the silicon model and the production costs were very low (average €50 including the planning process). Using a marker pen, it was easy to draw the delineation on the surface. The accuracy of the landmarks placed on the virtual delineation compared with the real delineation was calculated, resulting in a mean difference of 0.82 ± 0.32 mm. Transferring the incision pattern onto the patient was easy and fast (Fig. 4), as reported by the surgeon. The template was found to be very helpful in copying the delineation from front to back. The resulting incision pattern needed minor modifications by the surgeon before the surgery was performed, not modifying the original surgical plan. The surgeries were performed without any problems, with satisfying postoperative results.
Fig. 4.
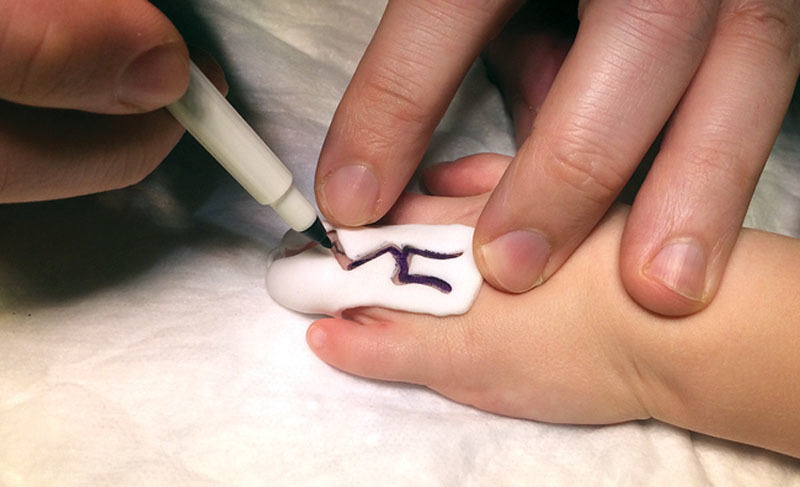
Usage of the template preoperatively. Transferring the incision pattern onto the patient was easy and fast by using the template.
DISCUSSION
Syndactyly is 1 of the most common congenital disorder of the limbs, in which normal hand development may be hindered when not treated in a timely manner. The basic principles of the desyndactylization procedure have been widely established.6–9 To reach the goal of creating a functional hand, every surgical procedure aims to produce a deep and wide webspace with as little as necessary skin grafting. 3D stereophotogrammetry is an easy to use, safe imaging technique,10,11 which has proven to be a valid method for capturing surface information and calculating volume deficits.2,10,12 By using 3D images for exact planning of the incision pattern, creating a deep webspace could be easier and therewith distal migration of the web, often requiring corrective surgery, would be avoided.13,14 Furthermore, when the amount of necessary skin can be calculated preoperatively, excessive skin grafting will be avoided, leading to less scarring.
With this first use of 3D images in preoperative planning, minor modifications were necessary due to the somewhat wide opening of the delineation in the template, resulting in broader markings on the patient than normally used. This was corrected preoperatively, and in the computer program for future delineations. The experiences of the hand surgeon proved the usage of the template to be easy and to simplify the surgical procedure, which will be helpful for less experienced surgeons or residents performing desyndactylization procedures.
In this study, we show an easy method for preoperative hand surgery planning based on 3D images. This first step proves that by using 3D hand images, a virtual incision pattern can be created and transferred back onto the patient successfully. The preoperative planning will reduce total surgery time, as the surgeon can directly copy the incision pattern from the template. The quality and therewith final result of the incision pattern will be improved, as different incisions and their results can be tested virtually, to reach the optimal, individual incision pattern. With our future research, we will continue to develop the virtual planning tool for desyndactylization procedures, therewith expanding the implementation of 3D imaging in hand surgery.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Hoevenaren IA, Maal TJ, Krikken E, et al. Development of a three-dimensional hand model using 3D stereophotogrammetry: evaluation of landmark reproducibility. J Plast Reconstr Aesthet Surg. 2015;68:709–716.. [DOI] [PubMed] [Google Scholar]
- 2.Hoevenaren IA, Meulstee J, Krikken E, et al. Development of a three-dimensional hand model using three-dimensional stereophotogrammetry: assessment of image reproducibility. PLoS One. 2015;10:e0136710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hynes SL, Harvey I, Thomas K, et al. CT angiography-guided single-stage release of adjacent webspaces in non-Apert syndactyly. J Hand Surg Eur Vol. 2015;40:625–632.. [DOI] [PubMed] [Google Scholar]
- 4.Brenner DJ, Hall EJ. Computed tomography—an increasing source of radiation exposure. N Engl J Med. 2007;357:2277–2284.. [DOI] [PubMed] [Google Scholar]
- 5.Lin EC. Radiation risk from medical imaging. Mayo Clinic Proceedings. 2010;85:1142–1146.; quiz 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Upton J. McCarthy JG MJ, Littler JW. Congenital anomalies of the hand and forearm. In: Plastic Surgery: The Hand Part 2. 1990:Philadelphia, Pa.: WB Saunders; 5213–5398.. [Google Scholar]
- 7.van der Biezen JJ, Bloem JJ. Dividing the fingers in congenital syndactyly release: a review of more than 200 years of surgical treatment. Ann Plast Surg. 1994;33:225–230.. [DOI] [PubMed] [Google Scholar]
- 8.Dao KD, Shin AY, Billings A, et al. Surgical treatment of congenital syndactyly of the hand. J Am Acad Orthop Surg. 2004;12:39–48.. [DOI] [PubMed] [Google Scholar]
- 9.Oda T, Pushman AG, Chung KC. Treatment of common congenital hand conditions. Plast Reconstr Surg. 2010;126:121e–133e.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Maal TJ, van Loon B, Plooij JM, et al. Registration of 3-dimensional facial photographs for clinical use. J Oral Maxillofac Surg. 2010;68:2391–2401.. [DOI] [PubMed] [Google Scholar]
- 11.Plooij JM, Swennen GR, Rangel FA, et al. Evaluation of reproducibility and reliability of 3D soft tissue analysis using 3D stereophotogrammetry. Int J Oral Maxillofac Surg. 2009;38:267–273.. [DOI] [PubMed] [Google Scholar]
- 12.Aldridge K, Boyadjiev SA, Capone GT, et al. Precision and error of three-dimensional phenotypic measures acquired from 3dMD photogrammetric images. Am J Med Genet A. 2005;138A:247–253.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kozin SH, Zlotolow DA. Common pediatric congenital conditions of the hand. Plast Reconstr Surg. 2015;136:241e–257e.. [DOI] [PubMed] [Google Scholar]
- 14.Richterman IE, DuPree J, Thoder J, et al. The radiographic analysis of web height. J Hand Surg. 1998;23:1071–1076.. [DOI] [PubMed] [Google Scholar]