

Abstract
Decreased red cell deformability is characteristic of several disorders. In some cases, the extent of defective deformability can predict severity of disease or occurrence of serious complications. Ektacytometry uses laser diffraction viscometry to measure the deformability of red blood cells subject to either increasing shear stress or an osmotic gradient at a constant value of applied shear stress. However, direct deformability measurements are difficult to interpret when measuring heterogenous blood that is characterized by the presence of both rigid and deformable red cells. This is due to the inability of rigid cells to properly align in response to shear stress and results in a distorted diffraction pattern marked by an exaggerated decrease in apparent deformability. Measurement of the degree of distortion provides an indicator of the heterogeneity of the erythrocytes in blood. In sickle cell anemia, this is correlated with the percentage of rigid cells, which reflects the hemoglobin concentration and hemoglobin composition of the erythrocytes. In addition to measuring deformability, osmotic gradient ektacytometry provides information about the osmotic fragility and hydration status of erythrocytes. These parameters also reflect the hemoglobin composition of red blood cells from sickle cell patients. Ektacytometry measures deformability in populations of red cells and does not, therefore, provide information on the deformability or mechanical properties of individual erythrocytes. Regardless, the goal of the techniques described herein is to provide a convenient and reliable method for measuring the deformability and cellular heterogeneity of blood. These techniques may be useful for monitoring temporal changes, as well as disease progression and response to therapeutic intervention in several disorders. Sickle cell anemia is one well-characterized example. Other potential disorders where measurements of red cell deformability and/or heterogeneity are of interest include blood storage, diabetes, Plasmodium infection, iron deficiency, and the hemolytic anemias due to membrane defects.
Keywords: Immunology, Issue 131, Fetal hemoglobin, osmotic gradient ektacytometry, erythrocyte, deformability, sickle cell anemia, diffraction distortion
Introduction
Ektacytometry provides a convenient measure of red cell deformability in response to alterations in shear stress (measured in pascals (Pa)) or suspending medium osmolality. Pertinent parameters of red cell deformability include the maximum elongation index (EI Max), a measure of the maximum deformability of a red cell in response to increasing shear stress, and shear stress ½ (SS ½), the shear stress required to achieve half maximal deformability.1 Osmotic gradient ektacytometry has several informative parameters. These include the elongation index minimum (EI Min), a measure of surface-to-volume ratio and the osmolality at which it occurs (O Min), which is a measure of osmotic fragility. EI Max and the osmolality at which it occurs (O (EI Max)) provide information on membrane flexibility and cell surface area. Half maximal elongation in the hypertonic arm of the osmotic gradient is represented by EI hyper. EI hyper and the osmolality at which it occurs, O hyper, provide information about the intracellular viscosity of the red cell which is determined by hemoglobin concentration.2,3 Measuring deformability in heterogenous blood is complicated by the fact that rigid cells, such as sickled red blood cells, do not properly align with the direction of flow such as deformable cells in response to increasing shear stress. Rather than producing a characteristic elliptical diffraction image, rigid cells produce a spherical pattern which results in a diamond-shaped diffraction pattern when overlaid on the ellipse produced by deformable cells.4,5,6 The spherical pattern has been shown to correspond to irreversibly sickled cells by performing ektacytometry on isolated fractions of cells following density centrifugation.6 The elongation index calculation includes measures of both the long and short axis of the ellipse; a diamond shape therefore produces an apparent decrease in elongation by increasing the width of the short axis.7 It has been previously shown that the degree of diffraction pattern distortion is correlated with both the percentage of sickle hemoglobin (HbS) and the percentage of sickled cells in the blood from patients with sickle cell anemia.5 The degree of diffraction pattern distortion can be obtained by complex mathematical analyses.8 It can also be obtained by adjusting the opening of the camera aperture on the ektacytometer or the grey level of the fitting software to alter the diffraction pattern height.5 However, details regarding how to adjust the grey level are not well defined and the camera aperture is not readily accessible on the latest generation of the commercially available ektacytometer. To circumvent these issues, the easily accessible camera gain can be used to adjust diffraction pattern heights.9 Using this method to estimate cellular heterogeneity, the degree of diffraction pattern distortion can be correlated with the percentage of fetal hemoglobin in the blood of patients with sickle cell anemia.10 Several osmotic gradient ektacytometry parameters are likewise correlated with the percentage of fetal or sickle hemoglobin in blood from patients with sickle cell anemia. Diffraction pattern distortion correlations likely reflect the contribution of hemoglobin composition to the percentage of rigid, non-deformable cells. Of additional interest, the entire osmotic gradient ektacytometry profile undergoes biphasic changes that correspond to the percentage of dense cells in circulation during sickle cell crisis.11
Ektacytometry is likewise useful in the study of several other disorders. Osmotic gradient ektacytometry is diagnostic for the inherited red cell membrane disorders, such as hereditary spherocytosis, hereditary elliptocytosis and hereditary pyropoikilocytosis.3,12,13,14 Decreased deformability occurs in iron deficiency.15 Characterization of the "storage lesion" of blood has employed ektacytometry and future studies investigating both the nature of the lesion and interventions to prevent its formation during the storage of banked blood are likely to benefit from the techniques presented here.16 Decreased red cell deformability has also been correlated with microvascular disease in diabetes.17 Recent studies linking hyperglycemia, red cell ascorbate concentrations and osmotic fragility suggest these factors may be important in the development of microvascular disease.18 Ektacytometry studies are currently underway to investigate this hypothesis (Parrow and Levine, unpublished data). Blood stage malarial infection is another interesting avenue of red cell deformability investigations. Cellular deformability of Plasmodium falciparum infected red blood cells decreases dramatically during the 48 hours of intracellular maturation of the parasite from ring stage to schizont stage. Evidence indicates that this decreased deformability is reversed upon maturation of the parasite. The reversal coincides with release of infected red cells into the circulation. Decreased deformability is thought to be mediated by Plasmodium proteins that promote sequestration of the red cell.19 These studies represent a small sampling of clinically important conditions where measuring erythrocyte deformability and osmotic gradient parameters are relevant. Several additional areas of study exist.
Alternative techniques for measuring red cell deformability include optical tweezers (also known as laser traps) which use the physical properties of photons to stretch single red cells in one or more directions.20 This technique has the advantage of measuring the deformability of single erythrocytes, but some uncertainty in force calibration has produced considerable variability across studies 21 and data analysis can be labor-intensive unless automated.22 Micropipette aspiration, which uses negative pressure to aspirate an erythrocyte into a micropipette, has also been used to measure deformability of red cells.7,23 Multiple measurements, such as the pressure required to aspirate the red cell, are possible with each measure defining different characteristics of the red cell.23 Atomic force microscopy is a high resolution technique that measures membrane stiffness by quantifying laser beam deflection as an indicator of cantilever deflection along the surface of a red cell.24 These techniques provide information about individual erythrocytes, are not easily adapted to measure changes in populations of red blood cells, and, in general, require considerable technical expertise.
The desire to sample both individual and populations of cells simultaneously has led to advances in automation and the development of microfluidics and array-based methods. Like ektacytometry, rheoscopy measures deformability as a function of shear stress but images are acquired directly via microscope.25 For higher through-put analyses, automated cell imaging has been employed to produce deformability distributions using the rheoscope.26 Cellular heterogeneity can be quantified by this method if data from a healthy control subject are available.27 Microfluidics techniques also allow for high through-put analyses of single cells; multiple designs using adaptations of filtration,28 cell transit analyzers,29 which measures the time required for an erythrocyte flow through a micropore, and alternatives that measure the pressure required for erythrocyte transit rather than time 30 have been developed. Another platform for high through-put analysis of individual cells is the single cell microchamber array chip, which has the additional advantage of allowing for downstream fluorescence-based characterization of the cells.31 Although each of these techniques is potentially useful and may be superior for particular applications, the comparative advantages of ektacytometry includes sensitivity, ease of use, and precision.32 The latest generation of commercially available ektacytometers also possess considerable versatility in the number of assays that can be performed.
Protocol
All subjects in this study gave written informed consent in accordance with the Declaration of Helsinki and the National Institutes of Health Institutional Review Board approved protocols.
1. Turning on the ektacytometer
Connect the tubing from the cleaning solution to the low and high osmolar polyvinylpyrrolidone (PVP) solutions. Be careful to connect the 0 osmolar tube to the low osmolar solution and the 500 osmolar tube to the high osmolar solution. Note: The low osmolar PVP solution should have an osmolality between 35 and 55 milliosmoles per kilogram (mOsm/kg), a pH of 7.25-7.45 at 25 °C and a viscosity between 27.0 and 33.0 centipoise (cP) at 37.0 ± 0.5 °C. The high osmolar PVP solution should have an osmolality between 764 and 804 mOsm/kg, a pH of 7.25-7.45 at 25 °C and a viscosity measure of 27.0-33.0 cP at 37.0 ° 0.5 °C.
Ensure that the bob is lowered completely into the cup. Launch the software and prime the machine (Hardware Check | Instrument IO). Allow the instrument to complete the priming cycle. Once the cycle is complete, lift the bob out of the cup and completely dry the bob and the cup with a low lint cleaning tissue. Note: Residual water will lyse red cells, producing interference.
2. Measuring deformability as a function of increasing shear stress
Obtain blood (less than 1 mL is adequate to perform these techniques with replicates) in vial containing an appropriate anticoagulant. Note: EDTA is preferred over heparin because it has less influence over hemorheological parameters.33 Keep blood at room temperature if measurements are performed within 6 hours of blood draw.
Gently mix whole blood sample before testing by inverting the vial several times. Add 25 µL of whole blood to 5 mL of iso-osmolar PVP solution by pipetting, cap the vial and mix gently by inverting several times. The iso-osmolar PVP solution should have an osmolality between 284 and 304 mOsm/kg, a pH of 7.3-7.4 at 25 °C and a viscosity of 27.0-33.0 cP at 37.0 ± 0.5 °C.
- On the software choose deformability from the main menu. Create a new analysis and add experimental details (Deformability | Add desired details | Okay).
- Lift lid to ektacytometer, verify that the bob is fully lowered into cup and the cup is turning.
- Add 1 mL of PVP blood solution into the space between the cup and bob by pipetting.
- Lift the bob slightly to bring samples down. Wait until all bubbles have moved out of the solution, then close the lid to the ektacytometer. If needed, press the aspiration button to help remove bubbles.
Adjust the gain to 200 by moving the arrow along the scroll bar on the software (see note). When the temperature is stable at 37 °C and the diffraction image is stable, press start (Start). Note: For many studies, a good diffraction image can be obtained from healthy blood (hemoglobin concentration > 12.0 g/dL, mean corpuscular volume of 80-96 fL and mean corpuscular hemoglobin concentrations of 33-36 g/dL) with the camera gain set to 200. For studies of blood from sickle cell anemia, adjusting the camera gain to generate a 4.5 cm diffraction image has been suggested as the default setting to allow comparison of results across studies and laboratories.9
Observe diffraction patterns as data acquisition progresses to ensure that they remain circular, elliptical or diamond shaped. When data acquisition is complete, save or print the report (File | Save or File | Print). EI Max and SS ½ values will be reported automatically, along with elongation indices corresponding to user-specified or default shear stresses. Data will also be saved automatically by the software.
At the end, press the clean option on the dialog box on the computer monitor (Clean). After the sample is aspirated, rinse the space between the cup and bob by squirting deionized water into the space while the instrument remains in the clean cycle. Once the clean cycle is complete, lift the bob out of the cup and completely dry the bob and the cup with a low lint cleaning tissue (critical: Residual water will lyse red cells, producing interference).
Click on the Main Menu button on the software to return to the main page (Main Menu).
3. Measuring cellular heterogeneity
Gently mix whole blood sample before testing by inverting the vial several times. Pipet 25 µL of whole blood to a new 5 mL vial of iso-osmolar PVP solution, cap the vial and mix gently by inverting until the mixture is homogenous.
- Choose deformability from the main menu. Create a new analysis and add experimental details (Deformability | Add desired details | Okay).
- Lift lid to ektacytometer, verify that the bob is fully lowered into cup and the cup is turning.
- Pipet 1 mL of the PVP blood solution into the space between the cup and bob.
- Wait until all bubbles have moved out of the solution, then close the lid to the ektacytometer.
- Ensure that a stable diffraction image is present on the screen. Adjust the camera gain by moving the arrow along the scrollbar on the software until it produces a 3.8 cm diffraction height. Use a ruler to verify the height of the image on the computer screen.
When the temperature is stable at 37 °C and the diffraction image is stable, press start (Start).
Observe diffraction patterns as data acquisition progresses to ensure that they remain circular, elliptical or diamond-shaped. When data acquisition is complete, save or print the report (File | Save or File | Print).
At the end, press the clean option on the dialog box on the computer monitor (Clean). After the sample is aspirated, rinse the space between the cup and bob by squirting deionized water from a squirt bottle into it while the instrument remains in the clean cycle. Once the clean cycle is complete, lift the bob out of the cup and completely dry the bob and the cup with a low lint cleaning tissue (critical: Residual water will lyse red cells, producing interference).
Repeat steps 2.1-2.5 and adjust camera gain to obtain a 4.5 cm diffraction pattern height (step 2.2).
Repeat steps 2.1-2.5 and adjust camera gain to obtain a 5.4 cm diffraction pattern height (step 2.2).
At the end, click on the main menu button to return to the main page of the software (Main Menu).
To determine the degree of diffraction pattern distortion based on EI Max as a percentage, use the following equation (the same equation can be performed with the data from the 4.5 cm diffraction pattern height if desired):

Similarly, to determine the degree of diffraction pattern distortion based on SS1/2 use the same equation with the reported SS1/2 value:

4. Osmotic gradient ektacytometry
Obtain sample as described in 1.1. Gently mix whole blood sample before testing by inverting several times. Add 250 µL of whole blood to 5 mL iso-osmolar PVP vial by pipetting, cap the vial and mix gently by inverting until the mixture is homogenous.
Choose osmoscan from the main menu (Osmoscan). Place vial containing the blood PVP solution underneath the needle on the left-hand side of the machine. Lower the needle until it touches the bottom of the vial. Make sure tubing is properly connected to the low and high osmolar solutions for gradient production. Close the lid to the ektacytometer and open the door on the lower half so that you can watch the blood enter the tubing.
- Press new analysis and type in experimental details (Osmoscan | New Analysis | Enter desired details | Okay). Adjust the camera gain to 200 by moving the arrow controlling it on the software and allow the machine run until blood is seen entering the cup from the tubing beneath the instrument.
- Once the blood has entered the cup and a stable diffraction pattern image is on the computer screen, begin data acquisition by pressing the start now button on the dialog box (Start Now).
Allow the ektacytometer to acquire data up to approximately 500 mOsm/kg, then stop the instrument. Save or print report (File | Save or File | Print). Data will also save automatically.
Remove the old PVP-blood vial. Replace it with a clean vial containing deionized water. Place it beneath the needle, bring the needle down so that it touches the bottom of the vial and press the rinse button in the dialog box to rinse the gradient system (Rinse).
Once the rinse is complete, press the clean option on the dialog box on the computer monitor (Clean). Once the clean cycle is complete, lift the bob out of the cup and completely dry the bob and the cup with a low lint cleaning tissue (critical: Residual water will lyse red cells, producing interference). Note: The osmoscan report provides elongation indices across the osmotic gradient. EI Min, O (EI Min), EI Max, O (EI Max), EI hyper and O hyper are generated automatically and included in the report. The range of osmotic gradient ektacytometry parameters obtained from blood from 9 healthy volunteers is: EI Min 0.12-0.196 arbitrary units (a.u.); O Min 117-144 mOsm/kg; EI Max 0.551-0.573 a.u.; O (EI Max) 272-312 mOsm/kg; EI hyper 0.278-0.286; O Hyper 454-505 mOsm/kg.
5. Turning off the ektacytometer
- Clean the instrument properly before it is shut down.
- To do this, connect the tubing from the low and high osmolar solutions to the y-adapter leading to the cleaning solution. Place a vial containing cleaning solution below the needle on the left-hand side of the machine and lower the needle until it touches the bottom of the vial. Ensure that the bob is lowered completely into the cup.
- Close the software, and press start on the end of day clean dialog box on the computer monitor (Close | Start). Allow the instrument to cycle through cleaning completely.
Disconnect the tubing to the waste bottle and remove it from the instrument to discard waste. Dry the bob completely. Turn the machine off.
Representative Results
The ektacytometry results described in this manuscript can be used to measure red cell deformability in any condition. A schematic of the general set up of an ektacytometer is shown in Figure 1. Homogeneous populations of erythrocytes will produce an elliptical diffraction pattern in response to increasing shear stress that can be used to calculate the elongation index as shown in Figure 2. Diffraction pattern distortion occurs in heterogenous blood samples because rigid red cells do not align properly with deformable cells and produce a spherical pattern that overlays the ellipse resulting in a diamond shaped diffraction pattern. This distorted pattern is increasingly detectable as the camera gain is adjusted to generate larger diffraction pattern sizes as shown in Figure 3. Homogeneous blood populations, as found in healthy volunteers, do not produce different deformability curves when different diffraction sizes are measured (Figure 4A). In contrast, heterogenous blood populations, such as blood from patients with sickle cell anemia, show significant decreases in deformability measures as a function of diffraction pattern size (Figure 4). In sickle blood, when the degree of diffraction pattern distortion is measured as a function of EI Max, it is correlated with HbS (Figure 5A) and the adult hemoglobin variant, HbA2 (Figure 5C). Transfusion corrects the distortion, as indicated by its inverse relationship with the percentage of normal adult hemoglobin (HbA) in the blood (Figure 5D). Whether the degree of diffraction pattern distortion is measured as a function of shear stress ½ (Figure 5B) or as a function of EI Max (Figure 5E), it is correlated with fetal hemoglobin. However, the relationship is stronger in the former than the latter. Key osmotic gradient ektacytometry parameters, such as O (EI Max), EI Min and O Min provide additional information about the cellular hydration, surface-to-volume ratios and osmotic fragility, respectively. Osmotic gradient curves obtained from sickle blood are characteristically left-shifted with marked decreases in deformability that become increasingly pronounced in the hypertonic region as shown in Figure 6.
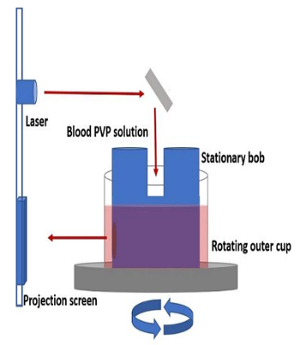
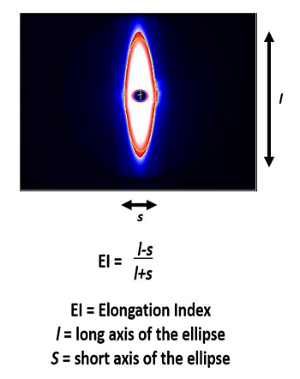
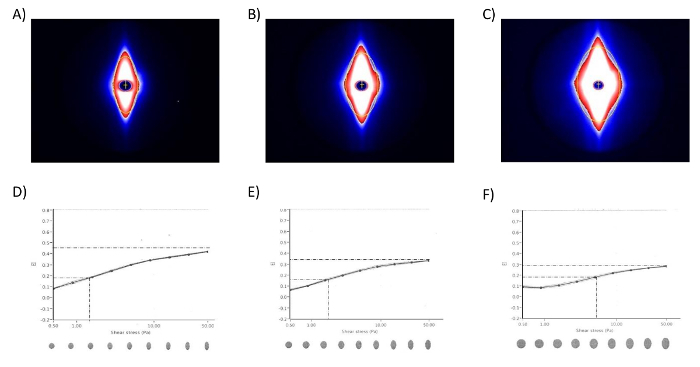
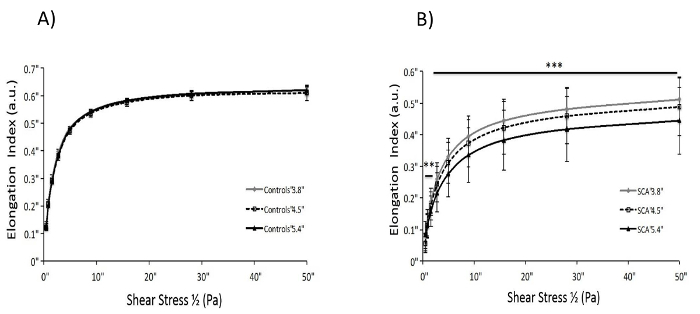
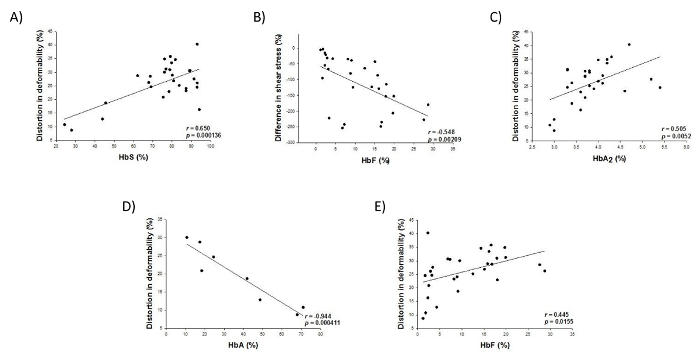
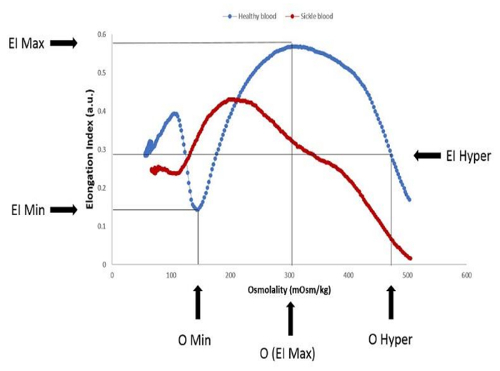
Figure 1. Schematic of ektacytometer set-up. An outer cup rotates around a stationary bob to generates shear stress on blood resuspended in a PVP solution of defined viscosity that is placed between them. A diffraction pattern is generated by a laser that passes through the solution and the diffraction pattern is displayed on a projection screen. Please click here to view a larger version of this figure.
Figure 2. General overview of the relationship between diffraction pattern and elongation index. Diffraction pattern obtained from healthy blood in response to shear stress shows the expected elliptical pattern. Elongation index (EI) is calculated using the equation indicated 7. Please click here to view a larger version of this figure.
Figure 3. Cellular heterogeneity produces diffraction pattern distortions. Diffraction patterns obtained from blood from a sickle cell anemia patient when the camera gain is adjusted to produce A) a 3.8 cm diffraction pattern, B) a 4.5 cm diffraction pattern and C) a 5.4 cm diffraction pattern. Deformability curves showing a progressive decrease in apparent deformability and a corresponding increase in apparent shear stress ½, indicated by the lines, from the same blood when the camera gain is adjusted to produce D) the 3.8 cm diffraction pattern, E) the 4.5 cm diffraction pattern and F) the 5.4 cm diffraction pattern. [Reprinted by permission from Parrow et al. 10]. Please click here to view a larger version of this figure.
Figure 4. Diffraction pattern distortions produce an apparent decrease in deformability across a range of shear stresses in blood from patients with sickle cell anemia. Comparison of deformability curves generated from A) blood from healthy volunteers and B) blood from patients with sickle cell anemia by adjusting the camera gain to generate a 3.8 cm, 4.5 cm and 5.4 cm diffraction pattern size. Deformability curves generated with blood from patients with sickle cell anemia, but not from healthy volunteers, show progressive and significant decreases in apparent deformability in response to as little as 5 Pa shear stress as a function of diffraction pattern size. [Reprinted by permission from Renoux et al.9]. Please click here to view a larger version of this figure.
Figure 5. The degree of diffraction pattern distortion is correlated with hemoglobin composition in blood from patients with sickle cell anemia. Linear regression analyses show the relationship between A) the EI Max-based distortion in deformability and the percentage of HbS, B) the SS 1/2-based distortion in deformability and the percentage of fetal hemoglobin (HbF), C) the EI Max-based distortion in deformability and the percentage of HbA2, D) the EI Max-based distortion in deformability and the percentage of HbA and E) for the purposes of direct comparison, the EI Max-based distortion in deformability and the percentage of HbF in blood from patients with sickle cell anemia. Pearson product moment correlation coefficient, r, and corresponding p-value are indicated. [Reprinted by permission from Parrow et al.10]. Please click here to view a larger version of this figure.
Figure 6. Blood from a patient with sickle cell anemia shows a characteristic left shift concomitant with decreased deformability compared to blood from a healthy volunteer when analyzed by osmotic gradient ektacytometry. Blood from a healthy volunteer (---) shows a representative osmotic gradient ektacytometry curve with the location of important parameters indicated. Osmotic gradient values from the healthy volunteer are 0.143 a.u. for EI Min, 146.3 mOsm/kg for O Min, 0.576 a.u. for EI Max and 473 mOsm/kg for O hyper. A representative osmotic gradient ektacytometry curve generated with blood from a patient with sickle cell anemia is overlaid (---). Osmotic gradient values from the sickle cell blood are 0.237 a.u. for EI Min, 110.3 mOsm/kg for O Min, 0.429 a.u. for EI Max and 406 mOsm/kg for O hyper. [ Adapted with permission from Parrow et al.10]. Please click here to view a larger version of this figure.
Discussion
The ektacytometry techniques described are straightforward and well automated, ensuring valid and reproducible results. Nonetheless, some critical steps exist. Proper temperature control of the blood is important. Storage at room temperature for more than eight hours may affect SS ½ values.34 Ensuring that the temperature of the machine is stable at 37 °C is also important, as viscosity of the suspending medium is temperature dependent. Blood should be fully oxygenated to avoid decreased deformability arising from non-oxygenated or partially oxygenated samples, unless these are experimental parameters of interest.35 From the point of view of instrumentation, proper cleaning of the instrument is critical to ensure that there is no PVP remaining in the tubing or the entry point of the bob as it will harden upon drying and block fluid flow through the instrument. Attention to these details will promote accurate results and keep the instrument in good running condition.
Quantification of cellular heterogeneity may require modification. In the 3.8 cm diffraction pattern, some samples may show a precipitous drop in the elongation index at the highest shear stresses. This can occasionally be overcome by repeating the measurement with a fresh sample. Otherwise, the degree of diffraction pattern distortion can be measured using an elongation index value from a lower shear stress or the 4.5 cm diffraction pattern can be used.9 It can also be difficult to obtain a 3.8 cm diffraction pattern from healthy blood because the long axis of the ellipse is too long even at the lowest camera gain. Again, the 4.5 cm diffraction pattern data can be used to circumvent this problem. The value that is chosen should, of course, be kept constant across the experiment as comparisons are only possible from data calculated using the same data point and diffraction pattern size. As the cellular heterogeneity measures are dependent on instrument set up, internal validation can be obtained by measuring diffraction pattern distortions on isolated cell fractions, or precisely defined mixtures of fractions, following density centrifugation as previously described.6
It is important to note that many ektacytometry parameters are sensitive to patient characteristics. Examples in sickle cell anemia include alpha globin status,36 MCV 37 and transfusion.10 Therefore, clinical studies need to be carefully designed and these relationships need to be accounted for when interpreting ektacytometry data.
Another important caveat is that there is not a direct general relationship between reduced ektacytometry measures and reduction in red cell survival. Asymptomatic conditions with severely decreased deformability, such as Southeast Asian ovalocytosis, exist.38 However, deformability measurements by any technique are complex and dependent on the cell surface area to volume ratio (sphericity), cytoplasmic viscosity (cellular hemoglobin concentration) and membrane rigidity. Red cell rheology is likewise complex, and there is not a technique available that can reproduce the complexity of physiologic blood flow in various vascular beds. Ektacytometry nevertheless provides important insights into altered red cell deformability and rheology.
The primary limitation of ektacytometry is the inability to measure deformability in individual cells. Thus, in sickle cell anemia, there is no way to determine the contribution of the fetal hemoglobin, which has a heterocellular distribution, on the deformability of a particular erythrocyte.10 Likewise, in a pool of Plasmodium infected blood from a patient there is no way to determine the influence of parasite maturity within a specific red blood cell.19 Future studies comparing ektacytometery results with those obtained using methods appropriate for individual cells would be valuable. Regardless of this limitation, ektacytometry provides a convenient and sensitive measure of the rheological properties of erythrocytes and the heterogeneity of blood populations. These data are important in the study of several disorders and are frequently of clinical relevance.
Disclosures
The authors have nothing to disclose.
Acknowledgments
This work was supported by the Intramural Research Program of the National Institutes of Diabetes, Digestive and Kidney Diseases and the National Heart, Lung and Blood Institute of the National Institutes of Health. The opinions expressed herein are the sole responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
References
- Bessis M, Mohandas N, Feo C. Automated ektacytometry: a new method of measuring red cell deformability and red cell indices. Blood Cells. 1980;6(3):315–327. [PubMed] [Google Scholar]
- Clark MR, Mohandas N, Shohet SB. Osmotic gradient ektacytometry: comprehensive characterization of red cell volume and surface maintenance. Blood. 1983;61(5):899–910. [PubMed] [Google Scholar]
- Da Costa L, et al. Diagnostic tool for red blood cell membrane disorders: Assessment of a new generation ektacytometer. Blood Cells Mol Dis. 2016;56(1):9–22. doi: 10.1016/j.bcmd.2015.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark MR, Mohandas N, Shohet SB. Deformability of oxygenated irreversibly sickled cells. J Clin Invest. 1980;65(1):189–196. doi: 10.1172/JCI109650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rabai M, et al. Deformability analysis of sickle blood using ektacytometry. Biorheology. 2014;51(2-3):159–170. doi: 10.3233/BIR-140660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bessis M, Mohandas N. Laser Diffraction Patterns of Sickle Cells in Fluid Shear Fields. Blood Cells. 1977;3:229–239. [Google Scholar]
- Kim Y, Kim K, Park Y. In: Blood Cell - An Overview of Studies in Hematology. Moschandreou TE, editor. InTech; 2012. [Google Scholar]
- Streekstra GJ, Dobbe JG, Hoekstra AG. Quantification of the fraction poorly deformable red blood cells using ektacytometry. Opt Express. 2010;18(13):14173–14182. doi: 10.1364/OE.18.014173. [DOI] [PubMed] [Google Scholar]
- Renoux C, et al. Importance of methodological standardization for the ektacytometric measures of red blood cell deformability in sickle cell anemia. Clin Hemorheol Microcirc. 2016;62(2):173–179. doi: 10.3233/CH-151979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parrow NL, et al. Measurements of red cell deformability and hydration reflect HbF and HbA2 in blood from patients with sickle cell anemia. Blood Cells Mol Dis. 2017;65:41–50. doi: 10.1016/j.bcmd.2017.04.005. [DOI] [PubMed] [Google Scholar]
- Ballas SK, Smith ED. Red blood cell changes during the evolution of the sickle cell painful crisis. Blood. 1992;79(8):2154–2163. [PubMed] [Google Scholar]
- Johnson RM, Ravindranath Y. Osmotic scan ektacytometry in clinical diagnosis. J Pediatr Hematol Oncol. 1996;18(2):122–129. doi: 10.1097/00043426-199605000-00005. [DOI] [PubMed] [Google Scholar]
- Mohandas N, Clark MR, Jacobs MS, Shohet SB. Analysis of factors regulating erythrocyte deformability. J Clin Invest. 1980;66(3):563–573. doi: 10.1172/JCI109888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarova E, Gulbis B, Oirschot BV, van Wijk R. Next-generation osmotic gradient ektacytometry for the diagnosis of hereditary spherocytosis: interlaboratory method validation and experience. Clin Chem Lab Med. 2017;55(3):394–402. doi: 10.1515/cclm-2016-0290. [DOI] [PubMed] [Google Scholar]
- Anderson C, Aronson I, Jacobs P. Erythrocyte Deformability is Reduced and Fragility increased by Iron Deficiency. Hematology. 1999;4(5):457–460. doi: 10.1080/10245332.1999.11746471. [DOI] [PubMed] [Google Scholar]
- Reinhart WH, et al. Washing stored red blood cells in an albumin solution improves their morphologic and hemorheologic properties. Transfusion. 2015;55(8):1872–1881. doi: 10.1111/trf.13052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shin S, et al. Progressive impairment of erythrocyte deformability as indicator of microangiopathy in type 2 diabetes mellitus. Clin Hemorheol Microcirc. 2007;36(3):253–261. [PubMed] [Google Scholar]
- Tu H, et al. Low Red Blood Cell Vitamin C Concentrations Induce Red Blood Cell Fragility: A Link to Diabetes Via Glucose, Glucose Transporters, and Dehydroascorbic Acid. EBioMedicine. 2015;2(11):1735–1750. doi: 10.1016/j.ebiom.2015.09.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tiburcio M, et al. A switch in infected erythrocyte deformability at the maturation and blood circulation of Plasmodium falciparum transmission stages. Blood. 2012;119(24):e172–e180. doi: 10.1182/blood-2012-03-414557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henon S, Lenormand G, Richert A, Gallet F. A new determination of the shear modulus of the human erythrocyte membrane using optical tweezers. Biophys J. 1999;76(2):1145–1151. doi: 10.1016/S0006-3495(99)77279-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mills JP, Qie L, Dao M, Lim CT, Suresh S. Nonlinear elastic and viscoelastic deformation of the human red blood cell with optical tweezers. Mech Chem Biosyst. 2004;1(3):169–180. [PubMed] [Google Scholar]
- Moura DS, et al. Automatic real time evaluation of red blood cell elasticity by optical tweezers. Rev Sci Instrum. 2015;86(5):053702. doi: 10.1063/1.4919010. [DOI] [PubMed] [Google Scholar]
- Evans EA. New membrane concept applied to the analysis of fluid shear- and micropipette-deformed red blood cells. Biophys J. 1973;13(9):941–954. doi: 10.1016/S0006-3495(73)86036-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen X, Feng L, Jin H, Feng S, Yu Y. Quantification of the erythrocyte deformability using atomic force microscopy: correlation study of the erythrocyte deformability with atomic force microscopy and hemorheology. Clin Hemorheol Microcirc. 2009;43(3):243–251. doi: 10.3233/CH-2009-1234. [DOI] [PubMed] [Google Scholar]
- Musielak M. Red blood cell-deformability measurement: review of techniques. Clin Hemorheol Microcirc. 2009;42(1):47–64. doi: 10.3233/CH-2009-1187. [DOI] [PubMed] [Google Scholar]
- Dobbe JG, Streekstra GJ, Hardeman MR, Ince C, Grimbergen CA. Measurement of the distribution of red blood cell deformability using an automated rheoscope. Cytometry. 2002;50(6):313–325. doi: 10.1002/cyto.10171. [DOI] [PubMed] [Google Scholar]
- Dobbe JG, et al. Analyzing red blood cell-deformability distributions. Blood Cells Mol Dis. 2002;28(3):373–384. doi: 10.1006/bcmd.2002.0528. [DOI] [PubMed] [Google Scholar]
- Kikuchi Y, Arai T, Koyama T. Improved filtration method for red cell deformability measurement. Med Biol Eng Comput. 1983;21(3):270–276. doi: 10.1007/BF02478493. [DOI] [PubMed] [Google Scholar]
- Moessmer G, Meiselman HJ. A new micropore filtration approach to the analysis of white cell rheology. Biorheology. 1990;27(6):829–848. doi: 10.3233/bir-1990-27604. [DOI] [PubMed] [Google Scholar]
- Guo Q, et al. Microfluidic analysis of red blood cell deformability. J Biomech. 2014;47(8):1767–1776. doi: 10.1016/j.jbiomech.2014.03.038. [DOI] [PubMed] [Google Scholar]
- Doh I, Lee WC, Cho YH, Pisano AP, Kuypers FA. Deformation measurement of individual cells in large populations using a single-cell microchamber array chip. Appl Phys Lett. 2012;100(17):173702–173703. doi: 10.1063/1.4704923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baskurt OK, et al. Comparison of three commercially available ektacytometers with different shearing geometries. Biorheology. 2009;46(3):251–264. doi: 10.3233/BIR-2009-0536. [DOI] [PubMed] [Google Scholar]
- Baskurt OK, et al. New guidelines for hemorheological laboratory techniques. Clin Hemorheol Microcirc. 2009;42(2):75–97. doi: 10.3233/CH-2009-1202. [DOI] [PubMed] [Google Scholar]
- Uyuklu M, et al. Effects of storage duration and temperature of human blood on red cell deformability and aggregation. Clin Hemorheol Microcirc. 2009;41(4):269–278. doi: 10.3233/CH-2009-1178. [DOI] [PubMed] [Google Scholar]
- Uyuklu M, Meiselman HJ, Baskurt OK. Effect of hemoglobin oxygenation level on red blood cell deformability and aggregation parameters. Clin Hemorheol Microcirc. 2009;41(3):179–188. doi: 10.3233/CH-2009-1168. [DOI] [PubMed] [Google Scholar]
- Embury SH, Clark MR, Monroy G, Mohandas N. Concurrent sickle cell anemia and alpha-thalassemia. Effect on pathological properties of sickle erythrocytes. J Clin Invest. 1984;73(1):116–123. doi: 10.1172/JCI111181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- von Tempelhoff GF, et al. Correlation between blood rheological properties and red blood cell indices(MCH, MCV, MCHC) in healthy women. Clin Hemorheol Microcirc. 2016;62(1):45–54. doi: 10.3233/CH-151944. [DOI] [PubMed] [Google Scholar]
- Da Costa L, Galimand J, Fenneteau O, Mohandas N. Hereditary spherocytosis, elliptocytosis, and other red cell membrane disorders. Blood Rev. 2013;27(4):167–178. doi: 10.1016/j.blre.2013.04.003. [DOI] [PubMed] [Google Scholar]