

Abstract
Purpose: Burst wave lithotripsy (BWL) is a new technology in development to fragment urinary stones. Ultrasonic propulsion (UP) is a separate technology under investigation for displacing stones. We measure the effect of propulsion pulses on stone fragmentation from BWL.
Materials and Methods: Two artificial stone models (crystalline calcite, BegoStone plaster) and human calcium oxalate monohydrate (COM) stones measuring 5 to 8 mm were subjected to ultrasound exposures in a polyvinyl chloride tissue phantom within a water bath. Stones were exposed to BWL with and without propulsion pulses interleaved for set time intervals depending on stone type. Fragmentation was measured as a fraction of the initial stone mass fragmented to pieces smaller than 2 mm.
Results: BegoStone model comminution improved from 6% to 35% (p < 0.001) between BWL and BWL with interleaved propulsion in a 10-minute exposure. Propulsion alone did not fragment stones, whereas addition of propulsion after BWL slightly improved BegoStone model comminution from 6% to 11% (p < 0.001). BegoStone model fragmentation increased with rate of propulsion pulses. Calcite stone fragmentation improved from 24% to 39% in 5 minutes (p = 0.047) and COM stones improved from 17% to 36% (p = 0.01) with interleaved propulsion.
Conclusions: BWL with UP improved stone fragmentation compared with BWL alone in vitro. The improvement was greatest when propulsion pulses are interleaved with BWL treatment and when propulsion pulses are applied at a higher rate. Thus, UP may be a useful adjunct to enhance fragmentation in lithotripsy in vivo.
Keywords: : burst wave lithotripsy, kidney stones, ultrasound
Introduction
Extracorporeal Shock wave lithotripsy (SWL) remains the only clinical option for extracorporeal treatment of nephrolithiasis; however, its utilization is decreasing relative to endoscopic management. A focus on ureteroscopy (URS) during residency training, higher stone-free rates, improving endoscopic technology, and the lower cost of URS relative to SWL,1,2 among other factors, have led to URS overtaking SWL as the most widely used intervention to treat kidney stones in the United States.3 While URS now appears more effective,4,5 many patients prefer SWL due to its less-invasive and noninstrumenting technique. Although SWL can be successful in the properly selected stone and patient, the lower stone-free rates with SWL are driven partly by unpredictable and incomplete fragmentation and clearance of stone fragments.6 An extracorporeal lithotripsy method that addresses the aforementioned shortcomings would therefore be an attractive stone management option.
Burst wave lithotripsy (BWL) is under investigation at the University of Washington as a potentially more effective and less injurious extracorporeal modality to fragment kidney stones.7 In comparison to SWL, where brief, impulsive, high-amplitude acoustic shocks are applied to break up the stone, BWL uses low-amplitude bursts of ultrasound delivered at relatively higher frequencies to cyclically stress stones until they fracture. During BWL, small pieces of consistent size break off from the surface of the larger body of the stone rather than breaking into a series of large fragments as is common in SWL.8 A prior study showed that the fracture pattern and resulting size of stone fragments are predictably determined by the frequency of BWL pulses.7 Thus, by appropriate choice of frequency, stones can be broken to fragments small enough to potentially pass without additional intervention.
When using BWL only in vitro, artificial stones visibly form fracture lines, but do not immediately break apart (Fig. 1). To overcome this barrier and complement the effects of BWL, we sought to incorporate a separate technology also under investigation by our group. Ultrasonic propulsion (UP) uses focused ultrasound pulses with relatively longer duration and lower amplitude than BWL to manipulate stones by acoustic radiation force.9,10 Previous studies have shown no indication of stone fragmentation due to UP pulses alone.11 A weak pulse can cause temporary agitation or “rocking” of a stone, whereas a strong pulse can cause the stone to reposition within the collecting system. By applying weak pulses to a stone during BWL, fragments may disperse from the stone, thus accelerating treatment. We hypothesized that the addition of interleaved UP pulses to BWL would accelerate stone fragmentation, compared with BWL alone. Using an in vitro lithotripsy model, we compared combinations of BWL with and without UP.
FIG. 1.
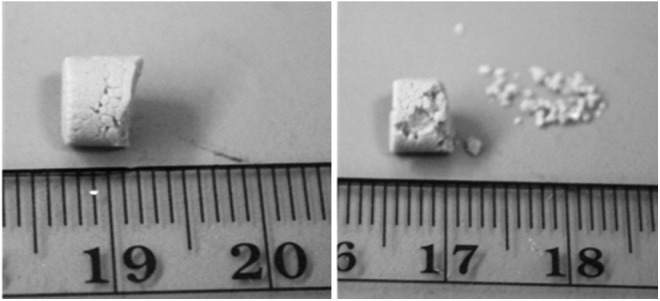
Artificial BegoStone model after 10 minutes of BWL exposure only (left) vs BWL with 6 propulsion pulses per minute (right), showing enhanced fragmentation with propulsion. BWL = burst wave lithotripsy.
Materials and Methods
Stone and tissue models
Experiments included two types of established artificial stone models, as well as human calcium oxalate monohydrate (COM) stones. The first artificial stone type was the BegoStone plaster model,12 which has acoustic properties similar to natural COM stones. For this model, BegoStone plaster powder (BEGO GmbH & Co. KG, Bremen, Germany) was mixed with deionized, degassed water in a ratio of 4:1 by weight, respectively. Aliquots of the mixture were then pipetted into a silicone rubber mold to form cylindrical stones of 6 mm diameter and 5 to 6 mm length. After the mold was allowed to set for at least 12 hours in a deionized water bath, the stones were removed from the mold and stored in deionized water until use.
An alternative artificial stone model tested was crystalline calcite, also known as Iceland Spar, a type of calcium carbonate with homogenous composition.13 The crystals were manually sectioned into 5- to 8-mm sized rhombohedral pieces (the crystals naturally cleave along rhombohedral planes). The BegoStone models were more consistent in size and mass than the crystalline calcite stones, due to variability of the exact size and shape of calcite crystals after sectioning.
Human COM stones, 5 to 8 mm in maximum dimension, were obtained whole or as fragments from ureteroscopic or percutaneous stone surgeries. All natural stones were analyzed to confirm primary COM composition by Beck Analytical Laboratories (Greenwood, IN) using infrared spectroscopy.
Stones were placed and treated in a polyvinyl chloride (PVC) tissue phantom that mimics human soft tissue acoustic properties, with a sound speed of 1400 m/s, a density of 1000 kg/m3, and an acoustic attenuation coefficient ∼0.1 dB/cm at 335 kHz.14 The phantom was cylindrical, 4 cm tall, 4.5 cm in diameter, and contained a 1.5 cm diameter depression for the stone in the middle to simulate a renal calyx.
BWL system
We performed BWL using a custom piezoelectric-focused ultrasound transducer with a focal length of 120 mm. The −6 dB focus size was 6 mm wide lateral to the acoustic axis and 53 mm length along the axis. The following BWL transducer acoustic parameters were chosen based on prior in vitro and in vivo studies7,15: 335 kHz frequency, 40 Hz pulse repetition frequency (PRF), 8 MPa peak focal pressure, and a 20 cycle pulse duration. At these settings, BWL consistently yielded small stone fragments, typically less than 2 mm.
UP system
A P4-2 diagnostic ultrasound probe (Philips Healthcare, Bothell, WA), connected to a Verasonics V-1 imaging system (Verasonics, Kirkland, WA) was positioned through a central aperture in the BWL transducer to be in line with the BWL focus. The P4-2 probe/Verasonics system served two roles: (1) It provided B-mode imaging for stone targeting on the imaging display, and (2) it generated UP pulses from the probe at preselected rates and amplitudes. UP settings were adjusted from prior studies of stone repositioning9,16 to administer relatively weaker pulses so that stones would be agitated but remain within the treatment focus area. For propulsion, 2.5 MHz pulses with pulse duration of 45 ms were applied to the stone at a peak pressure amplitude of ∼0.15 MPa. BWL and propulsion were not synchronized for interleaved exposure, although a majority of BWL pulses did not overlap propulsion pulses because of the different pulse repetition frequencies.
Experimental setup
The in vitro lithotripsy experiments were performed a 20-gallon tank filled with deionized, degassed water at 20% O2 saturation. The BWL transducer, imaging probe, and tissue phantom (with stone) were mounted inside the tank with the transducer and probe facing upward such that the center of the tissue phantom calyx was aligned with the transducer and probe foci (Fig. 2).
FIG. 2.

(A) In vitro lithotripsy experimental setup. A BWL therapy transducer was positioned in a bath of water underneath a PVC tissue phantom containing a stone. The focus was aligned to the stone by an ultrasound imaging probe in the center aperture of the BWL transducer. The imaging probe was also used to produce propulsion pulses during exposures. (B) A pulse timing diagram for the UP and BWL pulses applied in this study. Frequency, pulse duration, and amplitude were fixed. PRF for BWL was also fixed, whereas propulsion PRF varied between 1 and 60 pulses per minute. Propulsion and BWL pulses were not synchronized. Amplitudes and time in the diagram are not to scale. PRF = pulse repetition frequency; PVC = polyvinyl chloride; UP = ultrasonic propulsion.
All stone types were presoaked in water for at least 24 hours and weighed just before treatment. During treatment, ultrasound imaging was intermittently checked to ensure the stone remained within the transducer/probe focus. After treatment the remaining stone and associated fragments ≥2 mm in size were collected in an appropriate size mesh sieve and weighed to determine the proportion of stone mass treated. Stone fragments <2 mm were considered successfully treated due to their high probability of clinically passing spontaneously. Significance of differences in fragmented mass and stone fragmentation rate was calculated by a Student's t-test, with statistical significance set at p < 0.05.
Experimental trials
A set of BegoStone models was exposed in 5-minute intervals until complete comminution was achieved to measure the temporal progression of fragmentation with and without interleaved propulsion at 6 pulses per minute (n = 3 for each exposure condition).
In a second experiment, BegoStone models were treated for a fixed interval of 10 minutes with BWL and interleaved propulsion with rates ranging from 0 to 60 propulsion pulses per minute (n = 10 per rate setting) to examine the effect of rate on stone fragmentation. We chose this exposure time frame to produce measurable, but not complete comminution to detect differences between groups. The time needed for partial comminution was different between stone types, thus we chose different exposure times for different stone types below.
A separate trial using BegoStone models examined whether BWL and UP need to be applied interleaved vs sequentially for improved fragmentation. For these sequential exposures, BWL was administered for 10 minutes (n = 10), turned off, then followed by UP for 10 minutes at 6 pulses per minute.
We also performed exposures on two other stone compositions: artificial calcite stones and human COM stones. Calcite stones were exposed to either a 5-minute BWL-only treatment (n = 13) or a BWL treatment with interleaved propulsion pulses at 3 per minute (n = 10). Human COM stones, 5 to 8 mm in maximum dimension treated for 5 minutes. We compared stone breakage between BWL alone (n = 14) and BWL with interleaved UP at 6 (n = 12) or 60 (n = 16) propulsion pulses per minute.
Results
BegoStone models could be completely comminuted in a time of 45 to 60 minutes with BWL alone, vs 30 to 40 minutes when exposed to combined BWL and propulsion pulses (Fig. 3). The mass loss was nearly linear with time, although appeared slightly accelerated toward the end of treatment. A linear least-squares fit of data indicated a mass loss of 15.9 mg/min for BWL alone vs 24.5 mg/min for BWL+propulsion, yielding a statistically significant difference (p < 0.001).
FIG. 3.

Average proportion of stone fragmented vs time for BegoStone models exposed to BWL alone (empty squares) and BWL+UP (filled circles). The dashed lines are least-square fits to a linear regression model. Error bars indicate standard deviation.
With BegoStone models, we found a rate-dependent response to fragmentation combined with propulsion. Application of only 1 pulse per minute over 10 minutes substantially increased stone breakage (22% ± 3% vs 6% ± 1%, p < 0.01), although the peak pressure of the propulsion pulses is a small fraction of that from BWL. Stone fragmentation improved with increasing pulse rate, up to 35% ± 5% at 60 pulses per minute (p < 0.01) (Fig. 4).
FIG. 4.

Fragmentation efficacy of BegoStone models exposed to BWL+UP at varying pulse rates (n = 10 for each setting).
The sequence of BWL and propulsion application altered stone fragmentation. BWL alone treated 5.9% ± 1.3% of the total stone mass. When propulsion was administered sequentially after BWL, this led to a 1.9-fold increase in stone fragmentation 11% ± 2% vs BWL alone (p < 0.01). However, when BWL and UP were interleaved, 27% ± 2% of the stone mass was comminuted (p < 0.01), a 4.6-fold increase in stone fragmentation compared to BWL alone (p < 0.01) (Fig. 5).
FIG. 5.

Fragmentation efficacy of BegoStone models by combined exposure under different temporal configurations (n = 10 each group). An effect is shown with both sequential and interleaved exposures, but interleaved produced a stronger improvement in fragmentation.
In the calcite stone trials, BWL alone fragmented 24% ± 19% of the total stone mass. When propulsion was interleaved with BWL, an average 39% ± 24% of the total stone was broken into fragments <2 mm (p = 0.047), a 66% increase in stone fragmentation (Fig. 6A).
FIG. 6.

(A) Fragmentation of calcite stones achieved after exposure to BWL with/without UP at a rate of 3 pulses per minute (n = 13 for BWL only group and n = 10 for BWL+propulsion group). (B) Fragmentation efficacy of human COM stones exposed without and with UP at rates of 6 and 60 pulses per minute. COM = calcium oxalate monohydrate.
COM stone fragmentation was qualitatively similar to artificial stones, with small fragments ejecting from a larger remaining stone segment. Compared with BWL alone (17% ± 11%), there was no significant difference when administering interleaved propulsion pulses at 6 per minute (26% ± 26%) (p = 0.13); however, there was a significant increase in stone fragmentation, approximately twofold compared with BWL only, at 60 per minute (36% ± 28%) (p = 0.014) (Fig. 6B).
Discussion
The addition of ultrasound propulsion pulses appears to accelerate stone treatment during BWL in vitro. The effect is strongest when performed interleaved with BWL and with a faster rate of propulsion pulses.
Four ideas are discussed for the complementary effect. The first explanation is that the propulsion is physically ejecting fragments loosely attached to the stone. BWL usually proceeds by creating numerous fractures in the stone before fragmentation. Even gentle handling of the stone can cause fragments to fall off after treatment. Thus, radiation force may simply remove weakened fragments from the surface.
A second potential explanation is that the propulsion reorients the stone, exposing multiple sides to the incident BWL pulses. This reorientation could cause a redistribution of stresses in the stone, leading to fractures in new locations. An occasional repositioning could be beneficial depending on the time for fractures to develop. A possible experiment to evaluate this hypothesis would be to adhere the stone in a fixed position during exposure to determine the importance of reorientation.
A third possibility is that propulsion removes dust and residual cavitation bubbles on or around the stones that could shield it from BWL pulses. Shielding has been demonstrated in vitro for SWL and is an explanation for improved lithotripsy with lower shock wave rates to reduce cavitation shielding.17 The larger increase in fragmentation with BegoStone models, compared with calcite or COM stones, may be attributed to this effect. Because they are generated from a fine powder, the BegoStone models produce continuous dust (in addition to fragments) during treatment that could potentiate cavitation and shield the stone from BWL exposure. Calcite stones and COM stones form no and minimal dust, respectively. The UP pulses appeared to remove this dust readily, which could explain the more dramatic improvement in fragmentation observed with these stones compared with the other two stone types. However, the removal of dust clouds by themselves is not the sole cause for the complementary effect, as calcite stones do not create such dust. This effect may be tested by introducing fluid flow to remove dust and bubbles during a BWL treatment to see if a similar improvement in efficacy is observed.
A fourth hypothesis is that UP pulses are further stressing cracks in the stone or oscillating cavitation bubbles on the surface of the stone contributes to the overall damage to the stone. This is less likely as we have not seen stones fragment during UP. With each of these hypotheses, additional work is needed to pinpoint the exact mechanism.
Although the primary goal of adding UP to BWL is increasing lithotripsy efficiency, there may be additional safety benefits through decreasing the time and energy for BWL to treat a stone. Preliminary testing suggests increasing BWL signal amplitude (focal peak pressure) will expedite lithotripsy; however, there is a theoretical increased risk for collateral tissue injury,15 which is also known to occur in shock wave lithotripsy as peak pressure amplitudes and number of shocks increase. No injury or pain has been found from UP pulses alone, which yield peak pressures at a fraction of BWL.10,18,19 Thus, adding propulsion to BWL, even 1 pulse per minute, can significantly improve fragmentation at minimal added risk.
Calcite and human COM stones demonstrated larger standard deviation in fragmentation and a smaller improvement compared with BegoStone models. The larger variation was likely due to more heterogeneity in stone shape, size, and density of the calcite and COM stones, whereas the BegoStone models were nearly identical to each other. The human COM stones may have also already undergone partial fragmentation before collection.
This study had several additional limitations. We did not capture the full time course of fragmentation for all stones, but rather treated with a fixed time interval. However, those for which we did capture temporal data indicate that the fragmentation is fairly linear with time, thus a single interval is still useful in comparing between groups and estimating the utility of the combined treatment. Using a simplified in vitro model may not accurately reflect true in vivo or clinical conditions. While the experiment used a tissue phantom that mimics human tissue properties, and both artificial and natural stones, other factors such as differences in the fluid and variation in stones could cause different responses. The effect should be tested with more complex in vivo models and clinical testing to confirm the benefit of combined exposure. Additionally, the majority of experiments were carried out with artificial stones and fragments of human COM stones, which may not accurately reflect the response of intact human stones to similar treatment conditions. However, the complementary effect of propulsion and variability of human COM fragmentation closely matched that of calcite stones, suggesting comparability. For the purpose of understanding the basic synergy, each stone model had a different advantage. BegoStone models allowed for consistent stone weight, shape, and size across trials. Calcite stones served as a stone model that did not produce dust. COM stones demonstrated the applicability of the effect to human stones.
We evaluated only a small subset of BWL and UP parameters, and both of these technologies may be further optimized in vitro and in vivo. In this study, propulsion was produced by an imaging probe integrated with the BWL therapy transducer. It is also possible that propulsion could be applied from the therapy transducer itself. Future work in these areas will further evaluate the effectiveness of the combined treatment. We plan to also identify the primary mechanisms causing this synergy, which may lead to improvements in the effectiveness of this treatment strategy. Despite the limitations, this study demonstrates an advance in the efficiency of stone treatment with these novel minimally invasive therapies.
Conclusion
Application of UP to BWL can accelerate the fragmentation of both natural and artificial stones in vitro. The effect is strongest when pulses are interleaved with BWL and as the propulsion pulse rate is increased. This strategy can be easily implemented using an existing system with BWL.
Abbreviations Used
- BWL
burst wave lithotripsy
- COM
calcium oxalate monohydrate
- SWL
extracorporeal shock wave lithotripsy
- UP
ultrasonic propulsion
- URS
ureteroscopy
Acknowledgments
The first two authors contributed equally to this work. The authors thank Christopher Hunter from the University of Washington Applied Physics Laboratory for his assistance in data analysis. This work was supported by National Institutes of Health NIDDK P01 DK043881 and NIDDK K01 DK104854, resources through the VA Puget Sound Healthcare System, and the University of Washington Applied Physics Laboratory Boeing Scholars program.
Author Disclosure Statement
B.W.C., M.R.B., B.D., M.D.S., and A.D.M. have equity in and consulting agreements with SonoMotion, Inc, which has licensed technology related to this work from the University of Washington. The other authors have no competing conflicts of interest.
References
- 1.Lotan Y, Gettman MT, Roehrborn CG, Cadeddu JA, Pearle MS. Management of ureteral calculi: A cost comparison and decision making analysis. J Urol 2002;167:1621–1629 [PubMed] [Google Scholar]
- 2.Matlaga BR, Jansen JP, Meckley LM, Byrne TW, Lingeman JE. Economic outcomes of treatment for ureteral and renal stones: A systematic literature review. J Urol 2012;188:449–454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Oberlin DT, Flum AS, Bachrach L, Matulewicz RS, Flury SC. Contemporary surgical trends in the management of upper tract calculi. J Urol 2015;193:880–884 [DOI] [PubMed] [Google Scholar]
- 4.Scales CD, Jr., Lai JC, Dick AW, et al. Comparative effectiveness of shock wave lithotripsy and ureteroscopy for treating patients with kidney stones. JAMA Surg 2014;149:648–653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cone EB, Eisner BH, Ursiny M, Pareek G. Cost-effectiveness comparison of renal calculi treated with ureteroscopic laser lithotripsy versus shockwave lithotripsy. J Endourol 2014;28:639–643 [DOI] [PubMed] [Google Scholar]
- 6.Grasso M, Loisides P, Beaghler M, Bagley D. The case for primary endoscopic management of upper urinary tract calculi: I. A critical review of 121 extracorporeal shock-wave lithotripsy failures. Urology 1995;45:363–371 [DOI] [PubMed] [Google Scholar]
- 7.Maxwell AD, Cunitz BW, Kreider W, et al. Fragmentation of urinary calculi in vitro by burst wave lithotripsy. J Urol 2015;193:338–344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhu S, Cocks FH, Preminger GM, Zhong P. The role of stress waves and cavitation in stone comminution in shock wave lithotripsy. Ultrasound Med Biol 2002;28:661–671 [DOI] [PubMed] [Google Scholar]
- 9.Sorensen MD, Bailey MR, Hsi RS, et al. Focused ultrasonic propulsion of kidney stones: Review and update of preclinical technology. J Endourol 2013;27:1183–1186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Harper JD, Cunitz BW, Dunmire B, et al. First in human clinical trial of ultrasonic propulsion of kidney stones. J Urol 2016;195(4 Pt 1):956–964 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shah A, Harper JD, Cunitz BW, et al. Focused ultrasound to expel calculi from the kidney. J Urol 187:739–743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Liu Y, Zhong P. BegoStone—A new stone phantom for shock wave lithotripsy research. J Acoust Soc Am 2002;112:1265–1268 [DOI] [PubMed] [Google Scholar]
- 13.Blitz BF, Lyon ES, Gerber GS. Applicability of Iceland spar as a stone model standard for lithotripsy devices. J Endourol 1995;9:449–452 [DOI] [PubMed] [Google Scholar]
- 14.Spirou GM, Oraevsky AA, Vitkin IA, Whelan WM. Optical and acoustic properties at 1064 nm of polyvinyl chloride-plastisol for use as a tissue phantom in biomedical optoacoustics. Phys Med Biol 2005;50:N141–N153 [DOI] [PubMed] [Google Scholar]
- 15.May PC, Kreider W, Maxwell AD, et al. Detection and evaluation of renal injury in burst wave lithotripsy using ultrasound and magnetic resonance imaging. J Endourol 2017;31:786–792 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shah A, Owen NR, Lu W, et al. Novel ultrasound method to reposition kidney stones. Urol Res 2010;38:491–495 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pishchalnikov YA, McAteer JA, Williams JC., Jr. Effect of firing rate on the performance of shock wave lithotriptors. BJU Int 2008;102:1681–1686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Harper JD, Dunmire B, Wang YN, et al. Preclinical safety and effectiveness studies of ultrasonic propulsion of kidney stones. Urology 2014;84:484–489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wang YN, Simon JC, Cunitz BW, et al. Focused ultrasound to displace renal calculi: Threshold for tissue injury. J Ther Ultrasound 2014;2:5. [DOI] [PMC free article] [PubMed] [Google Scholar]