

Introduction
Lichen planus (LP) and other skin conditions have been reported in association with chronic hepatitis infections, specifically hepatitis C. However, this association is controversial, with comparative studies finding no significant difference in prevalence.1, 2, 3
Reports of LP arising in association with chronic hepatitis B infections are even less common. A systemic review of 151 cases in 44 papers studying cutaneous lesions in hepatitis B immunization, infection, or therapy only found 1 patient with chronic hepatitis B who had a lichenoid lesion.4
LP has been reported to develop or worsen with interferon therapy, largely in the context of hepatitis C.4, 5, 6 A prospective study found that of 67 patients with hepatitis B and 45 patients with hepatitis C treated with recombinant interferon α (IFN-α), 1 patient with hepatitis B and 2 with hepatitis C developed LP.5 Another study of 271 patients with hepatitis C treated with peginterferon and ribavirin found an exacerbation of lichen planus in 1 patient.6 A case of LP in a chronic hepatitis B carrier after starting peginterferon for delta hepatitis has also been reported.7
To our knowledge, apart from the above single case,5 there have been no other reports of de novo lichen planus developing after IFN therapy for hepatitis B. We report a case of erosive oral lichen planus after peginterferon therapy for chronic hepatitis B infection.
Case report
A 53-year-old woman with a history of hepatitis B liver cirrhosis was treated unsuccessfully with entecavir for 5 years. She had persistently detectable hepatitis B virus DNA levels in her blood and consequently was given peginterferon α-2b at a dose of 1.5 mcg/kg subcutaneously weekly for 48 weeks. She was negative for hepatitis C virus antibody.
At week 21 of IFN therapy, she began to report a burning, sharp sensation in the mouth that worsened with cold food. The symptoms became progressively worse with the development of oral ulcers as she completed a total of 48 weeks of IFN therapy. Her only other medication was lovastatin.
The ulcers persisted for 1 year despite cessation of IFN therapy, and she was referred to a dermatologist. On examination, there were atrophic and ulcerated erythematous plaques on the buccal mucosal surface with white striae (Figs 1 and 2). She did not have hair, skin, or nail changes. She continued to have a detectable hepatitis B viral load during follow-up.
Fig 1.

Oral lichen planus. Superficial ulcerated erythematous plaque over the buccal mucosa.
Fig 2.

Oral lichen planus. Wickham striae or whitish striations on buccal mucosa.
She underwent an incisional biopsy, which demonstrated a lichenoid lymphoplasmacytic infiltrate in the subepithelial stroma. The overlying squamous epithelium showed saw-toothed rete ridges, neutrophilic and lymphocytic exocytosis, occasional apoptotic keratinocytes, intercellular edema, and parakeratosis (Figs 3 and 4). This was consistent with oral lichen planus.
Fig 3.
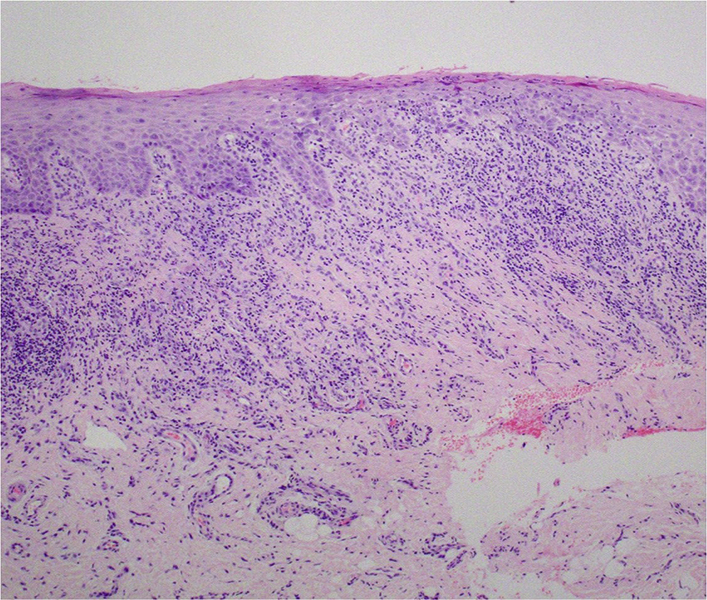
Photomicrograph of the oral mucosa showing a band-like lichenoid inflammation with saw-tooth rete ridges. (Hematoxylin-eosin stain; original magnification: ×40.)
Fig 4.
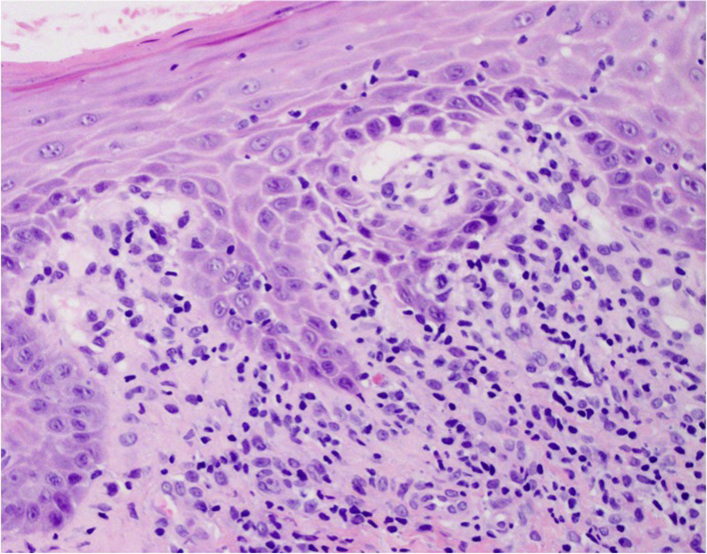
High-power view of oral mucosa showing saw-tooth rete ridges with vacuolar interface change. (Hematoxylin-eosin stain; original magnification: ×200.)
She was prescribed triamcinolone dental paste and reported an improvement in pain and burning discomfort over the next 4 weeks, with the ulcer decreasing in size.
Discussion
The role of IFN-α in the pathogenesis of oral LP has been postulated to relate to the cytokine cascade. IFN-α has been suggested to stimulate T cells and amplify the TH1 response by upregulating interleukins. Furthermore, IFN-α could promote T helper cell accumulation, migration, and adhesion to keratinocytes, resulting in cell toxicity.8, 9 The appearance of LP after IFN-α therapy has been reported in the context of malignancy, which could suggest an association independent of hepatitis B or C infection.8 The greater bioavailability and longer half-life of pegylated IFN compared with conventional IFN-α could increase the likelihood of developing or worsening LP.10
This rare case of erosive oral lichen planus arose in a patient treated with pegylated IFN for hepatitis B cirrhosis. The possible causality of LP with IFN therapy stems from the fact that LP began after initiation of IFN therapy. Regardless, of causal or incidental association, oral ulcers are common findings in patients on IFN therapy; a physician should be alerted to the differential of oral LP in a patient with nonhealing oral lesions plus risk factors and consider a biopsy for diagnosis.
Footnotes
Funding sources: None.
Conflicts of interest: None declared.
References
- 1.Friedrich R.E., Heiland M., El-Moawen A., Dogan A., von Schrenck T., Loning T. Oral lichen planus in patients with chronic liver diseases. Infection. 2003;31(6):383–386. doi: 10.1007/s15010-003-4074-5. [DOI] [PubMed] [Google Scholar]
- 2.Maticic M., Poljak M., Lunder T., Rener-Sitar K., Stojanovic L. Lichen planus and other cutaneous manifestations in chronic hepatitis C: pre- and post-interferon-based treatment prevalence vary in a cohort of patients from low hepatitis C virus endemic area. J Eur Acad Dermatol Venereol. 2008;22(7):779–788. doi: 10.1111/j.1468-3083.2008.02676.x. [DOI] [PubMed] [Google Scholar]
- 3.Remmerbach T.W., Liese J., Krause S. No association of oral lichen planus and hepatitis C virus infection in central Germany. Clin Oral Investig. 2016;20(1):193–197. doi: 10.1007/s00784-015-1602-5. [DOI] [PubMed] [Google Scholar]
- 4.Grigorescu I., Dumitrascu D.L. Spontaneous and antiviral-induced cutaneous lesions in chronic hepatitis B virus infection. World J Gastroenterol. 2014;20(42):15860–15866. doi: 10.3748/wjg.v20.i42.15860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dalekos G.N., Christodoulou D., Kistis K.G., Zervou E.K., Hatzis J., Tsianos E.V. A prospective evaluation of dermatological side-effects during alpha-interferon therapy for chronic viral hepatitis. Eur J Gastroenterol Hepatol. 1998;10(11):933–939. doi: 10.1097/00042737-199811000-00006. [DOI] [PubMed] [Google Scholar]
- 6.Patrk I., Morovic M., Markulin A., Patrk J. Cutaneous reactions in patients with chronic hepatitis C treated with peginterferon and ribavirin. Dermatology. 2014;228(1):42–46. doi: 10.1159/000353160. [DOI] [PubMed] [Google Scholar]
- 7.Kaya S., Arslan E., Baysal B., Baykara S.N., Uzun O.C., Kaya S. Lichen planus induced by pegylated interferon alfa-2a therapy in a patient monitored for delta hepatitis. Case Rep Infect Dis. 2015;2015:389131. doi: 10.1155/2015/389131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pinto J.M., Marques M.S., Correia T.E. Lichen planus and leukocytoclastic vasculitis induced by interferon alpha-2b in a subject with HCV-related chronic active hepatitis. J Eur Acad Dermatol Venereol. 2003;17(2):193–195. doi: 10.1046/j.1468-3083.2003.00583.x. [DOI] [PubMed] [Google Scholar]
- 9.Jadali Z. Dermatologic manifestations of hepatitis C infection and the effect of interferon therapy: a literature review. Arch Iran Med. 2012;15(1):43–48. [PubMed] [Google Scholar]
- 10.Higuchi M., Tanaka E., Kiyosawa K. Epidemiology and clinical aspects on hepatitis C. Jpn J Infect Dis. 2002;55(3):69–77. [PubMed] [Google Scholar]