

ABSTRACT
Many resource-limited countries are scaling up health services and health-information systems (HISs). The HIV Cascade framework aims to link treatment services and programs to improve outcomes and impact. It has been adapted to HIV prevention services, other infectious and non-communicable diseases, and programs for specific populations. Where successful, it links the use of health services by individuals across different disease categories, time and space. This allows for the development of longitudinal health records for individuals and de-identified individual level information is used to monitor and evaluate the use, cost, outcome and impact of health services. Contemporary digital technology enables countries to develop and implement integrated HIS to support person centred services, a major aim of the Sustainable Development Goals. The key to link the diverse sources of information together is a national health identifier (NHID). In a country with robust civil protections, this should be given at birth, be unique to the individual, linked to vital registration services and recorded every time that an individual uses health services anywhere in the country: it is more than just a number as it is part of a wider system. Many countries would benefit from practical guidance on developing and implementing NHIDs. Organizations such as ASTM and ISO, describe the technical requirements for the NHID system, but few countries have received little practical guidance. A WHO/UNAIDS stake-holders workshop was held in Geneva, Switzerland in July 2016, to provide a ‘road map’ for countries and included policy-makers, information and healthcare professionals, and members of civil society. As part of any NHID system, countries need to strengthen and secure the protection of personal health information. While often the technology is available, the solution is not just technical. It requires political will and collaboration among all stakeholders to be successful.
KEYWORDS: National health identifiers, resource limited countries, health-information systems, confidentiality security personal health information, person-centred care
Background
The ‘HIV Health Sector Cascade’ framework was recently introduced to monitor and evaluate a country’s HIV Response (Figure 1). This framework was first developed at CDC [1] and has since been developed in many countries, and forms the basis of the UNAIDS ‘90–90–90’ targets [2]. Similar frameworks are now being applied to HIV prevention [3], to specific sub-populations enrolled in particular programs [4], and to other communicable [5] and non-communicable diseases (NCDs) [6].
Figure 1.
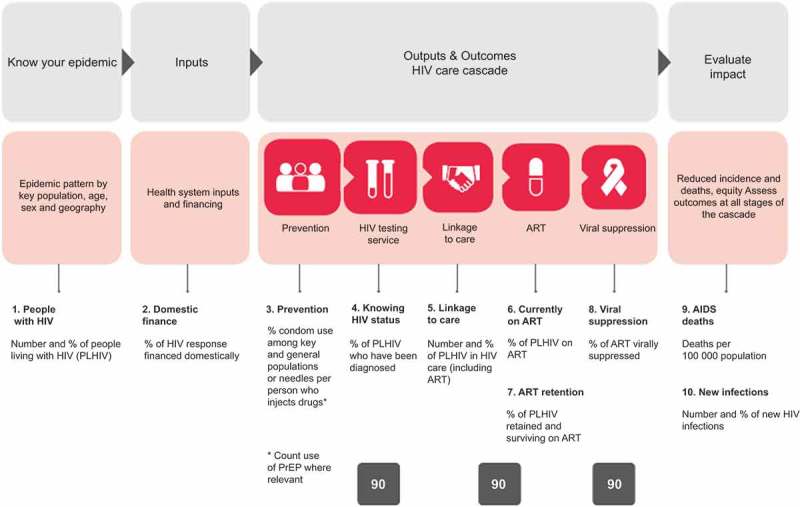
Ten WHO indicators assessing the ’90–90-90’ program showing linkages with other sources of data including case based surveillance and patient monitoring.
The framework tracks the use of different services by individuals and populations across disease categories, time and place, and aims to link information from a range of different sources, including vital statistics, person-centred patient monitoring and case surveillance (Figure 1) [7,8]. As individuals are tracked across different services, their information can be linked to develop longitudinal medical records. De-identified individual level information collected can also provide policy-makers, clinicians, PLHIV and other stakeholders with information to monitor and evaluate health services at facility, sub-national and national levels [9].
The implementation of anti-retroviral (ART) programs has increased the number of PLHIV in many resource limited countries, as their life-expectancy on ART approximates that of people not living with HIV, provided life-time ART is started with a CD4 count greater than 500 cells/mm3 [10]. The World Health Organization (WHO) now recommends that starting ART at time of diagnosis [11] and that will result in increased number of PLHIV aged 50 years or older [12]. The most common co-morbidities of older PLHIV are non-HIV cancers, cardiovascular disease and other NCDs, and these are also their commonest cause of death [13]. PLHIV will therefore increasingly need to use non-HIV services, especially in countries with successful HIV responses. To monitor and evaluate the HIV-response in these countries, the use, cost, outcome and impact of NCDs’ services used by PLHIV will also need to be tracked, especially as integrated HIV and non-HIV services are likely to be more cost-effective [14]. Such integration can contribute to the development of services for other chronic conditions in resource limited countries, especially as NCDs are an important cause of morbidity and mortality in their own right [15].
The use of health services within a country should be tracked across facilities and the personal health information linked over time as part of providing universal health coverage [16]. Countries increasingly recognize this need; while some still focus only on developing their HIV Cascade, other resource limited countries now recognize the need to develop and implement their HIS across all healthcare sectors. While Zambia has developed an extensive HIV specific cascade [17], AMPATH in western Kenya, which started as an HIV system, has now been expanded into a network of facilities that provides health services for a range of other diseases including HIV [18]. Some countries are even more ambitious and want to link healthcare information with information obtained from insurance systems, social services or other societal sectors, as has been developed in Denmark [19].
To ensure optimal service delivery across such a variety of sites, specific identifiers need to exist which link all information to that individual [20]. In health facilities, facility-identifiers are alpha-numeric codes used to identify an individual within that particular facility. Within facilities, different clinics may have their own identifier, clinic-identifiers. Several facilities can be linked with each other to provide services through a particular program, for instance a tuberculosis (TB)-program. Individuals who are part of that program can have specific program identifiers that track the use of services by that individual within the program. However, neither facility- nor program-identifiers can be used outside the specific facility or program, and the use of services used outside the facility or program cannot be tracked and data not linked. To link these data an identifier needs to capture all healthcare services; a national health identifier (NHID). NHID should be universally unique within the country’s health system, is assigned to an individual for life, is never used for another individual, and can be linked to track an individual through their health journey as they use services at different facilities or within different programs [20]. The five basic functions that a NHID should support and its seven core elements are described in Box 1.
Box 1.
The five basic functions and seven core elements of a NHID [20].
The five basic functions that a NHID should support are:
|
The seven core elements of a NHID, required for the system to perform its functions consist of:
|
Paper, power and network: three tier developmental infrastructure
While the development and implementation of NHID are facilitated by the existence of reliable electricity supplies in health facilities, in low- and middle-income countries many facilities may have no or limited access to electricity, computers or the internet; the presence or absence of electricity is a major defining factor. As infrastructure develops, health centres undergo technology transitions and three tiers of permanent facilities are recognized, while transient health posts and community-based care comprise Tier 0 facilities:
Tier 1 – Paper: facilities with no reliable power or telecom; cold chain may be burner powered.
Tier 2 – Power: facilities with a minimum of reliable daily power – solar, generator, power lines and uninterrupted power supply (UPS) – sufficient to charge/operate an efficient computer.
Tier 3 – Network: facilities with reliable daily telecommunications and power, at least sufficient to have certain deferrable clinic operations normally depended on internet-based applications.
Tier 1 health facility: operations provide continuity of care for patients across the system platform but for specific clinical programs, using semi-durable and portable paper documents. Familiar examples are ante-natal clinic (ANC) cards, delivery records, under-five cards for tracking growth and immunizations in children, and TB cards. South Africa has a ‘Road to health chart’ [21] that is used to track child care and is a requirement for a child to be enrolled in primary school. Most clients who need them carry them for the duration of using the service. Each of these tools provides a degree of continuity within the scope of a single protracted service. Each program may issue its own identifier for the duration of the episode of care and life of the paper documents: primary care records are usually collected in free form text.
Some countries have developed documents or ‘health passports’ which integrate some program specific information with general primary care records [22] but they have a finite capacity before needing to be restarted with a blank document. These are used across health programs and kept by patients. In other situations, clients may be expected to provide their own paper document, perhaps a student exercise book, for recording the clinical visit, and there is variability whether the facility or client retains the document.
Finding older paper documents may be difficult to do with consistency; after a certain number of years, old documents are archived or discarded to make room for new. Filing and retrieval may be improved by using a single standardized identifier; however, sharing a single physical copy record can introduce contention between programs due to their specific needs. Whether integration of a single physical record per facility might reduce the small degree of within-program discontinuity that years of paper operational experience produced, would need to be assessed and might depend on the filing logistics and size of the facility. The consensus is, however, that the use of a unified, cross-programmatic identifier is a pre-requisite to improve continuity of care across health services within as well as between health facilities.
Providing good long-term or complex care with paper records, without fax, copier or good paper supply, is quite hard but an important first step for linking records. If a client is mobile, continuity of care generally fails due to paper record sharing difficulty, not for lack of an NHID. Fixing these issues with Tier 1 resources is sometimes more difficult and less fruitful than efforts to get electricity. Sites need power to most effectively and efficiently implement the continuity of care purpose of a NHID.
Tier 2/3 – Electric facilities: due to the critical mass of a changing national economy, growing population or political developments, a more reliable electrical infrastructure with some excess capacity may be achieved, and the paper facility transitions to a Tier 2 – electric facility. This is the biggest and most enabling infrastructure transition.
In Zambia, 220 out of 1138 (19%) Tier 1–3 health facilities in 2000 had sufficient power for a simple decentralized electronic health record (EHR) with one computer, printer, universal serial bus (USB) smart card reader, and UPS. This number increased to 989 out of 1781 (56%) in 2008, and to an estimated 1200 out of 2405 (50%) facilities with basic electricity by early 2014. During this same period the population grew from 10 to over 14 million people (Figure 2).
Figure 2.
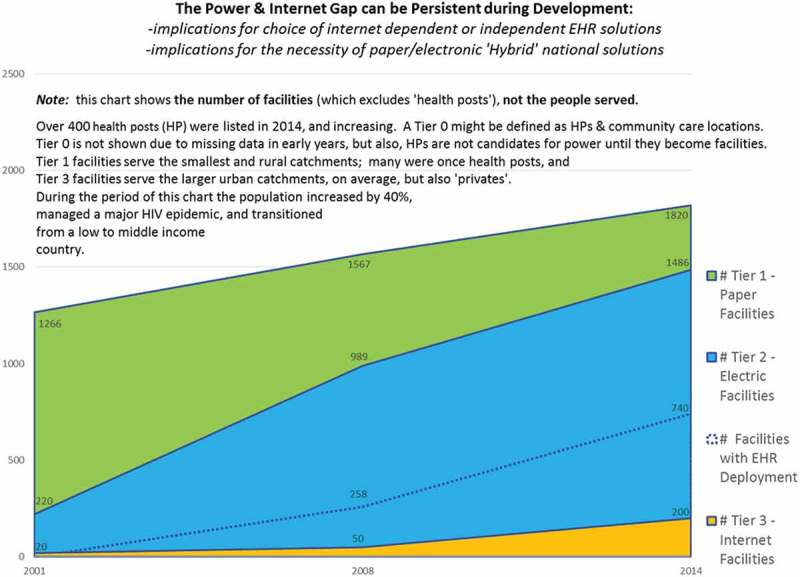
The transition from Tier 1 to Tier 3 facilities, sub-Saharan country 2000–2014.
While a Tier 1 ‘paper’ facility might hope to have developed to Tier 3 in 5–10 years, this does not mean that in just 5 years there will be no need for a hybrid system, or that the country should plan to upgrade immediately to an internet dependent EHR solution. If a country has a large number of Tier 1 and 2 facilities, an internet dependent design – Tier 3 – may not be optimal. Deployment of internet dependent solutions might block a large percentage of the population from receiving good continuity of care that can be delivered without the internet, for instance via a smart card held by the client. The latter can be used to store essential elements of any health records, along with identifier and quasi-identifier authentication elements.
Although an internet-based solution may provide added value in some clinics as the infrastructure develops, additional and more remote clinics may be built as a country’s population grows, that will often start as a Tier 1 paper facility before developing over time Tier 2 electrical capacities. However, even in fully electronic environments, paper ‘back-ups’ may be required. When there is a down-turn in the economy, infrastructure development may stall or even regress, and systems need to continue to function during hard times. In addition, systems should be designed that continue to function during natural or man-made disasters.
Developing and implementing a NHID and NHID-system
The development and implementation of a NHID is a system-wide process and to be successful the first step is carry out a comprehensive assessment (Figure 3). Early in this process a group of dedicated stakeholders should be brought together, who will start to define the vision for the country. All stakeholders that need to be involved in the process and are willing to act as medium- to long-term champions, need to be identified and engaged. This process also needs to provide a technical review of the health-information system operative in the country, drawing on all available information including secondary sources.
Figure 3.
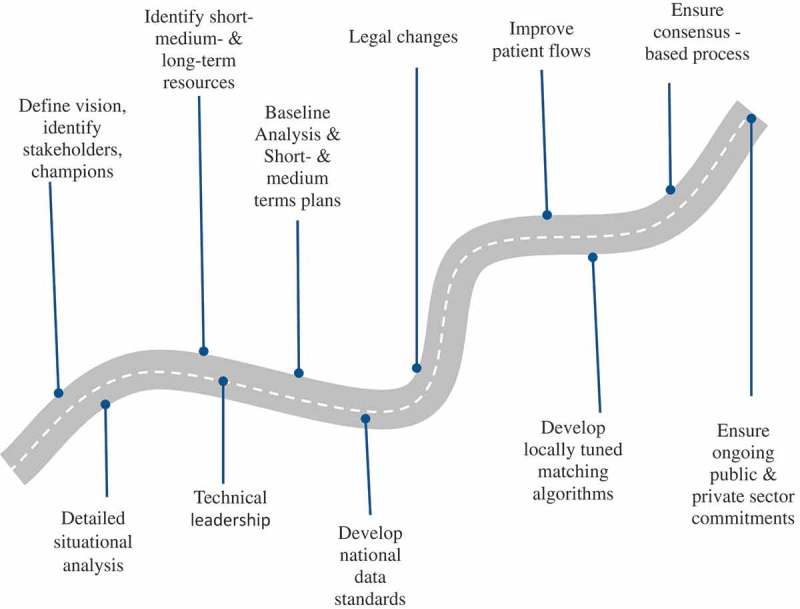
Initial steps to develop a NHID system.
The forms currently in use by the Ministry of Health and the data currently routinely collected by them need to be reviewed and assessed. Similarly, the key health service issues need to be identified and the extent that better information can address them, collected through a better information infrastructure or updated laws. The uses of a NHID need to be circumscribed as how they contribute to improvement of services and a decision made whether to focus on the public sector or also include the private health sector. An inventory of existing identifiers used in the country by major systems needs to be drawn up, their use and structure described as well as that of quasi-unique identifiers used in these same systems. Existing record linkage and de-duplication efforts also need to be identified. For example, one approach could be to consolidate the various systems, making use of matching algorithms to allocate NHIDs to existing information, and then use the new NHID to go forwards. It is important to consider legislation that governs existing identifiers and appropriate control of access to information. This will provide useful input into understanding governance arrangements between the authorities, using existing identifiers to link, access and use the information.
A baseline appraisal of the existing national health informatics infrastructure needs to be made, including the review of past assessments and secondary data (Box 2). The existing separate health-information systems in the various facilities need to be listed, the modules they support and users’ experiences with them. The strength of the development teams of any of the commercial systems needs to be assessed and the costs of integration, data conversion and scaling up to country level need to be explored. The top 5–10 systems in chosen sectors need to be explored in depth, to be able to identify which will become the inventory of health information standards and systems used in the country. The ownership of the information, which is created by linking data from the health sectors, needs to be agreed on.
Box 2.
Baseline assessment of existing national health information infrastructure.
|
Information technology professionals need to be identified for software development, database administration and networking, including health informatics and system analysts. In addition, persons who have experience in record linkage for multimillion record files also need to be identified. Ensure that software from vendors are used that can generate NHIDs based on local requirements and any vendor solutions should be owned by the country to avoid being locked in to any one vendor. Alternatively, ensure links to NHIDs generated by third-party systems can adapt to changing requirements. Identification of the right software systems, vendors and support infrastructure are key considerations, as these are part of an ever-evolving environment.
Identify or develop staff who can supervise the use and quality of data being collected, and analyse the data to provide feedback on the evolving structure of service provision. Find the best academic programs and talk to relevant academics while keeping abreast of new developments. Assess existing laws, regulation and policies, including human rights protection, information ownership and stewardship, information standards, accountability and governing authorities. Assess public perception, trust and buy-in for the vision of a NHID, popular conceptions or misconceptions. Assess existing privacy, confidentiality and security guidelines, and their implementation in the health sector in terms of data collection, access, storage, transfer, use, disposal and data stewardship. Based on this assessment, the process of changing any necessary legal and statutory requirements to deposit personal health information in data warehouses or repositories can commence. In parallel, one needs to make an assessment of operative administrative business processes and improve these where required and if possible.
Define the vision and the resources required
Focus on the benefits to the whole system that the NHID enables in terms of healthcare in a country and not on the actual NHID implementation. Reflect the sense of the needs and ambitions in the country that were uncovered during the assessment. It should be produced and owned through a group effort, including some key people who are committed to the vision they formulate. Find champions for the vision who are socially accepted, persistent and committed. These should be sought among clinicians, other healthcare professionals, academics, civil servants, politicians and community leaders. Share and sell the vision and try to link such a long-term project to multi-party support and not one political platform, while recognizing and highlighting the benefits obtained from each progressive step towards achieving the vision.
Identification and assessment of resources is a continuous process of developing and implementing large, multi-year, national systems efforts. Evaluate available resources in terms of funding, technical infrastructure, information, communication and technology, human resources, including technical, legal, political and civil society leaders. Different resources will come to bear for different areas and stages of the implementation. Similarly, different benefits will come to bear for different stakeholders at the various milestones during the implementation of the system. It is important to identify those and work according to strict timelines to satisfy expectations. Submit relevant grant applications, get public and private sector commitments, including industry, whether for technical assistance, logistics, data for testing or infrastructure development commitments. Developing working relationships with relevant academic colleagues and institutions is very important in this context. The most critical resource is enduring political will and strengthening of the information communication technology (ICT) infrastructure needs to be prioritized as part of the national HIS strategy.
Develop a short-term and medium-term plan
Various parallel processes will need to be planned, integrated and implemented during the first few years. Development of national data standards needs to be started very early, based on international standards and involving the colleagues and champions identified so far. Multiple information systems need to interchange data with each other and systems must send and receive data conforming to standard definitions, standard codes and standard field lengths. These are of fundamental importance to data quality and integrity, and should be used by staff of all disciplines, particularly those involved in the collection, processing and analysis of information. This involves the development of a single definitive national inventory of information on health and possibly social care datasets, and incorporates a national data dictionary, information on the existing national datasets and new developments. Such single inventory – called the National Data Catalogue in Scotland [25] – would:
Improve provision of comprehensive metadata on national data through a single point of access.
Eliminate duplication of information.
Enhance support to research on health and social care.
Encourage greater use and awareness of national data standards and definitions to improve the quality of information available to support health and social care services.
The data dictionary is a one-stop shop for health- and social-care data definitions and standards, and should be maintained by a single agency. As new definitions and standards are agreed they will be published on the data dictionary site. The national dataset section contains the full list of datasets held nationally, along with information about the datasets, such as size of dataset, population coverage, overall data quality, as well as publications that use these datasets and other general useful information [25].
These processes need to be driven by established governance structures that are supported by the political leadership to complete them, since it will involve making many changes, including to existing systems. A strategy needs to be developed in terms of the use of personal health information and, as the quality and quantity of this information increases, such information is increasingly used to monitor, evaluate and improve services.
All required changes in law need to be detailed such that personal health information will be safe for all in the future. The technicians need to find test data for developing locally tuned matching algorithms and learning what quasi-identifiers are needed in the country, what the other existing information systems do and whether they work well. Work with healthcare professionals to draw up patient flow charts and where possible improve work flows. Map out how data are captured and used throughout the information system. This information can be used to model how the information technology can facilitate this process and will also show how data should be exchanged between various vertical systems as data objects. Software such as Business Process Model and Notation 2.0 may provide useful tools for this purpose [26]. If matching algorithms are to be used that worked well for smaller number of individual files, they may not necessarily be adequate if they are used for a larger number of files.
A need exists to reduce the number of clinical and patient based administrative systems information systems to a few systems, either by executive order or through some competitive process that objectively assesses existing systems according to agreed functionality and compliance with standards that are able to converge into a standard in a reasonable time. For instance, unique identifiers are being produced and used for programs for key populations in various countries [27]. The greater the number of existing nonstandard systems, the slower the plan should be developed and implemented, and the greater the importance of building consensus. The vision needs to be discussed publicly, including the benefits and risks. Developing consensus is an iterative process. Different applications can theoretically work the same electronic health record data structures, and countries may in some situation maintain the services of the vendors of these different applications. However, this is not possible if multiple incompatible data structures exist in the country.
As the correct engineering and design start to evolve, they will need to be discussed regularly with technical experts, champions, lead users, political leadership and civil society. Developing and implementing the relevant legal framework is likely also to be a multi-year process. An incremental process provides time to pass laws, allows confidentiality and security issues to be considered carefully, and ideas can be tested at small scale. Civil society needs to know that the risks are not zero and understand their parts in keeping their information safe. Many interests will arise from the project and one needs to plan how to build the largest and most durable consensus: who gets the initial contracts, the contingencies for retaining the contracts, who owns the source code or to what extent is it ‘open source’, where pilots are to be performed, which organizations will be involved in the training, and who will be data stewards, if not already defined.
Usually more than one way to solve a problem exists, whether to build software or infrastructure. Learn about different opinions, understand them and persuade key individuals until congruence begins to emerge. Persistence and good will may bring design and engineering consensus on the same or faster time frame as establishing the national information standards, the necessary legal infrastructures and securing resources.
Planning what to do
The design of the NHID and system will need to address the issues raised by the assessment.
Significant design choices will still need to be made. The NHID itself will need to be unique, focused, assignable, accessible, atomic, content-free, usable, concise, linkable, unambiguous, can be verified and validated, retired, retroactive, and public in order to also support paper clinic needs (Figure 4). Use information from the algorithmic testing and the assessments of the enrolment processes of the various extant clinical information systems, to help solidify the minimum quasi-identifiers and biometric selection consensus. Given the existence of Tier 1 clinics, it is likely that in many countries a hybrid system will be needed.
Figure 4.
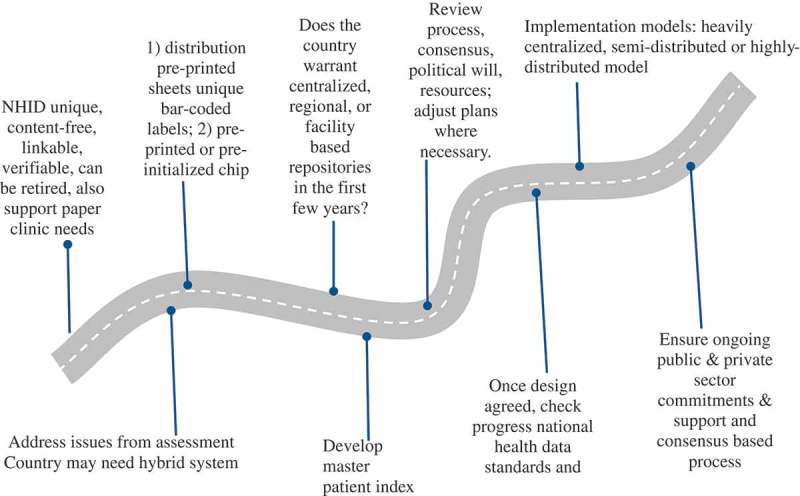
Developing and implementing NHIDs and sections of the NHID system.
Considering the infrastructure in the country, will it be possible to do central assignment or does one need to rely on distributed assignment? Aside from ‘blocking’, two reasonably practical types of central assignment can work without full network coverage. First, the distribution of pre-printed sheets of unique bar-coded labels to paper clinics, for subsequent pasting on the clinic documents, laboratory orders and prescriptions of a patient in paper contexts. The bar-coded identifier can also be used in automated settings, as for instance is done in South Africa and Malawi. This does require keeping supply lines full as the label sheets are used. One needs to pilot it to confirm this is workable with existing logistics. Second, the issuance of pre-printed or pre-initialized chip card identifiers, which can be both used manually in paper clinics and automatic with no manual look-up – in electronic clinics. In either case, the bar-coded identifier will work in both paper and electronic clinics as the public identifier.
In the Western Cape, South Africa, the distribution of pre-printed sheets of unique bar-coded labels to paper clinics works well, but there must be a single source system generating these, the Master Patient Index (MPI). Cheaper alternatives to the more expensive chip cards are available and have been found to work well in more stationary populations, including the use of laminated plastic cards with QR codes or bar codes. However, non-chip solutions exclude the possibility of carrying the digital health record data with the card identifier. The chip card provides an inter-facility continuity of care benefit to the client in Tier-2 non-network environments that competes with Tier-3 infra-structure of care. Giving bar codes on a sticker to a patient to bring to the clinic at the next appointment can also work well for identification and linkages at one clinic, but does not consolidate data for providers or enable inter-facility continuity of care. All of these solutions, however, require electricity to be available in the facility.
Use a system that is designed to be a population-oriented EHR that is proven to be interoperable, can handle large volumes, does not slow down the process and is proven to be robust. Consider whether, based on the size of the country, mobility and telecommunications limitations, the extent that country focuses on developing centralized, regional or facility based repositories in the first few years when the repositories are quite limited for producing aggregate indicator data or are full EHR repositories. Any Tier 1 solution will require physical transport of paper-based data from remote places with monthly update cycles, until power is deployed and the new Tier 2 facility has access to electricity. For such Tier 2 or 3 facilities, one model is to keep some or all data from EHRs in facilities or districts in compressed and encrypted format on a chip card, as has been introduced in Zambia [28]. Information will be accessible to clinicians in facilities for patient care but at the district level, confidential health data are used only for aggregate public health reporting and identifiers used only for record linkage and de-duplication. The size of the country and the percentage of Tier 1 facilities affect the difficulty with quasi-unique identifiers-based de-duplication and matching.
Review previous steps in the process, adjust plans where necessary, and confirm one has kept project consensus. Review resources required now that one can project the cost of the design given the type of technical resources needed. Ensure the availability of adequate funding and other resources based on the existing consensus and political will. Once a design has been agreed on, check that progress has been made on national health information standards and legal updates. If not, work on those areas that have weakened. Check with leadership to see if an executive decision may be forthcoming, including on what to do with incompatible systems.
There are a number of different models for implementing NHIDs, which vary in the number of service points, capacity to scale up and provide national services, complexity and costs. Box 3 describes three models as examples of the many variations that should be considered [20].
Box 3.
Different models for implementing a NHID [20].
Heavily centralized model. This model typically leverages existing government services that occur at one central location, such as the capital city. Characteristics of a heavily centralized model include the following:
|
| If the country has predominantly more Tier 1 facilities instead of Tier 2 or 3, one has to solve the logistic issues of having a printer in the capital serve the label printing needs of all the rural clinics in the country, something that can be insurmountable. A compromise between highly centralized and highly distributed Tier 2 or 3 facilities is to print bar codes on initialized chip cards centrally, thereby assuring their uniqueness, so that the identifier on the chip equals the printed bar-code. Such cards can be centrally produced but locally assigned to clients. |
Semi-distributed model. This model is similar to the heavily centralized model, but it leverages existing government services that typically occur at regional or provincial centres. Characteristics of a semi-distributed model include the following:
|
Highly distributed model. In this model, NHID administration occurs at the point of health service delivery throughout the country. Characteristics of a highly distributed model include the following:
|
How to do it
Training is critical for all staff, and it may also be the most expensive part of the national implementation (Figure 5). If only some staff are trained, this can potentially lead to difficulties that will affect the success of the implementation process. In a country with many disparate and incompatible clinical information systems, the training process may be very protracted. The introduction of such new technology will require the evaluation and potential redesign of workflow in the site. The training provided needs to be done within the context of the amended workflow. The move to using a NHID is likely to require a paradigm shift in many facilities from recoding services in an aggregated fashion to systematically recording each patient encounter.
Figure 5.
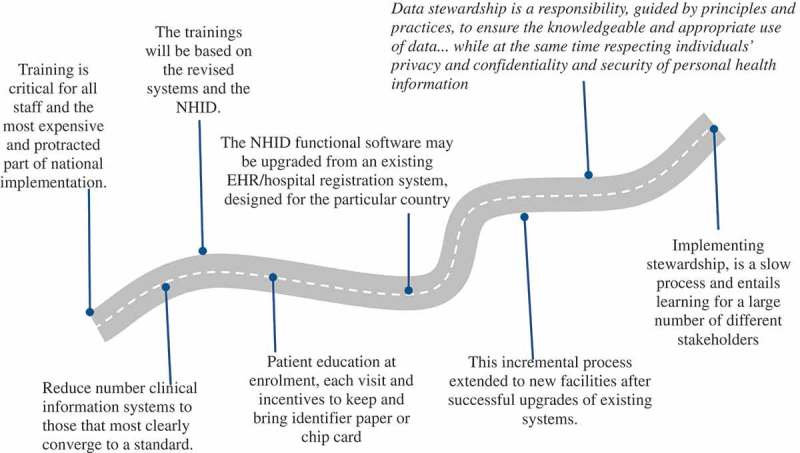
Training requirements, upgrades and data stewardship.
The trainings will be based on the revised systems and the NHID. The country will need to decide whether:
the performance of the clinical system users whose work is what gives the NHID meaning and value, and whose support for the system implementation is essential
the performance of donors and politicians and champions and visionaries keep all focused on the vision for 5 to 10 years
implementation will need to include full staff training, retraining and, for some, certification in searching for patients using unique identifiers and quasi-identifiers. The extent of searching prior to issuance of every new unique identifier needs to be logged and used for quality control. A failure to look and find results in the production of a duplicate record, a discontinuity of patient care, double counting of patients served and a reduction of quality of care indices
apart from training clinic staff, it should also include training of data analysts that can use the information for service improvement.
Patient education needs to be performed at enrolment, reinforcement at each visit, and incentives provided to ensure that they bring and keep the identifier that is used either a barcode or identifier chip card. Although not essential, and more expensive than the barcode, an identifier chip card can also function as storage of limited medical data, an additional benefit (Box 4).
Box 4.
Potential benefits of identifier chip cards.
|
A few countries have put their full primary care EHR on the chip card in lieu of moving from Tier 2 to Tier 3 facilities. This provides a very robust continuity of care model that works when internet or facility information retrieval fails, since the patient has an copy of his/her EHR.
Disincentives, if client forgets their identifier token or smart card, could include:
need to queue for process of full re-enrolment prior to clinic visit, if a search fails;
if a card is lost twice, may need to pay a nominal replacement fee thereafter.
Training in the use of identifier documents at enrolment is a necessity. Photographs or fingerprints can be used and it is necessary to train staff how to take photo and fingerprint biometrics. Fingerprinting may deter drug seeking, and reduce duplicate identifiers’ issuance but taking photographs is easier and less expensive. If neither options are available, the software should allow for robust matching algorithms, or just scan a barcode.
Deployment. The NHID functional software deployment may be an upgrade from an existing EHR or hospital registration system, which previously used different identifiers and now uses the NHID designed for the particular country. Software needs to be considered that is purpose-built for, being a population-based EHR with MPI functionality, ensuring that all the speed, interoperability, and patient search and match criteria are met. Deployment should be an incremental process. Only after upgrades of existing systems to use the new NHID have been performed are proceeding well, with the support of available resources, and the upgrade deployment has been successful, would it be a good time to consider moving the NHID and EHR system into new facilities. This process depends on the systems being addressed; in some cases merging records from existing systems could be a very feasible option and will assign new NHID to old records whilst linking the old identifier to the new NHID. This allows old identifiers to be phased out and should also be criteria for the MPI. The process of a new site deployment includes some work that may have been done during assessment, but may need to be revisited:
Reassess the physical environment – is there a secure room for locking up the system computer(s)? What is the reliability of the power, is there an UPS, generator set, or solar fail-over option for power? Are there any telecommunications?
Reassess logistics – does the site have transport? What is the distance to nearest site with the system?
Reassess the adequacy of the staff for the new technology: is the facility understaffed? Do staff rotate through other facilities that are or will be using the system? Have they used a computer before? How long has it been since the staff were trained and do they need to be retrained?
Follow up – institutionalizing and evolution
Data stewardship is a responsibility that is guided by principles and practices, to ensure the knowledgeable and appropriate use of data. More specifically, stewardship of health data recognizes the benefits to society of using personal health information to improve understanding of health and healthcare, while at the same time respecting individuals’ privacy and confidentiality [29].
Implementing stewardship is a progressive process over time and entails learning for a large number of different stakeholders. It has visible and concrete manifestations, including laws that spell out the protections accorded to personally identifiable information, and the proper uses that can be made of it. It also has invisible and subtle manifestations, such as reducing stigma and discrimination.
A national data repository is a national public good and, if correctly set-up and protected, is a benefit based on the process of aggregating individual health histories. The personal health information that this is based on will need protection through privacy policies that are implemented, and protect the confidentiality and security of that information. Country guidance on protecting personal health information has been developed [9] which countries can adapt, adopt and implement to suit local conditions. Furthermore, an Assessment Tool, Manual and Workbook to assess the existence and implementation of national guidance to protect personal health information have been developed for health facilities, data warehouses and repositories, and national levels [30–32].
Local computers, networks and data repositories have become major targets for political and criminal activities. Recent political activities involved the hacking of the 2016 US and 2017 French elections [33,34] and the 2016 UK Referendum on membership of the European Union [35]. The 2013 hacking of Yahoo [36], the 2016 leaking of information from the Chinese National Center for AIDS/STD Control and Prevention [37] and the mayhem caused by the ransomware cyber-attacks of May and June 2017 [38,39] are just some examples of criminally inspired cyber-attacks. The Wannacry attack of May 2017 affected many organizations across the world, including the UK National Health Service [38]. One expert was quoted that ‘a “massive” increase in spending is needed to prevent another “avoidable” cyber-attack on NHS computer systems’ [40]. While these occurrences should not deter the development and implementation of digital systems, it does reiterate the fact that notions of the confidentiality and security of personal health information need to be taken more seriously than they have been to date in many parts of the world.
The implementation of the stewardship of local and national data repository includes the incremental development and implementation of regulations as the execution of the stewardship proves itself technically and administratively capable and sufficiently autonomous. Relevant laws or regulations need to stipulate the formulation and independence of data repositories with relevant stewardship, and over time it will be apparent if they can protect it from misuse or abuse. Implementing the actual physical stewardship of valuable data is a highly technical endeavour [9], but when properly performed the benefits will outweigh the costs and risks. One needs to evaluate one’s technical capacity to first maintain security, and, second, to determine and maintain appropriate access.
Start slowly but initially focus on security. Once achieved, one can then make transparent accommodations of requests for information with ethics boards approval and consented studies. Via an open process, the ‘public use data’ can be defined to get the information used for the common good. Over time the number of users and the types or sensitivity of data released may increase, in a transparent manner, while monitoring outcomes and being sensitive to the level of public concern. Denmark is an example of a country that that has made a lot of progress in this area [41].
However, implementation and ensuring the confidentiality and security of personal information remains an ongoing issue, as was recently demonstrated in the problems faced by Sweden. Sweden experienced an ‘extremely serious’ security breach, ‘which followed a 2015 data outsourcing contract between the national transport agency and IBM Sweden’ in which security clearance requirements for foreign information technology workers were waived when signing the agreement, in breach of privacy and data protection laws” [42]. Swedish media reported that besides the ‘entire national driver’s license database, the records potentially included information on intelligence agents, military and police transport and personnel, people with criminal records and those in witness protection programs’ [42]. This event highlights the even greater need for protecting personal information, if personal health information can be tracked across different social sectors.
Institutionalization: institutionalizing these processes should begin at the earliest stages of the assessment process. Some reflect the understanding of national values as developed during the consensus meetings and reassessments. Others reflect a maturing of society’s understanding of shared benefits and associated risks and the need for tolerating differences to achieve the largest population benefits. The points described in Box 5 provide indications of public and political will, and manifestations at systems’ level.
Box 5.
Understanding of shared benefits, risks and actions.
Reflections of public and political will
|
Manifestations at the level of the system
|
For this process to be successful, it needs to have a long-term perspective, as long as personal health information needs to be in the public domain in order to improve public health, by harnessing the synergies of the different information streams based on the life-long health experiences of each person in the country.
Implementation is more of a political process than an engineering one and as such this process is never completed as technologies and political ideologies may change. Much of its success hinges on human will and performance:
the performance that the patient carries his/her card and trusts the system
the performance of the system registration staff who educate and reinforce the client
the potentially life-saving tasks of preventing duplicate and overlaid health records, preventing misidentification that remains a leading cause of death [43]
the performance of the many types of ICT and informatics staff who provide ongoing back-up maintenance and continuously upgrade the system security, retune the MPI algorithms as the database grows and changes, and continually assess risks
the maintenance of all the elements by the staff of a secure national system, serving millions of users in a manner that maintains their trust
that staff develop and maintain expertise in many types of hardware and equipment, devise and implement automated feedback control systems for every vital element of the national systems operation.
An example of how a national health system has become institutionalized can be seen in the UK. The UK NHS was established in 1948 and was based on a pre- and post-World War II political consensus that every UK citizen should have access to healthcare irrespective of who they are and where they are, and that was free at point of service provision [44]; public discussion about the need to develop an NHS goes back to the early 1900s. This taxation-based system has proved to be very popular and, despite many technological changes, changes in expectations of users of services and political ideologies since its foundation, every government has declared its intention to maintain and improve the NHS. Recent polls among UK citizens indicate that ‘There is strong support for the principles of the NHS across all sections of British society. Of those surveyed, 89% agree that the government should support a national health system that is tax funded, free at the point of use and provides comprehensive care for all citizens’ [45]. Nevertheless, the NHS has faced recurrent problems, there have been endless reorganizations, paying tribute to the notion that systems like the NHS will continue to evolve, as technologies and expectations by users and providers of services evolve and result in changing societal attitudes.
Conclusion
The development of individual longitudinal linked medical records across health services and the use of de-identified personal health information to monitor, evaluate and improve services on a continuous basis are going to be greatly aided by the development of NHIDs. For this process to be optimally successful it needs to be a progressive multi-stakeholder process that involves identifying champions to ‘carry the torch’ and highlight evidence of improvement during this medium- to long-term process. These ‘champions’ need to be representatives from different communities that have a stake in ensuring this process is not only technically successful but that it conforms to and is in line with accepted human right principles [46]. Champions should include members of the technical community, healthcare professionals, representatives from patient organizations and other relevant civil society organizations, academics, private investors and politicians from across the political spectrum. The focus should not only be on technical issues but provide ongoing evidence of improving service delivery through the use of this information. The technical aspects for the development and implementation of a NHID system are less of an issue compared with the social, economic and cultural aspects of these processes. It is these factors that will ultimately determine whether the process is successful or not.
Responsible Editor Peter Byass, Umeå University, Sweden
Funding Statement
Workshop and publication funded by the HIV Department, WHO, Geneva.
Acknowledgments
In addition to the participants of the WHO/UNAIDS July 2017 workshop, we are grateful to those who assisted in making the workshop happen, and Peter Ricketts, Health Information Unit, Commonwealth of Dominica, and Marcelo D’Agostino, Knowledge Management Health Information and Analysis, PAHO, who commented on drafts of this paper. We are also grateful for the comments made by the reviewers. This paper reflects the views of the authors and not necessarily UNAIDS.
Disclosure statement
No potential conflict of interest was reported by the authors.
Ethics and consent
Not applicable.
Paper context
Linking data from different sources enables longitudinal individual health records to be constructed and de-identified personal health information (PHI) can be used for monitoring and evaluating health services. National health identifiers (NHIDs) enable such linkages and this paper provides practical guidance for developing and implementing NHIDs. Success of this process is ultimately dependent on social, political and economic factor rather than technical ones, and protecting the confidentiality and security of PHI.
References
- [1]. Bradley H, Hall HI, Wolitski RJ, et al. Vital Signs: HIV diagnosis, care, and treatment among persons living with HIV United States, 2011. MMWR Morb Mortal Wkly Rep. 2014;63:11137 Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6347a5.htm [PMC free article] [PubMed] [Google Scholar]
- [2]. UNAIDS 90-90-90an ambitious treatment target to help end the HIV epidemic. Geneva (Switzerland): UNAIDS; 2014. Available from: http://www.unaids.org/en/resources/documents/2017/90-90-90 [Google Scholar]
- [3]. Hargreaves JR, Delany-Moretlwe S, Hallett TB, et al. The HIV prevention cascade: integrating theories of epidemiological, behavioural, and social science into program design and monitoring. Lancet HIV. 2016;3:e318–15. Available from: http://www.thelancet.com/pdfs/journals/lanhiv/PIIS2352-3018(16)30063-7.pdf [DOI] [PubMed] [Google Scholar]
- [4]. Rishera K, Mayer KH, Beyrer C.. HIV treatment cascade in MSM, people who inject drugs, and sex workers. Curr Opin HIV AIDS. 2015. November;10:420–429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5]. Yehia BR, Schranz AJ, Umscheid CA, et al. The treatment cascade for chronic hepatitis c virus infection in the United States: a systematic review and meta-analysis. PLoS One. 2014;9:e101554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6]. Longenecker CT, Aliku T, Beaton A, et al. Treatment cascade quality metrics for children with latent rheumatic heart disease in Uganda. Glob Heart. 2016;11:119–e120. Available from: http://www.sciencedirect.com/science/article/pii/S221181601630415X [Google Scholar]
- [7]. Medland NA, McMahon JH, Chow EPF, et al. The HIV care cascade: a systematic review of data sources, methodology and comparability. J Int AIDS Soc. 2015;18:20634 Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4666907/pdf/JIAS-18-20634.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8]. WHO Consolidated guidelines on person-centred HIV patient monitoring and case surveillance Guidelines. Geneva (Switzerland); 2017. Available from: http://apps.who.int/iris/bitstream/10665/255702/1/9789241512633-eng.pdf?ua=1 [Google Scholar]
- [9]. Beck EJ, Gill W, De Lay PR. Protecting the confidentiality and security of personal health information in low- and middle- income countries in the era of the SDGs and big-data: extended bibliography. Global Health Action. 2016. Available from: http://www.tandfonline.com/doi/pdf/10.3402/gha.v9.32089?needAccess=true [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10]. Marcus JL, Chao CR, Leyden WA, et al. Narrowing the gap in life expectancy between HIV-infected and HIV-uninfected individuals with access to care. J Acquir Immune Defic Syndr. 2016;73:39–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11]. WHO Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. Geneva (Switzerland); 2015. Available from: http://apps.who.int/iris/bitstream/10665/186275/1/9789241509565_eng.pdf?ua=1 [PubMed] [Google Scholar]
- [12]. Mahy M, Autenrieth C, Stanecki K, et al. Increasing trend in HIV prevalence among people aged 50 years and older: evidence from estimates and survey data. Aids. 2014;28:S453–S459. Available from: file:///C:/Users/User/Downloads/Increasing_trends_in_HIV_prevalence_among_people.6.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13]. Althoff KN, Smit M, Reissc P, et al. HIV and ageing: improving quantity and quality of life. Curr Opin HIV AIDS. 2016;11:527–536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14]. Hyle EP, Naidoo K, Su AE, et al. HIV, tuberculosis, and non-communicable diseases: what is known about the costs, effects, and cost-effectiveness of integrated care? J Acquir Immune Defic Syndr. 2014;67:S87–S95. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4147396/pdf/nihms604877.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15]. WHO Non-Communicable Diseases: the slow motion disaster. Ten Years in Public Health 2007–2017. Geneva (Switzerland); 2017. Available from: http://www.who.int/publications/10-year-review/ncd/en/ [Google Scholar]
- [16]. WHO/International Bank for Reconstruction and Development/The World Bank Tracking universal health coverage: 2017 global monitoring report; 2017. Available from: http://pubdocs.worldbank.org/en/193371513169798347/2017-global-monitoring-report.pdf
- [17]. Chung NC, Bolton-Moore C, Chilengi R, et al. Patient engagement in HIV care and treatment in Zambia, 2004-2014. Trop Med Int Health. 2017. Available from: http://onlinelibrary.wiley.com/wol1/doi/10.1111/tmi.12832/full [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18]. AMPATH Leading with care. Eldoret (Kenya) Available from: http://www.ampathkenya.org/ [Google Scholar]
- [19]. Pedersen CB, Gøtzsche H, Møller JØ, et al. The Danish civil registration system: a cohort of eight million persons. Dan Med Bull. 2006;53:441–449. [PubMed] [Google Scholar]
- [20]). UNAIDS/PEPFAR Considerations and Guidance for Countries Adopting National Health Identifiers. Geneva (Switzerland); 2014. Available from: http://www.unaids.org/en/resources/documents/2014/national_health_identifiers [Google Scholar]
- [21]. Kitenge G, Govender I. Nurses’ monitoring of the Road to Health Chart at primary healthcare level in Makhado, Limpopo province. South Afr Fam Pract. 2013;55:275–280. [Google Scholar]
- [22]. Neville R, Neville J. What can health care professionals in the United Kingdom learn from Malawi? Hum Resour Health. 2009;7:26 DOI: 10.1186/1478-4491-7-26 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23]. WHO Health statistics and information systems. Geneva (Switzerland) Available from: http://www.who.int/healthinfo/country_monitoring_evaluation/documentation/en/ [Google Scholar]
- [24]. WHO HMN country files. Geneva (Switzerland); 2016. Available from: https://www.dropbox.com/s/agme52z13pto136/countries.zip?dl=0 [Google Scholar]
- [25]). ISD Scotland Home National Data Catalogue Information Services Division. NHS National Services Scotland; 2018. Available from: http://www.ndc.scot.nhs.uk/ [Google Scholar]
- [26]. Object Management Group Documents associated with Business Process Model And Notation™ (BPMN™) Version 2.0; [cited January 2011]. Available from: http://www.omg.org/spec/BPMN/2.0/
- [27]. Castellan C, Lungo S, Oliva K, et al. Use of a Unique identifier system to track key populations reached under a combination prevention program in six countries in South America. Pan American Social Marketing Organization, AIDS, 2014, Melbourne Australia, WEPE458; 2014. Available from: http://www.psi.org/wp-content/uploads/2014/10/Use-of-unique-identifier-code-key-populations-prevention-Central-America.pdf
- [28]. Muyunda G. Zambia leads the way in smartcare electronic health records system, a benefit to both providers and patients. JHPIEGO [cited 2011. August 23] Available from: https://www.jhpiego.org/success-story/zambia-leads-the-way-in-smartcare-electronic-health-records-system-a-benefit-to-both-providers-and-patients/
- [29]. Health Information Privacy Guidance regarding methods for de-identification of protected health information in accordance with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule 2016. HHS Gov; 2016. Available from: https://www.hhs.gov/hipaa/for-professionals/privacy/special-topics/de-identification/index.html
- [30]. UNAIDS/PEPFAR The Privacy, Confidentiality and Security Assessment Tool: protecting personal health information. Geneva (Switzerland); 2016. Available from: http://www.unaids.org/en/resources/documents/2016/confidentiality_security_assessment_tool [Google Scholar]
- [31]. UNAIDS/PEPFAR The Privacy, Confidentiality and Security Assessment Tool: user manual. Geneva (Switzerland); 2016. Available from: http://www.unaids.org/en/resources/documents/2016/confidentiality_security_tool_user_manual [Google Scholar]
- [32]. UNAIDS/PEPFAR The Privacy, Confidentiality and Security Assessment Tool: workbook. Panama City (Panama); 2016. Available from: http://onusidalac.org/1/images/2016/workbook.pdf [Google Scholar]
- [33]. Wikipedia Russian interference in the 2016 United States elections. Available from: https://en.wikipedia.org/wiki/Russian_interference_in_the_2016_United_States_elections
- [34]. The Guardian Macron hackers linked to Russian-affiliated group behind US attack. [cited 2017. May 8] Available from: https://www.theguardian.com/world/2017/may/08/macron-hackers-linked-to-russian-affiliated-group-behind-us-attack
- [35]. Cadwalladr C. The great British Brexit robbery: how our democracy was hijacked. The Observer; [cited 2017. May 8] Available from: https://www.theguardian.com/technology/2017/may/07/the-great-british-brexit-robbery-hijacked-democracy
- [36]. Thielman S. Yahoo hack: 1bn accounts compromised by biggest data breach in history. The Guardian; [cited 2016. December 15] Available from: https://www.theguardian.com/technology/2016/dec/14/yahoo-hack-security-of-one-billion-accounts-breached
- [37]. Kan K. China investigating data leak and swindling of H.I.V. patients. New York Times; [cited 2016. July 21] Available from: https://www.nytimes.com/2016/07/22/world/asia/china-hiv-aids-leak.html
- [38]. BBC Massive ransomware infection hits computers in 99 countries; [cited 2017. May 13] Available from: http://www.bbc.com/news/technology-39901382
- [39]. BBC Global ransomware attack causes turmoil; [cited 2017. June 27] Available from: http://www.bbc.com/news/technology-40416611
- [40]. BBC Call for investment in NHS cybersecurity; [cited 2017. June 20] Available from: http://www.bbc.com/news/uk-scotland-scotland-politics-40341339
- [41]. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014. August;29:541–549. Available from: https://link.springer.com/article/10.1007/s10654-014-9930-3 [DOI] [PubMed] [Google Scholar]
- [42]. Henley J. Sweden scrambles to tighten data security as scandal claims two ministers. Guardian; [cited 2017. August 1] Available from: https://www.theguardian.com/technology/2017/aug/01/sweden-scrambles-to-tighten-data-security-as-scandal-claims-two-ministers?CMP=Share_AndroidApp_Gmail
- [43]. Just BH, Marc D, Munns M, et al. Why patient matching is a challenge: research on Master Patient Index (MPI) data discrepancies in key identifying fields. Perspectives in Health Information Management Spring 12016. Available from: http://perspectives.ahima.org/why-patient-matching-is-a-challenge-research-on-master-patient-index-mpi-data-discrepancies-in-key-identifying-fields/ [PMC free article] [PubMed]
- [44]. Webster C. The National Health Service: A Political History (OPUS). Oxford, UK: Oxford University Press; 1998. [Google Scholar]
- [45]. Gershlick B, Charlesworth A, Taylor E. Public attitudes to the NHS: an analysis of responses to questions in the British Social Attitudes Survey. NatCen Social Research, The Health Foundation; 2015. Available from: http://www.health.org.uk/publication/public-attitudes-nhs [Google Scholar]
- [46]. United Nations Educational, Scientific and Cultural Organization Universal Declaration on Bioethics and Human Rights. Adopted by acclamation on 19 October 2005 by the 33rd session of the General Conference of UNESCO Available from: http://portal.unesco.org/en/ev.php-URL_ID=31058&URL_DO=DO_PRINTPAGE&URL_SECTION=201.html [Google Scholar]