

Abstract
Nowadays, Klebsiella oxytoca is described as a causative organism for antibiotic-associated hemorrhagic colitis (AAHC). Here we report two cases of pediatric AAHC, from which K. oxytoca was cultured after starting amoxicillin-clavulanate or amoxicillin treatment. The patients developed severe abdominal pain and a large amount of bloody diarrhea. K. oxytoca was obtained in intestinal fluid culture of a boy through the colonoscopy. On the other hand, colonic tissue culture and intestinal fluid culture were negative of the other patient. K. oxytoca was detected in stool culture when he was admitted. These cases showed characteristic endoscopic findings of segmental hemorrhagic colitis, and both boys recovered spontaneously within 2–3 days after they stopped taking the antibiotics. Therefore, in children who develop relatively large amount of bloody diarrhea after antibiotic treatment, we should consider AAHC caused by K. oxytoca.
Keywords: Antibiotic-associated diarrhea, Klebsiella oxytoca, Bloody diarrhea
INTRODUCTION
Acute diarrhea associated with antibiotics can be represented by a variety of mechanisms. The most common type is pseudomembranous colitis. It is caused by overgrowth of toxin-producing Clostridium difficile [1]. Recently, antibiotic-associated hemorrhagic colitis (AAHC) caused by Klebsiella oxytoca has received great attention. Patients with AAHC usually have considerable bloody diarrhea. Therefore, this condition is likely to be misdiagnosed as lower gastrointestinal bleeding or chronic bowel disease.
AAHC was first described by Toffler et al. [2], and it is usually observed during therapy with amoxicillin-clavulanate, amoxicillin, penicillins, or ampicillin [2,3]. Patients with AAHC usually present with abdominal pain, or relatively large amount of bloody diarrhea due to right-sided colitis [4,5,6,7,8]. These symptoms typically begin 2 to 7 days after starting the antibiotic treatment but the patients recover quickly within 3 days of stopping the causative antibiotic [3]. K. oxytoca was cultured in a stool sample, colonic tissue, and/or intestinal fluid. Here we report two cases of pediatric AAHC, from which K. oxytoca was cultured after starting amoxicillin-clavulanate or amoxicillin treatment.
CASE REPORT
Case 1
A 13-year-old boy was admitted to the emergency room (ER) with acute, severe abdominal pain, nausea, vomiting, and 6 to 7 times fresh bloody diarrhea in two hours. The water in the toilet was turbid with bright red color due to relatively large amount of bloody diarrhea. Before admission, he had been taking amoxicillin-clavulanate and nonsteroidal anti-inflammatory drugs for three days due to acute otitis media, which were prescribed at a local clinic. Vital signs were within normal limits for his age. Physical examination revealed abdominal tenderness in the periumbilical area. Laboratory tests revealed the following finding: white blood cells (WBCs), 17,300/µL (neutrophils, 79%; lymphocytes, 13%; monocytes, 7%); hemoglobin, 14.8 g/dL; platelets, 288,000/µL; and C-reactive protein (CRP), 0.34 g/dL. Other laboratory findings, including a battery of chemistry tests, prothrombin time and activated partial thromboplastin time, were within the normal range.
Abdominal computed tomography (CT) showed colitis with edematous wall thickening from the ascending colon to the splenic flexure of the colon (Fig. 1). Esophagogastroduodenoscopy revealed minimal reflux esophagitis, and bile reflux gastritis. A colonoscopy revealed severe mucosal hemorrhge, erythema, and granular erosions with edema from the ascending colon to the transverse colon. Particularly in the hepatic flexure area, with the most severe erythema and friable mucosa with granular erosions and exudates were observed (Fig. 2). Pathologic findings were compatible with acute hemorrhagic colitis and they showed fibrinoid change of the destroyed red blood cells on the superficial mucosa without distortion of the gland or cryptitis (Fig. 3). Stool polymerase chain reaction (PCR) tests for Vibrio, Campylobacter, Salmonella, Shigella, Yersinia, Escherichia coli 0157: H7, astrovirus, group A rotavirus, enteric adenovirus and norovirus were negative. K. oxytoca was cultured on the intestinal fluid culture test during the colonoscopy, and it showed resistance to amoxicillin-clavulanate, ampicillin, aztreonam, cefazolin, and piperacillin-tazobactam.
Fig. 1. An abdominal computed tomography scan image revealed colitis involving from the ascending colon to the splenic flexure of the colon with the edematous bowel wall thickening (Case 1). A: ascending colon, D: desending colon, T: transverse colon.

Fig. 2. A colonoscopy revealed red mucosa and granular erosions with edema from the proximal colon (A) to the distal colon (B). In the hepatic flexure area was the most severe erythema and hemorrhage, friable mucosa and granular erosions with exudate (Case 1): a colonoscopy showed severe redness and hemorrhage in the proximal colon (C) to the distal colon (D) (Case 2).

Fig. 3. Photomicrographs of the H&E stained biopsy specimens from the colon of the patient 1 showing: (A) hyalinized lamina propria with hemorrhage and neutrophilic infiltration, reactive epithelial atypia, and cryptitis (H&E, ×200). (B) Neutrophilic cryptitis with mitosis and reactive atypia in the background of preserved crypt architecture (H&E, ×400).

Finally, he was diagnosed with AAHC caused by K. oxytoca. Administration of amoxicillin-clavulanate was discontinued after admission, and bloody diarrhea and abdominal pain rapidly improved by the third day. He was empirically treated with intravenous (IV) cefotaxime for 7 days before the diagnosis was confirmed. Ten days after discharge, he was in a good condition and did not have bloody diarrhea or abdominal pain.
Case 2
A 15-year-old boy was admitted to the ER with complaints of severe abdominal pain and bloody diarrhea occurring more than ten times in a single day. The amount of bloody diarrhea was about 100 g at a time. Before admission, he had been taking amoxicillin and probiotics. On admission, his vital signs were stable. Physical examination revealed mild tenderness in the periumbilical area. Laboratory test findings on admission were as follows: WBCs, 7,860/µL (neutrophils, 79%; lymphocytes, 14%; monocytes, 6%); hemoglobin, 16.6 g/dL; platelets, 288,000/µL; and CRP, 0.92 mg/dL. Other laboratory findings, including a battery of blood chemistry and coagulation tests, were within the normal range.
Abdominal CT showed pancolitis with edematous wall thickening and pericolic infiltration (Fig. 4). A colonoscopy was performed on the second day of hospitalization and showed severe redness and hemorrhage in the cecum and the ascending colon (Fig. 2). Pathological analysis of colonoscopic biopsies showed no signs of chronic inflammatory disease, but it showed focal active colitis with hemorrhage and ischemia in the cecum and ascending colon (Fig. 5). Cultures of colonic tissue and intestinal fluid were negative. Stool PCR tests for bacteria and virus were also negative. However, K. oxytoca was detected in stool culture at admission. It has susceptible to almost all antibiotics that are currently available, except ampicillin and cefazolin.
Fig. 4. Abdominal computed tomography showed pancolitis with edematous wall thickening and pericolic infiltration. A: ascending colon, D: desending colon, T: transverse colon.
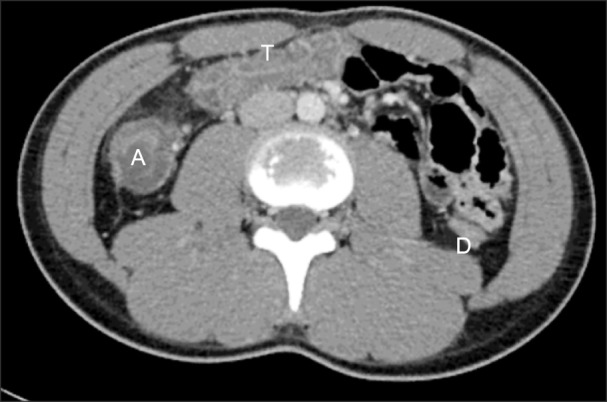
Fig. 5. H&E stained biopsy specimens from the ascending colon of the patient 2 showing: (A) hyalinized lamina propria with hemorrhage and neutrophilic infiltration (H&E, ×200). (B) Neutrophilic cryptitis with crypt abscess and eosinophilic infiltration (H&E, ×400).

After admission, we stopped the administration of amoxicillin. Bloody diarrhea and abdominal pain improved rapidly by the second day. K. oxytoca was not detected in the follow-up stool culture on the third day of hospitalization. He was discharged after 4 days of conservative treatment, and there were no further symptoms after discharge. Follow-up abdominal ultrasonography (USG) performed 3 months after discharge showed a normalized bowel wall thickening.
DISCUSSION
Acute diarrhea is a common adverse effect observed during or shortly after antibiotic therapy [9]. There are studies on AAHC without C. difficile, a special form of antibiotic-associated colitis (AAC). K. oxytoca was found to be a causative factor in these studies [1,5]. Clinical features of AAHC are different from those of AAC. Hemorrhagic diarrhea caused by K. oxytoca was mainly observed in young and out-patients after brief treatment with antibiotics such as amoxicillin-clavulanate, amoxicillin, penicillins, and ampicillin. But, diarrhea associated with C. difficile occurred mainly in older, hospitalized patients.
AAHC can be diagnosed based on a clinical history of taking antibiotics and endoscopic findings of segmental hemorrhagic colitis. AAHC is characterized by a sudden onset of bloody diarrhea after 2 to 7 days of treatment with oral antibiotics such as amoxicillin-clavulanate, amoxicillin, penicillins, and ampicillin [5,7]. It also presents as right-sided hemorrhagic colitis on colonoscopy and is accompanied by abdominal cramps [4,5,6,7,8,9].
In most cases, AAHC-related abdominal pain and endoscopic lesions resolve spontaneously within 2 to 3 days after discontinuing the causative antibiotic [3,5]. It is a self-limiting disease and is resolved by IV hydration alone without any special treatment. Colonoscopic findings of patients with AAHC include segmental colitis such as mucosal edema and mucosal hemorrhage with erosion or longitudinal ulceration. Histologic findings include mucosal inflammation, mainly with infiltration of the lamina propria by neutrophils, and epithelial damage [3,7]. However, the most important point is to identify K. oxytoca in the sample of bloody diarrheal stool, which occurs suddenly during antibiotic treatment [3,4,5,6,7,8,9].
The mechanisms by which K. oxytoca induces colitis have recently been identified. So far, K. oxytoca strains that produce cytotoxin called tilivalline were identified as the causative agents of AAHC [7]. The cytotoxic effect can be assessed by microscopy and is based on cell rounding and cell death. Therefore, besides endoscopy, microbiological tests are important for differential diagnoses of AAHC related to K. oxytoca [9]. Another mechanism has been proposed for mucosal allergic reaction, mucosal ischemia, and infection caused by K. oxytoca [2,4,5,6].
To date, there are several studies of AAHC caused by K. oxytoca in adults, but this condition is rare in children. Usually, when a child develops bloody diarrhea we initially suspect gastroenteritis caused by bacteria such as the most common Salmonella, Shigella, Campylobacter, or Enterobacter. If the child has a history of taking antibiotics, we suspect psedomembranous colitis caused by C. difficile. However, when a child presents with a large amount of bloody diarrhea, we should suspect bacterial enteritis as well as the other causes [10]. Therefore, it is necessary to perform imaging examinations such as abdominal CT, abdominal USG, etc. [2], and we should also suspect AAHC caused by K. oxytoca.
In Case 1, the patient who was taking amoxicillin- clavulanate was admitted with severe abdominal pain and 6 to 7 times fresh bloody diarrhea in two hours and was examined via abdominal CT scan and colonoscopy. K. oxytoca was identified in the intestinal fluid culture during colonoscopy. The stool and colonic tissue culture were negative. At that time, only routine stool cultures were performed, and we did not seek confirmation of K. oxytoca infection. In Case 2, the patient who was admitted with complaints of bloody diarrhea occurring more than ten times of about 100 g at a time. In Case 2, intestinal fluid and tissue cultures were normal. But we had previous experience which K. oxytoca was cultured in intestinal fluid of Case 1 with similar symptoms. So we were able to detect K. oxytoca in stool culture on special request. Both cases were admitted with a large amount of bloody diarrhea, but they did not show hypotension or anemia. This is thought to be due to relatively short duration of bloody diarrhea until admission or to rapidly improved of symptoms after discontinuing the causative antibiotic. It is also conceivable that dehydration due to persistent diarrhea may have resulted in higher hemoglobin levels than the actual values. Recent studies have reported that biopsy specimens and intestinal fluid during colonoscopy in patients with acute diarrhea are important in addition to stool culture [11]. Therefore, stool cultures, biopsy specimens, and colonic fluid culture should be performed during a colonoscopy to identify K. oxytoca.
Currently, K. oxytoca is not included in the routine stool culture analysis [10]. Amoxicillin-clavulanate, amoxicillin, penicillins, and ampicillin, which are the causes of AAHC, are most commonly used in the treatment of a variety of childhood infectious diseases. Therefore, if a child has a large amount of bloody diarrhea, we should enquire about a history of use of these antibiotics. Recent study shows that South Korea has a relatively high rate of antibiotic use [12]. Therefore, considering the high rate of antibiotic use in South Korea, we should try to identify K. oxytoca infection in stool samples or colonic tissue and intestinal fluid cultures on special request. We also hope that a test to identify the cytotoxin produced by K. oxytoca will be performed in the future.
References
- 1.Bartlett JG. Clinical practice. Antibiotic-associated diarrhea. N Engl J Med. 2002;346:334–339. doi: 10.1056/NEJMcp011603. [DOI] [PubMed] [Google Scholar]
- 2.Toffler RB, Pingoud EG, Burrell MI. Acute colitis related to penicillin and penicillin derivatives. Lancet. 1978;2:707–709. doi: 10.1016/s0140-6736(78)92704-6. [DOI] [PubMed] [Google Scholar]
- 3.Hoffmann KM, Deutschmann A, Weitzer C, Joainig M, Zechner E, Högenauer C, et al. Antibiotic-associated hemorrhagic colitis caused by cytotoxin-producing Klebsiella oxytoca. Pediatrics. 2010;125:e960–e963. doi: 10.1542/peds.2009-1751. [DOI] [PubMed] [Google Scholar]
- 4.Sakurai Y, Tsuchiya H, Ikegami F, Funatomi T, Takasu S, Uchikoshi T. Acute right-sided hemorrhagic colitis associated with oral administration of ampicillin. Dig Dis Sci. 1979;24:910–915. doi: 10.1007/BF01311944. [DOI] [PubMed] [Google Scholar]
- 5.Beaugerie L, Metz M, Barbut F, Bellaiche G, Bouhnik Y, Raskine L, et al. Klebsiella oxytoca as an agent of antibiotic-associated hemorrhagic colitis. Clin Gastroenterol Hepatol. 2003;1:370–376. doi: 10.1053/s1542-3565(03)00183-6. [DOI] [PubMed] [Google Scholar]
- 6.Yonei Y, Yoshizaki Y, Tsukada N, Inagaki Y, Miyamoto K, Suzuki O, et al. Microvascular disturbances in the colonic mucosa in antibiotic-associated haemorrhagic colitis: involvement of platelet aggregation. J Gastroenterol Hepatol. 1996;11:681–685. doi: 10.1111/j.1440-1746.1996.tb00314.x. [DOI] [PubMed] [Google Scholar]
- 7.Högenauer C, Langner C, Beubler E, Lippe IT, Schicho R, Gorkiewicz G, et al. Klebsiella oxytoca as a causative organism of antibiotic-associated hemorrhagic colitis. N Engl J Med. 2006;355:2418–2426. doi: 10.1056/NEJMoa054765. [DOI] [PubMed] [Google Scholar]
- 8.Dietrich CF, Lembcke B, Seifert H, Caspary WF, Wehrmann T. Ultrasound diagnosis of penicillin-induced segmental hemorrhagic colitis. Dtsch Med Wochenschr. 2000;125:755–760. doi: 10.1055/s-2007-1024491. [DOI] [PubMed] [Google Scholar]
- 9.Högenauer C, Hinterleitner T. Klebsiella oxytoca as a cause of antibiotic-associated colitis. Washington, DC: ASM Press; 2008. pp. 293–311. [Google Scholar]
- 10.Murphy MS. Management of bloody diarrhoea in children in primary care. BMJ. 2008;336:1010–1015. doi: 10.1136/bmj.39542.440417.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bellaïche G, Le Pennec MP, Choudat L, Ley G, Slama JL. Value of rectosigmoidoscopy with bacteriological culture of colonic biopsies in the diagnosis of post-antibiotic hemorrhagic colitis related to Klebsiella oxytoca. Gastroenterol Clin Biol. 1997;21:764–767. [PubMed] [Google Scholar]
- 12.Youngster I, Avorn J, Belleudi V, Cantarutti A, Díez-Domingo J, Kirchmayer U, et al. Antibiotic use in children-a cross-national analysis of 6 countries. J Pediatr. 2017;182:239–244. doi: 10.1016/j.jpeds.2016.11.027. [DOI] [PubMed] [Google Scholar]