

Key Points
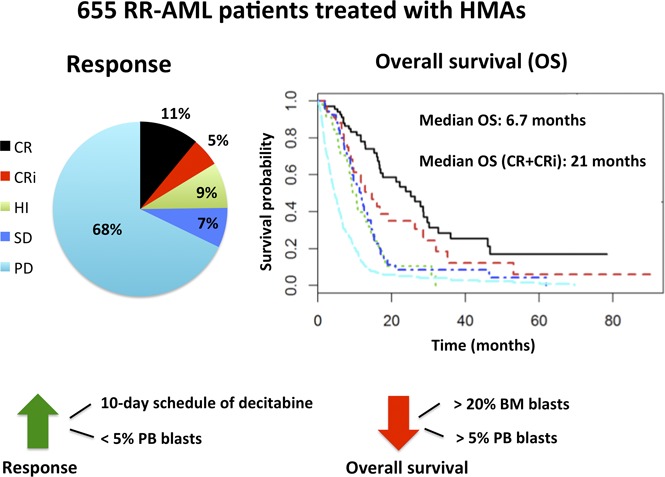
In the largest study of HMAs in RR-AML to date, 16% of patients achieved CR/CRi and experienced a median OS of 21 months.
Low proliferative disease (peripheral blood blasts <5%) was associated with improved response and OS.
Abstract
Although hypomethylating agents (HMAs) are frequently used in the frontline treatment of older acute myeloid leukemia (AML) patients, little is known about their effectiveness in relapsed or primary treatment–refractory (RR)-AML. Using an international multicenter retrospective database, we studied the effectiveness of HMAs in RR-AML and evaluated for predictors of response and overall survival (OS). A total of 655 patients from 12 centers received azacitidine (57%) or decitabine (43%), including 290 refractory (44%) and 365 relapsed (56%) patients. Median age at diagnosis was 65 years. Best response to HMAs was complete remission (CR; 11%) or CR with incomplete count recovery (CRi; 5.3%). Additionally, 8.5% experienced hematologic improvement. Median OS was 6.7 months (95% confidence interval, 6.1-7.3). As expected, OS differed significantly by best response, with patients achieving CR and CRi having a median OS of 25.3 and 14.6 months, respectively. In multivariate analysis, the presence of ≤5% circulating blasts and a 10-day schedule of decitabine were associated with improved response rates, whereas the presence of >5% circulating blasts and >20% bone marrow blasts were associated with decreased OS. A significant subset of RR-AML patients (16%) achieved CR/CRi with HMAs and experienced a median OS of 21 months. Outside of a clinical trial, HMAs represent a reasonable therapeutic option for some patients with RR-AML.
Visual Abstract
Introduction
Although intensive chemotherapy (IC) remains the standard of care for younger and more functionally fit individuals with acute myeloid leukemia (AML), patients with advanced age or poor performance status are often not treated with IC because of concerns for increased treatment-related morbidity and mortality, as well as inherent biologic disease resistance to cytotoxic therapy.1-3 For these patients, low-dose cytarabine and the hypomethylating agents (HMAs) azacitidine and decitabine have been increasingly used as less-intensive treatment options.1,4,5
The prognosis of older patients with relapsed or primary treatment–refractory AML (RR-AML) is particularly poor, with a median overall survival (OS) of only 3 to 7 months.6 There is no standard salvage therapy for RR-AML.1,2,7 The role of HMAs in patients with RR-AML after failure of IC is not well studied, with data limited to small and/or single-institution retrospective studies.8-10 The objective of this international retrospective study was to examine the patterns of use and efficacy of HMAs in a multicenter cohort of RR-AML patients and to assess for clinical and laboratory markers that could identify patients most likely to benefit from HMAs.
Patients and methods
Data source and eligibility
Deidentified data were collected by the individual centers, and the datasets were combined and analyzed at the coordinating center (Yale University). All patients aged ≥16 years with a pathologically confirmed World Health Organization (WHO)–defined AML (with ≥20% marrow blasts at time of diagnosis) who had received azacitidine or decitabine after relapse of AML or after failure of induction with ≥1 course of IC were included in the study. Patients were not selected based on response to therapy, and patients who relapsed after allogeneic stem cell transplantation (alloSCT) were included in this study. Data were collected spanning the period from 2006 to 2016. The participating centers included 12 large academic centers: 7 in the United States and 5 in Europe. There was no central review of the pathology, and the responses were determined by the local investigators. The study was approved by the institutional review boards of the authors' institutions and was conducted in accordance with the Declaration of Helsinki.
Relapse of AML was defined as the recurrence of >5% blasts in the peripheral blood (PB) and/or bone marrow (BM) of patients after achieving a complete remission (CR), whereas primary treatment-refractory AML was defined as the lack of achievement of CR or CR with incomplete count recovery (CRi) after therapy with ≥1 course of IC.11 Duration of the first CR was defined as the duration between CR achievement and the date of relapse and was set to 0 in patients with refractory AML.
Patient characteristics
When available, clinical and laboratory data were collected at the time of diagnosis, as well as at initiation of HMA. Cytogenetics were classified according to the Modified British Medical Research Council classification.12,13 Molecular data, including mutations in the FLT3, NPM1, CEBPα, TP53, DNMT3A, TET2, IDH1/2, ASXL1, and SF3B1 genes, were collected when available. Additional data extracted include the specific type of HMA (azacitidine or decitabine), the administration regimen, the number of cycles, and any concurrent therapy used along with HMAs.
Response criteria and survival
The primary end point of the study was OS, whereas the secondary end points included rates of CR and CRi. Best response was evaluated according to the 2003 revised International Working Group (IWG) AML criteria11 and was assigned by the investigator providing the data. Other response end points, including achievement of hematologic improvement (HI), stable disease (SD), and progressive disease (PD), as defined by the 2006 modified IWG criteria for myelodysplastic syndromes (MDS), were also collected.14 Response duration was measured from the date of response to progression or death, whichever happened sooner. OS was measured from time of initiation of HMAs until death or last follow-up.
Statistical analysis
Descriptive statistics were calculated to characterize the study cohort. We used the Student t test and χ2 test to compare continuous and categorical variables, respectively. Missing data were imputed using the multivariate imputation by chained equation approach, implemented with the mice package in R, with 10 iterations per variable.15 Details of the imputation methods are provided in the supplemental data. Survival outcomes were assessed at the last follow-up. Median OS was estimated with the Kaplan-Meier method, and the log-rank test was used to assess survival differences between groups. Univariate and multivariate Cox proportional hazards and logistic regression models assessed the association of covariates with OS and response rates, respectively (supplement data). All tests were 2-sided, with an α significance level of 0.05. All analyses were performed using R version 3.3.2.
Results
Study population
A total of 655 patients was studied, of whom 365 (56%) had relapsed and 290 (44%) had refractory AML (Table 1). By the end of the study, 87% of the patients had died. Median age at diagnosis was 65 years (range, 16-92). In total, 70% of patients had been diagnosed with de novo AML. Of the 30% who had secondary AML, 27% had therapy-related AML. The median number of prior therapies was 1 (range, 1-7); 26% had received 2 prior lines of therapy, and 18% had received ≥3 prior lines. Prior alloSCT was performed in 19% of patients. Among all patients, only 2% harbored a good-risk karyotype, whereas 40% had a poor-risk karyotype. Chromosome 5 and 7 abnormalities and a monosomal karyotype were reported in 20%, 22%, and 16% of patients, respectively. Data regarding FLT3, NPM1, and TP53 mutational status at the time of diagnosis were available in 269, 228, and 93 patients, respectively, of whom 17%, 24%, and 8% were reported to have FLT3, NPM1, or TP53 mutations, respectively. Information about other mutations was only available in a minority of patients, with IDH1/2 and CEBPα being the most commonly reported.
Table 1.
Patient characteristics
| All patients (N = 655) | Relapsed patients (n = 365) | Refractory patients (n = 290) | P | ||||
|---|---|---|---|---|---|---|---|
| Median or n | Range or % | Median or n | Range or % | Median or n | Range or % | ||
| Age, y (n = 636) | 65 | 16-92 | 65 | 16-89 | 64 | 19-92 | .8197 |
| Sex (N = 655) | .5432 | ||||||
| Male | 381 | 58.2 | 208 | 57 | 173 | 59.7 | |
| Female | 274 | 41.8 | 157 | 43 | 117 | 40.3 | |
| AML type (n = 650) | .0065 | ||||||
| De novo | 458 | 70.5 | 272 | 74.9 | 186 | 64.8 | |
| Secondary | 192 | 29.5 | 91 | 25.1 | 101 | 35.2 | |
| WHO type at diagnosis (n = 651) | |||||||
| AML with recurrent genetic abnormalities | 38 | 5.8 | 31 | 8.5 | 7 | 2.4 | .0020 |
| AML with myelodysplasia-related features | 175 | 26.9 | 86 | 23.6 | 89 | 31.1 | .0385 |
| Therapy-related AML | 52 | 8 | 31 | 8.5 | 21 | 7.3 | .6952 |
| AML, not otherwise specified | 386 | 59.3 | 217 | 59.5 | 169 | 59.1 | .9899 |
| CBC prior to initiation of HMA | |||||||
| WBC (n = 455) | 3.2 | 0.1-110.5 | 3.2 | 0.1-110.5 | 3.3 | 0.1-79.8 | .2843 |
| ANC (n = 415) | 0.9 | 0-72 | 1 | 0-72 | 0.8 | 0-54 | .7160 |
| Platelets (n = 454) | 40 | 0.6-810 | 44 | 2-293 | 35 | 0.6-810 | .4455 |
| PB blast % (n = 392) | 8 | 0-98 | 8 | 0-96 | 8 | 0-98 | .4862 |
| BM prior to initiation of HMA | |||||||
| BM blast % (n = 305) | 27 | 2-100 | 27 | 2-100 | 26.5 | 2-95 | .5606 |
| BM cellularity % (n = 244) | 40 | 2-100 | 40 | 2-100 | 40 | 2-100 | .2496 |
| MRC cytogenetic risk group prior to initiation of HMA (n = 225) | .7794 | ||||||
| Good | 4 | 1.8 | 3 | 2.5 | 1 | 1 | |
| Intermediate | 131 | 58.2 | 70 | 57.9 | 61 | 58.7 | |
| Poor | 90 | 40 | 48 | 39.7 | 42 | 40.4 | |
| Chromosomal abnormalities | |||||||
| Complex (n = 224) | 54 | 24.1 | 29 | 24 | 25 | 24.3 | 1 |
| Monosomy (n = 234) | 37 | 15.8 | 20 | 15.6 | 17 | 16 | 1 |
| Chromosome 7 abn (n = 224) | 50 | 22.3 | 28 | 23.1 | 22 | 21.4 | .8744 |
| Chromosome 5 abn (n = 224) | 44 | 19.6 | 21 | 17.4 | 23 | 22.3 | .4441 |
| Mutational status (prior to start of HMA or at diagnosis) | |||||||
| TP53 (n = 93) | 7 | 7.5 | 5 | 7.7 | 2 | 7.1 | 1 |
| FLT3 (n = 269) | 46 | 17.1 | 34 | 20.9 | 12 | 11.3 | .0622 |
| NPM1 (n = 228) | 55 | 24.1 | 42 | 30.7 | 13 | 14.3 | .0076 |
| CEBPa (n = 124) | 8 | 6.5 | 7 | 8.3 | 1 | 2.5 | .4349 |
| DNMT3A (n = 39) | 5 | 12.8 | 3 | 11.1 | 2 | 16.7 | .6342 |
| TET2 (n = 37) | 2 | 5.4 | 2 | 7.4 | 0 | 0 | 1 |
| IDH1/2 (n = 39) | 5 | 12.8 | 4 | 13.8 | 1 | 10 | 1 |
| ASXL1 (n = 11) | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| SF3B1 (n = 7) | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Number of therapy lines prior to HMA (n = 648) | 1 | 1-7 | 1 | 1-7 | 1 | 1-7 | .8463 |
| Duration of CR1 prior to initiation of HMA (n = 329) | 1.95 | 0-180 | 8 | 0.5-180 | 0 | 0-0 | <.0001 |
| AlloSCT prior to initiation of HMA (months) (n = 618) | 115 | 18.6 | 91 | 27 | 24 | 8.5 | <.0001 |
| HMA used (n = 634) | .1695 | ||||||
| Azacitidine | 360 | 56.8 | 192 | 54.2 | 168 | 60 | |
| Decitabine | 274 | 43.2 | 162 | 45.8 | 112 | 40 | |
| Number of cycles of HMA (n = 633) | 3 | 1-36 | 3 | 1-36 | 3 | 1-34 | .4922 |
| Azacitidine | 3 | 1-36 | 3 | 1-36 | 4 | 1-34 | .4684 |
| Decitabine | 2 | 1-35 | 2 | 1-35 | 2 | 1-22 | .8129 |
| HMA administration schedule (n = 587) | .3654 | ||||||
| Azacitidine (n = 336) | |||||||
| 7-0 | 257 | 76.5 | 131 | 73.2 | 126 | 80.3 | |
| 5-2-2 | 18 | 2.4 | 10 | 5.6 | 8 | 5.1 | |
| 5-0 | 60 | 17.9 | 38 | 21.2 | 22 | 14.0 | |
| 10-0 | 1 | 0.3 | 0 | 0 | 1 | 0.6 | |
| Decitabine (n = 251) | |||||||
| 7-0 | 3 | 1.2 | 1 | 0.7 | 2 | 1.8 | |
| 5-2-2 | 2 | 0.8 | 0 | 0 | 2 | 1.8 | |
| 5-0 | 181 | 72.1 | 104 | 73.8 | 77 | 70.0 | |
| 10-0 | 50 | 19.9 | 29 | 20.6 | 21 | 19.1 | |
| Others | 15 | 6.0 | 7 | 5.0 | 8 | 7.3 | |
| Agents used concurrently with HMA (n = 532) | .0585 | ||||||
| Gemtuzumab ozogamicin | 64 | 12 | 25 | 9 | 39 | 15.4 | |
| Valproic acid | 7 | 1.3 | 2 | 0.7 | 5 | 2 | |
| Valproic acid plus all-trans retinoic acid | 24 | 4.5 | 11 | 3.9 | 13 | 5.1 | |
| Hydroxyurea | 12 | 2.3 | 5 | 1.8 | 7 | 2.8 | |
| Cytarabine | 2 | 0.4 | 1 | 0.4 | 1 | 0.4 | |
| Anthracycline | 4 | 0.8 | 0 | 0 | 4 | 1.6 | |
| Sorafenib | 13 | 2.4 | 10 | 3.6 | 3 | 1.2 | |
| Hedgehog inhibitor | 4 | 0.8 | 1 | 0.4 | 3 | 1.2 | |
| IDH inhibitor | 1 | 0.2 | 0 | 0 | 1 | 0.4 | |
| Erythrocyte-stimulating agents | 7 | 1.3 | 5 | 1.8 | 2 | 0.8 | |
| Granulocyte colony-stimulating factor | 8 | 1.5 | 4 | 1.4 | 4 | 1.6 | |
| JAK | 1 | 0.2 | 1 | 0.4 | 0 | 0 | |
| Dead at end of study (n = 608) | 529 | 87 | 295 | 86.8 | 234 | 87.3 | .9376 |
abn, abnormality; ANC, absolute neutrophil count; MRC, Modified British Medical Research Council.
At the onset of HMA treatment, median white blood cell count (WBC) was 3.2 × 109/L (range, 0.1-110.5 × 109/L), with only 20 patients having WBCs >50 × 109/L; 254 (55.9%) patients had platelet counts <50 × 109/L, and 220 (53.0%) had absolute neutrophil counts <1.0 × 109/L. Median BM blast percentage was 24%, with 213 patients (55.0%) having >20% BM blasts at the time of HMA initiation. A total of 272 patients (69.4%) had blasts detected in the blood, whereas 120 patients (30.6%) had no blasts detected in the blood (for 263 patients data regarding PB blasts was missing).
Patterns of treatment with HMA
Azacitidine was used in 57% of patients, whereas decitabine was administered in the other 43%. The median number of azacitidine cycles was 3 (range, 1-36), compared with 2 for decitabine (range, 1-35; P = .5) (Table 1). Among patients who were treated with azacitidine, 76.5% received the US Food and Drug Administration–approved 7-day (7-0) schedule of azacitidine, whereas 17.9% and 2.4% of patients used a 5-day (5-0) and a 7-day schedule with a weekend break (5-2-2), respectively. Among decitabine users, the drug was given on a 5-day (5-0), 7-day (7-0), and 10-day (10-0) schedule in 72.1%, 1.2%, and 19.9% of patients, respectively (Table 1). HMAs were stopped in the majority of patients because of progression of disease (55.5%) or because no response was achieved with HMAs (27.6%), whereas in a smaller group of patients, they were stopped because of the treatment protocol (9.1%) or side effects (6.3%); 1.4% of patients were still receiving HMAs at the time of the study.
A total of 146 patients (28%) received other therapeutic agents in combination with azacitidine and decitabine; the most frequently used were gemtuzumab ozogamicin and valproic acid (Table 1). Following HMA therapy, 62% of patients did not receive any further therapy; 37 patients (5.6%) underwent alloSCT (Table 2).
Table 2.
Outcome analysis
| Characteristic | All patients (N = 655) | Relapsed AML (n = 365) | Refractory AML (n = 290) | Bridging to alloSCT (n = 63) | P |
|---|---|---|---|---|---|
| Response (n = 638), n (%) | Relapsed vs refractory = .0248, alloSCT vs no alloSCT < .0001 | ||||
| CR | 70 (11) | 41 (11.6) | 29 (10.2) | 18 (28.6) | |
| CRi | 34 (5.3) | 25 (7.1) | 9 (3.2) | 15 (23.8) | |
| HI | 54 (8.5) | 21 (5.9) | 33 (11.6) | 2 (3.2) | |
| SD | 47 (7.4) | 24 (6.8) | 23 (8.1) | 8 (12.7) | |
| PD | 433 (67.9) | 242 (68.6) | 191 (67.0) | 20 (31.7) | |
| OS based on response (n = 621), median (95% CI), mo | 6.7 (6.1-7.3) | 6.2 (5.6-7.4) | 7 (6.4-8.9) | 12.5 (9.7-17) | Relapsed vs refractory = .47, alloSCT vs no alloSCT < 0.0001 |
| CR | 25.3 (17-30.2) | 23.9 (16.8-46.2) | 25.3 (16.7-Inf) | 17.7 (15.3-Inf) | |
| CRi | 14.6 (9.5-32) | 11.7 (9.5-Inf) | 16.1 (8.9-Inf) | 11.7 (9.5-Inf) | |
| HI | 11.7 (9.4-14.6) | 9.4 (7.8-46.5) | 11.7 (9.7-14.9) | 9.4 (NA) | |
| SD | 10.4 (8.7-14) | 8.7 (5.8-16.4) | 10.6 (9.1-17.7) | 16.4 (10.6-Inf) | |
| PD | 4.5 (4.1-5.3) | 4.7 (3.9-5.6) | 4.4 (3.8-5.9) | 6.7 (4.5-16.6) | |
| OS based on HMA used (n = 621), median (95% CI), mo | |||||
| Azacitidine | 6.8 (6-8.5) | 6.3 (5.3-8.4) | 7.5 (6.5-9.4) | 16.1 (9.5-Inf) | Relapsed vs refractory = 0.532, alloSCT vs no alloSCT = 0.0237 |
| Decitabine | 6.2 (5.3-7.3) | 6.2 (5.3-8.4) | 6.5 (4.4-7.7) | 11.7 (9.3-17.7) | Relapsed vs refractory = 0.969, alloSCT vs no alloSCT < 0.0001 |
| Duration of response (n = 62), median (range), mo | 8.5 (1-84) | 10 (1-84) | 5 (2-36.9) | 5 (1-36.9) | Relapsed vs refractory = .3112, alloSCT vs no alloSCT = .4014 |
| Reason for discontinuation of HMA (n = 492), n (%) | Relapsed vs refractory = .0905, alloSCT vs no alloSCT < .0001 | ||||
| Intolerance | 31 (6.3) | 18 (6.4) | 13 (6.2) | 2 (3.2) | |
| No response | 136 (27.6) | 65 (23) | 71 (33.8) | 8 (12.7) | |
| Progression of disease | 273 (55.5) | 170 (60.3) | 103 (49) | 24 (38.1) | |
| End of protocol | 45 (9.1) | 25 (8.9) | 20 (9.5) | 29 (46) | |
| Ongoing treatment, n (%) | 7 (1.4) | 4 (1.4) | 3 (1.4) | 0 (0) | |
| Number of lines of therapy after HMA failure (n = 612), median (range) | 0 (0-6) | 0 (0-5) | 0 (0-6) | 1 (0-6) | Relapsed vs refractory = .6315, alloSCT vs no alloSCT = .0004 |
| AlloSCT after HMA therapy (n = 629), n (%) | 37 (5.6) | 16 (43.2) | 21 (56.8) | — | Relapsed vs refractory = .5108 |
Inf, infinity; NA, not applicable.
Response to HMA therapy and predictors
Best responses achieved with HMA therapy were CR in 11%, CRi in 5.3%, HI in 8.5%, and SD in 7.4%, whereas 67.9% of patients had PD (Table 2). Among patients who achieved CR/CRi, the response duration was limited, with a median of 8.5 months (95% CI, 8.3-15.1). The median duration of CR was 10 months (95% confidence interval [CI], 8-17.3), whereas it was 8.4 months (95% CI, 5.2-14.5; P = .4) for CRi. The CR/CRi rate was not significantly different between relapsed and refractory AML patients (P = .09). Similarly, response duration did not differ between refractory and relapsed AML patients (P = .3). Results of univariate logistic regression analysis are provided in supplemental Table 1.
In a multivariate logistic-regression analysis, variables that were significantly associated with higher odds of achieving CR/CRi included presence of ≤5% PB blasts (odds ratio [OR], 1.87; 95% CI, 1.07-3.26; P = .0278) and a 10-day schedule of decitabine (OR, 2.37; 95% CI, 1.05-5.33; P = .0374). Age, sex, Eastern Cooperative Oncology Group (ECOG) performance status of the patient, disease status (refractory vs relapsed AML), WHO subtype of AML, cytogenetic risk group, and the use of a specific type of HMA did not significantly affect the odds of achieving CR/CRi (Figure 3A; supplemental Table 2).
Figure 3.

Forrest plots from multivariate analysis. Forrest plot for prognostic factors of response (CR+CRi) (A) and mortality (B).
OS after HMA treatment and predictors
The 30-day mortality from the date of HMA initiation was 6.4% (95% CI, 4.6-8.8). Median OS from the time of initiation of HMA was 6.7 months (95% CI, 6.1-7.3) for the entire study population (Figure 1A; Table 2). The OS correlated significantly with the best response achieved with HMA therapy (Figure 1B; Table 2). Median OS was 25.3 months (95% CI, 17-30.2) or 14.6 months (95% CI, 9.5-32) for patients achieving a CR or CRi, respectively. The OS of those who achieved CR or CRi as their best response to HMA therapy was significantly better than the OS of patients who demonstrated PD (median OS, 4.5 months; 95% CI, 4.1-5.3 for patients with PD; P < .0001 for both comparisons). Patients who achieved HI or SD as their best response to HMA therapy had a median OS of 11.7 months (95% CI, 9.4-14.6 months) or 10.4 months (95% CI, 8.7-14 months), respectively; these results were significantly higher than the OS of patients who developed PD (P < .0002 for both comparisons, Figure 1B; Table 2). In a landmark analysis, at 2, 4, and 6 months from the start of HMA treatment, the effect of response to HMA (CR+CRi) on OS remained significant. In landmark analyses, the median OS for responders vs nonresponders was 21.9 vs 5.1 months, 19.9 vs 5.1 months, and 19.3 vs 4.9 months at 2, 4, and 6 months, respectively (all log-rank P < .0001). Survival curves did not change significantly when follow-up was assessed at the time of alloSCT (supplemental Figure 1).
Figure 1.

Outcome for all patients based on response achieved and type of treatment used. (A) OS probability from onset of HMA treatment in the global cohort. OS probability from onset of HMA treatment according to AML IWG response criteria (for CR/CRi/PD) and MDS IWG response criteria (SD/HI) (B) and according to HMA used (azacitidine vs decitabine) (C).
In the univariate and multivariate Cox proportional hazards model for OS, the presence of circulating blasts (PB blasts > 5% vs ≤5%, hazard ratio [HR], 1.29; 95% CI, 1.05-1.58; P = .02) and >20% blasts in the BM (BM blasts > 20% vs ≤20%, HR, 1.24; 95% CI, 1.01-1.53; P = .04) were significant predictors for inferior OS. Additionally, in univariate analysis, a longer duration of CR1 (duration of CR1 > 12 months vs ≤12 months, HR, 0.74; 95% CI 0.58-0.93; P = .01) was associated with better OS, whereas a lower platelet count (platelet count ≤ 30 × 109/L vs >30 × 109/L, HR, 1.31; 95% CI 1.07-1.6; P = .008), more lines of prior therapy (2 vs 1 prior line of therapy, HR, 1.25; 95% CI 1.02-1.5; P = .03), and the use of decitabine (decitabine vs azacitidine, HR, 1.2; 95% CI 1.02-1.45; P = .03) were associated with shorter OS (Figures 1C, 2A, and 3B; supplemental Tables 3 and 4). The age, sex, ECOG performance status of the patient and the disease status (refractory vs relapsed AML), WHO subtype of AML, and cytogenetic risk group did not significantly affect survival with HMA therapy (Figures 2B and 3B; supplemental Tables 3 and 4). In contrast to the effects on achieving CR/CRi, the schedule of HMA therapy did not have a significant impact on OS. Patients who used the 10-day schedule of decitabine did not have a better OS than patients receiving any other schedule of HMA (HR, 0.87; 95% CI, 0.62-1.24; P = .46) (supplemental Figure 1C; supplemental Table 4). The mutational status (TP53, FLT3, and NPM1 mutations) did not have an impact on OS (supplemental Figure 1D-E; supplemental Tables 3 and 4). The combination of additional agents with HMA therapy did not improve OS or response rates.
Figure 2.

Outcome based on PB blast percentage, as well as cytogenetic markers. OS probability from onset of HMA treatment according to PB blast percentage (>5% vs ≤5%) (A) and cytogenetic risk (intermediate/normal vs poor) (B).
Discussion
To our knowledge, this international study represents the largest reported experience of HMA use in patients with RR-AML.8-10,16-18 As expected, patients in this cohort were older (median age 65 years) and exhibited high-risk disease features, such as poor-risk karyotypes (40%) and secondary AML (30%). Although the OS for the entire cohort was poor (median, 6.7 months), a significant subset of patients (16%) achieved CR/CRi with HMAs and achieved a median OS of 21.2 months (95% CI, 16.3-28.6).
For this cohort of RR-AML with many patients exhibiting high-risk features, the observed CR/CRi rates appear reasonable and compare favorably with rates that can be achieved with other lower-intensity therapy options (eg, low-dose cytarabine, clofarabine) in the relapsed and refractory (RR) setting.6,19-21 Although the CR/CRi rate with HMAs in the RR setting in our study was lower compared with the use of azacitidine in elderly AML patients, with >30% BM blasts in the frontline setting (CR/CRi 27.8%),5 the median OS for patients who achieved a CR/CRi was impressive for patients in the RR setting (Figure 1B). Although most patients progressed eventually on HMA therapy, the response duration of 8.5 months for CR/CRi (CR 10 months, 95% CI, 8-17.3; CRi 8.4 months, 95% CI, 5.2-14.5) was comparable to the duration of CR/CRi (10.5 months) in older AML patients treated with azacitidine in the frontline setting.5
Similar to what was observed in the setting of IC for AML, achievement of CR was associated with a trend for improved OS compared with CRi (25.3 vs 14.6 months; P = .05). Although HI and SD are not formally identified objective responses in AML, compared with MDS, the achievement of HI and SD in our cohort was associated with improved OS compared with those who had PD (Figure 1B). These observations support the efforts of refining existing criteria or establishing new criteria associated with meaningful clinical benefit in AML, such as those recently seen in clinical trials of novel agents, such as IDH inhibitors, FLT3 inhibitors, and venetoclax.22-24
Given the low response rates associated with HMAs in AML, there have been efforts to identify predictors of clinical benefit. However, no consistently predictive clinical, pathological, or laboratory parameters have been identified. In one study of older RR-AML patients, higher PB blast counts were associated with worse response rates to HMA therapy, whereas high-risk cytogenetics and PB blasts >10% were predictive of inferior OS in a multivariate analysis.8 Similarly, in our much larger cohort, worse response rates and OS were predicted by a higher percentage of blasts in the PB and the BM (for OS), which argues for HMAs being more effective in AML patients with lower proliferation rates. We did not observe an adverse prognostic impact for poor-risk cytogenetics after IC failure, which was reported in prior studies (Figure 2B).6,8,25-28 Neither age nor WBC at relapse, which are prognostic markers for salvage IC, had a significant prognostic impact on OS in our cohort of patients treated with HMAs.6,25 The prognostic impact of molecular information in RR-AML is understudied and controversial.25,29 In a multivariate analysis of patients with RR-AML, shorter CR1 duration was associated with decreased OS, but FLT3 and NPM1 mutation status was not significantly associated with OS.29 Similarly, in our study, NPM1 and FLT3 mutational status was not significantly associated with response or OS.
In a recent study of AML and MDS patients treated with 10-day cycles of decitabine, response rates were higher in patients with unfavorable-risk cytogenetic abnormalities compared with those with intermediate- or favorable-risk cytogenetics.30,31 All patients with TP53 mutations responded to decitabine, and the OS for patients with TP53 mutations was not significantly different from the OS seen in patients without the mutations and was longer than that historically observed in such patients treated with more aggressive therapies.32,33 Our patients with poor-risk cytogenetics and TP53 mutations similarly did not have a statistically significant worse OS compared with patients with intermediate/good-risk cytogenetics and no TP53 mutations, respectively (Figure 3B).
Azacitidine and decitabine have not been directly compared in the setting of RR-AML in randomized prospective trials. In our analysis, the response rates and OS associated with azacitidine and decitabine were not significantly different in multivariate analyses, whereas decitabine-treated patients had worse OS compared with azacitidine-treated patients in univariate analyses. Interestingly, patients receiving the 10-day schedule of decitabine had a higher CR/CRi rate than patients who received other HMA schedules (28% vs 15.7%, P = .04). The higher response rate associated with a 10-day schedule of decitabine in our study is intriguing, because longer exposure to decitabine might lead to improved efficacy,10,34 and in the above-mentioned study, a 10-day schedule of decitabine led to surprisingly high response and OS rates in a high-risk patient population.30,31 However, given the retrospective nature of our study with potential differences in characteristics between groups of patients receiving different HMAs on various schedules, it is impossible to conclude with certainty whether the prolonged administration of decitabine had a causal effect on response rates. Furthermore, the improved response rate seen with a 10-day schedule of decitabine in multivariate analyses did not translate to a difference in OS (8 months vs 6.6 months, P = .13) in multivariate analyses, although an association between CR/CRi and improved survival was observed in the entire cohort.
Like any other retrospective study, selection bias is an important limitation. Furthermore, all patients were treated in specialized tertiary care centers, and this may impact the broad applicability of the data. We did not specifically measure or qualify comorbidities that might influence patient outcomes. We also did not measure days of hospitalization or side effects associated with HMAs, although the investigators reported that only a minority of patients (6%) stopped HMAs because of intolerance, and the 30-day mortality was relatively low (6.4%) compared with IC.
It is important to recognize that to achieve a CR with HMA treatment, a sufficient number of cycles of HMAs is required .The median number of azacitidine cycles was 3 (range, 1-36) compared with 2 for decitabine (range, 1-35; P = .5). We did not have detailed information available regarding why treatment was stopped early in some patients. Additionally, patient frailty is often not identified by the patient’s age and performance status alone, which were the surrogate markers for frailty in this study. In this context, it would have been helpful if there had been universal adoption of geriatric measures or formal comorbidity screening. Finally, molecular mutation data were missing for many patients.
The value of our study is that it helps to inform the discussion between providers and patients regarding HMAs as a treatment option for RR-AML, shows the urgent need for improved therapeutic options, and serves as a valuable reference in the development of future clinical trial using HMAs as the backbone.
Our study shows that 16% of RR-AML patients achieved CR/CRi with HMA therapy, which is associated with a survival benefit. Although this remission rate is objectively low, it is comparable to other salvage approaches in RR-AML, and therapies with HMAs provide a manageable side effect profile that allows for outpatient therapy. For these reasons, HMAs are a reasonable therapeutic option for patients with RR-AML in the absence of clinical trial options.
Future efforts should focus on identifying predictive factors to select patients who are most likely to derive benefit from HMA therapy and on rationally designing combination-based trials using agents that exhibit synergistic effects with HMAs. Because many future HMA-based combination studies will be conducted as single-arm studies before proceeding to a randomized study, our efficacy data for HMAs in RR-AML in this very large and diverse cohort serve as an important reference point for the design of these trials.
Supplementary Material
The full-text version of this article contains a data supplement.
Acknowledgments
The authors acknowledge all of the patients whose data were added to this database.
The Frederick A. DeLuca Foundation supported the statistical analyses.
Authorship
Contribution: M.S., M.D., and A.M.Z. conceived and designed the study; M.S., M.D., J.D.B. and A.M.Z. analyzed and interpreted data; and all authors provided study materials or patients; collected and assembled data; wrote, critically revised, and gave final approval of the manuscript; and are accountable for all aspects of the work.
Conflict-of-interest disclosure: P.M. received honoraria and research funding from Celgene. R.I. received research funding from Janssen Pharmaceuticals and Novartis. E.K.R. is a consultant for Novartis, Incyte, Celgene, and Pfizer; a member of the speaker’s bureau for Incyte, Celgene, Novartis, and ARIAD; has received travel monies from Celgene and Novartis; has an advisory role for Incyte, Pfizer, and Celgene; and received institutional research funding from Pfizer, Astellas Pharma, Bristol-Myers Squibb, and NS Pharma. M.A.S. is on the Board of Directors or advisory committees for Celgene, Takeda, and Opsona. N.A.P. is a consultant for CTI BioPharma, Alexion Pharmaceuticals, ARIAD, and Incyte and received institutional research funding from Boehringer Ingelheim, Astellas Pharma, Daiichi Sankyo, Sunesis Pharmaceuticals, Celator, Pfizer, and Astex Pharmaceuticals. A.M.B. received institutional research funding from Celgene and Takeda. R.S.K. has stock or other ownership in AbbVie; has received travel monies from Celgene, Alexion Pharmaceuticals, and Incyte; has received honoraria from or is a consultant for Celgene and Novartis; is a member of the speaker’s bureau for Novartis and Alexion Pharmaceuticals; and has received institutional research funding from Celgene, GlaxoSmithKline, Eleos, Boehringer Ingelheim, and Incyte. A.A.-K. received institutional research funding from Novartis, Onconova Therapeutics, Celgene, Bristol-Myers Squibb, Astex Pharmaceuticals, and Ambit Biosciences. V.S. is a consultant for Janssen Pharmaceuticals, AbbVie, and Otsuka; has received honoraria from Celgene, Janssen Pharmaceuticals, and Novartis; has received research funding from Celgene; and is on the Board of Directors or advisory committees for AbbVie and Amgen. A.T.F. is a consultant for Seattle Genetics, Celgene, Agios, MedImmune, and Amgen; has received honoraria from Seattle Genetics, Celgene, Agios, and Pfizer; is on the Board of Directors or advisory committees for Seattle Genetics, Juno, Celgene, Agios, MedImmune, and Amgen; and has received research funding from Seattle Genetics, Takeda, and Celgene. G.J.R. is a consultant for AbbVie, Agios, Amgen, Amphivena, Array Biopharma, Astex Pharmaceuticals, AstraZeneca, Celator, Celgene, Clovis Oncology, CTI BioPharma, Genoptix, Immune Pharmaceuticals, Janssen Pharmaceuticals, Juno, MedImmune, MEI Pharma, Novartis, Onconova Therapeutics, Pfizer, Roche, Boehringer Ingelheim, GlaxoSmithKline, Shire, Astex Pharmaceuticals, Cellectis, and Sunesis Pharmaceuticals; received research funding from Cellectis; received travel monies from AstraZeneca, Shire, Astellas Pharma, Celator, Incyte, Roche, Amphivena, MEI Pharma, Astex Pharmaceuticals, Janssen Pharmaceuticals, and Juno Therapeutics; and received institutional research funding from AbbVie, Agios, Astex Pharmaceuticals, Celgene, CTI BioPharma, Karyopharm Therapeutics, MedImmune, MEI Pharma, Moffitt, Novartis, Onconova Therapeutics, Pfizer, Sunesis Pharmaceuticals, Tensha Therapeutics, and Cellectis. P.F. received honoraria and research funding from Amgen, Astex, Celgene, and Janssen Pharmaceuticals. M.R.L. has received research funding from Amgen, Novartis, Astellas Pharma, and Actinium Pharmaceuticals; has received honoraria and travel monies from Amgen; and is a consultant for Amgen. N.V. received honoraria from and is a consultant for Amgen, Celgene, Novartis, Roche, and Servier. U.G. received honoraria and research funding from Celgene and Novartis and received honoraria from Janssen Pharmaceuticals. A.M.Z. received honoraria from and is a consultant for AbbVie, Ostuka, Pfizer, Gilead, Celgene, Ariad, Incyte, Agios, Novartis, Takeda, Daiichi Sankyo, and Boehringer Ingelheim; received honoraria from and is a member of the speaker’s bureau for Takeda; and received institutional research funding from Celgene, Pfizer, Incyte, ADC Therapeutics, Medimmune, Takeda, AbbVie, and Boehringer Ingelheim. The remaining authors declare no competing financial interests.
Correspondence: Amer M. Zeidan, Section of Hematology, Department of Internal Medicine, Yale School of Medicine, 333 Cedar St, New Haven, CT 06510-3222; e-mail: amer.zeidan@yale.edu.
References
- 1.Podoltsev NA, Stahl M, Zeidan AM, Gore SD. Selecting initial treatment of acute myeloid leukaemia in older adults. Blood Rev. 2017;31(2):43-62. [DOI] [PubMed] [Google Scholar]
- 2.Döhner H, Estey EH, Amadori S, et al. ; European LeukemiaNet. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010;115(3):453-474. [DOI] [PubMed] [Google Scholar]
- 3.Büchner T, Berdel WE, Haferlach C, et al. Age-related risk profile and chemotherapy dose response in acute myeloid leukemia: a study by the German Acute Myeloid Leukemia Cooperative Group. J Clin Oncol. 2009;27(1):61-69. [DOI] [PubMed] [Google Scholar]
- 4.Burnett AK, Milligan D, Prentice AG, et al. A comparison of low-dose cytarabine and hydroxyurea with or without all-trans retinoic acid for acute myeloid leukemia and high-risk myelodysplastic syndrome in patients not considered fit for intensive treatment. Cancer. 2007;109(6):1114-1124. [DOI] [PubMed] [Google Scholar]
- 5.Dombret H, Seymour JF, Butrym A, et al. International phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood. 2015;126(3):291-299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sarkozy C, Gardin C, Gachard N, et al. Outcome of older patients with acute myeloid leukemia in first relapse. Am J Hematol. 2013;88(9):758-764. [DOI] [PubMed] [Google Scholar]
- 7.Thol F, Schlenk RF, Heuser M, Ganser A. How I treat refractory and early relapsed acute myeloid leukemia. Blood. 2015;126(3):319-327. [DOI] [PubMed] [Google Scholar]
- 8.Itzykson R, Thépot S, Berthon C, et al. Azacitidine for the treatment of relapsed and refractory AML in older patients. Leuk Res. 2015;39(2):124-130. [DOI] [PubMed] [Google Scholar]
- 9.Gemuenden C, Benz R, Senn O, Goede JS, Manz MG, Gerber B. Efficacy of azacitidine in de novo and relapsed acute myeloid leukemia: a retrospective comparative study. Clin Lymphoma Myeloma Leuk. 2015;15(12):811-815. [DOI] [PubMed] [Google Scholar]
- 10.Ritchie EK, Feldman EJ, Christos PJ, et al. Decitabine in patients with newly diagnosed and relapsed acute myeloid leukemia. Leuk Lymphoma. 2013;54(9):2003-2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cheson BD, Bennett JM, Kopecky KJ, et al. ; International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. Revised recommendations of the International Working Group for diagnosis, standardization of response criteria, treatment Outcomes, and reporting standards for therapeutic trials in acute myeloid leukemia [published correction appears in J Clin Oncol. 2004;22(3):576]. J Clin Oncol. 2003;21(24):4642-4649. [DOI] [PubMed] [Google Scholar]
- 12.Grimwade D, Hills RK, Moorman AV, et al. ; National Cancer Research Institute Adult Leukaemia Working Group. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood. 2010;116(3):354-365. [DOI] [PubMed] [Google Scholar]
- 13.Breems DA, Van Putten WL, De Greef GE, et al. Monosomal karyotype in acute myeloid leukemia: a better indicator of poor prognosis than a complex karyotype. J Clin Oncol. 2008;26(29):4791-4797. [DOI] [PubMed] [Google Scholar]
- 14.Cheson BD, Greenberg PL, Bennett JM, et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood. 2006;108(2):419-425. [DOI] [PubMed] [Google Scholar]
- 15.van Buuren S, Groothuis-Oudshoorn K. mice: Multivariate Imputation by Chained Equations in R. J Stat Software. 2011;45(3). [Google Scholar]
- 16.Al-Ali HK, Jaekel N, Junghanss C, et al. Azacitidine in patients with acute myeloid leukemia medically unfit for or resistant to chemotherapy: a multicenter phase I/II study. Leuk Lymphoma. 2012;53(1):110-117. [DOI] [PubMed] [Google Scholar]
- 17.Maurillo L, Venditti A, Spagnoli A, et al. Azacitidine for the treatment of patients with acute myeloid leukemia: report of 82 patients enrolled in an Italian Compassionate Program. Cancer. 2012;118(4):1014-1022. [DOI] [PubMed] [Google Scholar]
- 18.Pleyer L, Stauder R, Burgstaller S, et al. Azacitidine in patients with WHO-defined AML - results of 155 patients from the Austrian Azacitidine Registry of the AGMT-Study Group. J Hematol Oncol. 2013;6(1):32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Faderl S, Wetzler M, Rizzieri D, et al. Clofarabine plus cytarabine compared with cytarabine alone in older patients with relapsed or refractory acute myelogenous leukemia: results from the CLASSIC I Trial. J Clin Oncol. 2012;30(20):2492-2499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Roboz GJ, Rosenblat T, Arellano M, et al. International randomized phase III study of elacytarabine versus investigator choice in patients with relapsed/refractory acute myeloid leukemia. J Clin Oncol. 2014;32(18):1919-1926. [DOI] [PubMed] [Google Scholar]
- 21.Mangan JK, Luger SM. Salvage therapy for relapsed or refractory acute myeloid leukemia. Ther Adv Hematol. 2011;2(2):73-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutantIDH2relapsed or refractory acute myeloid leukemia. Blood. 2017;130(6):722-731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Perl AE, Altman JK, Cortes J, et al. Selective inhibition of FLT3 by gilteritinib in relapsed or refractory acute myeloid leukaemia: a multicentre, first-in-human, open-label, phase 1-2 study. Lancet Oncol. 2017;18(8):1061-1075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Konopleva M, Pollyea DA, Potluri J, et al. Efficacy and biological correlates of response in a phase II study of venetoclax monotherapy in patients with acute myelogenous leukemia. Cancer Discov. 2016;6(10):1106-1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chevallier P, Labopin M, Turlure P, et al. A new Leukemia Prognostic Scoring System for refractory/relapsed adult acute myelogeneous leukaemia patients: a GOELAMS study. Leukemia. 2011;25(6):939-944. [DOI] [PubMed] [Google Scholar]
- 26.Itzykson R, Thépot S, Quesnel B, et al. ; Groupe Francophone des Myelodysplasies(GFM). Prognostic factors for response and overall survival in 282 patients with higher-risk myelodysplastic syndromes treated with azacitidine. Blood. 2011;117(2):403-411. [DOI] [PubMed] [Google Scholar]
- 27.van der Helm LH, Alhan C, Wijermans PW, et al. Platelet doubling after the first azacitidine cycle is a promising predictor for response in myelodysplastic syndromes (MDS), chronic myelomonocytic leukaemia (CMML) and acute myeloid leukaemia (AML) patients in the Dutch azacitidine compassionate named patient programme. Br J Haematol. 2011;155(5):599-606. [DOI] [PubMed] [Google Scholar]
- 28.Ravandi F, Issa JP, Garcia-Manero G, et al. Superior outcome with hypomethylating therapy in patients with acute myeloid leukemia and high-risk myelodysplastic syndrome and chromosome 5 and 7 abnormalities. Cancer. 2009;115(24):5746-5751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.How J, Sykes J, Minden MD, et al. The prognostic impact of FLT3-ITD and NPM1 mutations in patients with relapsed acute myeloid leukemia and intermediate-risk cytogenetics. Blood Cancer J. 2013;3(5):e116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Welch JS, Petti AA, Miller CA, et al. TP53 and decitabine in acute myeloid leukemia and myelodysplastic syndromes. N Engl J Med. 2016;375(21):2023-2036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Estey E. Acute myeloid leukemia - many diseases, many treatments. N Engl J Med. 2016;375(21):2094-2095. [DOI] [PubMed] [Google Scholar]
- 32.Ohgami RS, Ma L, Merker JD, et al. Next-generation sequencing of acute myeloid leukemia identifies the significance of TP53, U2AF1, ASXL1, and TET2 mutations. Mod Pathol. 2015;28(5):706-714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bowen D, Groves MJ, Burnett AK, et al. TP53 gene mutation is frequent in patients with acute myeloid leukemia and complex karyotype, and is associated with very poor prognosis. Leukemia. 2009;23(1):203-206. [DOI] [PubMed] [Google Scholar]
- 34.Blum W, Garzon R, Klisovic RB, et al. Clinical response and miR-29b predictive significance in older AML patients treated with a 10-day schedule of decitabine. Proc Natl Acad Sci USA. 2010;107(16):7473-7478. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.