

Key Points
There was no difference in overall survival after allogeneic transplant between patients aged 55-64 years and patients ≥65 years.
Age alone should not be a determinant for allogeneic transplant eligibility among older non-Hodgkin lymphoma patients.
Abstract
The application of allogeneic hematopoietic cell transplantation (allo-HCT) in non-Hodgkin lymphoma (NHL) patients ≥65 years in the United States is limited by lack of Medicare coverage for this indication. Using the Center for International Blood and Marrow Transplant Research (CIBMTR) database, we report allo-HCT outcomes of NHL patients aged ≥65 years (older cohort; n = 446) compared with a cohort of younger NHL patients aged 55-64 years (n = 1183). We identified 1629 NHL patients undergoing a first reduced-intensity conditioning (RIC) or nonmyeloablative conditioning allo-HCT from 2008 to 2015 in the United States. Cord blood or haploidentical transplants were excluded. The median age was 68 years (range 65-77) for the older cohort vs 60 years (range 55-64) in the younger cohort. The 4-year adjusted probabilities of nonrelapse mortality (NRM), relapse/progression (R/P), progression-free survival (PFS), and overall survival (OS) of the younger and older groups were 24% vs 30% (P = .03), 41% vs 42% (P = .82), 37% vs 31% (P = .03), and 51% vs 46% (P = .07), respectively. Using multivariate analysis, compared with the younger group, the older cohort was associated with increased NRM, but there was no difference between the 2 cohorts in terms of R/P, PFS, or OS. The most common cause of death was disease relapse in both groups. In NHL patients eligible for allo-HCT, there was no difference in OS between the 2 cohorts. Age alone should not determine allo-HCT eligibility in NHL, and Medicare should expand allo-HCT coverage to older adults.
Visual Abstract
Introduction
Allogeneic hematopoietic cell transplantation (allo-HCT) is a potentially curative option for patients with advanced high-risk hematological malignancies. Despite its established effectiveness, wider application of this procedure has been historically limited to younger patients with few medical comorbidities. However, in the last 2 decades, the advent and adoption of reduced-intensity conditioning (RIC) or nonmyeloablative (NMA) regimens has led to an increase in the number of allo-HCT procedures performed in the United States, including increased utilization of this modality for older patients or those with limiting medical comorbidities.1,2
The feasibility of allo-HCT with lower-intensity regimens is well established in select older (age ≥65 years) patients. In a large retrospective analysis of 372 patients aged 60-75 years (age ≥65 years, n = 134) with various hematological malignancies undergoing NMA allo-HCT, survival was not impacted by increasing patient age, but rather by the presence of medical comorbidities, underscoring the importance of assessing physiological age over an arbitrary chronological age cutoff when determining allo-HCT eligibility.2 However, patients aged ≥65 years with certain hematological malignancies (myelodysplastic syndrome [MDS], myeloma, myelofibrosis, or non-Hodgkin lymphoma [NHL]) with Medicare as primary insurance in the United States, historically did not have coverage for allo-HCT, leading to disparities in access between those with private versus Medicare insurance. The Centers for Medicare and Medicaid services (CMS) in the United States, as part of the national coverage determination, may provide coverage of an item or service (eg, a particular allo-HCT indication) only in the context of a clinical study (ie, via the coverage with evidence development [CED] mechanism). On 4 August 2010, using its CED mechanism, CMS established coverage for allo-HCT for Medicare beneficiaries with MDS in an ongoing Center for International Blood and Marrow Transplant Research (CIBMTR) observational study comparing the outcomes of patients aged 55-64 years vs those ≥65 years.3 Since that time, other allo-HCT indications (myeloma, myelofibrosis, and sickle cell disease) have also acquired CMS coverage, again only if performed within the context of approved ongoing CIBMTR protocols.4
Unfortunately, allo-HCT is still not covered for NHL patients in the United States according to current CMS guidelines,4 despite the fact that the median age at diagnosis of NHL is 67 years in the United States.5 This, combined with the fact that most patients aged ≥65 years in the United States receive their primary insurance coverage through Medicare (and most private insurance providers follow CMS guidelines), means that the vast majority of NHL patients lack access to this potentially curative treatment modality. Although there is ample evidence that allo-HCT can provide long-term disease control in select NHL patients in the frontline or relapsed setting,6-13 most of these studies included only a small subset of patients over the age of 65 years. For example, in the study by Sorror et al,2 with 372 older patients, only ∼25 patients aged 65-75 years had lymphoma or myeloma. We report here a registry analysis evaluating outcomes of US NHL patients aged ≥65 years undergoing a RIC allo-HCT compared with a younger cohort aged 55-64 years to determine whether the arbitrary age cutoff is justifiable for those in need of this potentially lifesaving procedure (younger cohort age cutoff being identical to the control population age in the ongoing CMS CED study for MDS).3
Methods
Data sources
Data for this study were acquired from the CIBMTR registry (see supplemental Section 1 for details).
Patients
Included in this analysis are adult (≥55 years) patients with mature B-, T-, or NK-cell NHL who underwent a first RIC or NMA conditioning allo-HCT from matched related donors (MRDs), matched unrelated donors (MUDs), or mismatched unrelated donors (mmURDs) from 2008 to 2015. Bone marrow and peripheral blood grafts were included. Patients receiving haploidentical or cord blood transplants were excluded. The analysis was limited to US transplant centers for generating data in a patient population relevant to CMS coverage area.
Definition and study end points
The intensity of conditioning regimens was defined using consensus criteria.14 Response to last line of therapy before allo-HCT on CIBMTR forms is defined using established criteria.15
The primary end point was overall survival (OS); death from any cause was considered an event, and surviving patients were censored at last contact. Nonrelapse mortality (NRM) was defined as death without evidence of lymphoma progression/relapse; relapse was considered a competing risk. Progression/relapse was defined as progressive lymphoma after hematopoietic cell transplantation (HCT) or lymphoma recurrence after a complete remission; NRM was considered a competing event. For progression-free survival (PFS), a patient was considered a treatment failure at the time of progression/relapse or death from any cause. Patients alive without evidence of disease relapse or progression were censored at last follow-up. Acute graft-versus-host disease (GVHD)16 and chronic GVHD17 were graded using standard criteria.
Statistical analysis
Clinical outcomes of the cohort aged ≥65 years were compared against the cohort aged 55-64 years. Adjusted probabilities of PFS and OS were calculated as described previously.18 Adjusted cumulative incidence of NRM and lymphoma progression/relapse was calculated to accommodate for competing risks.19 Unadjusted cumulative incidence of acute/chronic GVHD was calculated. Associations among patient-, disease-, and transplantation-related variables and outcomes of interest were evaluated using Cox proportional hazards regression. A stepwise model-building approach was used to identify covariates that influenced outcomes. Covariates with a P < .05 were considered statistically significant. The proportional hazards assumption for Cox regression was tested by adding a time-dependent covariate for each risk factor and each outcome. Covariates that violated the proportional hazards assumption were added as time-dependent covariates, where the best cutoff for each time-dependent covariate was determined using the maximum likelihood method. Interactions between the main effect and significant covariates were examined (in particular disease histology, GVHD prophylaxis regimen, and remission status at HCT); none were found. Results are expressed as relative risks (RRs). The variables considered in multivariate analysis are shown in supplemental Table 1. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Baseline characteristics
Using the CIBMTR database, we identified 1629 NHL patients (≥65 years, n = 446; 55-64 years, n = 1183) undergoing a first RIC or NMA conditioning allo-HCT from 2008 to 2015 in the United States (Figure 1). The baseline patient-, disease-, and transplantation-related characteristics are detailed in Table 1. The median patient age was 68 years (range 65-77 years) for the older cohort vs 60 years (range 55-64 years) for the younger cohort. There were no significant differences between the 2 cohorts in terms of patient gender, race, Karnofsky performance score (KPS), HCT comorbidity index (HCT-CI), disease status prior to transplant, time from diagnosis to transplant, GVHD prophylaxis used, in vivo T-cell depletion, or type of conditioning regimen(s) used. A higher proportion of patients had undergone a prior autologous HCT in the younger cohort compared with the older cohort (38% vs 31%, P = .01). Significantly more patients in the younger cohort underwent an MRD allo-HCT (46% vs 35%, P < .001). The median follow-up of survivors was 48 months (range 6-98) and 48 months (range 4-101) in the older and younger cohorts, respectively.
Figure 1.

Consort diagram.
Table 1.
Baseline patient characteristics of NHL patients aged 55-64 years vs ≥65 years reported to CIBMTR from 2008 to 2015
| Variable | 55-64 years (n = 1183) | ≥65 years (n = 446) | P |
|---|---|---|---|
| Age at HCT, median (range), y | 60 (55-64) | 68 (65-77) | <0.001 |
| Male sex, n (%) | 773 (65) | 303 (68) | 0.32 |
| White, n (%) | 1099 (93) | 421 (94) | 0.28 |
| KPS ≥90, n (%) | 720 (61) | 257 (58) | 0.26 |
| HCT-CI, n (%) | 0.41 | ||
| 0 | 361 (31) | 135 (30) | |
| 1-2 | 367 (31) | 122 (27) | |
| ≥3 | 443 (37) | 185 (42) | |
| Missing | 12 (1) | 4 (<1) | |
| Histology, n (%) | 0.02 | ||
| Follicular lymphoma | 273 (23) | 82 (18) | |
| Diffuse large B-cell lymphoma | 363 (31) | 129 (29) | |
| Mantle cell lymphoma | 257 (22) | 131 (29) | |
| Mature T/NK-cell lymphoma | 237 (20) | 87 (20) | |
| Others | 53 (4) | 17 (4) | |
| Interval from diagnosis to HCT, median (range), mo | 33 (1-386) | 37 (2-322) | 0.59 |
| Disease status prior to HCT, n (%) | 0.68 | ||
| Sensitive | 993 (84) | 384 (86) | |
| Resistant | 179 (15) | 59 (13) | |
| Untreated/unknown | 11 (<1) | 3 (<1) | |
| Prior autologous HCT, n (%) | 451 (38) | 140 (31) | 0.01 |
| Year of HCT, n (%) | 0.18 | ||
| 2008-2010 | 416 (35) | 137 (31) | |
| 2011-2013 | 502 (43) | 195 (44) | |
| 2014-2015 | 265 (22) | 114 (25) | |
| Conditioning regimens, n (%) | 0.35 | ||
| Flu/Bu ± others | 323 (27) | 124 (28) | |
| Flu/CY ± others | 162 (14) | 55 (12) | |
| Flu/CY/TBI ± others | 64 (5) | 30 (7) | |
| Flu/Mel ± others | 311 (26) | 109 (24) | |
| TBI ± others | 41 (3) | 9 (2) | |
| TBI/Flu | 148 (13) | 53 (12) | |
| TLI/ATG | 67 (6) | 36 (8) | |
| Others* | 67 (6) | 30 (7) | |
| ATG/alemtuzumab in conditioning | 323 (27) | 130 (29) | 0.12 |
| Graft source, n (%) | 0.003 | ||
| Bone marrow | 54 (5) | 37 (8) | |
| Peripheral blood | 1129 (95) | 409 (92) | |
| Donor type, n (%) | <0.001 | ||
| MRD | 546 (46) | 156 (35) | |
| MUD | 508 (43) | 241 (54) | |
| mmURD | 129 (11) | 49 (11) | |
| Donor–recipient sex match, n (%) | 0.08 | ||
| Male–male | 502 (42) | 216 (48) | |
| Others | 674 (57) | 226 (51) | |
| Missing | 7 (<1) | 4 (<1) | |
| Donor–recipient CMV status, n (%) | 0.66 | ||
| D−/R+ | 270 (23) | 122 (27) | |
| Others | 744 (63) | 266 (60) | |
| Missing | 169 (14) | 58 (13) | |
| GVHD prophylaxis, n (%) | 0.21 | ||
| CNI + MTX + other(s) except MMF, post-Cy | 572 (48) | 201 (45) | |
| CNI + MMF + other(s) except post-Cy | 403 (34) | 149 (33) | |
| CNI + other(s) except MMF, MTX, post-Cy | 134 (11) | 56 (13) | |
| Others† | 68 (6) | 33 (7) | |
| Missing | 6 (<1) | 7 (2) | |
| Follow-up of survivors, median (range), mo | 48 (4-101) | 48 (6-98) |
ATG, antithymocyte globulin; Bu, busulfan; CMV, cytomegalovirus; CNI, calcineurin inhibitors; Cy, cyclophosphamide; D, donor; Flu, fludarabine; Mel, melphalan; MMF, mycophenolate mofetil; MTX, methotrexate; R, recipient; TBI, total body irradiation; TLI, total lymphoid irradiation.
16 beam-like; 56 Flu ± other(s); 25 Mel ± other(s).
43 CNI alone; 58 post-Cy ± other(s).
Acute and chronic GVHD
The cumulative incidence of grades II-IV acute GVHD at day 180 post–allo-HCT was 38% (95% confidence interval [CI], 35-41) in the younger cohort vs 35% (95% CI, 31-40) in the older cohort (P = .39) (Table 2). The cumulative incidence of grades III-IV acute GVHD at day 180 post–allo-HCT was 15% (95% CI, 13-17) vs 17% (95% CI, 14-21), respectively (P = .21). The cumulative incidence of chronic GVHD at 2 years posttransplant in patients aged 55-64 years was 48% (95% CI, 45-51) compared with 45% (95% CI, 40-49) in patients aged ≥65 years (P = .25) (Table 2).
Table 2.
Probabilities at fixed time points
| Outcomes | 55-64 years (N = 1183) | ≥65 years (N = 446) | P | ||
|---|---|---|---|---|---|
| n | Probability, % (95% CI) | n | Probability, % (95% CI) | ||
| Acute GVHD (II-IV), 180 d | 1108 | 38 (35-41) | 425 | 35 (31-40) | 0.39 |
| Acute GVHD (III-IV), 180 d | 1108 | 15 (13-17) | 426 | 17 (14-21) | 0.21 |
| Chronic GVHD, y | 1145 | 438 | |||
| 1 | 40 (37-43) | 35 (31-40) | 0.06 | ||
| 2 | 48 (45-51) | 45 (40-49) | 0.25 | ||
| NRM | 1183 | 446 | |||
| 100 d | 7 (5-8) | 7 (5-10) | 0.69 | ||
| 1 y | 15 (13-17) | 18 (15-22) | 0.14 | ||
| 4 y | 24 (21-27) | 30 (25-35) | 0.03 | ||
| Relapse/progression, y | 1183 | 446 | |||
| 1 | 30 (27-32) | 29 (24-33) | 0.70 | ||
| 4 | 41 (38-44) | 42 (37-47) | 0.82 | ||
| PFS, y | 1183 | 446 | |||
| 1 | 55 (52-58) | 53 (49-59) | 0.51 | ||
| 4 | 37 (34-40) | 31 (26-35) | 0.03 | ||
| OS, y | 1183 | 446 | |||
| 1 | 69 (67-72) | 67 (62-71) | 0.31 | ||
| 4 | 51 (48-54) | 46 (41-51) | 0.07 | ||
NRM and relapse
The adjusted cumulative incidence of NRM at day 100 was 7% in both groups (P = .69) (Table 2). At 1-year posttransplant, the cumulative incidence of NRM was 15% (95% CI, 13-17) for the younger cohort vs 18% (95% CI, 15-22) for the older cohort (P = .14). Using multivariate analysis, compared with the younger cohort, patient age ≥65 years was associated with a significantly higher risk for NRM (RR, 1.29; 95% CI, 1.04-1.61, P = .02; Table 3; Figure 2A). Independent of patient age, KPS <90 (RR, 1.52; 95% CI, 1.24-1.88; P < .0001), HCT-CI ≥3 (RR, 1.63; 95% CI, 1.27-2.10; P = .0001), and allo-HCT from MUDs and mmURDs (with or without in vivo T-cell depletion) were associated with a higher risk for NRM (supplemental Table 2).
Table 3.
Multivariable analysis results
| n | RR | 95% CI | P | |
|---|---|---|---|---|
| NRM, y | ||||
| 55-64 | 1166 | 1 | 0.02 | |
| ≥65 | 436 | 1.29 | 1.04-1.61 | |
| Progression/relapse, y | ||||
| 55-64 | 1166 | 1 | 0.80 | |
| ≥65 | 436 | 1.02 | 0.86-1.22 | |
| PFS, y | ||||
| 55-64 | 1166 | 1 | 0.14 | |
| ≥65 | 436 | 1.11 | 0.97-1.27 | |
| OS, y | ||||
| 55-64 | 1166 | 1 | 0.10 | |
| ≥65 | 436 | 1.14 | 0.97-1.33 |
Detailed results of multivariate analysis are provided in supplemental Table 2.
Figure 2.

Adjusted NRM and relapse/progression for allo-HCT in younger and older patients with NHL. (A) NRM; (B) relapse.
The adjusted cumulative incidence of disease progression/relapse at 4 years was 41% (95% CI, 38-44) in the younger group vs 42% (95% CI, 37-47) in the older group and was not significantly different (P = .82) (Table 2). Using multivariate analysis, compared with the younger cohort, patient age ≥65 years was not associated with a significantly increased risk for disease progression/relapse (RR, 1.02; 95% CI, 0.86-1.22; P = .80; Table 3; Figure 2B). Other independent variables associated with risk for disease progression/relapse are provided in supplemental Table 2.
PFS and OS
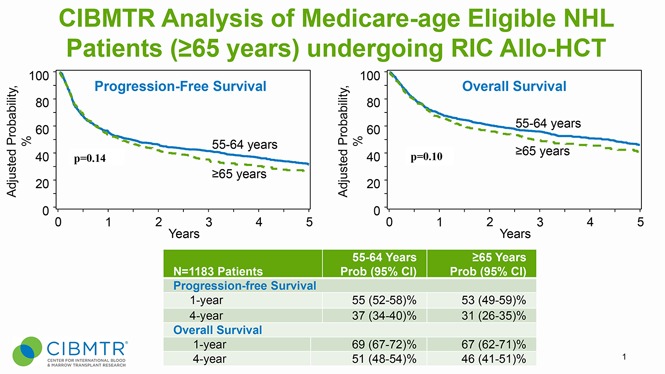
The adjusted 4-year PFS for the younger group was 37% (95% CI, 34-40) vs 31% (95% CI, 26-35) in the older group (P = .03) (Table 2; Figure 3A). Using multivariate analysis, compared with the younger cohort, patient age ≥65 years was not associated with a significantly inferior PFS (RR, 1.11; 95% CI, 0.97-1.27; P = .14). Other independent variables associated with the risk for therapy failure (inverse of PFS) are provided in supplemental Table 2. The adjusted 4-year OS for the younger cohort (51%; 95% CI, 48-54) was not significantly different from the older cohort (46%; 95% CI, 41-51; P = .07; Table 2; Figure 3B). Using multivariate analysis, compared with the younger cohort, patient age ≥65 years was not associated with a significantly increased risk for mortality (RR, 1.14; 95% CI, 0.97-1.33; P = .10) (Table 3). Independent of patient age, KPS <90 (RR, 1.34; 95% CI, 1.15-1.56; P = .0001), HCT-CI ≥3 (RR, 1.30; 95% CI, 1.09-1.55; P = .003), refractory disease (RR, 1.43; 95% CI, 1.19-1.73; P = .0002), histology other than follicular lymphoma and transplantation from an mmURD while using in vivo T-cell depletion (RR, 1.79; 95% CI, 1.29-2.48; P = .0005) were associated with an increased risk for mortality (supplemental Table 2).
Figure 3.

PFS and OS for allo-HCT in younger and older patients with NHL. (A) PFS; (B) OS.
Subgroup analysis of patients ≥70 years
We performed a subset analysis to evaluate outcomes of patients who were ≥70 years old at the time of allo-HCT (n = 73). Among this patient population, the cumulative incidence of NRM at 1 year was 22% (95% CI, 13-32), whereas the cumulative incidence of progression/relapse at 4 years was 43% (95% CI, 32-54). The 4-year PFS and OS were 27% (95% CI, 17-38) and 44% (95% CI, 32-56), respectively.
Cause of death
At last follow-up, there have been 550 (46%) deaths in the 55-64–year cohort and 232 (52%) deaths in the ≥65-year cohort. The most common cause of death in both groups was relapse of the primary disease (n = 212 and n = 79, respectively) (supplemental Table 3). The next most common cause of death in the 55-64–year cohort was GVHD (n = 86), followed by infection (n = 39). In contrast, infection was the second most common cause of death in the ≥65-year group (n = 39), followed by GVHD (n = 32).
Discussion
There is growing awareness that age, by itself, is an insufficient and often inaccurate determinant of medical fitness for any specific treatment. In this study, we report allo-HCT outcomes for a large cohort of (potentially) Medicare-eligible patients aged ≥65 years relative to a younger, generally Medicare-noneligible group. Currently, coverage for allo-HCT in NHL in the United States is limited to only those states that are in the National Government Services (NGS) jurisdiction. NGS is a Medicare Administrative Contractor that makes claims on behalf of CMS. It is plausible that a small subset included in our study could have undergone HCT using non-Medicare payers (eg, private insurance, self-pay). However, because NHL is not a covered CMS indication for allo-HCT, and the majority of states are not under NGS jurisdiction, there is significant disparity in the access to allo-HCT in NHL in the United States.
Through this registry analysis we found no significant difference in OS between the 2 cohorts, with 46% of patients aged ≥65 years still alive at 4 years posttransplantation. Secondly, although there was a modest, but statistically significant, risk for increased NRM in the older cohort, this finding did not translate into significant differences in PFS or OS in multivariate analysis. Additionally, NRM was identical at 100 days posttransplant, and it was only beyond 1 year posttransplant that the increase in NRM becomes appreciable. Because the patients in the older cohort were, on average, almost a decade older, the difference in NRM at 4 years may be partially attributed to expected age-related mortality. Lastly, there was no difference in acute or chronic GVHD, and relapse rates were similar between the 2 groups, suggesting that the efficacy of transplantation (and possibly graft-versus-lymphoma effect) is comparable, despite differences in age.
We acknowledge that allo-HCT is not the only therapeutic option available to older patients with relapsed/refractory or high-risk NHL. The intent of our analysis is not to prove superiority of allo-HCT in older NHL patients relative to other available tools (eg, novel agents, autologous HCT, gene-modified T-cell therapies). Rather, we aim to demonstrate that, in any given NHL patient ≥65 years old, if after consideration of multiple variables the treating physician has decided that allo-HCT is the next best therapy, an arbitrary age cutoff and lack of third-party (eg, CMS) reimbursement should not remain a barrier against transplantation. Our study utilizing a large contemporary dataset suggests that survival outcomes of such Medicare-age eligible patients are not dramatically inferior to a decade-younger patient cohort undergoing similar allo-HCT procedures.
Although other series have also evaluated the efficacy and toxicity of allo-HCT in older adults, the number of patients has been much smaller, and ours is the first to focus singularly on allo-HCT outcomes of NHL patients aged ≥65 years. In a prior CIBMTR analysis of NHL patients aged ≥40 years who underwent allo-HCT between 2001 and 2007, the 3-year OS ranged from 39% to 54%, stratified by age.11 However, among the 1248 NHL patients included in that CIBMTR analysis, only 82 patients were 65 years or older. Recently, CIBMTR reported outcomes of patients aged ≥70 years undergoing allo-HCT for various hematologic malignancies between 2000 and 2013 and showed improving patient outcomes in more recent years (2008-2013). The 2-year OS of the study population transplanted from 2008 to 2013 was 39%, but outcomes of NHL patients (∼10% of study population) were not reported separately. Among 73 NHL patients aged ≥70 years in our report who underwent allo-HCT, the 4-year OS was 44%, which is encouraging considering the aforementioned data. With the development of effective in vivo and ex vivo T-cell depletion approaches (eg, posttransplant cyclophosphamide or TCR-α/β and CD19 depletion), the utilization of adult alternative donors is rapidly increasing.20 The CIBMTR12,21 and the European Society for Blood and Marrow Transplantation22,23 have recently reported that outcomes of lymphoma patients undergoing haploidentical transplantation are comparable to MRD and MUD allo-HCT. A report from Johns Hopkins University suggests the feasibility of NMA haploidentical transplantation in older adults (50-75 years, median age 61 years) with hematological malignancies.24 An ongoing CIBMTR study evaluating the role of haploidentical HCT in older patients will further elucidate its role.
It is important to acknowledge that allo-HCT is applicable only to the subset of healthy older individuals with few or no serious medical comorbidities. The importance of appropriate patient selection for allo-HCT cannot be overemphasized. To help with decision making in an older population, objective tools, such as HCT-CI,25 can be useful in making determinations for allo-HCT candidacy. Our study found, similar to other reports,26 that an HCT-CT ≥ 3 negatively impacts OS and PFS. Furthermore, there are evolving data suggesting that comprehensive performance assessment tools may have value when evaluating an older patient for allo-HCT. Muffly et al demonstrated that a comprehensive geriatric assessment has independent prognostic utility in evaluating older patient candidacy for allo-HCT.27 The effectiveness of such tools will be validated in an upcoming Blood and Marrow Transplantation Clinical Trials Network study that intends to incorporate geriatric assessments as part of the prospective clinical trial. Lastly, disease subtype may play a role in decision making for allo-HCT in NHL. Although we included multiple histologies, our multivariate analysis found that patients with nonindolent subtypes (eg, diffuse large B-cell lymphoma, mantle cell lymphoma, or NK/T cell lymphoma) had a higher risk for relapse and worse PFS and OS (supplemental Table 2).
There are several limitations to this analysis. As a registry study, our analysis is limited to the information available in the database. Although we aimed to adjust for possible confounders with our multivariate analysis, unmeasured variables could influence our findings. Although the benefit of allo-HCT in elderly NHL patients (relative to other treatment options) can only be established via prospective randomized studies, these are logistically challenging and unlikely to be performed. Another limitation is the inherent bias in only evaluating transplanted patients. Patients who are eligible to undergo allo-HCT represent a select population that is healthy enough with responding disease to be candidates for transplant; as a result, our findings are not applicable to all elderly patients with NHL. Because we did not include cord or haploidentical donors, our results are not applicable to those groups. Lastly, there were differences in the use of autologous transplant prior to allo-HCT between the 2 groups. Although it is difficult to elucidate the etiology of this difference in a registry study, we speculate that this may be due to poorer mobilization in older adults and/or center practices to avoid high-dose chemotherapy in patients aged ≥65 years.
In conclusion, for NHL patients who are eligible for allo-HCT, there was no difference in OS for patients aged 55-64 years compared with patients aged ≥65 years. These data strongly support that age alone should not be a determinant for allo-HCT eligibility in NHL. The role and relative benefit of allo-HCT in NHL will undoubtedly evolve in the coming years with the advent of new cellular and targeted therapies; however, for now, allo-HCT represents an opportunity for cure in patients without other options and should be available to all suitable candidates regardless of age and insurance coverage. We hope that the data from this study will provide the direct evidence needed to justify modification of the current Medicare national coverage determination to allow for allo-HCT in NHL.
Supplementary Material
The full-text version of this article contains a data supplement.
Acknowledgments
The authors thank Morgan Geronime for administrative support.
This work was supported by the CIBMTR. The CIBMTR is supported by Public Health Service Grant/Cooperative Agreement U24-CA076518 from the National Institutes of Health, National Cancer Institute, National Heart, Lung and Blood Institute, and National Institute of Allergy and Infectious Diseases; Grant/Cooperative Agreement 5U10HL069294 from the National Institutes of Health, National Heart, Lung and Blood Institute and National Cancer Institute; Contract HHSH250201200016C with the Health Resources and Services Administration (Department of Health and Human Services); Grants N00014-13-1-0039 and N00014-14-1-0028 from the Office of Naval Research; and grants from *Actinium Pharmaceuticals, Allos Therapeutics, Inc., *Amgen, Inc., anonymous donation to the Medical College of Wisconsin, Ariad, Be the Match Foundation, *Blue Cross and Blue Shield Association, *Celgene Corporation, Chimerix, Inc., Fred Hutchinson Cancer Research Center, Fresenius-Biotech North America, Inc., *Gamida Cell Teva Joint Venture Ltd., Genentech, Inc.,*Gentium SpA, Genzyme Corporation, GlaxoSmithKline, Health Research, Inc., Roswell Park Cancer Institute, Histogenetics, Inc., Incyte Corporation, Jeff Gordon Children’s Foundation, Kiadis Pharma, The Leukemia & Lymphoma Society, Medac GmbH, The Medical College of Wisconsin, Merck & Co, Inc., Millennium: The Takeda Oncology Co., *Milliman USA, Inc., *Miltenyi Biotec, Inc., National Marrow Donor Program, Onyx Pharmaceuticals, Optum Healthcare Solutions, Inc., Osiris Therapeutics, Inc., Otsuka America Pharmaceutical, Inc., PerkinElmer, Inc., *Remedy Informatics, *Sanofi US, Seattle Genetics, Sigma-Tau Pharmaceuticals, Soligenix, Inc., St. Baldrick’s Foundation, StemCyte, A Global Cord Blood Therapeutics Co., STEMSOFT Software, Inc., Swedish Orphan Biovitrum, *Tarix Pharmaceuticals, *Terumo BCT, *Teva Neuroscience, Inc., *Therakos, Inc., University of Minnesota, University of Utah, and *Wellpoint, Inc. (*corporate members).
The views expressed in this article do not reflect the official policy or position of the National Institutes of Health, the Department of the Navy, the Department of Defense, the Health Resources and Services Administration, or any other agency of the US Government.
Authorship
Contribution: N.N.S. and M.H. conceived and designed the project and wrote the manuscript; C.L. and M.H. collected and assembled data; K.W.A., C.L., and M.H. analyzed the data; and all authors interpreted the data, helped to revise the manuscript, and approved the final version.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Mehdi Hamadani, Center for International Blood and Marrow Transplant Research, Medical College of Wisconsin, 9200 W. Wisconsin Ave, Suite C5500, Milwaukee, WI 53226; e-mail: mhamadani@mcw.edu.
References
- 1.D’Souza A, Lee S, Zhu X, Pasquini M. Current use and trends in hematopoietic cell transplantation in the United States. Biol Blood Marrow Transplant. 2017;23(9):1417-1421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sorror ML, Sandmaier BM, Storer BE, et al. Long-term outcomes among older patients following nonmyeloablative conditioning and allogeneic hematopoietic cell transplantation for advanced hematologic malignancies. JAMA. 2011;306(17):1874-1883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Atallah E, Horowitz MM, Logan B, et al. Outcome of patients 65 years and older with myelodysplastic syndrome (MDS) receiving allogeneic hematopoietic stem cell transplantation compared to patients 55-64 years of age. Blood. 2015;126:193. [Google Scholar]
- 4.National Coverage Determination (NCD) for Stem Cell Transplantation. (Formerly 110.8.1) (110.23), Centers of Medicare and Medicaid Services. Available at: https://www.cms.gov/Medicare/Coverage/Coverage-with-Evidence-Development/. Accessed 20 January 2018.
- 5.SEER Cancer Statistics Review (CSR), 1975-2014. National Cancer Institute Surveillance, Epidemiology, and End Results Program. Available at: http://seer.cancer.gov/csr/1975_2014/. Accessed 18 December 2017.
- 6.Fenske TS, Ahn KW, Graff TM, et al. Allogeneic transplantation provides durable remission in a subset of DLBCL patients relapsing after autologous transplantation. Br J Haematol. 2016;174(2):235-248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Smith SM, Burns LJ, van Besien K, et al. Hematopoietic cell transplantation for systemic mature T-cell non-Hodgkin lymphoma. J Clin Oncol. 2013;31(25):3100-3109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dreger P, Döhner H, Ritgen M, et al. ; German CLL Study Group. Allogeneic stem cell transplantation provides durable disease control in poor-risk chronic lymphocytic leukemia: long-term clinical and MRD results of the German CLL Study Group CLL3X trial. Blood. 2010;116(14):2438-2447. [DOI] [PubMed] [Google Scholar]
- 9.Hamadani M, Saber W, Ahn KW, et al. Allogeneic hematopoietic cell transplantation for chemotherapy-unresponsive mantle cell lymphoma: a cohort analysis from the Center for International Blood and Marrow Transplant Research. Biol Blood Marrow Transplant. 2013;19(4):625-631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Robinson SP, Boumendil A, Finel H, et al. Reduced intensity allogeneic stem cell transplantation for follicular lymphoma relapsing after an autologous transplant achieves durable long term disease control. An analysis from the Lymphoma Working Party of the EBMT. Ann Oncol. 2016;27(6):1088-1094. [DOI] [PubMed] [Google Scholar]
- 11.McClune BL, Ahn KW, Wang HL, et al. Allotransplantation for patients age ≥40 years with non-Hodgkin lymphoma: encouraging progression-free survival. Biol Blood Marrow Transplant. 2014;20(7):960-968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kanate AS, Mussetti A, Kharfan-Dabaja MA, et al. Reduced-intensity transplantation for lymphomas using haploidentical related donors vs HLA-matched unrelated donors. Blood. 2016;127(7):938-947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Klyuchnikov E, Bacher U, Kröger NM, et al. Reduced-intensity allografting as first transplantation approach in relapsed/refractory grades one and two follicular lymphoma provides improved outcomes in long-term survivors. Biol Blood Marrow Transplant. 2015;21(12):2091-2099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bacigalupo A, Ballen K, Rizzo D, et al. Defining the intensity of conditioning regimens: working definitions. Biol Blood Marrow Transplant. 2009;15(12):1628-1633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cheson BD, Pfistner B, Juweid ME, et al. ; International Harmonization Project on Lymphoma. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25(5):579-586. [DOI] [PubMed] [Google Scholar]
- 16.Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995;15(6):825-828. [PubMed] [Google Scholar]
- 17.Shulman HM, Sullivan KM, Weiden PL, et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med. 1980;69(2):204-217. [DOI] [PubMed] [Google Scholar]
- 18.Zhang X, Loberiza FR, Klein JP, Zhang MJ. A SAS macro for estimation of direct adjusted survival curves based on a stratified Cox regression model. Comput Methods Programs Biomed. 2007;88(2):95-101. [DOI] [PubMed] [Google Scholar]
- 19.Zhang X, Zhang MJ. SAS macros for estimation of direct adjusted cumulative incidence curves under proportional subdistribution hazards models. Comput Methods Programs Biomed. 2011;101(1):87-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Passweg JR, Baldomero H, Bader P, et al. Use of haploidentical stem cell transplantation continues to increase: the 2015 European Society for Blood and Marrow Transplant activity survey report. Bone Marrow Transplant. 2017;52(6):811-817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ghosh N, Karmali R, Rocha V, et al. Reduced-intensity transplantation for lymphomas using haploidentical related donors versus HLA-matched sibling donors: a Center for International Blood and Marrow Transplant Research analysis. J Clin Oncol. 2016;34(26):3141-3149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Martínez C, Gayoso J, Canals C, et al. ; Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. Post-transplantation cyclophosphamide-based haploidentical transplantation as alternative to matched sibling or unrelated donor transplantation for Hodgkin lymphoma: a registry study of the Lymphoma Working Party of the European Society for Blood and Marrow Transplantation. J Clin Oncol. 2017;35(30):3425-3432. [DOI] [PubMed] [Google Scholar]
- 23.Dietrich S, Finel H, Martinez C, et al. Post-transplant cyclophosphamide-based haplo-identical transplantation as alternative to matched sibling or unrelated donor transplantation for non-Hodgkin lymphoma: a registry study by the European Society for Blood and Marrow Transplantation. Leukemia. 2016;30(10):2086-2089. [DOI] [PubMed] [Google Scholar]
- 24.Kasamon YL, Bolaños-Meade J, Prince GT, et al. Outcomes of nonmyeloablative HLA-haploidentical blood or marrow transplantation with high-dose post-transplantation cyclophosphamide in older adults. J Clin Oncol. 2015;33(28):3152-3161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sorror ML, Maris MB, Storb R, et al. Hematopoietic cell transplantation (HCT)-specific comorbidity index: a new tool for risk assessment before allogeneic HCT. Blood. 2005;106(8):2912-2919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Muffly L, Pasquini MC, Martens M, et al. Increasing use of allogeneic hematopoietic cell transplantation in patients aged 70 years and older in the United States. Blood. 2017;130(9):1156-1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Muffly LS, Kocherginsky M, Stock W, et al. Geriatric assessment to predict survival in older allogeneic hematopoietic cell transplantation recipients. Haematologica. 2014;99(8):1373-1379. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.