

Abstract
OBJECTIVES
To describe the method of delivery, dosage regimens, and outcomes of sedatives and analgesics administered via the extravascular route for laceration repair in children
METHODS
Medline, Embase, and International Pharmaceutical Abstracts were searched using the keywords “child,” “midazolam,” “ketamine,” dexmedetomidine,” “fentanyl,” “nitrous oxide” (N2O), and “laceration repair.” Articles evaluating the use of extravascular sedation in children for laceration repair published in the English language between 1946 and June 2017 were included. Two authors independently screened each article for inclusion. Reports were excluded if they did not contain sufficient details on dosage regimen and outcomes.
RESULTS
A total of 16 reports representing 953 children receiving sedatives and analgesics via the extravascular route were included for analyses. A statistical analysis was not performed because of heterogeneity in dosing and types of analyses conducted. Midazolam and N2O were the most common agents, with oral (PO) midazolam being the most common agent. Other agents that have supporting data were intranasal (IN) dexmedetomidine, IN ketamine, IN midazolam, PO diazepam, PO ketamine, transmucosal (TM) midazolam, and TM fentanyl.
CONCLUSIONS
Most of the agents administered through the extravascular route were efficacious. Selection of the agents should be based on perceived need for analgesia versus sedation, patient accessibility, and adverse drug events. Future research is needed to determine the optimal agent and route for laceration repair.
Keywords: analgesia, child, dexmedetomidine, fentanyl, ketamine, midazolam, nitrous oxide, sedation
Introduction
Analgesia and sedation are essential for short, painful procedures like laceration repair. This procedure, although relatively short, can result in increased anxiety and stress for children. Adequate sedation prior to administration of local or topical anesthetics can facilitate more rapid repair and possibly better cosmetic outcomes. In 2016, the American Academy of Pediatrics and American Academy of Pediatric Dentistry published updated guidelines for sedation during diagnostic and therapeutic procedures.1 Their recommendations include maximization of patient safety, minimization of discomfort and pain, and controlling behavior and movement during the procedure. Although laceration repair could feasibly be completed with topical or local anesthetics, children may still need systemic analgesics and sedatives to ensure that they remain still and comfortable.
Intravenous (IV) analgesics and sedatives have been used to facilitate laceration repair. However, the insertion of an IV line is an additional noxious stimulus. According to the 2012 American Academy of Pediatrics Clinical Report on the Relief of Pain and Anxiety in Pediatric Patients in Emergency Medical Systems,2 analgesics and sedatives should be administered in a manner that is as painless as possible. Recent studies have focused on the use of sedatives and analgesics administered via extravascular routes, including oral (PO), inhaled, rectal, intranasal (IN), or transmucosal (TM) routes. This article reviews published reports describing the agent, route of administration, effective dose, onset time, and adverse drug events (ADEs) for medications administered via the extravascular route for laceration repair.
Literature Review
Relevant articles were identified using Medline (1946–June 2017), Embase (1980–June 2017), and International Pharmaceutical Abstracts (1970–June 2017), using the individual sedative agents (midazolam, ketamine, dexmedetomidine, fentanyl, nitrous oxide), laceration, and child as keywords. Results were limited to human studies written in the English language.
A 2-step selection process was conducted. The initial reports were screened by 2 reviewers (JLM and PNJ), and all authors determined final selection. To be included, the published report had to include children ages 18 years or younger receiving these selected medications via an extravascular route for laceration repair. Reports were excluded if they lacked sufficient details regarding the dosage regimen and outcomes. Statistical analysis was not performed, given the expected discrepancies in dosing and types of analyses (retrospective versus prospective design).
RESULTS
A total of 64 articles were identified using the search strategy. Three additional reports were identified within the references of screened papers. Overall, 51 articles were excluded because they included adult patients, were review articles, or did not contain a thorough description of the dosing regimens. A total of 16 studies including 953 patients receiving agents via the extra-vascular route were included. Tables 1 and 2 provide a summary of the type of report, dosing regimen, and main results.3–18
Table 1.
Summary of Studies Evaluating Benzodiazepine Agents for Laceration Repair
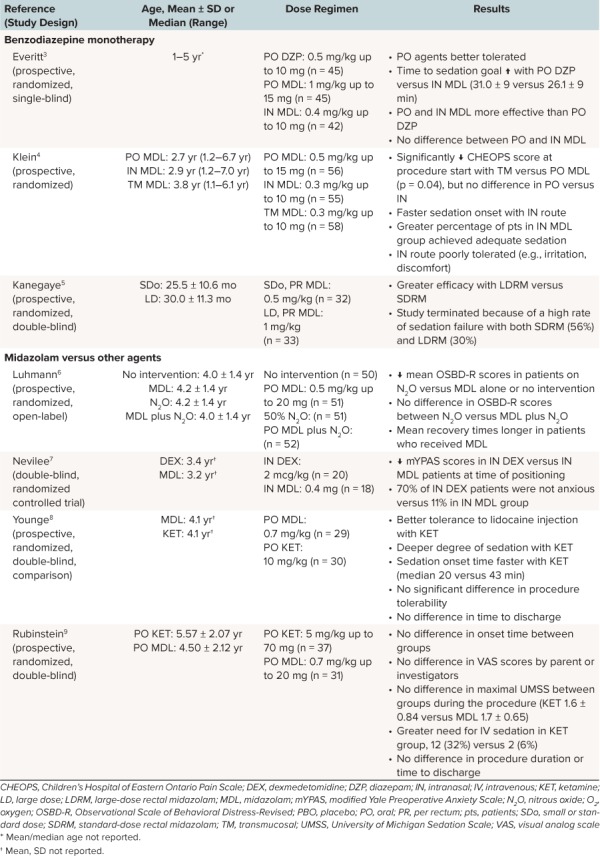
Table 2.
Summary of Studies Evaluating Non-Benzodiazepine Agents and Combination Therapies for Laceration Repair
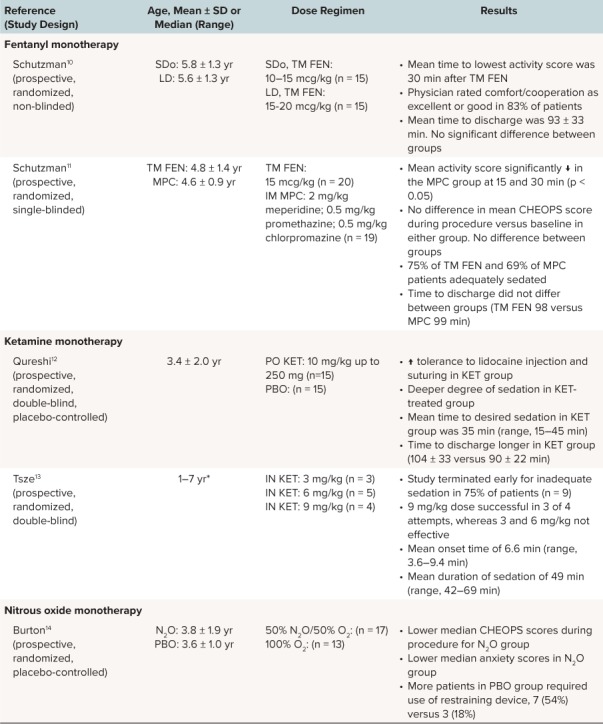
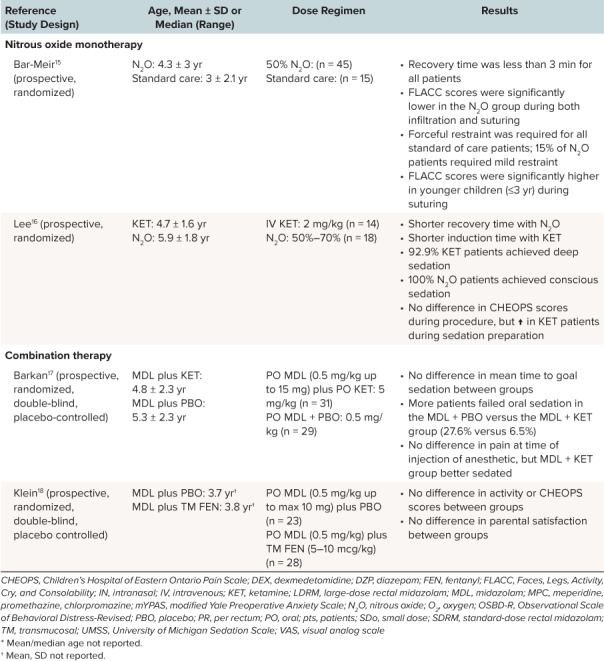
Table 2.
Summary of Studies Evaluating Non-Benzodiazepine Agents and Combination Therapies for Laceration Repair (cont.)
The focus of this review was to assess the efficacy and safety of sedatives and analgesics via an extravascular route for laceration repair. Patients in these studies may have received topical and/or local anesthetics in addition to these agents. Studies were categorized according to monotherapy or combination therapy. Monotherapy was defined as a single sedative or analgesic compared against placebo, another active agent, or a different dose or route of the same agent. Combination therapy was defined as the use of 2 or more sedative or analgesic agents versus a comparator group. To evaluate the efficacy of the agent, the specific scoring tools that evaluated sedation, analgesia, and/or anxiety used in each study were included.
Benzodiazepine Monotherapy. Midazolam was the most common agent used for sedation during laceration repair and is often considered the standard of care in comparison studies. Several routes of midazolam administration have been explored, including PO, IN, TM, and rectal routes. Everitt and Barnett3 compared the efficacy and safety of midazolam and diazepam in a prospective, single-blind study of preschool children undergoing laceration repair. Patients were randomized to receive diazepam 0.5 mg/kg PO, midazolam 1 mg/kg PO, or midazolam 0.4 mg/kg IN. The 5 mg/mL IV midazolam formulation was used for PO and IN administration; IN administration was accomplished by slow droplet instillation using a syringe. Tolerance of the route of administration and the child's distress during the procedure was assessed by nursing staff using a 100-mm visual analog scale (VAS). A 5-point anxiety scale was used, and the time needed to reach a score of 4 (drowsy, eyes closed but responding to minor stimulation) or 5 (asleep, eyes closed, able to be aroused but not responsive to minor stimulation) was recorded. Administration of PO medications was better tolerated than IN, as indicated by lower VAS scores for PO midazolam (30 ± 30) and diazepam (26 ± 25) versus IN midazolam (43 ± 31), p = 0.05 and p = 0.034, respectively. However, the mean time to sedation was significantly longer with PO diazepam compared with IN midazolam, 31.0 ± 9 versus 26.1 ± 9 minutes, p = 0.011; no statistical differences were noted in other comparisons. The onset time for PO midazolam was not reported. There were no differences in patient distress during suturing when comparing PO and IN midazolam; however, significantly more distress was noted with PO diazepam when compared to both PO and IN midazolam (p < 0.05). Following discharge, more children in the PO midazolam group reported drowsiness versus the PO diazepam group, 51.4% versus 32.2%, p = 0.032. In addition, 1 patient in the PO (2.2%) and 1 in the IN (2.4%) midazolam groups had a prolonged period of inconsolability after discharge. No other ADEs were described. The authors concluded that PO benzodiazepines were better tolerated than IN midazolam, but they noted that PO and IN midazolam were more effective than PO diazepam. Thus, PO midazolam appeared to be the best choice in terms of tolerability and efficacy.
Another study by Klein et al4 compared administration of midazolam by 3 different routes for sedation during laceration repair. Patients were randomized to 0.5 mg/kg PO, 0.3 mg/kg IN, or 0.3 mg/kg TM. A mucosal atomizer device (MAD) was used for administration of the IV midazolam solution for IN and TM administration. The child's distress was evaluated using the modified Children's Hospital of Eastern Ontario Pain Scale (CHEOPS), and level of sedation was evaluated using a 5-point activity score. The time needed to achieve a score of 3 (drowsy, readily responds) to 4 (awake, calm) was recorded. The primary outcome was the comparison of the first CHEOPS score after procedure initiation. Compared with PO, there was significantly less distress at procedure onset in the TM group (p = 0.04) and no difference in the IN group (p = 0.08). However, the IN midazolam had a faster median onset time (28 minutes) versus PO and TM (34 and 32 minutes, respectively). A greater number of patients (84.6%) achieved adequate sedation with IN midazolam compared with PO and TM midazolam, 66.7% and 59.6%, respectively. However, IN midazolam was determined to be less readily accepted by patients and caused more irritation, defined as cough, gag, or sore throat. Irritation was noted in 40% of patients receiving IN midazolam versus only 16% and 17% of patients receiving PO and TM midazolam, respectively. Adverse drug events were similar between groups. One patient (1.7%) in the PO midazolam group was deeply sedated and was placed on oxygen; however, the patient did not require further intervention. Other ADEs included postdischarge vomiting (PO [1.7%], IN [3.4%], and TM [1.7%]) and postdischarge nightmares (PO [1.7%] and IN [1.7%]). These authors concluded that IN midazolam was the most effective agent in terms of onset time and adequate sedation. However, children with nasal congestion or a laceration involving the nose may have delayed onset of activity or significant agitation, respectively, with IN midazolam, and thus PO or TM midazolam may be preferred.
Because of the observations that IN midazolam causes discomfort and that PO midazolam is susceptible to first-pass metabolism and has a longer onset time, Kanegaye et al5 compared 2 different dosage regimens of rectal midazolam for sedation during laceration repair. They used 2 dosage regimens: standard dose (0.5 mg/kg) versus large dose (1 mg/kg). The rectal formulations were compounded using the 1 and 5 mg/mL IV solutions to a total volume of 0.5 mL/kg per dose. This dose was delivered via a small feeding tube inserted rectally. Efficacy was assessed using a validated 5-point behavioral scale, the Sedation Scale (0 = agitated; 5 = asleep). The authors noted a high rate of sedation failure in the standard-dose and large-dose groups, 56% versus 30%. A higher incidence of postprocedure agitation was noted in the large-dose versus standard-dose group, 27% versus 6%, p = 0.04. No other ADEs were noted. Two patients had loss of drug during administration, which may have adversely contributed to the study findings. Based on the high failure rate, the study was stopped after the first interim analysis. The authors concluded that the large-dose regimen was more effective than the low-dose regimen but was more likely to cause postprocedure agitation.
Overall, benzodiazepine monotherapy had variable rates of efficacy. It is difficult to compare the results of the studies that evaluated both PO and IN midazolam because different doses were used in the 2 studies.3,4 Intranasal midazolam appears to be more effective for achieving goal sedation for laceration repair according to the data reported by Klein et al4; however, no differences in sedation scores between PO and IN midazolam groups were noted by Everitt and Barnett.3 Perhaps no difference was observed because these investigators dripped the medication into the nares, whereas Klein et al4 used a MAD. The limitation of IN midazolam is administration tolerability, as discussed in both studies that compared PO and IN administration.3,4 Transmucosal midazolam appears to be better tolerated and has a slightly faster onset time, but it does not appear to be as efficacious. Oral and TM midazolam may be better options in children with lacerations around their nose or nasal congestion. Rectal midazolam appears to be a last-line option if other routes are not available.
Midazolam Versus Other Agents. For laceration repair, PO midazolam has been compared to N2O, as well as in combination with N2O. Luhmann et al 6 randomized patients to no intervention, PO midazolam, N2O, and PO midazolam plus N2O. Midazolam 0.5 mg/kg PO was administered 20 minutes prior to suturing and 50% N2O was initiated right before wound preparation. The Observational Scale of Behavioral Distress-Revised was used to measure anxiety during the procedure. Patients who received N2O had less anxiety during lidocaine injection, cleaning, and suturing of the wound (p < 0.001). When comparing midazolam plus N2O versus N2O monotherapy, no advantage was noted for combination therapy. Mean recovery times were longer in patients who received midazolam monotherapy (30 minutes) and combination therapy (28 minutes) versus N2O monotherapy (21 minutes). All patients were hemodynamically stable during the procedure. The most common ADE with N2O therapy was vomiting during the emergency department visit (5.8%), and for midazolam was ataxia during the first 24 hours (25.2%). In addition, 11 patients (21.6%) in the PO midazolam and 4 patients (4.0%) in the N2O group had increased sleepiness in the first 24 hours following the procedure. Based on these data, the authors concluded that patients receiving N2O had less anxiety and a shorter recovery time versus PO midazolam. Further, they suggested that the combination of midazolam and N2O offered no clear advantage compared with N2O alone.
Midazolam Versus Dexmedetomidine. Neville et al7 conducted a double-blind randomized controlled trial comparing dexmedetomidine 2 mcg/kg IN versus midazolam 0.4 mg/kg IN for children requiring laceration repair. Midazolam and dexmedetomidine were prepared using IV solutions—5 mg/mL and 100 mcg/mL—respectively, and delivered via a MAD. The primary objective was comparison of the modified Yale Preoperative Anxiety Scale (mYPAS; range, 23.3–100; higher scores indicate greater anxiety) at baseline, positioning for procedure, wound washout, and time of first stich. A significant difference in the median mYPAS score was noted only at the time of positioning between dexmedetomidine versus midazolam, 23.3 versus 36.3, p = 0.007. A number needed to treat of 2 patients was calculated in favor of dexmedetomidine to maintain an mYPAS score of 23.3 at the time of positioning. There was no significant difference between groups for perception of anxiety with parents/guardians or procedural sedation providers. No significant differences in ADEs were noted. One patient (5.6%) in the midazolam group developed ataxia, and another patient (5.6%) developed emesis. The authors only noted a significant difference in anxiety reduction at the time of positioning for the procedure, but they commented that their study was underpowered to detect significant differences in other points during the procedure. Based on their findings, it appears that IN dexmedetomidine may be an alternative therapy for children requiring laceration repair because it had similar efficacy and had no ADEs reported compared with midazolam.
Midazolam Versus Ketamine. Younge and Kendall8 compared PO ketamine to PO midazolam for laceration repair. They randomized children to receive ketamine 10 mg/kg PO or midazolam 0.7 mg/kg PO. The primary outcomes of the study were comparison of the “Anxiety and Tolerance Scores” (1 = cooperative; 4 = uncontrolled crying, additional restraint needed) before and during the procedure and behavioral changes for up to 2 weeks after the procedure. In addition, they compared the difference in the time to achieve a sedation score of ≤3 (i.e., sleepy and arousable). The ketamine patients had greater tolerance of the local anesthetic injection (p = 0.029); however, there was no difference in the tolerance of the suturing process (p = 0.098). Patients receiving ketamine had a shorter time to achieve a sedation score ≤3, median (range), 20 (14–55) versus 43 (5–50) minutes, p = 0.001. However, there was no difference in the median time to discharge between groups (p > 0.05). Inconsolable agitation was the most prominent ADE in the midazolam group (20.7%), whereas vomiting (20.0%) occurred most frequently in the ketamine group. The authors noted that nystagmus occurred significantly more often in the ketamine group, but the number of patients affected was not reported. Follow-up monitoring information was available for 92% of patients, and behavioral changes (i.e., agitation, sleep disturbance, nightmares, bedwetting, temper tantrums, disobedience, separation anxiety) were noted by care-givers of patients in the midazolam group (48% versus 25%, p = 0.049). The investigators did not provide a specific breakdown of these ADEs, so it is difficult to determine what the most common behavioral changes were. They concluded that patients in the PO ketamine group had better tolerance with the procedure and fewer behavioral changes noted upon discharge than the PO midazolam group.
Rubinstein et al9 also compared PO ketamine versus PO midazolam. They randomized children to receive ketamine 5 mg/kg PO or midazolam 0.7 mg/kg PO. Visual analog scale scores were used to evaluate pain before and during the procedure, and University of Michigan Sedation Scale (UMSS) scores were used to assess sedation. The laceration repair was initiated once the UMSS score was ≥ 2. The primary objective was to compare caregiver VAS scores and the number of children that required IV sedation. There was no difference in the mean time to reach goal sedation between ketamine and midazolam, 23.61 ± 9.23 versus 25.79 ± 10.52 minutes, p = 0.44. Likewise, there was no difference noted in the mean maximum UMSS score during the procedure, 1.6 ± 0.84 versus 1.7 ± 0.65, p = 0.6. Despite this, a greater number of ketamine patients required IV sedation to complete the procedure, 12 (32%) versus 2 (6%), p = 0.014. When controlling for age and sex, patients who received ketamine were 6.1 times (95% CI, 1.2–30.5 times) more likely to require IV sedation. There were no differences in the length of procedure or time to discharge. When specifically looking at the patients who did not receive IV sedation, there were no differences in caregiver or investigator VAS scores. There were 2 ketamine patients (5.4%) who demonstrated significant agitation, and 1 patient (2.7%) who had vomiting. There was 1 midazolam patient (3.2%) who demonstrated agitation, and 1 patient (3.2%) who experienced vomiting. The authors noted that there was no difference in the level of pain between groups, but more patients receiving ketamine required the use of breakthrough IV sedation.
Based on this review, IN dexmedetomidine and N2O appear to be viable options for sedation and/or analgesia for laceration repair. Both demonstrated similar efficacy and fewer ADEs than either PO or IN midazolam.6,7 There was mixed evidence for support of PO ketamine versus PO midazolam. The efficacy of ketamine appears to be dose dependent, given that the study by Younge and Kendall8 found more favorable outcomes than Rubinstein et al9 with the 10 mg/kg versus 5 mg/kg regimen. However, it appears that the larger dose of ketamine was associated with increased ADEs.8
Fentanyl Monotherapy. Two studies have evaluated the use of TM fentanyl as monotherapy. Schutzman et al10 conducted an open-label, dose-finding study in which children were randomized to a small-dose (10–15 mcg/kg) or a large-dose (15–20 mcg/kg) group. Lozenges containing 200, 300, 400, or 500 mcg of fentanyl were administered 30 minutes prior to the repair. Pain was self-assessed using the Oucher Score and by observers using the CHEOPS at baseline and during repair. No differences in pain scores were noted between groups. Physician ratings of patient comfort and cooperation were acceptable in 83% of patients. There were statistically significant decreases from baseline pulse (98 ± 13 beats per minute) at 15 and 30 minutes (92 ± 13 and 89 ± 12 beats per minute, respectively, p < 0.05) in the small-dose group, and no significant changes in the large-dose group. Statistically significant differences were noted in respiratory rates from baseline in both groups, but these were deemed to be clinically insignificant. Only 1 patient (6.7%) experienced an oxygen desaturation <95% without clinical impact, and none of the patients experienced clinically significant hypotension. Vomiting and pruritus were the most frequently reported ADEs. The large-dose group had a higher rate of vomiting (47% versus 20%, p > 0.05). The onset of vomiting occurred 90 to 300 minutes after TM fentanyl administration. Pruritus occurred in 67% and 60% of the small- and larger-dose groups, respectively (p > 0.05). Based on the study results, the lower end of the dosing range should be targeted because efficacy was similar between groups, and the large-dose group experienced more vomiting.
Schutzman et al11 built on this dose-finding study and compared 10 to 15 mcg/kg TM fentanyl to their then-current standard of care (i.e., meperidine 2 mg/kg, promethazine 0.5 mg/kg, and chlorpromazine 0.5 mg/kg, intramuscular). The treating physician only was blinded to the treatment. Pain was assessed at baseline, at 30 minutes, and during the laceration repair by the CHEOPS; sedation was assessed using a 5-point activity scale measured in 15-minute increments. The patients in the standard of care group were significantly more sedated (p < 0.05); however, the CHEOPS pain scores did not differ between groups, and sedation was considered adequate in 75% of fentanyl and 69% of standard of care patients, p > 0.05. Similarly to the previous study, a clinically insignificant decrease in respiratory rate was noted. A higher rate of vomiting with TM fentanyl was noted in this study versus the previous study, 45% versus 20%10; however, rates of pruritus were similar between studies (60% versus 67%). The time to discharge was significantly lengthened in those patients who experienced vomiting versus those who did not (115 ± 23 versus 83 ± 20 minutes, p = 0.006). This study demonstrates that TM fentanyl has an efficacy comparable to that of the investigator's standard of care, although this IM regimen has fallen out of favor in clinical practice. The authors note that the high incidence of vomiting may be a limitation to acceptance of TM fentanyl.
Overall, TM fentanyl appears to be an effective analgesic and sedative at doses of 10 to 15 mcg/kg, 30 minutes prior to repair. The significant vomiting associated with TM fentanyl may limit its acceptance and could result in delayed discharge. In addition, the fixed-dosage forms of the lozenges could further limit use.
Ketamine Monotherapy. Two studies have evaluated the use of PO ketamine as monotherapy. Qureshi et al12 conducted a prospective, randomized study comparing ketamine 10 mg/kg PO versus placebo administered 30–45 minutes prior to laceration repair. The IV ketamine solution was added to cherry-flavored syrup to make a 25 mg/mL extemporaneous oral solution. The primary objective was comparison of pain tolerance during the lidocaine injection and at the start of laceration closure as measured by a quantitative tolerance scale (1 = cooperative; 4 = unable to complete procedure without additional sedation). More patients receiving ketamine were rated as “cooperative” during the lidocaine injection (66.7% versus 6.7%, p < 0.001) and during the suturing (73.3% versus 20.0%, p = 0.009). Most patients in the ketamine group (80%) were deemed to be adequately sedated during the suturing process and did not require continuous physical restraint. The mean time to discharge was longer in the ketamine group (104.0 ± 33.0 versus 90.0 ± 22.0 minutes, p = 0.04). No significant differences in hemodynamic parameters were noted between groups. However, nystagmus occurred in 20% and vomiting occurred in 13.3% of the ketamine group. The authors concluded that PO ketamine provides an option for sedation and analgesia for laceration repair.
Only 1 study has evaluated the use of IN ketamine for procedural sedation for laceration repair. Tsze et al13 conducted a prospective pilot study, which randomized patients to receive 3, 6, or 9 mg/kg IN ketamine. A 100 mg/mL IV ketamine solution was administered IN using a MAD. A Ramsey sedation score was assessed every 15 seconds until a score of 4 to 6 was achieved. If adequate sedation was not achieved within 30 minutes, IV ketamine was administered. The primary outcomes were time to onset of adequate sedation and efficacy of sedation based on the Observational Scale of Behavioral Distress-Revised. Adequate sedation was achieved in only 3 of 4 patients (75%) in the 9 mg/kg group, and the duration of sedation was 36 to 69 minutes in these patients. No patient receiving 3 or 6 mg/kg dose was adequately sedated. Serum concentrations of ketamine were evaluated 15 minutes after administration and at termination of the procedure or before administration of IV ketamine; however, no association was found between dose and serum concentrations. The only ADE reported was vomiting in 1 patient (8.3%) in the 9 mg/kg group. The authors concluded that the 9 mg/kg dose administered IN might provide adequate sedation but that further studies should be conducted to compare IN ketamine to other agents.
Ketamine 10 mg/kg PO monotherapy provided an efficacy comparable to that of PO midazolam. There are limited data with IN ketamine suggesting that larger dosing may be needed rather than lower dosing, but Tsze et al13 did not include a comparator agent, so it is difficult to determine its role in therapy. Nystagmus and vomiting appear to be the major ADEs.
Nitrous Oxide Monotherapy. Burton et al14 conducted a prospective, randomized trial to evaluate the efficacy of 50% N2O/50% oxygen versus 100% oxygen for the reduction of anxiety during laceration repair. All patients had to receive nothing by mouth for ≥2 hours, and the inhaled gas was administered 3 minutes prior to the procedure. Patients were evaluated using a modified CHEOPS score to assess pain, and the “Anxiety Level Scale” (1 = cooperative; to 4 = uncontrolled crying) to assess anxiety. The median CHEOPS scores during the procedure decreased by 5 points in the N2O group and increased by 3 points in the placebo group (p < 0.001). Further, the median anxiety scores decreased by 1 point in the N2O group, and they increased by 1 point in the placebo group (p < 0.001). A restraining device was required more frequently in the placebo group, 7 (54%) versus 3 (18%), p < 0.001. In the N2O group, dizziness and oversedation were reported in 23.5% and 11.8% of patients, respectively. Only 1 patient (5.9%) experienced vomiting. The authors concluded that N2O was a simple and effective modality for sedation.
Two additional studies provide support for the efficacy and safety of N2O monotherapy. Bar-Meir et al 15 compared 50% N2O to topical lidocaine alone. The N2O was administered 3 minutes prior to infiltration. Pain was assessed using the Faces, Legs, Activity, Cry, and Consolability (FLACC) scale. Pain scores were significantly lower during infiltration and suturing in the N2O group (p < 0.01). In addition, all patients in the control group required forceful restraint, whereas only 15% of the N2O group required minimal restraint (p = 0.0001). Of note, younger patients (i.e., <3 years) had higher FLACC scores during suturing than older patients who received N2O, 3.1 ± 3.6 versus 0.8 ± 2.0, p < 0.05. In patients who received N2O, 95.6% recovered in less than 1 minute, and all recovered within 3 minutes. One third of N2O patients experienced an ADE, with vomiting (11%) and euphoria (8%) occurring most frequently. The authors noted that N2O reduced pain scores with a fast onset and recovery time, with minimal ADEs.
Lee et al16 provided further support of the efficacy of N2O. Patients were randomized to 50% to 70% N2O or ketamine 2 mg/kg IV. Most patients (88.9%) received 50% to 60% N2O. Pain and sedation were assessed using the CHEOPS tool and the Children's Hospital of Wisconsin Sedation Scale, respectively. Patients in the N2O group had a lower but appropriate level of sedation, and their median pain scores during sedation preparation were lower than those of the IV ketamine group, 5 versus 12, p = 0.00. No differences in pain scores were noted during the remainder of the procedure. The median recovery time was significantly shorter in the N2O group (0 versus 21.5 minutes, p < 0.05). Only 1 patient (5.6%) in the N2O group experienced dizziness; no other ADEs were noted. N2O provided an adequate level of sedation and a fast recovery time.
Overall, it appears that N2O is an effective agent for laceration repair. Although deeper sedation was achieved with the comparator agents, it appears that adequate sedation was achieved to complete the procedure, and minimal if any restraint was needed. In addition, the onset time is relatively quick and little preparation is needed compared with IV sedatives. Of most benefit is the offset time, which is faster than that of other agents used as comparison groups.
Oral Midazolam Versus Oral Midazolam/Ketamine. Only 1 study has evaluated the combination therapy of PO ketamine plus PO midazolam. Barkan et al17 randomized patients to receive midazolam 0.5 mg/kg PO plus either ketamine 5 mg/kg PO or placebo. A 5-point sedation scale was used, and the procedure was initiated when a sedation score ≤4 (awake, calm) was achieved. If a sedation score of 4 was not achieved within 30 minutes, IV sedation was administered. In addition, caregivers used a VAS to assess pain. The primary objective was the comparison of caregiver VAS scores and investigator sedation scores. Mean time to achieve a sedation score ≤4 was shorter with the midazolam/ketamine (14.6 versus 17.9 minutes, p = 0.11). However, 8 patients (27.6%) in the midazolam/placebo group required IV sedation compared with 2 patients (6.5%) in the midazolam/ketamine group, p = 0.039. There were no differences in VAS scores by caregivers during administration of local anesthetic (p = 0.91); however, sedation scores were significantly lower during the procedure in the midazolam/ketamine group (p = 0.001). The authors did note a significantly longer mean time to discharge in the midazolam/ketamine group (186.8 versus 121.8 minutes, p = 0.003). No major ADEs were noted, although 3 patients (19.4%) in the midazolam/ketamine group experienced vomiting, and 1 patient (3.2%) had an oxygen desaturation <90% that resolved without intervention. The authors noted that the combination of PO ketamine and midazolam had faster onset and fewer children required IV sedation, but that there was a significant increase in time to discharge.
Oral Midazolam Versus Oral Midazolam/Transmucosal Fentanyl. Klein et al18 evaluated combination therapy of PO midazolam and TM fentanyl, in an effort to use lower TM fentanyl doses and minimize ADEs. All patients received midazolam 0.5 mg/kg PO and were randomized to receive either fentanyl 5 to 10 mcg/kg TM or placebo lozenge within 30 minutes of procedure. The primary objective was comparison of CHEOPS scores and the “Activity Scale” at baseline, at time of local anesthetic injection, and at 5-minute intervals until discharge. Similar activity scores, pain scores, and parental satisfaction were reported between groups. However, a greater number of ADEs were noted in the TM fentanyl group. There were 7 patients (26.9%) in the midazolam/fentanyl group who experienced vomiting versus none in the midazolam/placebo group, p = 0.01. In addition, 4 patients (15.4%) in the midazolam/fentanyl group and 2 (9.1%) in the midazolam/placebo group experienced pruritus, p = 0.36. This study demonstrates that the addition of TM fentanyl to midazolam did not result in increased efficacy but was associated with increased ADEs. The selection of a lower fentanyl dose versus those used in monotherapy studies may have affected the efficacy; however, as noted in these previous studies, larger doses are associated with a higher incidence of vomiting.10,11
Discussion
Practical Considerations. Fourteen studies provided data comparing sedatives and analgesics via the extra-vascular route to placebos or comparator agents and the sedatives and analgesics were noted to be efficacious.3–16 Two studies compared combination therapy using PO midazolam.17,18 It is difficult to compare the findings of these studies given the variability of sample size in the studies as well as the variety of agents, dosage forms, and dosing used. Further, the investigators used different scoring tools to assess tolerance of the procedure, pain, and/or sedation. The most common agent used for monotherapy was midazolam (n = 502), with the most common route being midazolam PO (n = 264).3–9,17,18 Based on this review, the next most common agent was N2O (n = 131).6,14–16
Table 3 provides a summary of the 10 different sedatives or analgesics used for monotherapy. Five different routes of administration were assessed, including IN, PO, TM, rectal, and inhaled. Based on these data, there appear to be a number of options available to clinicians for laceration repair, and there are a number of different factors that must be considered, including onset time, administration concerns, and ADEs. First, the onset time was not clearly defined in every study. Some studies had a clear objective sedation goal, and others included a predefined wait time between drug administration and procedure initiation. This being said, N2O had the shortest onset time, administered within 3 minutes before the procedure was initiated.14,15
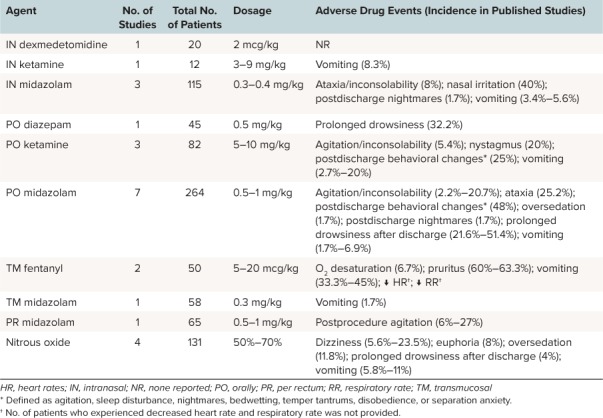
Table 3.
Summary of Medications Used as Monotherapy for Laceration Repair3–18
The route of administration can influence onset time and tolerability. For instance, Klein et al4 noted that IN midazolam had a faster onset time than PO midazolam. However, the IN route is associated with irritation, resulting in pain and agitation and decreased acceptance. Of the 4 studies that evaluated IN delivery, 3 studies used a MAD, and these studies used the IV dosage forms of ketamine, dexmedetomidine, and midazolam.3,4,7,13 Based on our review, 40% of patients receiving IN midazolam experienced irritation on administration, whereas no issues were noted with dexmedetomidine and ketamine (Table 2). This could be secondary to the pH of midazolam, which is more acidic (3), whereas the pH of ketamine (3.5–5.5) and the pH of dexmedetomidine (4.5–7) are less acidic.19,20 One potential solution that has been described in the literature is the use of 10 mg of lidocaine spray prior to IN midazolam with MADs to prevent discomfort.21 N2O is also inhaled as a gas mixture with oxygen, and hence has a very quick onset time, but children younger than 5 years may not tolerate the use of a facemask, which is needed to effectively deliver the gas mixture.22 However, 3 studies included in our review showed acceptable tolerance for children as young as 3 years, and the quick onset may offset any tolerability issues.6,14,15
Rectal administration may be poorly tolerated because of the perceived invasive delivery. In fact, Kanegaye et al5 noted that 2 patients had loss of rectal midazolam during administration. Several considerations should also be made for oral medication delivery. Some studies used the IV formulation of midazolam for PO administration,3,9,12,17 which is bitter and could affect palatability, and thus efficacy. When possible, clinicians should use the commercially available midazolam syrup. Currently there is no commercially available oral liquid for ketamine, so it may be prudent to consider masking the taste with a flavoring agent to improve tolerability. In the 2 studies evaluating TM fentanyl, the investigators used fixed-dosage forms of fentanyl lozenges.10,11 One concern with this formulation in children is biting of the lozenge instead of sucking, resulting in rapid release of fentanyl. In fact, Schutzman et al10 noted that 2 children bit and chewed the lozenge, although no significant ADEs were noted.
The ADEs associated with specific agents should also be taken into consideration. Table 2 provides a summary of the major ADEs reported. Vomiting was noted with a number of different agents, but it appears that PO and IN ketamine had the highest incidence compared with other agents. Tsze et al13 noted that larger doses of IN ketamine were needed to achieve better sedation and analgesia, but that this may be associated with a higher incidence of vomiting. Ataxia and nystagmus were noted with PO ketamine, PO midazolam, and IN midazolam. It is difficult to determine from these articles the onset time and time to resolution of these ADEs, so it seems prudent that clinicians should ensure that patients have an adequate monitoring period before discharge. Agitation, inconsolability, postdischarge behavioral changes, and postdischarge nightmares were noted with IN midazolam, PO ketamine, PO midazolam, and rectal midazolam. Although these results are not surprising given that these agents have been associated with intensive care unit delirium, these data indicate that caregivers should be counseled to watch for these symptoms after discharge. It is interesting to note that TM fentanyl was associated with a relatively high incidence of pruritus and vomiting, as well as decreased heart rate and respiratory rate. These ADEs are to be expected with systemic exposure of opioids. However, it should be noted that all of these patients received fixed doses of TM fentanyl, and this resulted in a larger dose of 5 to 20 mcg/kg compared with other doses used for other procedures.23 The only agent that was not found to have significant ADEs was IN dexmedetomidine. These results should be interpreted with caution given the small sample size and the lower dosing used compared with other studies with IN dexmedetomidine.24
Based on our findings, a number of unanswered questions remain regarding the most acceptable option for sedation and analgesia for laceration repair. There was a wide variety in the therapeutic end points and doses used between the studies. Most of the studies involved comparison of different agents for monotherapy. There are limited data to ascertain whether combination agents provided better efficacy and acceptable ADEs compared with monotherapy. Future research should involve a comparison of single agents versus combination agents incorporating standardized dosing and use of validated assessment tools for pain, sedation, and/or procedure tolerance. Two agents that should be considered for future research are IN fentanyl and dexmedetomidine. Several studies have evaluated the efficacy and safety of IN fentanyl for acute pain, but no such studies have been conducted for laceration repair.25,26 Only 1 study to date has evaluated IN dexmedetomidine for laceration repair, but studies have shown efficacy and safety for other procedures.27,28
CONCLUSIONS
Sedation and analgesia in addition to local/topical anesthetics are essential components to the treatment of laceration repair in children. There are data to support the use of IN dexmedetomidine, IN/PO ketamine, IN/PO/TM midazolam, PO diazepam, TM fentanyl, and N2O. Midazolam and N2O were the agents with the most data. Selection of the agents should be based on perceived need for pain versus sedation, patient accessibility, and ADEs. Future research is needed to determine the optimal agent and route for laceration repair.
ABBREVIATIONS
- ADE
adverse drug event
- CHEOPS
Children's Hospital of Eastern Ontario Pain Scale
- FLACC
Faces, Legs, Activity, Cry, and Consolability
- IV
intravenous
- IN
intranasal
- MAD
mucosal atomizer device
- mYPAS
modified Yale Preoperative Anxiety Scale
- PO
oral
- PR
per rectum
- TM
transmucosal
- UMSS
University of Michigan Sedation Scale
- VAS
visual analog scale
Footnotes
Disclosure No authors declare conflicts or financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, gifts, and honoraria.
Copyright Published by the Pediatric Pharmacy Advocacy Group. All rights reserved. For permissions, email: matthew.helms@ppag.org
REFERENCES
- 1. Cote CJ, Wilson S; American Academy of Pediatrics; . et al. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures: update 2016. Pediatrics. 2016; 138 1: e1– e31. [DOI] [PubMed] [Google Scholar]
- 2. Fein JA, Zempsky WT, Cravero JP, . et al. Clinical report: relief of pain and anxiety in pediatric patients in emergency medical systems. Pediatrics. 2012; 130 5: e1391– e1405. [DOI] [PubMed] [Google Scholar]
- 3. Everitt IJ, Barnett P.. Comparison of two benzodiazepines used for sedation of children undergoing suturing of a laceration in an emergency department. Pediatr Emerg Care. 2002; 18 2: 72– 74. [DOI] [PubMed] [Google Scholar]
- 4. Klein EJ, Brown JC, Kobayashi A, . et al. A randomized clinical trial comparing oral aerosolized intranasal and aerosolized buccal midazolam. Ann Emerg Med. 2011; 58 4: 323– 329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kanegaye JT, Favela JL, Acosta M, . et al. High-dose rectal midazolam for pediatric procedures: a randomized trial of sedative efficacy and agitation. Pediatr Emerg Care. 2003; 19 5: 329– 336. [DOI] [PubMed] [Google Scholar]
- 6. Luhmann JD, Kennedy RM, Porter FL, . et al. A randomized control trial of continuous flow nitrous oxide and midazolam for sedation of young children during laceration repair. Acad Emerg Med. 2001; 37 1: 20– 27. [DOI] [PubMed] [Google Scholar]
- 7. Neville DN, Hayes KR, Ivan Y, . et al. Double-blind randomized controlled trial of intranasal dexmedetomidine versus intranasal midazolam as anxiolysis prior to pediatric laceration repair in the emergency department. Acad Emerg Med. 2016; 23 8: 910– 917. [DOI] [PubMed] [Google Scholar]
- 8. Younge PA, Kendall JM.. Sedation for children requiring wound repair: a randomized controlled double blind comparison of oral midazolam and oral ketamine. Emerg Med J. 2001; 18 1: 30– 33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Rubinstein O, Barkan S, Breitbart R, . et al. Efficacy of oral ketamine compared to midazolam for sedation of children undergoing laceration repair: a double-blind, randomized, controlled trial. Medicine (Baltimore). 2016; 95 26: e3984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Schutzman SA, Burg J, Liebelt E, . et al. Oral transmucosal fentanyl citrate for premedication of children undergoing laceration repair. Ann Emerg Med. 1994; 24 6: 1059– 1064. [DOI] [PubMed] [Google Scholar]
- 11. Schutzman SA, Liebelt E, Wisk M, . et al. Comparison of oral transmucosal fentanyl citrate and intramuscular meperidine, promethazine, and chlorpromazine for conscious sedation of children undergoing laceration repair. Ann Emerg Med. 1996; 28 4: 385– 390. [DOI] [PubMed] [Google Scholar]
- 12. Qureshi FA, Mellis PT, McFadden MA.. Efficacy of oral ketamine for providing sedation and analgesia to children requiring laceration repair. Pediatr Emerg Care. 1995; 11 2: 93– 97. [DOI] [PubMed] [Google Scholar]
- 13. Tsze DS, Steele DW, Machan JT, . et al. Intranasal ketamine for procedural sedation in pediatric laceration repair. Pediatr Emerg Care. 2012; 28 8: 767– 770. [DOI] [PubMed] [Google Scholar]
- 14. Burton JH, Auble TE, Fuchs SM.. Effectiveness of 50% nitrous oxide/50% oxygen during laceration repair in children. Acad Emerg Med. 1998; 5 2: 112– 117. [DOI] [PubMed] [Google Scholar]
- 15. Bar-Meir E, Zaslansky R, Regev E, . et al. Nitrous oxide administered by the plastic surgeon for repair of facial lacerations in children in the emergency room. Plast Reconstr Surg. 2006; 117 5: 1571– 1575. [DOI] [PubMed] [Google Scholar]
- 16. Lee JH, Kim K, Kim TY, . et al. A randomized comparison of nitrous oxide versus intravenous ketamine for laceration repair in children. Pediatr Emerg Care. 2012; 28 12: 1297– 1301. [DOI] [PubMed] [Google Scholar]
- 17. Barkan S, Breitbart R, Brenner-Zada G, . et al. A double-blind, randomised, placebo-controlled trial of oral midazolam plus oral ketamine for sedation of children during laceration repair. Emerg Med J. 2014; 31 8: 649– 653. [DOI] [PubMed] [Google Scholar]
- 18. Klein EJ, Diekema DS, Paris CA, . et al. A randomized, clinical trial of oral midazolam plus placebo versus oral midazolam plus oral transmucosal fentanyl for sedation during laceration repair. Pediatrics. 2002; 109 5: 894– 897. [DOI] [PubMed] [Google Scholar]
- 19. Precedx [package insert]. Lake Forest, IL: Hospira Inc; 2013. [Google Scholar]
- 20. Trissel LA. Trissel's Stability of Compounded Formulations. 5th ed Washington, DC: American Pharmacists Association; 2012: 270. [Google Scholar]
- 21. Chiaretti A, Barone G, Rigante D, . et al. Intranasal lidocaine and midazolam for procedural sedation in children. Arch Dis Child. 2011; 96 2: 160– 163. [DOI] [PubMed] [Google Scholar]
- 22. Thomas A, Miller JL, Couloures K, . et al. Non-intravenous sedatives and analgesics for procedural sedation for imaging procedures in pediatric patients. J Pediatr Pharmacol Ther. 2015; 20 6: 418– 430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Chung S, Lim R, Goldman RD.. Intranasal fentanyl versus placebo for pain in children during cauterization for voiding cystourethrography. Pediatr Radiol. 2010; 40 7: 1236– 1240. [DOI] [PubMed] [Google Scholar]
- 24. Patel VJ, Ahmed SS, Nitu ME, . et al. Vasovagal syncope and severe bradycardia following intranasal dexmedetomidine for pediatric procedural sedation. Pediatr Anesth. 2014; 24 4: 446– 448. [DOI] [PubMed] [Google Scholar]
- 25. Schaefer JA, Mlekoday TJ.. Time to opioid administration after implementation of an intranasal fentanyl protocol. Am J Emerg Med. 2015; 33 12: 1805– 1807. [DOI] [PubMed] [Google Scholar]
- 26. Schacherer NM, Erikson Ramirez D, . et al. Expedited delivery of pain medication for long-bone fractures using an intranasal fentanyl clinical pathway. Pediatr Emerg Care. 2015; 31 8: 560– 563. [DOI] [PubMed] [Google Scholar]
- 27. Cao Q, Lin Y, Xie Z, . et al. Comparison of sedation by intranasal dexmedetomidine and oral chloral hydrate for pediatric ophthalmic examination. Paediatr Anaesth. 2017; 27 6: 629– 636. [DOI] [PubMed] [Google Scholar]
- 28. Ghai B, Jain K, Saxena AK, . et al. Comparison of oral midazolam with intranasal dexmedetomidine premedication for children undergoing CT imaging: a randomized, double-blind, and controlled study. Paediatr Anaesth. 2017; 27 1: 37– 44. [DOI] [PubMed] [Google Scholar]