

Abstract
Rationale:
Popliteal cyst developing in the sheath of a peripheral nerve or joint capsule may cause compression neuropathy. Although popliteal cyst is very common lesion, it seldom causes serious complications. Common peroneal nerve compression is rarely caused by an extraneural popliteal cyst.
Patient concerns:
We presented the case of a 52-year-old female with common peroneal nerve compression caused by an extraneural popliteal cyst.
Diagnoses:
Electromyography showed the damage of common peroneal nerve. MRI magnetic resonance imaging showed the lump to be a popliteal cyst. She was diagnosed as peroneal nerve injury and popliteal cyst.
Interventions:
The patient was performed peroneal nerve decompression and popliteal cyst excision surgery. We excised the cyst completely and soluted the common peroneal nerve thoroughly. The cyst was filled with thick mucinous material.
Outcomes:
The pathological report showed that the excised mass was a popliteal cyst. There were no postoperative complications. Pain and hypoesthesia resolved 6 months after surgery.
Lessons:
In this case, compression of the common peroneal nerve was due to an extraneural popliteal cyst, a situation rarely encountered. MRI can show in better detail their size and internal contents as well as their relation with surrounding anatomic structures. Patients with nerve entrapment caused by enlarged or ruptured cysts must be microsurgically excised if symptomatic.
Keywords: common peroneal nerve, popliteal cyst
1. Introduction
The first report on a popliteal cyst was written by Bamzai,[1] who related it to chronic rheumatoid arthritis of the knee joint. Thirty-seven years later, Baker [2] published his famous paper (on the formation of the synovial cysts in the leg) and already insisted on the connection between the cyst and a disease of the knee joint. He also gave his name to the condition, which became known as Baker/s cyst.
Common peroneal nerve compression is most common at the lateral aspect of the head of the fibula, but is rarely caused by an extraneural popliteal cyst. Although popliteal cyst is very common lesion, it seldom causes serious complications. Popliteal cyst developing in the sheath of a peripheral nerve or joint capsule may cause compression neuropathy. Compression neuropathy of common peroneal nerve caused by a popliteal cyst is rare. We report on 1 case of compression neuropathy of the common peroneal nerve caused by an extraneural popliteal cyst in our hospital recently. This study was approved by Institutional Review Boards and the patient signed in informed consent of operation and publication.
A 52-year-old female noted the development of a lump over her left popliteal fossa approximately 4 months prior to the consultation, which was associated with anaesthesia in the left calf for 1 month. Initially, the lump was found over her left popliteal fossa incidentally by palpation. It was quite small and no pain or discomfort was noted. Electromyography showed the damage of common peroneal nerve. MRI showed the lump to be a popliteal cyst (Fig. 1). Plain radiograph images of the left leg showed no abnormalities. With time, however, the lump appeared to grow in size. About 1 month prior to the consultation, the patient started to experience lower leg numbness sensation, especially over the lateral aspect of the left calf and the dorsum of foot. No apparent muscle weakness and pain was noted. The patient denied any apparent history of trauma to the affected left calf. On examination, there was a smooth and soft lump, sized about 3×2×3 cm3, over the left popliteal fossa which was not tender on palpation. The borders of the swelling were defined, and it was not fixed to the skin or underlying tissues. Positive Tinel's sign could be incited with tapping of the mass. There was no apparent muscle atrophy of both the lower limbs and neurological examination showed hypoesthesia over the dorsum of his left foot and the lateral aspect of the left calf, ankle, and knee joint motion were normal. Muscle power of the left lower limb, especially the big toe and ankle dorsiflexion as well as ankle plantar flexion, was comparable to those of the left lower limb. The left foot had a full range of movement with no disturbances in motor functions. The rest of the physical examination was unremarkable.
Figure 1.
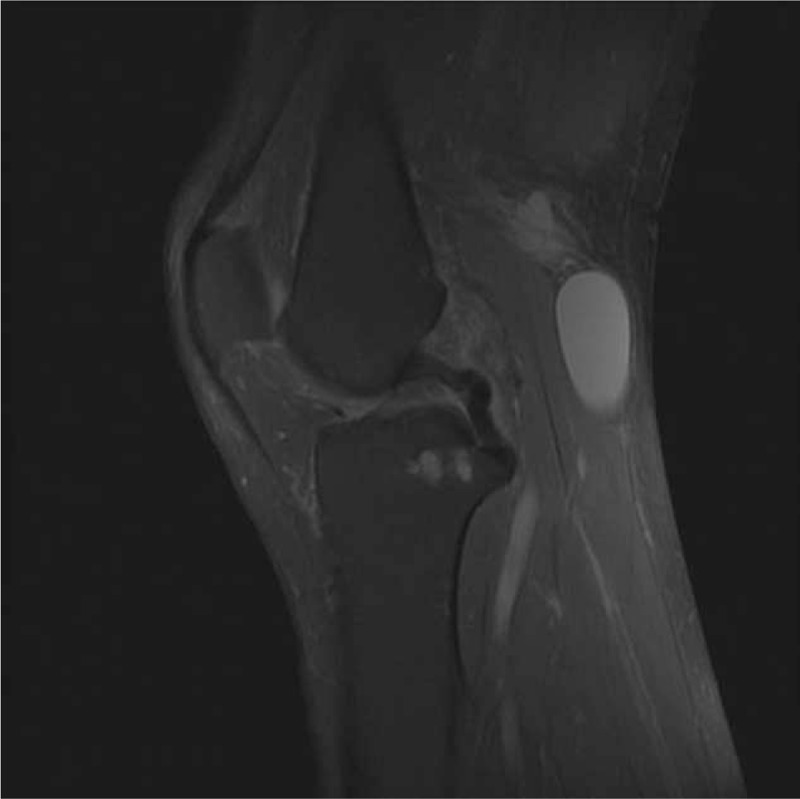
MRI of the knee showing a popliteal cyst (marked by the white arrow) extending from the proximal to the distal end of the popliteal fossa. MRI = magnetic resonance imaging.
With the sufficient preoperative preparation, we selected the direct posterior approach. The cyst was approached through the popliteal region by an S-shaped incision. Intraoperatively, a popliteal mass sized about 3×2×3 cm3 extending from the proximal to the distal end of the popliteal fossa was noted (Fig. 2). It tightly encased about 6 cm length of left common peroneal nerve at the level of 8 cm away from capitulum fibulae. We dissected sharply the mass with microsurgery scissors from the normal common peroneal nerve, and then we found that the common peroneal nerve encased by the mass became thin and there were serval bleeding point in the epineurium (Fig. 3). We excised the cyst completely and soluted the common peroneal nerve thoroughly. The cyst was filled with thick mucinous material. The pathological report showed that the excised mass was a Popliteal cyst (Fig. 4). There were no postoperative complications. Pain and hypoesthesia resolved 6 months after surgery.
Figure 2.
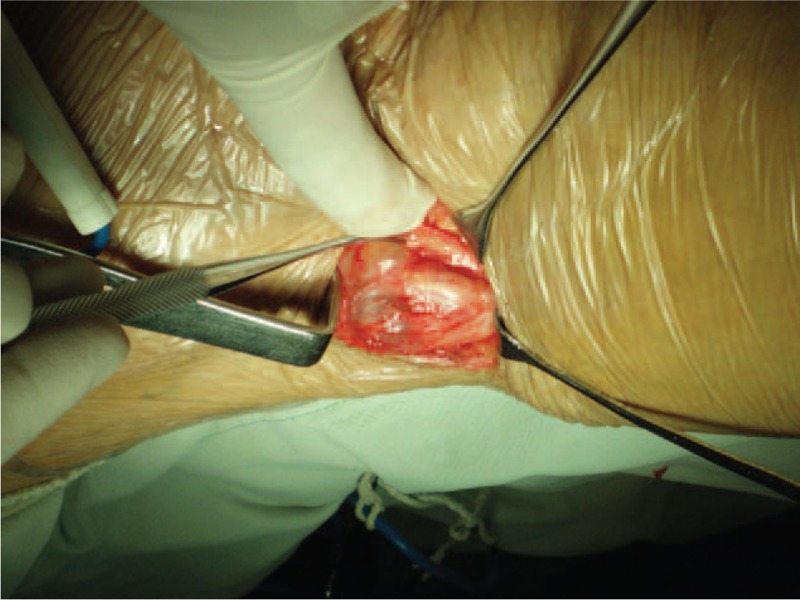
Intraoperative photograph of the popliteal fossa. A popliteal cyst (marked by the long arrow) sized about 3×2×3 cm3 extending from the proximal to the distal end of the popliteal fossa. It tightly encased left common peroneal nerve (marked by the short arrow) at the level of 8 cm away from capitulum fibulae.
Figure 3.
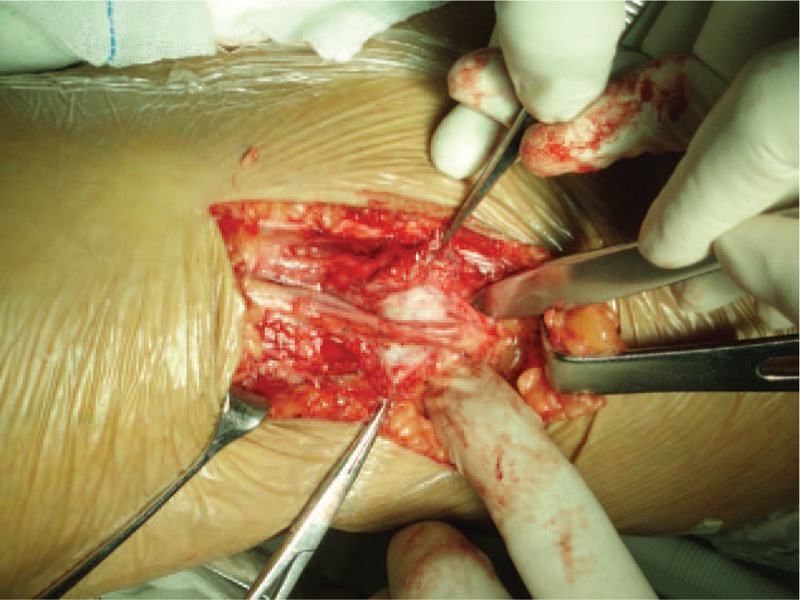
Intraoperative photograph of common peroneal nerve after the dissection of the popliteal cyst (marked by the long arrow). The common peroneal nerve (marked by the short arrow) encased by the mass became thin and there were serval bleeding point in the epineurium.
Figure 4.
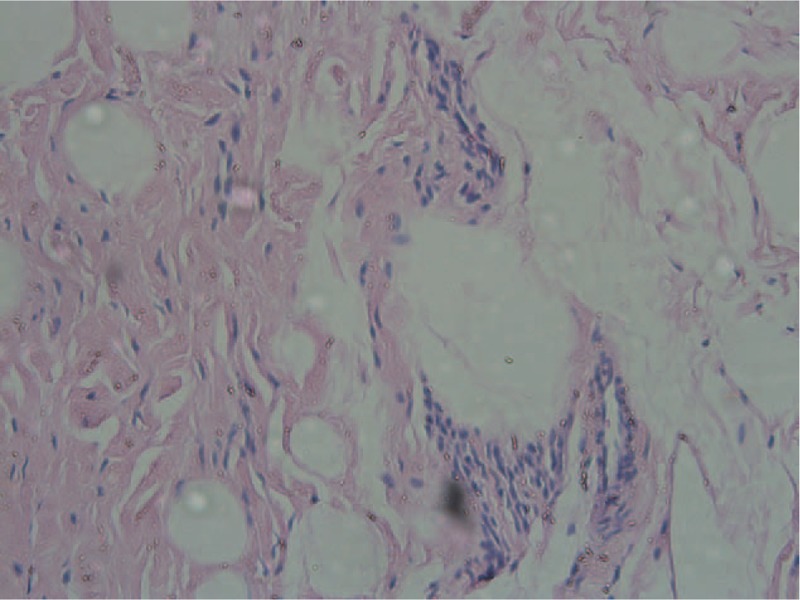
The pathological report showed that the excised mass was a popliteal cyst. (HE ×20).
2. Discussion
Popliteal cyst (Baker/s cyst) was a generic name of synovial cyst in the popliteal fossa. It can compress various anatomical structures. According to Malghem et al,[3] an anatomic classification distinguishes between synovial, meniscal, and ganglion cysts. The most frequent synovial popliteal cyst is generally considered to be a distension of the bursa located beneath the medial head of the gastrocnemius muscle. Another bursa has been described under the common tendon of the semimembranosus muscle. The common peroneal nerve is a branch of the sciatic nerve, usually arising at the junction of the upper two-thirds and lower third of the posterior compartment of the thigh. The common peroneal nerve descends obliquely along the lateral side of the popliteal fossa to the fibular head. It is medial to the biceps femoris and lies between its tendon and the lateral head of the gastrocnemius. It curves lateral to the fibular neck, where it is fixed to the bone by connective tissue, and then runs deep to the peroneus longus muscle where it divides into the deep and superficial peroneal nerves.[4] The common peroneal nerve may be entrapped anywhere along its course, giving rise to the clinical syndrome of peroneal nerve palsy.[5] Most of the popliteal cysts described in the literature causing peroneal nerve compression were of an intraneural type.[6] In our case, compression of the common peroneal nerve was due to an extraneural popliteal cyst, a situation rarely encountered. This type of cyst is often related to a history of knee injury,[7] which was not the case in our case. The most common symptoms of this condition are weakness in the tibialis anterior and peroneus longus and brevis muscles, and pain radiating from the knee to the lateral malleolus.[8] Hypoesthesia of the first web space and swelling of the proximal tibio-fibular joint are less common.[9]
2.1. Diagnosis
Standard plain radiographs are of little use in demonstrating soft tissue lesions but are routinely obtained because they are inexpensive, allow a panoramic view of the knee and can diagnose a variety of pathological conditions. Ultrasonography may be useful in showing the cystic nature of the mass and in distinguishing it from solid tumors. Cysts and their relations with adjacent muscles, tendons, nerves, and vessels can be accurately evaluated. MRI can show in better detail their size and internal contents as well as their relation with surrounding anatomic structures. Specific entities such as pigmented villonodular synovitis can be diagnosed. So MRI is the gold standard for evaluation of popliteal cysts. The final diagnosis is established by aspiration of the palpated mass, which is much easier when the swelling is large.[10]
2.2. Treatments
Surgical excision may very infrequently be required if the cyst remains symptomatic with pain and/or limited mobility attributable to the cyst despite treatment of the underlying disorder and administration of intra-articular glucocorticoids. Generally, surgical excision should be reserved only for those cases where more conservative interventions have failed and where there is significant functional impairment that can be ascribed to the cysts. Patients with nerve entrapment caused by enlarged or ruptured cysts must be microsurgically excised if symptomatic.[11] In this case, popliteal cyst tightly encased and compressed left common peroneal nerve lead to nerve injury. So it should be treated by microsurgical exploration as soon as possible.[12]
Author contributions
Data curation: Xiaobin Zeng, Lifeng Xie.
Methodology: Zhiqiang Qiu.
Writing – original draft: Kuo Sun.
Footnotes
Abbreviation: MRI = magnetic resonance imaging.
This work is supported by National Natural Science Foundation of China (No. 81660443) to KS.
XZ and LX contributed equally to this work.
The authors have no conflicts of interest to disclose.
References
- [1].Bamzai A, Krieger M, Kretschmer RR. Synovial cysts in juvenile rheumatoid arthritis. Ann Rheum Dis 1978;37:101–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Baker WM. On the formation of synovial cysts in the leg in connection with disease of the knee-joint. 1877. Clin Orthop Relat Res 1994;13:2–10. [PubMed] [Google Scholar]
- [3].Malghem J, Vandenberg BC, Lebon C, et al. Ganglion cysts of the knee: articular communication revealed by delayed radiography and CT after arthrography. Am J Roentgenol 1998;170:1579–83. [DOI] [PubMed] [Google Scholar]
- [4].Bang SU, Kim DJ, Bae JH, et al. Minimum effective local anesthetic volume for surgical anesthesia by subparaneural, ultrasound-guided popliteal sciatic nerve block: a prospective dose-finding study. Medicine (Baltimore) 2016;95:e4652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Jenkins MJ, Farhat M, Hwang P, et al. The distance of the common peroneal nerve to the posterolateral structures of the knee. J Arthroplasty 2016;31:2907–11. [DOI] [PubMed] [Google Scholar]
- [6].Sobol GL, Lipschultz TM. Successful surgical treatment of an intraneural ganglion of the common peroneal nerve. Am J Orthop (Belle Mead NJ) 2015;44:E123–6. [PubMed] [Google Scholar]
- [7].Yazid Bajuri M, Tan BC, Das S, et al. Compression neuropathy of the common peroneal nerve secondary to a ganglion cyst. Clin Ter 2011;162:549–52. [PubMed] [Google Scholar]
- [8].Brooks DM. Nerve compression by simple ganglia. J Bone Joint Surg Br 1952;34-B:391–400. [DOI] [PubMed] [Google Scholar]
- [9].Stack RE, Bianco AJ, MacCarthy CS. Compression of the common peroneal nerve by ganglion cysts: report of nine cases. J Bone Joint Surg Am 1965;47:773–8. [PubMed] [Google Scholar]
- [10].Zhou XN, Li B, Wang JS, et al. Surgical treatment of popliteal cyst: a systematic review and meta-analysis. J Orthop Surg Res 2016;11:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Petit-Lacour MC, Pico F, Rappoport N, et al. Fluctuating peroneal nerve palsy caused by an intraneural cyst. J Neurol 2002;249:490–1. [DOI] [PubMed] [Google Scholar]
- [12].Rawal A, Ratnam KR, Yin Q. Compression neuropathy of common peroneal nerve caused by an extraneural ganglion: a report of two cases. Microsurgery 2004;24:63–6. [DOI] [PubMed] [Google Scholar]