

Abstract
Nicotinamide phosphoribosyltransferase (NAMPT) possesses various functions in human cells, and altered NAMPT expression is associated with human carcinogenesis. The present study detected the expression of NAMPT in normal and cancerous breast tissues from 83 patients using immunohistochemistry, and analyzed its association with the clinicopathological and survival data of the patients. NAMPT was significantly overexpressed in the breast invasive ductal carcinoma tissues compared with adjacent normal mammary gland tissues. Upregulated NAMPT expression was associated with a larger tumor size, lymph node metastasis, advanced clinical tumor-node-metastasis stages, and estrogen receptor and progesterone receptor expression. Furthermore, NAMPT expression was associated with poor overall and disease-free survival in patients with breast cancer. In conclusion, NAMPT increased protein expression in tumor cells may contribute to the development and progression of breast invasive ductal carcinoma. Thus, detection of NAMPT expression might be useful as a biomarker for the early detection and prognosis prediction of breast cancer.
Keywords: breast cancer, nicotinamide phosphoribosyltransferase, immunohistochemistry, prognosis
Introduction
Breast cancer is a significant health problem in women globally, and breast cancer incidence rates are higher in North America and Western Europe, compared with those in other parts of the world. In the United States in 2016, there were ~249,260 new cases of breast cancer and 40,890 cancer-related deaths (1). In China, breast cancer has become one of the most frequently diagnosed cancers in women aged 30–59 years old (2), and a high proportion of the patients are diagnosed at the advanced stages of disease (2); for those patients, treatment responses, even with post-surgical chemotherapy and radiotherapy, remain poor (2). Thus, novel molecular biomarkers are required for the early detection and treatment response prediction in patients with breast cancer.
Mammalian cell nicotinamide phosphoribosyltransferase (NAMPT) is the rate-limiting enzyme in the biosynthesis of nicotinamide adenine dinucleotide (NAD) that is responsible for transferring a phosphoribosyl group from 5-phosphoribosyl-1-pyrophosphate to nicotinamide, resulting in the production of nicotinamide mononucleotide (NMN) and pyrophosphate. NMN is then converted to NAD by NMN adenylyltransferase (Fig. 1) (3). Increasing evidence suggests that NAMPT is a multifunctional enzyme with crucial roles in in metabolism and immune response, and altered NAMPT expression is associated with human tumorigenesis (4). Silencing of NAMPT expression in pancreatic cancer cells has been demonstrated to induce tumor cell metabolic collapse and cell death both in vitro and in vivo (5), whereas NAMPT overexpression is associated with poor treatment response of breast cancer patients to doxorubicin-based chemotherapy (6). Previous studies from our group have demonstrated that NAMPT is highly expressed in gastric cancer and is associated with malignant behaviors of cancer cells as well as resistance to chemotherapy (7,8). The aim of the present study was to detect NAMPT expression in normal and cancerous breast tissues using immunohistochemistry and to examine its association with clinicopathological and survival data from breast cancer patients.
Figure 1.

The NAD biosynthesis pathway. NAMPT can transfer a phosphoribosyl group obtained from PRPP to nicotinamide, resulting in the production of NMN and PPi. Thereafter, NMN is converted to NAD by NMNAT. NAD, nicotinamide adenine dinucleotide; NAMPT, nicotinamide phosphoribosyltransferase; PRPP, 5-phosphoribosyl-1-pyrophosphate; NMN, nicotinamide mononucleotide; PPi, pyrophosphate; NMNAT, nicotinamide mononucleotide adenylyltransferase.
Materials and methods
Patient samples
Paired cancerous and adjacent noncancerous breast tissues were collected from 83 newly diagnosed and surgically treated breast cancer patients at Weihai Municipal Hospital (Weihai, China) between January and December 2008. The adjacent normal tissues were >5 cm away from the tumor lesions. All patients were histologically diagnosed with invasive ductal carcinoma and aged 29–66 years old, with an average age of 47 years. None of the patients received presurgical radiotherapy or chemotherapy. The present study was approved by the Ethics Committee of Weihai Municipal Hospital, and informed consent was obtained from each patient. The histologic types and grades of the primary tumors were determined according to the modifications of the World Health Organization classification (9), whereas the staging of breast cancer was defined according to the tumor-node-metastasis (TNM) system (10).
Immunohistochemistry
All tissue samples were fixed in 10% buffered formalin at room temperature for 24 h and subsequently embedded into paraffin. Tissue sections 4-µm thick were then prepared from these paraffin blocks and immunohistochemically stained using the streptavidin peroxidase (SP) technique. In brief, tissue sections were deparaffinized in xylene, rehydrated in a series of ethanol solutions, and then submerged in tap water. The tissue sections were subjected to antigen retrieval in a pressure cooker containing 0.01 M citrate buffer and blocking of the peroxidase activity in 3% H2O2 for 30 min at room temperature. Next, they were incubated with 20% normal goat serum (Abcam, Cambridge, MA, USA) diluted in PBS for 30 min and then with an anti-NAMPT antibody (cat. no., ab45890; 1:50; Abcam) at 4°C overnight. The next day, the tissues sections were washed with PBS briefly three times, and then incubated with a goat anti-mouse immunoglobulin G (cat. no., sc-2039; 1:200; Santa Cruz Biotechnology, Inc., Dallas, TX, USA) conjugated with SP for 30 min at room temperature. After washing with PBS, the tissue sections were subjected to a colorimetric reaction using 3,3′-diaminobenzidine solution, then counterstained with hematoxylin briefly, mounted with mounting medium, and covered with a coverslip. The immunostained tissue sections were reviewed and photographed under a light microscope. Image acquisition and analysis were then performed. Positively stained cells appeared brown or displayed brown cytoplasmic granules in the cytoplasm. NAMPT immunostaining scores were based on the intensity of the immunostaining and the % of positively stained cells. Immunostaining intensity was scored as follows: 0, no staining; 1, weak staining; 2, moderate staining; and 3, strong staining. Percentage of positive staining was scored as follows; 1, ≤25% positive cells; 2, 26–50% positive cells; 3, 51–75% positive cells; and 4, ≥76% positive cells. The sum of these two scores resulted in a final score for each case to determine high vs. low expression of NAMPT protein (a score of ≥3 was termed high NAMPT expression, whereas a score of 1–2 was termed low NAMPT expression). The staining of each tissue section was scored separately by two independent experts simultaneously, and discordant scores were re-evaluated and scored with their consensual opinion.
Statistical analysis
All statistical analyses were performed using the SPSS version 17.0 software (SPSS, Inc., Chicago, IL, USA). Comparisons of NAMPT expression with clinicopathological parameters, including tumor stage, tumor grade, age at diagnosis, body mass index, tumor size, lymph node status, recurrence, estrogen receptor (ER) status, progesterone receptor (PR) status, and human epidermal growth factor receptor 2 (HER2) status, were analyzed using the χ2 or Fisher's exact test (when a cell in a 2×2 table had an expected frequency of ≤5). Survival curves were generated using Kaplan-Meier curves and statistically analyzed using the log-rank test. Multivariate analysis was performed using Cox's proportional hazard model. P<0.05 was considered to indicate a statistically significant difference.
Results
Differential expression of NAMPT in normal breast and cancerous tissues
NAMPT protein expression was localized in the cytoplasm and cell membrane of positive tumor or normal cells. Specifically, NAMPT protein was mostly expressed in breast invasive ductal carcinoma as well as in a few adjacent normal mammary glands (Fig. 2). There was no single tumor with completely negative NAMPT expression (Fig. 2). Expression of NAMPT protein was significantly upregulated in breast cancer tissues compared with normal breast tissues (P<0.001; Table I). Then, the association of NAMPT expression with the clinicopathological data from the breast cancer patients was analyzed. The results demonstrated that upregulated NAMPT protein expression was associated with a larger tumor size, lymph node metastasis, advanced clinical TNM stages, and ER and PR expression (Table II).
Figure 2.

Immunohistochemical analysis of NAMPT expression in normal and cancerous breast tissues. (A) Strong immunostaining of NAMPT protein in breast cancer tissue. Arrow indicates NAMPT positive expression. (B) Strong and moderate immunostaining of NAMPT protein in breast cancer tissue. Arrow indicates NAMPT positive expression. (C) Negative immunostaining of NAMPT in normal breast tissue. Magnification, ×400. NAMPT, nicotinamide phosphoribosyltransferase.
Table I.
NAMPT expression in breast cancer tissue samples.
| Group | High NAMPT expression | Low or no NAMPT expression | P-value |
|---|---|---|---|
| Breast cancer | 40 | 43 | |
| Adjacent normal tissues | 0 | 83 | 0.001 |
NAMPT, nicotinamide phosphoribosyltransferase.
Table II.
Association of NAMPT expression with clinicopathological characteristics in breast cancer patients.
| Level of NAMPT expression | |||
|---|---|---|---|
| Variables | Low (n) | High (n) | P-value |
| Age (years) | |||
| ≤50 | 25 | 19 | |
| >50 | 18 | 21 | 0.330 |
| Tumor size (cm) | |||
| <2 | 25 | 12 | |
| ≥2 | 18 | 28 | 0.010 |
| LN metastasis | |||
| No | 36 | 24 | |
| Yes | 7 | 16 | 0.016 |
| TNM stage | |||
| I/II | 37 | 26 | |
| III/IV | 6 | 14 | 0.030 |
| Grade | |||
| I/II | 34 | 28 | |
| III | 9 | 12 | 0.340 |
| ER expression | |||
| Negative | 6 | 19 | |
| Positive | 37 | 21 | 0.001 |
| PR expression | |||
| Negative | 11 | 23 | |
| Positive | 32 | 17 | 0.003 |
| HER2 expression | |||
| Negative | 24 | 27 | |
| Positive | 19 | 13 | 0.274 |
NAMPT, nicotinamide phosphoribosyltransferase; LN, lymph node; TNM, tumor-node-metastasis staging; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2.
Association of NAMPT protein expression with survival of breast cancer patients
Next, the association of NAMPT expression with survival of the breast cancer patients was examined. Kaplan-Meier curves, stratified by high vs. low NAMPT expression, revealed that high NAMPT expression was associated with a poor overall and disease-free survival in patients, while breast cancer tissues without or with low NAMPT expression had better disease-free and overall survival rates (P=0.010 and P=0.045; Fig. 3). Furthermore, compared with patients with ER-positive tumors, patients with ER-negative tumors had a significantly worse disease-free survival both in the high NAMPT group and in the low NAMPT group (P=0.022 and P=0.002, respectively) and overall survival both in the high NAMPT group and in the low NAMPT group (P=0.042 and P=0.019, respectively) (Figs. 4 and 5).
Figure 3.
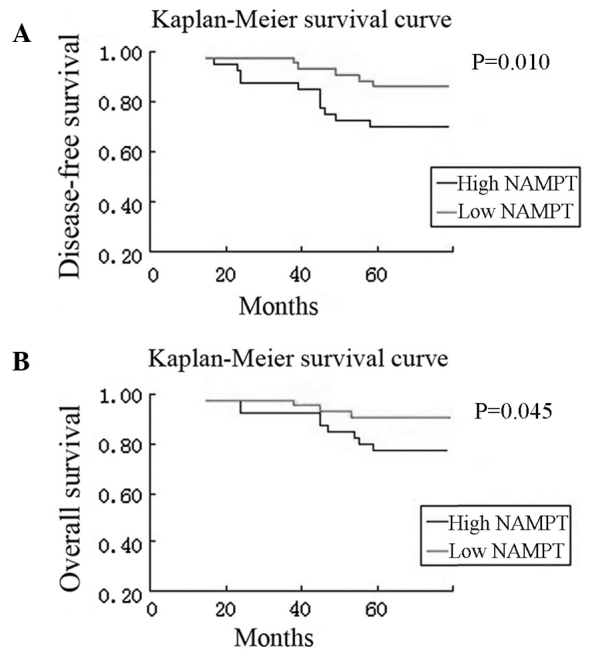
Kaplan-Meier survival curves stratified by NAMPT expression in breast cancer patients. (A) Disease-free survival. (B) Overall survival. NAMPT, nicotinamide phosphoribosyltransferase.
Figure 4.
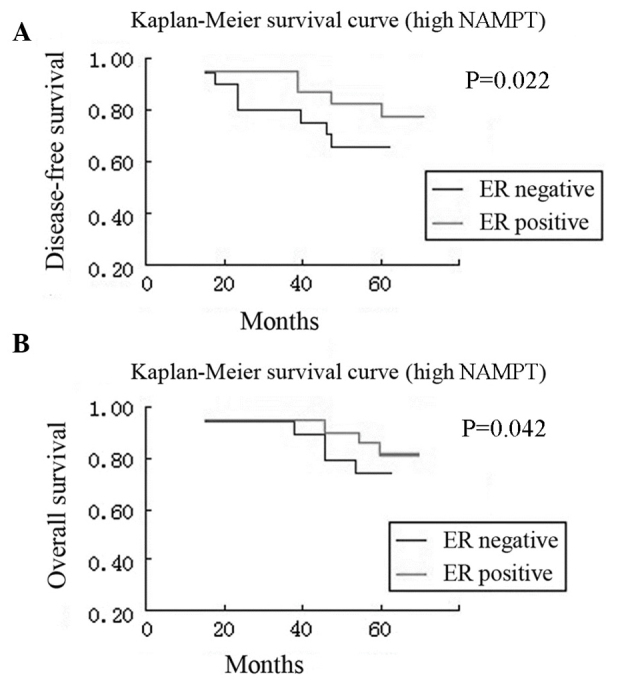
Kaplan-Meier curves stratified by ER expression in patients with high tumor expression of NAMPT. (A) Disease-free survival. (B) Overall survival. ER, estrogen receptor; NAMPT, nicotinamide phosphoribosyltransferase.
Figure 5.
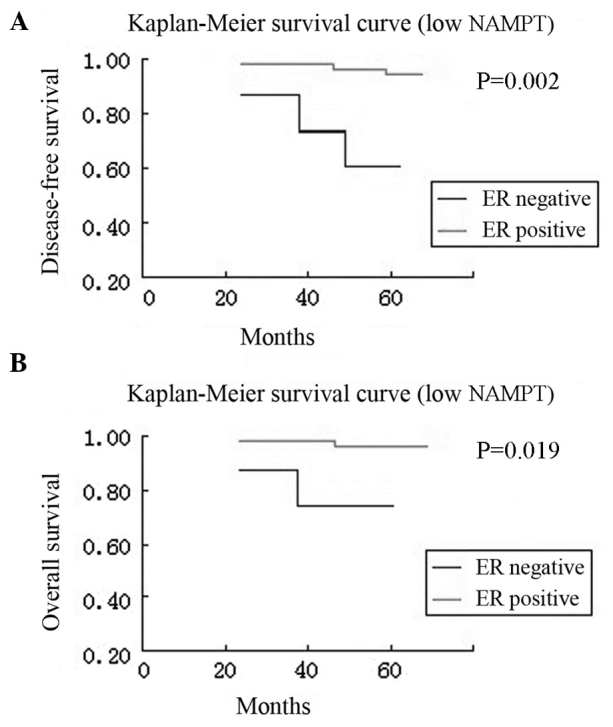
Kaplan-Meier curves stratified by ER expression in patients with low tumor expression of NAMPT. (A) Disease-free survival. (B) Overall survival. ER, estrogen receptor; NAMPT, nicotinamide phosphoribosyltransferase.
To evaluate the factors associated with NAMPT expression in these patients, hazard ratios (HRs) were estimated by univariate and multivariate Cox regression analyses (Tables III and IV). For the univariate analysis, the significant factors associated with disease-free survival included tumor stage (HR=52.39, 95% CI=11.90–230.65, P<0.001), tumor grade (HR=2.66, 95% CI=1.01–7.01, P=0.047), ER status (HR=0.29, 95% CI=0.12–0.72, P=0.007) and NAMPT expression (HR=3.13, 95% CI=1.27–7.73, P=0.013; Table III). By contrast, the only significant factor associated with overall survival was tumor stage (HR=55.02, 95% CI=7.12–425.20, P<0.001; Table IV). However, after adjusting for the patient age at diagnosis, tumor stage, tumor grade, ER status, HER2 status, and NAMPT expression by multivariate Cox regression analysis, only tumor stage (HR=63.42, 95% CI=12.91–311.48, P<0.001 and HR=115.26, 95% CI=13.24–1003.63, P<0.001, respectively) and NAMPT expression (HR=0.53, 95% CI=0.17–1.59, P=0.255 and HR=0.20, 95% CI=0.04–0.89, P=0.034, respectively) were significant independent predictors of disease-free and overall survival in the breast cancer patients (Tables III and IV).
Table III.
Univariate and multivariate analyses of disease-free survival in breast cancer cases.
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | P-value | HR | 95% CI | P-value |
| Age (years) | ||||||
| >50 | 0.80 | 0.32–1.98 | 0.622 | 0.91 | 0.32–2.59 | 0.861 |
| ≤50 | 1.00 | 1.00 | ||||
| Stage | ||||||
| III/IV | 52.39 | 11.90–230.65 | <0.001 | 63.42 | 12.91–311.48 | <0.001 |
| I/II | 1.00 | 1.00 | ||||
| Grade | ||||||
| III/IV | 2.66 | 1.01–7.01 | 0.047 | 0.98 | 0.33–2.95 | 0.967 |
| I/II | 1.00 | 1.00 | ||||
| ER | ||||||
| Positive | 0.29 | 0.12–0.72 | 0.007 | 0.49 | 0.16–1.54 | 0.225 |
| Negative | 1.00 | 1.00 | ||||
| HER2 | ||||||
| Positive | 0.97 | 0.38–2.45 | 0.942 | 0.81 | 0.28–2.32 | 0.687 |
| Negative | 1.00 | 1.00 | ||||
| NAMPT | ||||||
| High | 3.13 | 1.27–7.73 | 0.013 | 0.53 | 0.17–1.59 | 0.255 |
| Low | 1.00 | 1.00 | ||||
HR, hazard ratio; CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; NAMPT, nicotinamide phosphoribosyltransferase.
Table IV.
Univariate and multivariate analyses of overall survival in breast cancer cases.
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | P-value | HR | 95% CI | P-value |
| Age (years) | ||||||
| >50 | 0.96 | 0.32–2.86 | 0.941 | 0.82 | 0.24–2.81 | 0.754 |
| ≤50 | 1.00 | 1.00 | ||||
| Stage | ||||||
| III/IV | 55.02 | 7.12–425.20 | <0.001 | 115.26 | 13.24–1003.63 | <0.001 |
| I/II | 1.00 | 1.00 | ||||
| Grade | ||||||
| III/IV | 2.56 | 0.79–8.31 | 0.118 | 0.90 | 0.24–3.33 | 0.872 |
| I/II | 1.00 | 1.00 | ||||
| ER | ||||||
| Positive | 0.59 | 0.19–1.81 | 0.359 | 0.80 | 0.19–3.39 | 0.766 |
| Negative | 1.00 | 1.00 | ||||
| HER2 | ||||||
| Positive | 0.72 | 0.22–2.35 | 0.591 | 0.80 | 0.22–2.91 | 0.731 |
| Negative | 1.00 | 1.00 | ||||
| NAMPT | ||||||
| High | 1.34 | 0.41–4.35 | 0.628 | 0.20 | 0.04–0.89 | 0.034 |
| Low | 1.00 | 1.00 | ||||
HR, hazard ratio; CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; NAMPT, nicotinamide phosphoribosyltransferase.
Discussion
Although early detection and treatment of breast cancer have significantly advanced compared with decades ago, more research is needed for the molecular diagnosis and prognosis prediction of breast cancer. In the current study, NAMPT expression was analyzed and associated with breast cancer development and progression in order to potentially identify it as a novel biomarker for breast cancer. The present data demonstrated that NAMPT expression was significantly higher in breast cancer tissues compared with normal mammary gland tissues, and that upregulated NAMPT protein expression was associated with a larger tumor size, advanced clinical TNM stages, lymph node metastasis, and ER and PR expression. Furthermore, NAMPT expression was associated with poor overall and disease-free survival in patients, whereas breast cancer without or with low NAMPT expression had a better disease-free and overall survival. In conclusion, the present findings suggest that NAMPT upregulation may contribute to breast cancer development and progression and that detection of NAMPT protein levels may serve as a biomarker for the early detection and prognosis prediction of breast cancer.
Indeed, NAMPT has been reported to be overexpressed in several types of human cancer and to induce resistance to therapy (3), suggesting that NAMPT could be used as a chemotherapeutic target (3). Translationally, NAMPT might be a useful biomarker for carcinogenesis and tumor progression (4). For example, upregulated NAMPT expression has been associated with an increase in melanoma volume, early metastases, and tumor cell de-differentiation (11). In addition, NAMPT overexpression has been observed in hematological malignancies, such as lymphomas, and is associated with aggressive phenotypes of malignant lymphoma (12). In solid tumors, NAMPT is upregulated in prostate, gastric, and colorectal cancers (13–15), and NAMPT inhibition reduces the growth and invasiveness of prostate cancer cells in vitro (15). A previous study has reported that detection of NAMPT, vascular endothelial growth factor, and HER2 could be useful as a biomarker panel for the diagnosis and prognosis of human breast cancer (16). The current study further confirmed the overexpression of NAMPT protein in invasive breast cancer and it association with breast cancer progression and prognosis. Of note, a previous in vitro study has demonstrated that NAMPT expression influences breast cancer cell metastatic activity and adhesion by inhibition of integrin function (17).
Breast cancer exhibits many molecular alterations; for example, BRCA mutations are the main hereditary factor in the development of breast cancer, while the expression of poly (ADP-ribose) polymerase 1 (PARP1) contributes to the BRCA1 phenotype in basal-like and triple-negative breast cancers (18). In addition, BRCA1-mediated NAD synthesis is largely responsible for PARP1 activity in breast cancer cells, while NAMPT regulates NAD levels towards aberrant PARP1 activity (19). Indeed, Bajrami et al (20) have reported that an NAMPT inhibitor in combination with a PARP inhibitor has a significant therapeutic potency in nude mouse triple-negative breast cancer cell xenografts. NAMPT was originally cloned as a putative cytokine to enhance the maturation of B lymphocyte precursors (21). Later, it was reported that NAMPT is able to promote both B lymphocyte and vascular smooth muscle cell maturation as well as inhibit neutrophil apoptosis (22). A previous study has demonstrated that NAMPT expression can predict recurrence-free survival of lung and breast cancer patients (23). Another recent study has revealed a novel mechanism by which breast cancer cells are able to protect themselves from glucose deprivation-induced oxidative stress through NAMPT to maintain NADPH levels (24). Together, these findings indicate that NAMPT overexpression can alter human immune responses and promote breast cancer progression.
FK866 (also known as APO866) is a small-molecule inhibitor of NAMPT with potency and selectivity; in vitro, it is able to suppress the growth of cancer cells and induce tumor cells to undergo apoptosis through NAD depletion (25). Notably, FK866 can selectively inhibit various types of cancer cells, but not normal cells (25). The current data indicate that breast cancer may be another organ site where NAMPT inhibitors may be useful in the clinic.
To fully understand the physiological relevance of NAMPT expression in normal and cancerous mammary gland cells, further research will be necessary. For example, future studies may include information on subtypes of breast cancer and expression of other molecules to examine the associations with NAMPT expression. In addition, the data from the current study need to be verified using a larger sample size before NAMPT is used clinically as a biomarker. Further studies will also assess NAMPT in mediating breast cancer progression and the potential of targeting NAMPT as a therapeutic strategy in breast cancer.
Acknowledgements
The authors would like to thank the staff of the Genetic Disease Research Institution, Xi'an Jiaotong University (Xi'an, China) for their technical assistance.
Funding
This study was supported in part by a grant from Weihai Municipal Hospital Research Fund (grant no. WHSLYYZBB2016-107).
Availability of data and materials
The analyzed datasets generated during the study are available from the corresponding author upon reasonable request.
Author's contributions
SJZ and TQB generated and analyzed data for all figures; CXQ generated and analyzed data for Tables I and II; XQY generated data for Tables III and IV; KP verified statistical analysis; TQB wrote the manuscript, which was approved by all authors; SJZ supervised the project and secured funding.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Weihai Municipal Hospital (Weihai, China), and informed consent was obtained from all patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have competing interests.
References
- 1.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. doi: 10.3322/caac.21332. [DOI] [PubMed] [Google Scholar]
- 2.Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–132. doi: 10.3322/caac.21338. [DOI] [PubMed] [Google Scholar]
- 3.Shackelford RE, Mayhall K, Maxwell NM, Kandil E, Coppola D. Nicotinamide phosphoribosyltransferase in malignancy: A review. Genes Cancer. 2013;4:447–456. doi: 10.1177/1947601913507576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bi TQ, Che XM. Nampt/PBEF/visfatin and cancer. Cancer Biol Ther. 2010;10:119–125. doi: 10.4161/cbt.10.2.12581. [DOI] [PubMed] [Google Scholar]
- 5.Chini CC, Guerrico AM, Nin V, Camacho-Pereira J, Escande C, Barbosa MT, Chini EN. Targeting of NAD metabolism in pancreatic cancer cells: Potential novel therapy for pancreatic tumors. Clin Cancer Res. 2014;20:120–130. doi: 10.1158/1078-0432.CCR-13-0150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Folgueira MA, Carraro DM, Brentani H, Patrão DF, Barbosa EM, Netto MM, Caldeira JR, Katayama ML, Soares FA, Oliveira CT, et al. Gene expression profile associated with response to doxorubicin-based therapy in breast cancer. Clin Cancer Res. 2005;11:7434–7443. doi: 10.1158/1078-0432.CCR-04-0548. [DOI] [PubMed] [Google Scholar]
- 7.Bi TQ, Che XM, Liao XH, Zhang DJ, Long HL, Li HJ, Zhao W. Overexpression of Nampt in gastric cancer and chemopotentiating effects of the Nampt inhibitor FK866 in combination with fluorouracil. Oncol Rep. 2011;26:1251–1257. doi: 10.3892/or.2011.1378. [DOI] [PubMed] [Google Scholar]
- 8.Long HL, Che XM, BI TQ, Li HJ, Liu JS, Li DW. The expression of nicotinamide phosphoribosyl transferase and vascular endothelial growth factor-A in gastric carcinoma and their clinical significance. Zhonghua Wai Ke Za Zhi. 2012;50:839–842. [PubMed] [Google Scholar]
- 9.Tavassoli FA. Pathology of the Breast. McGraw-Hill Medical; New York, NY, USA: 1999. pp. 254–397. [Google Scholar]
- 10.Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010. [Google Scholar]
- 11.Maldi E, Travelli C, Caldarelli A, Agazzone N, Cintura S, Galli U, Scatolini M, Ostano P, Miglino B, Chiorino G, et al. Nicotinamide phosphoribosyltransferase (NAMPT) is over-expressed in melanoma lesions. Pigment Cell Melanoma Res. 2013;26:144–146. doi: 10.1111/pcmr.12037. [DOI] [PubMed] [Google Scholar]
- 12.Olesen UH, Hastrup N, Sehested M. Expression patterns of nicotinamide phosphoribosyltransferase and nicotinic acid phosphoribosyltransferase in human malignant lymphomas. APMIS. 2011;119:296–303. doi: 10.1111/j.1600-0463.2011.02733.x. [DOI] [PubMed] [Google Scholar]
- 13.Nakajima TE, Yamada Y, Hamano T, Furuta K, Gotoda T, Katai H, Kato K, Hamaguchi T, Shimada Y. Adipocytokine levels in gastric cancer patients: Resistin and visfatin as biomarkers of gastric cancer. J Gastroenterol. 2009;44:685–690. doi: 10.1007/s00535-009-0063-5. [DOI] [PubMed] [Google Scholar]
- 14.Nakajima TE, Yamada Y, Hamano T, Furuta K, Matsuda T, Fujita S, Kato K, Hamaguchi T, Shimada Y. Adipocytokines as new promising markers of colorectal tumors: Adiponectin for colorectal adenoma, and resistin and visfatin for colorectal cancer. Cancer Sci. 2010;101:1286–1291. doi: 10.1111/j.1349-7006.2010.01518.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wang B, Hasan MK, Alvarado E, Yuan H, Wu H, Chen WY. NAMPT overexpression in prostate cancer and its contribution to tumor cell survival and stress response. Oncogene. 2011;30:907–921. doi: 10.1038/onc.2010.468. [DOI] [PubMed] [Google Scholar]
- 16.Zhu Y, Guo M, Zhang L, Xu T, Wang L, Xu G. Biomarker triplet NAMPT/VEGF/HER2 as a de novo detection panel for the diagnosis and prognosis of human breast cancer. Oncol Rep. 2016;35:454–462. doi: 10.3892/or.2015.4391. [DOI] [PubMed] [Google Scholar]
- 17.Santidrian AF, LeBoeuf SE, Wold ED, Ritland M, Forsyth JS, Felding BH. Nicotinamide phosphoribosyltransferase can affect metastatic activity and cell adhesive functions by regulating integrins in breast cancer. DNA Repair. 2014;23:79–87. doi: 10.1016/j.dnarep.2014.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Domagala P, Huzarski T, Lubinski J, Gugala K, Domagala W. PARP-1 expression in breast cancer including BRCA1-associated, triple negative and basal-like tumors: Possible implications for PARP-1 inhibitor therapy. Breast Cancer Res Treat. 2011;127:861–869. doi: 10.1007/s10549-011-1441-2. [DOI] [PubMed] [Google Scholar]
- 19.Li D, Bi FF, Chen NN, Cao JM, Sun WP, Zhou YM, Li CY, Yang Q. A novel crosstalk between BRCA1 and poly (ADP-ribose) polymerase 1 in breast cancer. Cell Cycle. 2014;13:3442–3449. doi: 10.4161/15384101.2014.956507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bajrami I, Kigozi A, van Weverwijk A, Brough R, Frankum J, Lord CJ, Ashworth A. Synthetic lethality of PARP and NAMPT inhibition in triple-negative breast cancer cells. EMBO Mol Med. 2012;4:1087–1096. doi: 10.1002/emmm.201201250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Samal B, Sun Y, Stearns G, Xie C, Suggs S, McNiece I. Cloning and characterization of the cDNA encoding a novel human pre-B-cell colony-enhancing factor. Mol Cell Biol. 1994;14:1431–1437. doi: 10.1128/MCB.14.2.1431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jia SH, Li Y, Parodo J, Kapus A, Fan L, Rotstein OD, Marshall JC. Pre-B cell colony-enhancing factor inhibits neutrophil apoptosis in experimental inflammation and clinical sepsis. J Clin Invest. 2004;113:1318–1327. doi: 10.1172/JCI19930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhou T, Wang T, Garcia JG. Expression of nicotinamide phosphoribosyltransferase-influenced genes predicts recurrence-free survival in lung and breast cancers. Sci Rep. 2014;4:6107. doi: 10.1038/srep06107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hong SM, Park CW, Kim SW, Nam YJ, Yu JH, Shin JH, Yun CH, Im SH, Kim KT, Sung YC, Choi KY. NAMPT suppresses glucose deprivation-induced oxidative stress by increasing NADPH levels in breast cancer. Oncogene. 2016;35:3544–3554. doi: 10.1038/onc.2015.415. [DOI] [PubMed] [Google Scholar]
- 25.Zerp SF, Vens C, Floot B, Verheij M, van Triest B. NAD+ depletion by APO866 in combination with radiation in a prostate cancer model, results from an in vitro and in vivo study. Radiother Oncol. 2014;110:348–354. doi: 10.1016/j.radonc.2013.10.039. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The analyzed datasets generated during the study are available from the corresponding author upon reasonable request.